
Abstract
Psychosocial adaptation to chronic illness and disability (CID) involves a complex interplay of the client’s background factors with resilience and coping. To date, there have been few studies on psychosocial adaptation to CID in the Chinese context. To examine the predictors of psychosocial adaptation, we surveyed people with CID from community-rehabilitation settings and self-help groups (N = 224). The research questionnaire collected information on demographics, health-related factors, social support, resilience, coping strategies, psychosocial adaptation, and mental well-being. Resilience, coping strategies, health-related factors, and sex were found to be important predictors of psychosocial adaptation. Using structural equation modeling (SEM), we tested a conceptual model on how social support and health-related factors predict adjustment variables (resilience and coping strategies), which further affect psychosocial adaptation and mental well-being. All the variables are closely linked and the path coefficients are all significant. An overall fair model fit (comparative fit index [CFI] = 0.89; root mean square error of approximation [RMSEA] = 0.089) was obtained. The results provide support for the conceptual model we proposed based on health-related coping and the phase model of psychosocial adaptation. The key predictors of psychosocial adaptation and mental well-being in Chinese people with CID in Hong Kong are similar to those identified in non-Chinese studies.
Health, illness, and disability are key determinants of well-being and quality of life. Chronic diseases and disabilities have become common experiences in the aging population. According to the last census of Hong Kong in 2015, approximately 19.2% of the population had chronic diseases and 8.1% had acquired and developmental disabilities. Those with chronic illnesses and acquired physical disabilities (CIDs) often need ongoing medical treatment and rehabilitation over extended periods of time (Livneh, 2001). Chronic illness refers to a wide range of diseases such as diabetes, cardiovascular disorders, cancer, arthritis, autoimmune disorders, chronic lung disorders, and neurological disorders (Bernell & Howard, 2016). Acquired physical disabilities, such as traumatic brain injuries (TBIs) and spinal cord injuries (SCIs), are often caused by accidents, falls, violence, or recreational activities (Psarra & Kleftaras, 2013). Chronic illnesses and acquired physical disabilities (CIDs) can affect people’s ability to take care of themselves and disrupt their productivity, lifestyle, and relationships (de Ridder et al., 2008; Strine et al., 2008). Systematic reviews have shown that depression, anxiety disorders, and substance abuse are more prevalent among people who have CID than those who do not (Clarke & Currie, 2009; Lenze et al., 2001). It is often a considerable challenge for health professionals to maintain motivation for treatment and rehabilitation among people with CID (White et al., 2008). Psychosocial factors, especially catastrophizing beliefs, coping strategies, and social support, have significant impacts on a client’s pain and functionality (Jensen et al., 2011). People with CID face challenges with regard to body image and integrity, independence and autonomy, emotional adjustment, fulfillment of life roles, economic stability, and quality of life (Oris et al., 2018).
Current models of psychosocial adaptation suggest that several psychosocial factors are key to psychosocial adaptation, well-being, and quality of life of people with CID (Moos & Holahan, 2007; Moss-Morris, 2013). Health-related coping models assume that CID often places tremendous and overwhelming demands on individuals and their caregivers. Personal resources, health-related factors (such as course and history of illness, pain and fatigue symptoms, and visibility of illness/disability; Emerson et al., 2021; Gunn et al., 2012; Jensen et al., 2014), and social and environmental support are the background factors and resources in adaptation (Emerson et al., 2021; Jensen et al., 2014). For people with CID, cognitive reappraisal, the application of coping strategies, and learning adaptive tasks can contribute greatly to psychosocial adaptation and well-being.
This study aimed to address several research gaps and challenges in understanding psychosocial adaptation among people with CID. First, from a theory building and testing perspective, the role of resilience and coping strategies in psychosocial adaptation must be examined, in addition to illness variables and personal and social resources. Resilience is the process of adapting well to an extremely stressful or traumatic event and is regarded as the ability to “bounce back” and achieve personal growth in the process (Cal et al., 2015; White et al., 2008). There is accumulating evidence that resilience and coping are important mediators between symptoms or disabilities and psychosocial adaptation (Chen et al., 2019; Terrill et al., 2014; Thompson et al., 2018). Using structural equation modeling (SEM), we can test and identify the role of resilience and coping in psychosocial adaptation and how they interact with variables on illness characteristics and personal and social resources (Cal et al., 2015; Stuntzner & Hartley, 2014).
