
Abstract
Acquired brain injury (ABI) is the second most common cause of disability in the United States. Prior research highlights family functioning as an important predictor of psychosocial outcomes in the ABI population; however, there remains limited research aimed at understanding the role of family functioning in predicting rehabilitation progress and community participation. A quantitative, exploratory, descriptive research design was used for this study. A total sample of 49 individuals with mild-to-moderate ABI were recruited from a university medical center and outpatient rehabilitation center. Participants completed measures of demographics, community participation, family functioning, and perceived rehabilitation barriers. Data were analyzed using descriptive statistics and multiple regression (MR) analysis. Two MR models were examined, one with rehabilitation barriers as the dependent variable and one with community participation as the dependent variable. Financial support and perceived rehabilitation barriers contributed significantly to variance in community participation satisfaction, while financial support, family functioning, and community participation satisfaction each accounted for a significant portion of variance in perceived rehabilitation barriers. Overall, the full MR 1 model accounted for 33% of variance in community participation satisfaction, while the full MR 2 model accounted for 51% of variance in perceived rehabilitation barriers. Although more research with larger, more diverse samples is needed, this study provides rehabilitation and counseling professionals with important psychosocial concepts to consider in assessment and treatment and helps clarify the role of family in promoting positive rehabilitation and participation outcomes in the ABI community.
Acquired brain injury (ABI) is defined as any type of damage to the brain that occurs after birth (i.e., traumatic brain injury [TBI], stroke; De Luca et al., 2016). ABI is the second most common cause of physical disability in America, affecting roughly 13.5 million Americans (Goldman et al., 2022). Common forms of ABI include TBI and stroke, while less common forms include brain damage due to anoxia, tumors, and neurodegenerative conditions (Goldman et al., 2022). ABI is associated with a wide variety of long-term impairments in cognitive, perceptual, physical, and behavioral functioning. Additionally, ABIs often have a negative impact on family functioning, community participation, and quality of life in general (Aza et al., 2020; Larøi, 2003; Man et al., 2004). More specifically, both quantitative and qualitative research indicates that individuals with ABI and related disabilities experience less community participation and less satisfaction with community participation because of inaccessible environments, stigma toward brain injury and disability, lack of support services, lack of equitable social opportunities, communication challenges, and the impact of anxiety and depression post-injury (Lakhani et al., 2022; Thompson et al., 2016).
Although research has contributed greatly to our understanding of factors that influence community participation and functional outcomes, there is still a mixed understanding of which environmental factors (e.g., family) contribute to improved rehabilitation and community participation outcomes in the ABI population. Community participation is related to quality of life and functional improvement after ABI, and it is a key component of successful rehabilitation (Cicerone, 2004; Lama et al., 2020; Nalder et al., 2018). Although there remain disagreements in the operationalizing of community participation, it is commonly defined as meaningful integration within the home, workplace, and personal social contexts (Cicerone, 2004; Kersey et al., 2020). Past research has demonstrated the benefits of community participation to one’s well-being, self-efficacy, life satisfaction, and overall psychological and physical health (Cicerone et al., 2004; Lama et al., 2020; Nalder et al., 2018). Community integration in one’s community has been directly linked to self-esteem and adaptive coping (So et al., 2023). Additionally, current literature indicates that community participation is associated with greater self-efficacy, health, social functioning, and rehabilitation after an ABI (Burns-Lynch & Musa, 2016; Cicerone et al., 2004; Haldane et al., 2019). Given the importance of community participation to psychosocial adjustment post-injury, it is important to develop psychosocial interventions that promote positive rehabilitation and participation outcomes. Identifying modifiable predictors of community participation and rehabilitation progress/barriers is often a prerequisite to developing effective psychosocial interventions. The development of counseling and related psychosocial interventions requires intervention targets that can be changed, such as environmental accessibility, coping skills, family relationships, and social support. However, while there must be consideration of stable factors, such as age, race/ethnicity, intelligence, and type of injury or impairment, counseling and related psychosocial interventions do not target these as agents of change. Thus, the identification of factors that can be modified or adapted through counseling and related interventions is often necessary for developing interventions that effectively promote positive psychosocial change.
Common modifiable psychosocial factors that predict community participation and rehabilitation outcomes in those with ABI include psychological health and well-being, coping style, family functioning and caregiver support, access to services and resources, and knowledge about disability (Hoffman et al., 2007; Juengst et al., 2014; Wolters et al., 2010). Research on the role of psychological and coping variables in ABI rehabilitation has received some attention in recent decades (e.g., Rickardsson et al., 2022; Wolters et al., 2010). However, there remains a dearth of literature identifying the specific role of family functioning and family system factors in predicting community participation and related rehabilitation outcomes in the ABI population. Given that research identifies community participation and family support as important components of overall quality of life for persons living with disability (Kersey et al., 2020), it is beneficial to gain a clearer understanding of the relationship among family functioning, community participation, and rehabilitation outcomes in the ABI community. This information will also likely help with the development of family system-level psychosocial and rehabilitation interventions.
ABI and Family Functioning
Research has consistently indicated that ABI significantly affects functioning and relationships within the family system (Kreutzer et al., 2009; Maggio et al., 2018; Perlesz et al., 1999; Tramonti et al., 2015). Individuals experiencing TBI generally report increased relational and interpersonal difficulties, poorer family relationships, and less family support compared with individuals without TBI. Problems with family functioning after TBI onset are well-documented, as evidenced by less effective coping, problem-solving, and communication (Haarbauer-Krupa et al., 2021; Kreutzer et al., 2009). Additionally, studies have indicated that caregivers are more susceptible to developing depression and anxiety symptoms post-injury (Ennis et al., 2013). Similarly, families post-stroke often indicate a significant increase in family distress and functioning, including challenges in problem problem-solving, family communication, role definition, behavior control, and affective involvement (Clark & Smith, 1999; Palmer & Glass, 2003). Pre- and post-injury family functioning has been shown to predict various psychosocial and functional outcomes in the ABI population, including neurobehavioral recovery, participation in rehabilitation services, psychological well-being, and quality of life (Epstein-Lubow et al., 2009; Palmer & Glass, 2003; Sady et al., 2010; Sander et al., 2002; Yang et al., 2021). Although multiple models of family functioning exist (e.g., Beavers Systems Model of Family Functioning [Beavers & Hampson, 1993], McMaster Model of Family Functioning [Epstein et al., 1978], Process Model of Family Functioning [Steinhauer et al., 1984]), the construct generally refers to conceptual frameworks that define adaptive and maladaptive functioning and processes within a family.