Second, we noted that many studies on people with CID used well-being or quality of life as outcomes of psychosocial adaptation, and many studies did not measure psychosocial adaptation. This study employed a phase model of emotional adjustment (Livneh, 2001; Livneh et al., 2006; Livneh & Parker, 2005) to measure psychosocial adaptation as an outcome of coping and adaptation. Based on this model, the Reaction to Impairment and Disability Inventory (RIDI) is a well-validated instrument that measures emotional adaptation as being either non-adaptive (e.g., anxiety, depression, externalized hostility) or adaptive (acknowledgment and acceptance).
Third, this study aimed to address the lack of research on psychosocial adaptation among people with CID in China. Due to cultural differences, the predictors of psychosocial adaptation in China could differ from those indicated in overseas study findings. A few notable examples of such studies have focused on a specific illness, such as SCI, epilepsy, or rheumatoid arthritis (RA; Chan et al., 2000; Lau et al., 2001; Liu et al., 2017; Siu et al., 2007). Few studies have recruited a large sample group with different types of disabilities and chronic illnesses to study psychosocial adaptation in Chinese populations.
Fourth, this study aimed to address the growing concerns about mental health issues and suicidality of people with CID in Hong Kong, where there is no formal practice of rehabilitation counseling (Russell et al., 2009; Szulc & Duplaga, 2019; Turner et al., 2006). This study could help raise community awareness about the importance of providing care and support for people with CID and the development of counseling services for them. The identification of key predictors of psychosocial adaptation will help deepen our understanding of the challenges faced by people with CID and provide suggestions on how rehabilitation counseling and social support services could address their psychosocial needs and help them develop resilience and growth.
In sum, this study aimed to examine and identify the significant predictors of psychosocial adaptation and mental well-being. It hypothesized that two groups of variables—one related to personal background and resources (demographic variables, health-related factors, social support) and another related to the adjustment process (resilience and coping)—are important predictors of psychosocial adaptation and mental well-being among people with CID.
Method
Participants
The target participants were people with CIDs who lived in the community independently or with support from carers or related services. The participants were required to read and complete a Chinese research questionnaire. We asked for help from the self-help groups for people with the following illnesses and disabilities to recruit participants: stroke, heart diseases, RA and autoimmune diseases, neurological diseases, epilepsy, traumatic disabilities (mainly brain injuries [TBIs] and SCIs), neurological disease, motor neuron disease, and Parkinson’s disease. Most of the research questionnaires were distributed to potential participants through community-rehabilitation services or self-help groups. The study involved 224 participants.
Instruments
The self-completed questionnaire collected information on demographic and social backgrounds and information on illness variables, including visibility of illness, symptoms, pain, and fatigue. We adopted several standardized measures of social support, coping strategies, resilience, psychosocial adaptation, and mental well-being. Table 1 lists the standardized scales used in the study with the estimation of internal consistency obtained from our data.
Structure and Internal Consistency of the Scales Used in the Research Questionnaire.
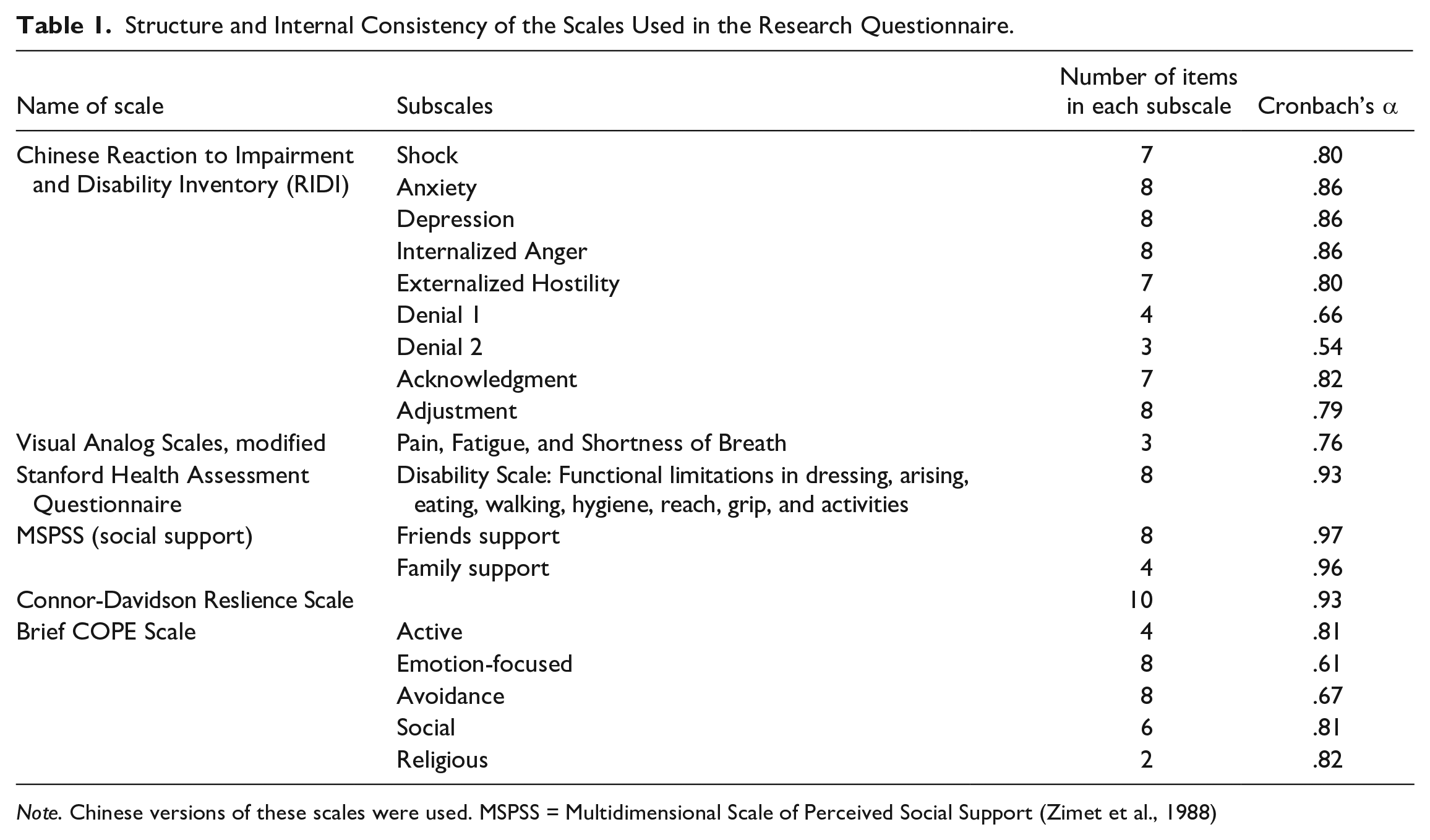
Note. Chinese versions of these scales were used. MSPSS = Multidimensional Scale of Perceived Social Support (Zimet et al., 1988)
Health-related factors
We employed three scales to measure pain, fatigue, and shortness of breath which are modified versions of the Visual Analog Scales (VASs) used for rating illness experiences among people with chronic illnesses (Lorig et al., 2005). The participants were asked to circle a number (ranging from 0 to 10) on the pain, fatigue, and shortness of breath scales, which could reflect the extent to which an individual was affected by the experience of each symptom over the past 2 weeks. A 6-point rating scale was used to measure the visibility of illness and participants answered using a scale ranging across invisible, barely visible, slightly visible, visible, very visible, and extremely visible.
Functional limitations
We used the 8-item Disability Scale of the Stanford Health Assessment Questionnaire (HAQ) to screen participants for functional disabilities in eight areas: dressing, arising, eating, walking, hygiene, reach, grip, and activities. Participants were scored on a 4-point scale from 0 (no difficulty) to 3 (unable to do). A higher score indicated more functional limitations. The test–retest reliability of the HAQ ranges from .87 to .99 and has a significant correlation with the convergent measures of disability (Bruce & Fries, 2003).
Social support
We used the Chinese version of the Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) to measure the levels of social support experienced by the participants. The MSPSS has been translated into multiple languages and is widely used as a brief measure of social support. The Chinese version of the MSPSS has been used to study coping among Chinese adolescents, schoolteachers, and caregivers of children with cerebral palsy. The study of the Chinese version confirmed a four-factor structure of the scale with subscale reliability coefficients ranging from .84 to .90 (Chou, 2000; Ho & Chan, 2017; Wang et al., 2017).