For this study, the Process Model of Family Functioning (Steinhauer et al., 1984) was utilized to conceptualize family functioning, as it has been applied and validated with individuals from brain injury and related disability communities (Zhang, 2018). The Process Model (Steinhauer et al., 1984) identifies the following components of family functioning: (a) Task Accomplishment, (b) Role Performance, (c) Communication (including Affective expression), (d) Affective Involvement, (e) Control, and (f) Values and Norms. The Process Model states that the main goal of a family is to successfully work together to achieve a variety of basic, developmental, and crisis tasks throughout life (Task Accomplishment). Task accomplishment is viewed as the most basic activity of the family. Task Accomplishment requires Role Performance, which is defined as the willingness of family members to take on specific roles (e.g., parent, breadwinner, caregiver) and carry out the prescribed behaviors of each role. In a similar way, Task Accomplishment relies upon other family factors, including Affective Expression (ways emotion is communicated across the family), Communication (how the family communicates and receives messages), Involvement (the kind of involvement/boundaries family members have with each other), and Control (the process by which family members influence each other). Lastly, the Process Model suggests that Values and Norms of the family culture determine how tasks are defined and how they are accomplished (Skinner et al., 2000; Skinner et al., 1995).
Historically, family research with the ABI population has focused on general family functioning/support and/or caregiver stress/burden post-ABI (e.g., Perlesz et al., 1999). More recent research, however, has begun to investigate the role of family functioning (and its components) in predicting psychosocial and related rehabilitation outcomes in individuals with ABI (Epstein-Lubow et al., 2009; Maggio et al., 2018; Palmer & Glass, 2003; Sady et al., 2010; Sander et al., 2002; Sander et al., 2012; Tramonti et al., 2015; Yang et al., 2021). Maggio and colleagues (2018), for example, found that individuals with ABI that have more cohesive and flexible families had better rehabilitation outcomes. Additionally, individuals with ABI that have families with clearly defined family roles, greater capacity to express emotions, and who proactively solve problems, demonstrate greater goal attainment and positive rehabilitation outcomes (Gerber & Gargaro, 2015).
ABI Rehabilitation, Community Participation, and Family Functioning
Within the context of rehabilitation, individuals with ABI often depend on family for diverse caregiving needs, activities of daily living, attending rehabilitation therapies and medical appointments, and helping maintain an at-home exercise regimen (Elbaum, 2019; Lundine et al., 2022; Maggio et al., 2018). Thus, when the family is experiencing adjustment difficulties, relational conflicts, and poor overall functioning, the individual’s recovery and rehabilitation are often negatively affected (Gan & Schuller, 2002; Scholten et al., 2020). For example, caregivers/carepartners that experience high levels of burden or emotional difficulties are less likely to be able to provide the kind of caregiving support needed, including helping with rehabilitation therapies or attending medical appointments (Qadeer et al., 2017). Lack of family support and family involvement also create challenges for rehabilitation progress and community participation (Bogner et al., 2019; Fisher et al., 2020; Kreutzer et al., 2009). In fact, family members are often excluded from many of the primary rehabilitation and psychosocial interventions and assessments post-injury (Maggio et al., 2018). Research considering the relationships among family functioning, rehabilitation progress, and community participation are lacking (Rasmussen et al., 2020); however, there a number of studies that have provided preliminary evidence of significant relationships.
Preliminary studies in this area suggest that family functioning and support play a critical role in the recovery and rehabilitation of individuals with ABI, as well as with psychosocial and family adjustment post-injury (e.g., Epstein-Lubow et al., 2009; Maggio et al., 2018; Palmer & Glass, 2003; Sady et al., 2010; Yang et al., 2021). Healthy family functioning is synonymous with improved social support, and social support is one of the most robust and consistent predictors of functional ability after onset of ABI (Kwakkel et al., 1996; Muldoon et al., 2019). Poor family functioning can also interfere with the family’s ability to provide appropriate and stimulating physical and cognitive activities needed for rehabilitation and improved independent functioning. For example, some family members may respond with overprotection by limiting the social activities and social participation of their care recipient with ABI (Palmer & Glass). Other family members may respond by distancing themselves and reducing relational contact. In both cases, the individual’s rehabilitation, functional recovery, and community participation are negatively affected. Other studies (Lax Pericall & Taylor, 2014; Palmer & Glass, 2003; Sander et al., 2002) indicate further consequences of poor family functioning, including poor treatment adherence, increased rehospitalizations, increased disability, and reduced rehabilitation progress, decreased management of co-occurring medical conditions and increased presence of psychological health issues such as depression.
Although current literature in this area has provided a foundational understanding, there remains a need for more studies that clarify the relationship among family functioning, rehabilitation and functional outcomes, and community participation (Sander et al., 2012; Sawasdinaruenart et al., 2021). Additionally, there is a need to identify which specific components of family functioning most significantly contribute to rehabilitation and participation outcomes (Foster et al., 2012; Rasmussen et al., 2023). The present exploratory study sought to address this gap by investigating the relationship among family functioning, rehabilitation barriers (and progress), and community participation outcomes in individuals with ABI. This study, specifically, investigated: (a) the specific contributions of family functioning and perceived rehabilitation barriers (progress) on community participation satisfaction; and (b) the specific contributions of family functioning and community participation satisfaction on perceived rehabilitation barriers (progress).
Method
Sample
The study sample consisted of 49 individuals with mild-to-moderate ABI. All the participants were diagnosed with ABI, but no specific type of ABI was targeted. Participant demographics are presented in Table 1. The participants were a convenience sample, given the exploratory nature of the study, and were recruited from a university medical center and outpatient rehabilitation center. The average age of the sample was 51.65 years (SD = 15.02). Approximately 63.3% of the sample identified as male, and the majority of the sample identified as white (n = 39; 79.6%). With respect to types of ABI, 24 (49.0%) individuals experienced a TBI, 20 (40.8%) experienced a stroke, and five (10.2%) with other forms of ABI (e.g., brain anoxia, brain tumor).