Resilience
The 10-item Connor–Davidson Resilience Scale (CD-RISC) is a short version of the 25-item resilience assessment tool (Battalio et al., 2017; Campbell-Sills & Stein, 2007; L. Wang et al., 2010). The instrument asked participants to respond to statements using a 5-point scale ranging from 0 (not true at all) to 4 (true nearly all the time), such as whether they viewed changes as a challenge, accepted responsibility to manage stress, and were able to remain optimistic. We used a 10-item Chinese version developed for (Yu et al., 2011) young people. The validation study confirmed the higher-order five-factor structure of the instrument with a Cronbach’s α of .89. The scale was also significantly correlated with measures of anxiety, depression, and social support.
Coping strategies
We adopted the Chinese version of the Brief COPE Scale, which is a theory-based, well-validated, and widely used measure of coping strategies (Carver, 1997; Carver et al., 1989; Tang et al., 2016). The original English Brief COPE scale provided an overall view of coping strategies among individuals under 14 subscales. Over the years, there have been many attempts to re-assess the factor structure of the scale, and we observed that several studies supported the use of five subscales: Emotion-Focused, Active (or Rational), Avoidance, Social, and Religious Coping Strategies (Krägeloh, 2011; Litman, 2006; Lyne & Roger, 2000; Tang et al., 2016).
Psychosocial adaptation to CID
Based on the theories of adaptation to loss, the RIDI was designed to measure adaptive and non-adaptive emotional reactions in response to CIDs (Antonak & Livneh, 1991; Livneh & Antonak, 1990; Livneh et al., 2006). A Chinese version of the RIDI (C-RIDI) was developed and validated for this study (Siu et al., 2021). The C-RIDI has satisfactory psychometric properties with satisfactory internal consistency, convergent validity, criterion-related validity, and factorial validity. We included the subscales under two second-order factors: (a) non-adaptive reactions comprising shock, anxiety, depression, internalized anger, and externalized hostility, and (b) adaptive factors covering the acknowledgment and adjustment subscales.
Mental well-being
We used the Chinese Short Warwick-Edinburgh Mental Well-being Scale (C-SWEMWBS) to measure the participants’ mental well-being (Ng et al., 2014; Tennant et al., 2007). The participants were asked to respond using a 5-point Likert-type scale. The possible total scores ranged from 7 to 35, with a higher score reflecting a higher level of mental well-being. A total score below 23 indicates poor well-being. Ng et al.’s (2014) study demonstrated that it has a good test–retest reliability of .68, and a significant correlation of .49 with the convergent measures of the World Health Organization Well-Being Index (WHO5).
Procedures
This study was reviewed and approved by the Human Subjects Ethics Committee of the Hong Kong Polytechnic University. To recruit participants, we contacted and solicited support from community-rehabilitation services and self-help organizations. The collaborating organizations invited their clients or members to participate in the study through notices, social media, or messaging apps. A research information sheet was distributed to potential participants and informed consent was obtained before data collection. The survey was done anonymously and potential participants were made aware that they were free to return the questionnaire to self-help group staff or research assistants if they did not want to participate in the study. The participants had the option of either completing the survey online or filling out hard copies. Hard copies of the survey questionnaire were distributed to and collected from the participants through the self-help groups and community rehabilitation centers. The questionnaire had 155 items and, during the pilot test, took 30 to 45 min to complete. We provided supermarket coupons to participants as incentives to participate in the study.
Data Analysis
We used multivariate analysis of variance (MANOVA) in the Statistical Package for Social Sciences (SPSS) to analyze the extent to which demographic variables (sex, primary disability), health-related factors (pain, fatigue, breathing, visibility, functional limitations), resilience, and coping strategies could predict adaptive and non-adaptive reactions in psychosocial adaptation. Using SPSS AMOS, we tested a structural equation model (SEM) derived from our conceptual model (see Figure 1) by combining the health-related coping and phase models of psychosocial adaptation. We hypothesized that social support is a key resource and that visibility, fatigue, breathing difficulty, pain, and functional limitations are important background factors. Social support and health-related factors are expected to determine resilience and coping, leading to adaptive and non-adaptive reactions to CID. Among the generic indicators of mental health, we selected mental well-being as the ultimate outcome of coping and psychosocial adaptation in people with CID.