Demographics of Sample (N = 49).

Note. M = means; SD = standard deviation. Mean and standard deviations for categorical variables are not reported.
Procedure
Researchers obtained approval from their designated Institutional Review Board before initiating the study. Participants for this study were recruited through email, phone, and in-person. Due to the coronavirus pandemic, there were more participants recruited through phone and email than in-person. Interested participants were first screened to ensure they met inclusion criteria: (a) 18 years of age or older, (b) medically documented mild-to-moderate ABI, (c) no significant and persistent psychiatric disability prior to ABI onset, and (d) received any form of caregiving assistance from family post-injury. The last criteria regarding caregiving was included to help ensure that participants had received at least some form of assistance from family for the purpose of measuring family functioning. To help ensure diagnosis, participants were primarily identified for recruitment using a central data repository containing clinical, research, and administrative data sourced from a health care system in the Eastern U.S. Furthermore, the central data repository included information about prior psychiatric history and age.
Participants were also recruited through other methods, such as flier recruitment and in-person recruitment, at a University Medical Center and Outpatient Rehabilitation Center in North Carolina. In either case, participants were given directions to review the study consent form and the Health Insurance Portability and Accountability (HIPAA) forms (online or in person) prior to engaging in the study. HIPAA forms were required to be signed by participants if they agreed with having their medical record information reviewed or confirmed by key study personnel. Prior to consent, participants were asked a series of four questions that were taken from an instrument developed for assessing decisional capacity in clinical research (i.e., Jeste et al., 2007). The screener included questions regarding the purpose of the study, the reason for participating, the voluntary nature of the study, and the activities that are being asked of participants. The participants were required to correctly answer all four questions to demonstrate independent decision-making capacity and to show their understanding of the study. All participants demonstrated independent decision-making capacity. After participants were deemed eligible and gave their consent to participate, they were directed to the online study questionnaires.
Most participants completed all five questionnaires (see “Measures” section for details) through a data collection platform. The remaining participants (n = 5) were mailed a paper version of the questionnaires and mailed back the completed forms. After completion of study questionnaires, participants were mailed or emailed a US$20 to US$25 gift card.
Measures
There was a total of five questionnaires that participants were asked to complete. A brief description of these study questionnaires is provided below.
Demographics
Demographics for each participant were gathered throughout the study. The demographic variables collected included age, gender, race/ethnicity, educational level, income, type of ABI, living situation, financial support, and marital status (see Table 1 for subcategories). Age was collected as a continuous variable, while all other variables were collected as categorical variables. Financial support was defined as a binary categorical variable (yes = 1/no = 0), and included examples such as The Special Supplemental Nutrition Program for Women, Infants, and Children and “food stamps.” For example, if the participant receives a form of financial support, including food stamps, social security insurance, and/or other forms of state/federal financial support, this would be marked as a “Yes.”
Living situations included “living independently in a house or apartment,” ‘living with an immediate family member (e.g., parent or sibling), “living with extended family or close friends,” or “other.” ‘Living independently’ was defined as living without the current need for regular caregiving help and/or having one’s own housing. This included those that had their children still living with them, spouses, or other dependents. “Living with an immediate family member” was described as living with any family member that is within the more immediate biological family—sibling, parent, grandparents, or adult child that is providing housing. Importantly, the main purpose of the living situation question was to get a general sense of their living environment (rather than specific caregiving information). Although specific definitions were not provided on the measure, we believe that the item answers captured the living situation accurately. Lastly, marital status was categorized as “single” or “married/living with a partner.” Importantly, there were no significant differences across stroke and TBI groups on the primary outcomes nor predictor variables.
Primary Outcome Measures
Temple University Community Participation Measure
The Temple University Community Participation Measure (TUCPM) was used to measure community participation satisfaction. The original TUCPM (Salzer & Baron, 2006; Salzer & Burns-Lynch, 2016) was developed for measuring community participation in individuals with psychiatric disabilities. For this study, the TUCPM was used to measure community participation in those with ABI. The TUCPM is a 26-item measure that helps individuals explore their self-directed participation in the community. The measure includes questions that consider the different self-directed activities participants may have done either independently or with friends and family in the community over the last 30 days (Salzer & Burns-Lynch, 2016). Additionally, the TUCPM asks participants to identify whether the activity is important and whether it is done “enough,” “not enough,” or “too much.” For this study, we used this measure to get a “community participation satisfaction” score. This score was calculated for each participant by adding up activities identified as both “important” and that were done “enough,” and then dividing that number by the total number of activities marked as important. Community participation satisfaction scores range from 0 to 1.0, with 1.0 indicating satisfaction with participation in all important activities and 0 representing total dissatisfaction across all important activities. Reliability and validity of the instrument have been confirmed with the psychiatric disability population (i.e., Salzer et al., 2014). For this study, the original TUCPM (Salzer & Burns-Lynch, 2016) instrument instructions were modified to say, “Please answer questions as you would have prior to the coronavirus restrictions. In other words, what did you do BEFORE the coronavirus activity restrictions were put in place?” These changes allowed for study researchers to finish study recruitment without substantial changes to study protocol or negative impacts on data validity and generalizability.
Rehabilitation Checklist
Parts 1 and 2 of the Rehabilitation Checklist (RCL) were used to measure a primary outcome of the study, perceived rehabilitation barriers (and progress). The RCL (Salmon, 1998) is a client-centered instrument that was originally created to serve as a measure that enables clinicians to “accurately identify potential obstacles to rehabilitation and the degree of adverse impact that a traumatic experience or disease process has had on the life of a client” (p. 1). The RCL helps determine the needs of clients recovering from injuries and illness with cognitive, physical, and/or emotional components (Rehabilitation Research Education and Evaluation Services [RRES], 2019). The RCL is developed for use by rehabilitation professionals, rehabilitation caseworkers, and vocational and physical rehabilitation personnel, and emphasizes the importance of assessing client’s needs in the rehabilitation process.
The RCL has been used in research to determine individual’s self-perceptions of their disability, rehabilitation progress, and long-term prognosis (Salmon, 1998). Part 1 of the RCL asks the participant to mark an “x” near the rehabilitation barriers that are relevant for them and that prevent or discourage them from returning to their regular lifestyle. There are 49 specific barriers listed, with the opportunity to add rehabilitation barriers that were not identified in the list. Most of the rehabilitation barriers are categorized into one of the following categories: Emotional, Work Environment, Cognitive, Employment, Physical, and Psychosocial (P-S). Some examples of items include, “Problems with dizziness,” “Worried about layoff,” “Difficulty engaging in social activities,” “Irritability/anger control,” and “Problems organizing/planning/making decisions/problem-solving.” Part 2 of the RCL asks the participant to identify and rank the five most significant barriers. A total RB score is calculated based on the number of rehabilitation barriers identified across each participant, with subscores for each type/category of rehabilitation barrier (Salmon, 1998). The subscale scores (Emotional, Work Environment, Cognitive, Employment, Physical, and Psychosocial) provide information on which categories (or types) of rehabilitation barriers are most represented within each participant, as well as across the whole participant sample. Reliability and validity of the RCL with individuals with brain injuries and related disabilities have been confirmed (Salmon, 1998). In a sample of 294 individuals with brain injuries and other traumatic injuries, the Cronbach Alpha reliability statistic for Total Barriers was strong (α = .85), with subscales ranging from α = .56 (Psychosocial) to α = .78 (Emotional).
Family Variables
Family Assessment Measure, Version III
The Family Assessment Measure, Version III (FAM-III; Skinner et al., 1995) is a self-report instrument that quantifies components of family functioning, as well as overall family functioning. The FAM-III is based on the Process Model of Family Functioning (Steinhauer et al., 1984). The Process Model is a framework for conducting family assessments and states that the main goal of a family is to successfully work together to achieve a variety of basic, developmental, and crisis tasks throughout life (Task Accomplishment). Task accomplishment is viewed as the most basic activity of the family. Task Accomplishment requires Role Performance, which is defined as the willingness of family members to take on specific roles (e.g., parent, breadwinner, caregiver) and carry out the prescribed behaviors of each role. In a similar way, Task Accomplishment relies upon other family factors, including Affective Expression (ways emotion is communicated across the family), Communication (how the family communicates and receives messages), Involvement (the kind of involvement family members have with each other), and Control (the process by which family members influence each other). Lastly, the Process Model suggests that Values and Norms of the family culture determine how tasks are defined and how they are accomplished (Skinner et al., 1995, 2000). The FAM-III includes an overall family functioning score and a subscale score for each of the components described above.
The FAM-III General Scale (Skinner et al., 1995) was the measure used for this study. The FAM-III General Scale includes 50 items with Likert-type response options (Strongly Agree, Agree, Disagree, Strongly Disagree). Most items are factored into one of seven family functioning components/subscales: (a) Task Accomplishment, (b) Role Performance, (c) Affective Expression, (d) Communication, (e) Involvement, (f) Control, or (g) Values and Norms. FAM-III subscale scores are normalized with a mean of 50 and standard deviation of 10. Higher subscale scores indicate poorer functioning within that component of family functioning, while lower scores indicate better functioning within that component. Similarly, lower overall family functioning scores indicate better overall family functioning. The FAM-III has been deemed reliable and valid across various families affected by disability, including developmental disabilities, psychiatric disabilities, eating disorders, chronic pain, and brain injuries (Gan et al., 2006; Sawasdinaruenart et al., 2021; Skinner et al., 1995, 2000).
Family Support for Community Participation after Brain Injury
This study modified the original Support for Community Integration questionnaire (Salzer & Baron, 2006 [UPENN Collaborative on Community Integration]) to account for this study’s focus on family. The original instrument was developed to measure “program staff” support for individuals with psychiatric disabilities. The questionnaire in this study (i.e., Family Support for Community Participation after Brain Injury) kept the same item content and most of the same verbiage from the original instrument but replaced “program staff” with “family” for each item. Sample items from the measure include, “I am encouraged and supported by my family to pursue employment opportunities,” “I am encouraged and supported by my family to pursue and participate in leisure and recreational activities,” and “I am encouraged and supported by my family to have romantic/intimate relationships.” Participants were asked to complete a Likert-type scale for each item (i.e., Strongly Agree, Agree, Disagree, Strongly Disagree). The higher the total score, the greater the family support for community participation. In other words, higher scores represented greater family support and encouragement for engaging in community-based activities.
To account for changes in family support due to the COVID-19 pandemic, the original instrument instructions were modified to include the following statement, “Please answer questions as it was before coronavirus restrictions were put in place.” These changes allowed for study researchers to finish study recruitment without substantial changes to study protocol or negative impacts on data validity and generalizability. Although no specific psychometric data has been published on this measure, it was developed specifically for measuring family support for community participation (Salzer & Baron, 2006) and mirrors the items in commonly accepted family support measures.
Data Analyses
Data was analyzed using preliminary screening procedures, descriptive statistics, and multiple regression (MR) to test the hypothesized relationships. Given the sample size, number of predictors, research questions, and exploratory nature of the study, the use of MR was deemed an appropriate method for detecting relationships (Gelman & Hill, 2021). SPSS 27.0 for Windows (IBM Corp., 2020) was used to perform all data analyses. Upon completion of data collection, additional analyses of outliers, missing data, and multicollinearity were conducted to ensure normality of the distribution.
MR was used to determine the relationships between the predictor variables and outcome variables. Demographic variables were entered into the regression equation, with family/rehabilitation/community participation variables entered as well. Entering the demographic variables was necessary to statistically control for participant demographics. None of the demographic variables significantly correlated with the primary outcomes. Age and education were chosen as the most representative demographic variables, given their relationship to other demographic variables in the sample and the historical significance of age and education on community participation and rehabilitation outcomes (e.g., Akyurek et al., 2019; Dashner et al., 2019). Due to lack of predictive significance and low racial/ethnic heterogeneity in the sample, the race/ethnicity variable was excluded from analyses. Overall, there were two MRs conducted, with rehabilitation progress/barriers and community participation satisfaction being the two primary outcomes. Materials and analysis code for this study are available by emailing the corresponding author.