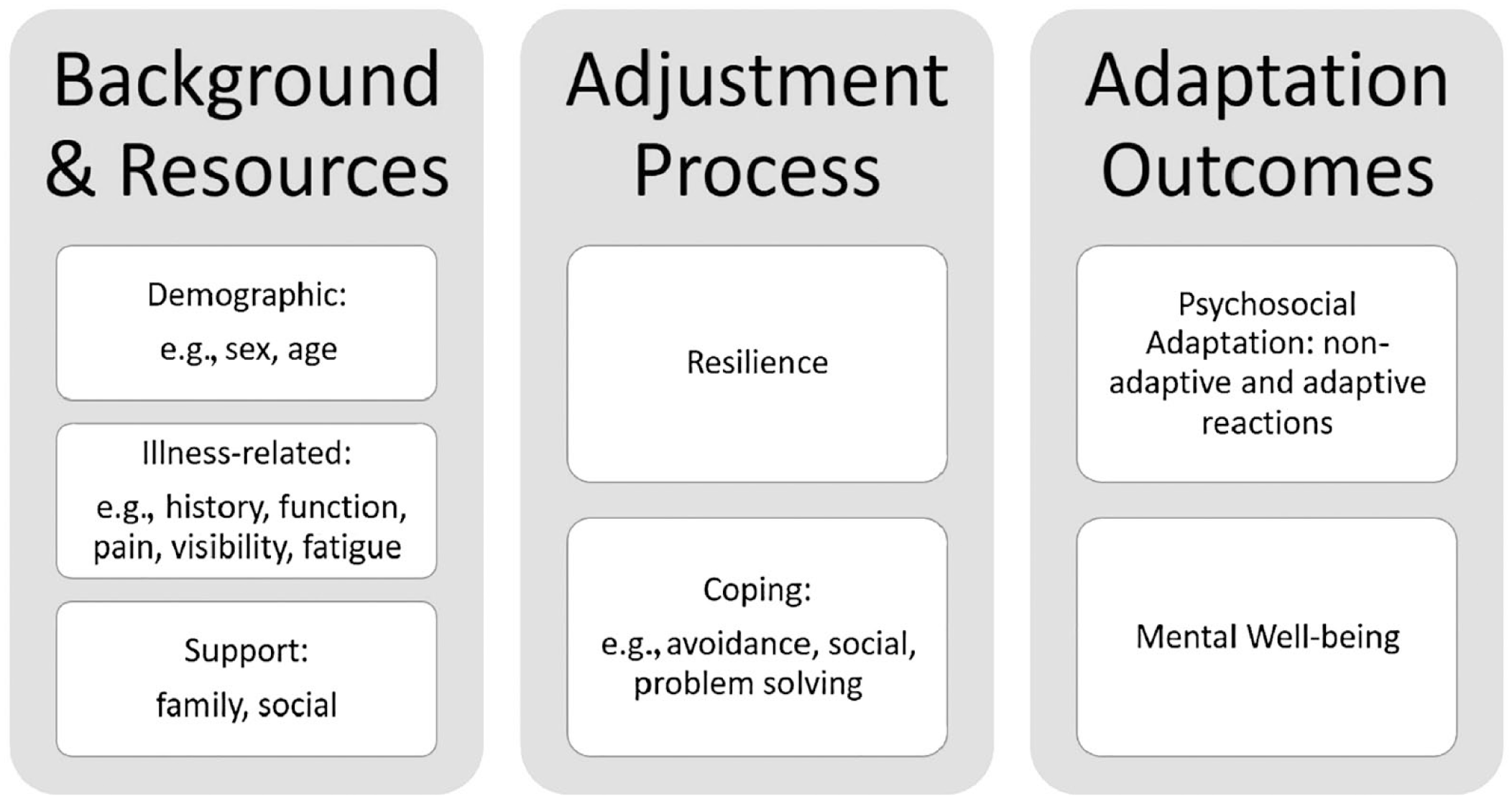
Conceptual model and variables measured in this study.
Results
Profile of Participants
Among the 224 participants, there were more women (64.1%) than men (35.9%). The participants had a mean age of 57.8 (SD = 12.9) years, and their history of illness was 14.4 years (SD = 13.0; see Table 2). The primary illnesses or disabilities were diabetes (15.2%), cancer (15.2%), heart disease (14.7%), RA or autoimmune disease (14.7%), stroke (12.9%), acquired physical disabilities or brain injuries (12.1%), neurological diseases (8.9%), and others (7.1%). The majority (73.2%) of participants had a secondary education or higher, and many were retired (41.2%), homemakers (18.6%), or unemployed (25.3%). In terms of family income, a large proportion (51.8%) of participants were from lower income families. In terms of health-related factors, participants tended to have low functional limitations (M = 1.6 out of scale 1–4) and low visibility of their illness (M = 1.6, out of scale 1–6). Fatigue was the most common illness experienced by participants (M = 5.38, SD = 2.32, out of range of 0–10), followed by pain (M = 4.31, SD = 2.88). A few participants experienced breathing difficulties (M = 2.42, SD = 2.59). The participants reported satisfactory support from both family (M = 5.17, SD = 1.77, out of a scale of 1–7) and friends (M = 4.79, SD = 1.73).