Results
Preliminary analyses found no significant differences between participants with a history of stroke versus TBI in regard to the main predictors and outcome variables. The only significant differences across these two main types of ABI were that participants with a history of stroke (n=20) were significantly more likely than participants with TBI (n = 24) to report physical limitations and barriers as their main rehabilitation barriers, t(42) = 3.42, p = .001,; participants with a history of TBI, however, were significantly more likely to report cognitive barriers as their main rehabilitation barriers, t(42) = −2.15, p = .038. The finding that there were limited differences within the sample supports the notion that the findings in this study are likely generalizable across the two main types of ABI, stroke and TBI. Overall, the full MR 1 model accounted for 33% of variance in community participation satisfaction, while the full MR 2 model accounted for 51% of variance in perceived rehabilitation barriers. Primary research findings for the two main research questions and analyses are described below.
MR Model 1
The first research aim was to investigate the specific contributions of family functioning and perceived rehabilitation barriers (progress) on community participation satisfaction. Family functioning and family support did not correlate with community participation (see Table 2), so these family variables were excluded from the MR analysis. Some of the statistically significant correlations found in the preliminary analysis included family functioning and perceived rehabilitation barriers (r = .35, p<.05), Community participation satisfaction and perceived rehabilitation barriers (r = −.40, p<.01), and financial support and perceived rehabilitation barriers (r = .44, p<.01). It is important to note that high Family Functioning scores are interpreted as worse family functioning, which may explain the positive correlation with perceived rehabilitation barriers. There were no significant relationships found among the main demographics and the primary outcome of community participation satisfaction. A correlation matrix of study variables is provided in Table 2.
Correlation Matrix of Study Variables.
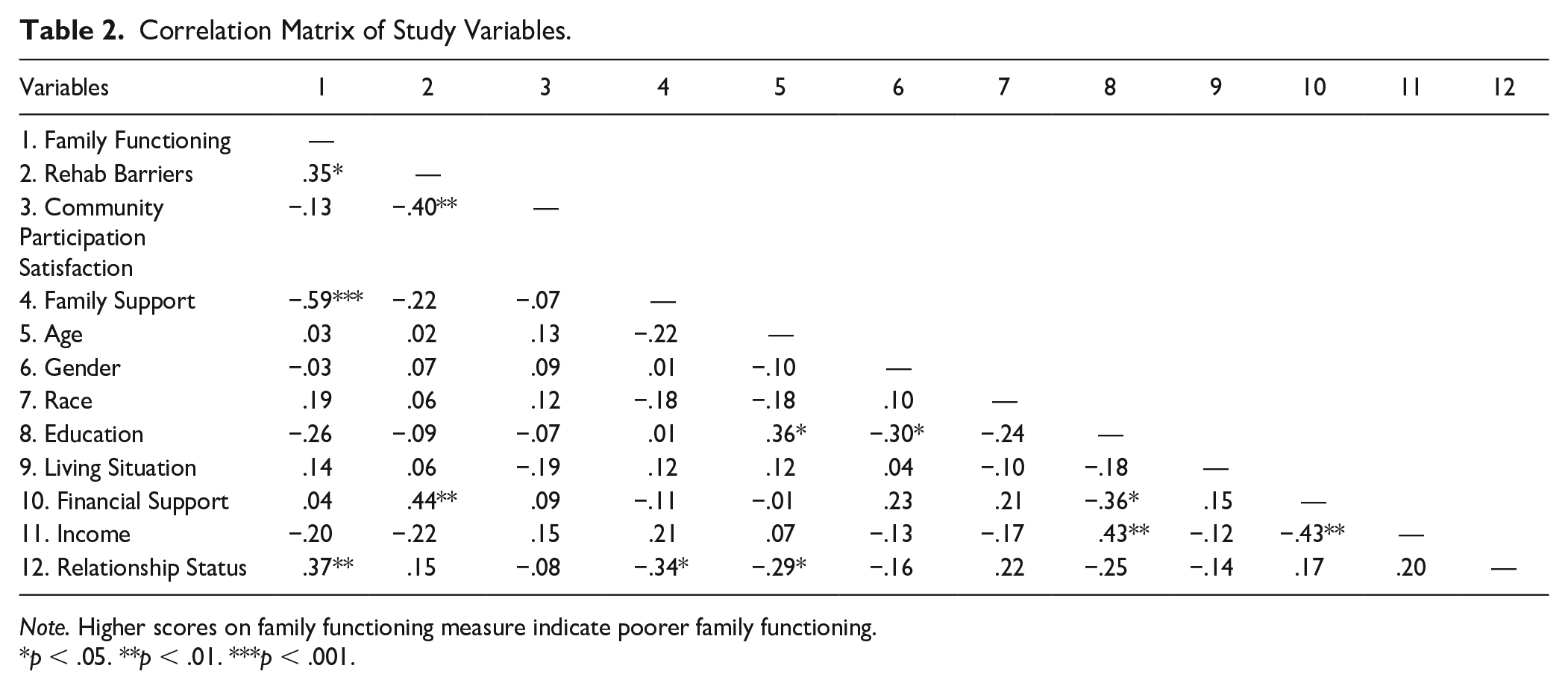
Note. Higher scores on family functioning measure indicate poorer family functioning.
p < .05. **p < .01. ***p < .001.
For the initial MR analysis, community participation satisfaction was the primary outcome. The predictor variables, in order of entry, were age, education, living situation, financial support, and rehabilitation barriers. As noted earlier, age and education were added to the model to statistically control these demographic variables. Living situation was entered into the model due to its historical importance in predicting social support and community participation (e.g., Mazzella et al., 2010; McLean et al., 2014). Financial support was added to the model because financial support and related economic indicators have been shown to predict disability, ABI rehabilitation outcomes, and community participation (Corrigan et al., 2021; Johnstone et al., 2003; Lorenz & Doonan, 2021). The last variable entered in the model was rehabilitation barriers, which was added because of its historical significance in predicting rehabilitation and community participation outcomes, and its connection to our main research question (e.g., Kortte et al., 2012; Lindén et al., 2010; Nicholson et al., 2014). Examining the standardized partial regression coefficients in the MR 1 model, F(5, 43) = 4.75, p = .003, R2 = .334, two individual predictors contributed significantly to variance in community participation satisfaction: financial support (β = .33, SE = .08, p < .05) and perceived rehabilitation barriers (β = −.54, SE = .003, p < .001). The results of MR 1 are presented in Table 3.
Summary of Linear Regression Model Predicting Community Participation.
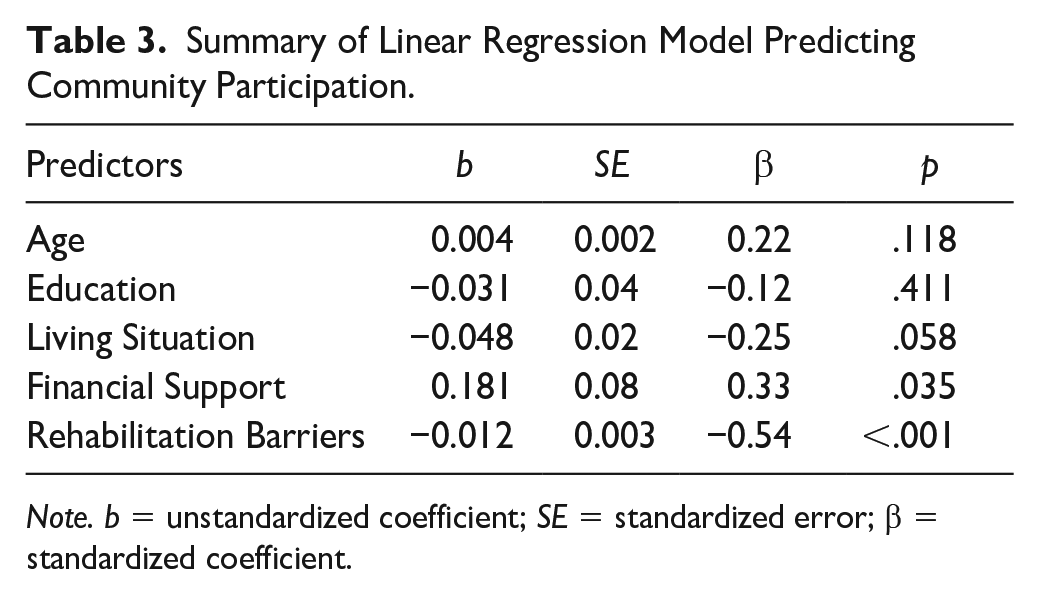
Note. b = unstandardized coefficient; SE = standardized error; β = standardized coefficient.
MR Model 2
The second research aim was to investigate the specific contributions of family functioning and community participation satisfaction on perceived rehabilitation barriers (or progress) in those with ABI. For the second MR analysis, perceived rehabilitation barriers was the primary outcome. The predictor variables, in order of entry, were age, education, financial support, family functioning, and community participation satisfaction. Age and education were added to the model to statistically control these demographic variables. The other variables were added because of their historical relevance to rehabilitation outcomes (Corrigan et al., 2021; Kortte et al., 2012; Maggio et al., 2018) and their significant correlation with perceived rehabilitation barriers in our preliminary analysis. As shown in the MR 2 Model below (Table 4) and correlational matrix (Table 2), other than financial support (r = .44, p<.01), demographic predictors did not significantly correlate with perceived rehabilitation barriers and did not account for much variance in perceived rehabilitation barriers. Examining the standardized partial regression coefficients in the MR2 model, F(5, 42) = 8.66, p < .001, R2 = .507, three individual predictors contributed significantly to variance in perceived rehabilitation barriers: financial support (β = .55, SE = 3.13, p < .001), family functioning (β = .31, SE = .15, p = .01), and community participation satisfaction (β = −.43, SE = 5.28, p < .001). The results of the second MR analysis are presented in Table 4.
Summary of Linear Regression Model Predicting Rehabilitation Barriers.
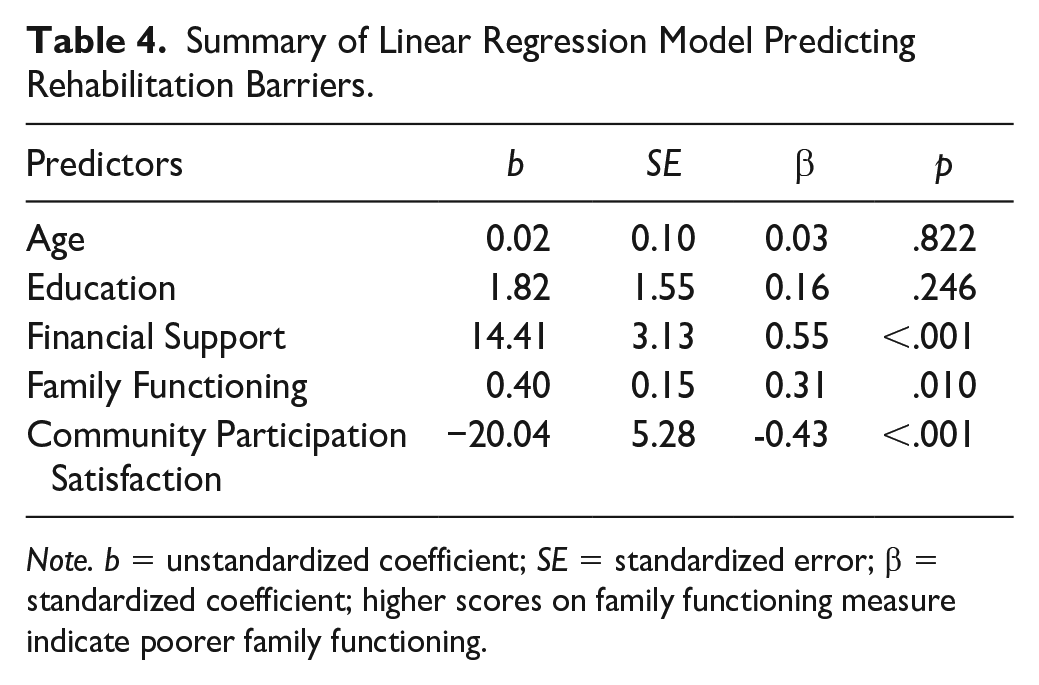
Note. b = unstandardized coefficient; SE = standardized error; β = standardized coefficient; higher scores on family functioning measure indicate poorer family functioning.
Discussion
This exploratory study sought to better understand relationships among family functioning, community participation, and perceived rehabilitation barriers in those living with ABI. To accomplish these goals, correlational and MR analyses were conducted. Results from the first MR analysis indicated that perceived rehabilitation barriers are a significant predictor of community participation satisfaction, even after controlling for age, education, living situation, and financial support. Specifically, community participation satisfaction increases as perceived rehabilitation barriers decrease. This finding regarding the inverse relationship between community participation and rehabilitation barriers is supported in prior research that highlights the role of functional limitations, disability, and psychosocial difficulties in predicting community participation (e.g., Ezekiel et al., 2019; Kortte et al., 2012; Lindén et al., 2010; Nicholson et al., 2014). Furthermore, this finding supports the notion that it is important for rehabilitation professionals to gather subjective client perceptions of rehabilitation progress, as it not only provides information about needed clinical/rehabilitation supports but can offer important insights into a client’s community participation satisfaction and, potentially, quality of life.
Interestingly, this study indicated that financial support and rehabilitation barriers are highly correlated (r = .44). These findings highlight that financial support may be a valuable rehabilitation assessment item and predictor of rehabilitation outcomes. Although more research is needed to confirm, assessing financial support status early in the rehabilitation process may give rehabilitation counselors, psychologists, and professionals a better understanding of potential barriers that may affect the rehabilitation journey for persons living with ABI.
Results of the second MR model indicated that financial support, family functioning, and community participation satisfaction are significant predictors of perceived rehabilitation barriers and progress, even after controlling for age and education. Although these findings have been supported in prior literature (e.g., Corrigan et al., 2021; Johnstone et al., 2003; Lorenz & Doonan, 2021; Sady et al., 2010; Sander et al., 2002, 2012), this study is one of the only studies that looked specifically at the relationships between family functioning, perceived rehabilitation barriers/progress, and community participation satisfaction in the ABI community. Importantly, family functioning remained a significant predictor of perceived rehabilitation barriers, even with the addition of age, education, financial support, and community participation satisfaction. Given that family functioning significantly predicted perceived rehabilitation barriers across individuals with differing age, education levels, financial support, and community participation satisfaction, it appears that family functioning is an important and fairly stable contributor to perceived rehabilitation barriers/progress in individuals with ABI.
Notably, while not displayed in the results section, most subcomponents of family functioning (task accomplishment, role performance, involvement, affective expression, control, values/norms) were significantly correlated with, and predictive of, perceived rehabilitation barriers, suggesting the important role of each family functioning component in predicting rehabilitation outcomes. These findings are important because it suggests that targeting specific family components in treatment and therapy may lead to improvements in rehabilitation and/or participation outcomes, however, more longitudinal intervention research is needed to establish any causal link. Prior research has supported the importance of family in rehabilitation (e.g., Maggio et al., 2018), and this study further solidifies the important role of, not just general family functioning, but specific subcomponents of family functioning as well. Future research should investigate these subcomponents more specifically, including whether a change in specific subcomponents of family functioning create changes in rehabilitation progress and related functional and participation outcomes for those in the ABI community.
Another interesting finding from the study included a significant association between the type of ABI (Stroke vs. TBI) and the type of barrier identified as most problematic in rehabilitation. Participants with a history of stroke were significantly more likely than participants with TBI to report physical limitations/barriers as their main rehabilitation barriers, while participants with a history of TBI were more likely to report cognitive limitations/barriers as their main rehabilitation barriers. This finding indicates that participants with a history of stroke perceived physical difficulties, such as physical restrictions for certain activities, restricted physical mobility, or limitations in self-care, as the most significant barrier to rehabilitation. Similarly, this finding suggests that individuals with a history of TBI perceive cognitive barriers, including challenges related to thinking/executive functioning, difficulty learning a new job, concentration and memory difficulties, and problems with planning/organizing, as the main barriers to rehabilitation. This finding likely has important implications for practice, as rehabilitation and psychosocial treatments post-injury may be able to more effectively tailor their programming to address the specific types of barriers most likely to create challenges to quality of life and rehabilitation progress, based on a client’s ABI status. For example, rehabilitation professionals and counselors may benefit treatment by incorporating more physical/mobility-related accommodations and/or interventions for individuals affected by stroke, while incorporating more cognitive-related accommodations and/or interventions for individuals affected by TBI. Larger sample, longitudinal research, however, is needed to fully establish these relationships and intervention effectiveness.
Overall, the results of this exploratory study suggest that family functioning factors are important predictors of perceived rehabilitation barriers, and perceived rehabilitation barriers are significant predictors of community participation satisfaction for those living with ABI. Interestingly, our study did not indicate a direct relationship between family functioning and community participation satisfaction. The lack of a detected relationship among these two variables is likely affected by the structure of the questionnaire, wherein participants differed on the number of activities they identified as “important.” Given the discrepancy across participants, it is possible that an actual significant relationship exists. In fact, prior research has highlighted the significant role of family functioning in predicting community participation (e.g., Bogner et al., 2019; Fisher et al., 2020; Kreutzer et al., 2009; Maggio et al., 2018). More research, with larger, more diverse samples is needed to confirm the strength and nature of this relationship. Future research would benefit from longitudinally designed studies that can establish a causal effect between specific family functioning factors and rehabilitation and functional outcomes.
Implications for Future Research and Practice
The study results suggest that assessing perceived rehabilitation barriers (or progress) during the rehabilitation process may be an effective method for understanding satisfaction with community participation for individuals living with ABI. In other words, rehabilitation professionals and counselors can administer a measure of perceived rehabilitation progress to not just gather information about the client’s perception of rehabilitation and their needs/strengths/supports, but to also gain a general understanding of their client’s community participation satisfaction. In essence, administering a perceived rehabilitation progress measure would potentially provide information about a client’s community participation without having to administer a separate participation assessment. A measure of rehabilitation progress or strengths may also have significant utility in the development of effective and individualized rehabilitation and psychosocial interventions. Given the importance of person-centered approaches, these findings further support the importance of highlighting the client’s voice, perceptions, and needs in assessment and treatment. Furthermore, this study highlighted the importance of assessing financial support and family functioning throughout ABI rehabilitation. Assessing perceived rehabilitation barriers/progress, family functioning, and financial support during different stages of rehabilitation may offer benefits for treatment planning and promoting positive rehabilitation outcomes. Future research and practice would benefit from investigating the impact of perceived rehabilitation progress assessments on rehabilitation and quality of life outcomes for persons living with ABI.
Although further research is needed to confirm (and clarify) the impact of family functioning (and its subcomponents) on rehabilitation progress and community participation for those living with ABI, this study establishes a likely relationship. Given the relationship between family functioning and perceived rehabilitation barriers, and the significant relationship between rehabilitation barriers and community participation satisfaction, this study suggests that addressing family functioning post-injury may have positive indications for both rehabilitation and overall quality of life. As research progresses, the authors hope to see more counseling, psychological, and psychotherapy studies identifying how improving specific family system components (i.e., communication, role performance, emotional expression) could create positive change in functioning, rehabilitation, and community participation outcomes for those living with brain injuries. Counselors, clinicians, psychologists, and rehabilitation professionals would benefit from the inclusion of family members as primary stakeholders throughout the assessment, rehabilitation, and clinical processes (Bogner et al., 2019). Many psychologists, counselors, and therapists are trained to address family adjustment, distress, and functioning, and should be a key part of the rehabilitation treatment plan for those with brain injuries. Targeted interventions that include modifying family dynamics to improve family functioning may improve outcomes for individuals with ABI. For example, counseling interventions that help improve family communication and relationships have been linked to improved psychosocial adjustment and quality of life in individuals living with ABI/TBI (Kreutzer et al., 2010). Additionally, including the family as a central element of the rehabilitation process may increase compliance, satisfaction, and other meaningful psychosocial outcomes for those experiencing ABI (Maggio et al., 2018).
It is important to note that there may be situations where family support is absent, where family functioning and changes in the family system are not realistic, and scenarios where families may not be able to access family therapy and/or family-directed interventions. For these individuals (and many others), there are additional avenues for getting support with community participation and rehabilitation after a brain injury. Other important services and supports for individuals with ABI include vocational rehabilitation, brain injury clubhouses, day treatment programs, peer support programs, Centers for Independent Living, and brain injury and stroke support groups.
In summary, this study supports the value of addressing family adjustment and functioning throughout ABI rehabilitation and therapy processes. From a family-systems perspective, the process of brain injury rehabilitation is not only about functional, cognitive, and physical improvements; rather, it is a collaborative process, in which rebuilding the foundations of identities, roles, and relationships is critically important (if not more so; Gan et al., 2006; Gan & Schuller, 2002). Family systems that are supportive, flexible, adaptive, and high functioning facilitate a successful psychosocial adjustment post-injury and help ensure maintenance of meaningful family relationships and community participation. Family dysfunction, in turn, confounds and multiplies the difficulties involved in successful rehabilitation and community participation (Palmer & Glass, 2003). Although interventions to target family functioning have been recommended for individuals with ABI, there remains a relative dearth of family system-level interventions for adults with ABI and their families due to focus on physical rather than holistic health (Rickardsson et al., 2022; Wolters et al., 2010).
Limitations
Due to the exploratory nature of the study, there are several limitations to highlight. First, the study sample was racially/ethnically homogenous, and the race/ethnicity variable was excluded from analyses due to lack of diversity. Future research should develop intentional research designs that more accurately represent the ABI population, especially the inclusion of more diverse samples, as health and rehabilitation experiences differ for Black, Indigenous, and People of Color (BIPOC) communities. Similarly, there remains limited research on brain injury and rehabilitation outcomes for persons from BIPOC communities, as most historical research includes primarily white, middle-class samples. Future studies should develop partnerships with families from BIPOC communities to identify barriers and facilitators to research participation so that researchers can increase engagement of marginalized communities in brain injury research.
Secondly, this exploratory study included a sample size of 49, which limits the generalization of the findings to the larger population of individuals with ABI. Future research with larger sample sizes, greater sample heterogeneity, and longitudinal designs are needed to confirm this study’s findings and to clarify the nature and directionality of relationships among family functioning, rehabilitation outcomes, and community participation. Future research should also implement an intentional recruitment design that more accurately reflects the ABI population, represents BIPOC communities, and ensures sufficient numbers of participants to allow for generalizability to the larger ABI population.
Third, we were not able to conduct reliability and validity testing with the measures used in the study, so it is recommended that future researchers conduct more psychometric reliability and validation studies on participation and rehabilitation measures with the ABI population. Lastly, due to the low participation rate of individuals with ABIs other than TBI and Stroke, we were not able to include participants with less common forms of ABI (e.g., brain anoxia, brain tumor) in some of the t-test and regression analyses. This limits the knowledge gained about other forms of ABI and limits the generalization of study findings to types of ABI beyond stroke and TBI. Future research should confirm whether relationships supported in this study are consistent across these other, less common forms of ABI. For example, future researchers can develop study inclusion criteria that focus specifically on individuals living with ABI resulting from anoxic brain injuries, brain tumors, and/or infection, rather than TBI or stroke.
Conclusion
The role of family functioning in predicting rehabilitation progress and community participation for those living with ABI is an important, yet underappreciated, area of research. The current exploratory study indicates that family functioning holds utility in predicting perceived rehabilitation barriers (and progress) for individuals with ABI. Furthermore, perceived rehabilitation barriers are predictive of greater community participation satisfaction for those living with ABI. Given the sample size and exploratory nature of this study, there remains a great need for further research with larger, more diverse samples to better clarify the relationship among family factors, rehabilitation progress, and community participation in the ABI community. Future clinical practice would benefit from including family-system level interventions throughout the rehabilitation journey, including within primary care, clinical, community, and psychosocial program settings.
Footnotes
Acknowledgements
The authors would like to thank Yasmine Eshera, M.S. and Abigail Thielemann, M.S. for their assistance with recruitment, data collection, and data organization.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded through a University of North Carolina Junior Faculty Development award funded by IBM and R.J. Reynolds Industries Inc.
Data Availability
Materials and analysis code for this study are available by emailing the corresponding author.