Summary Statistics of Demographic and Health-Related Factors of Participants (N = 224).
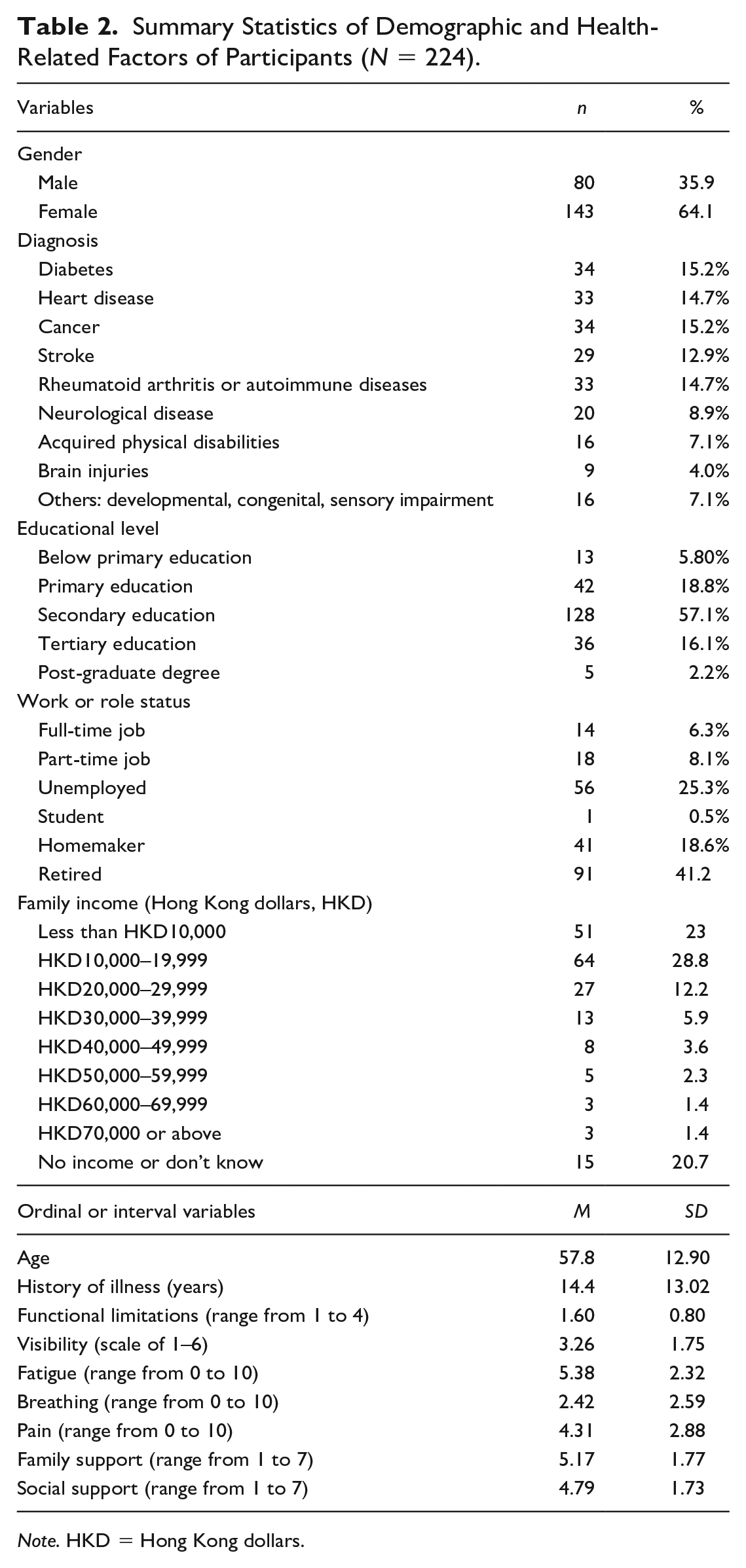
Note. HKD = Hong Kong dollars.
Predictors of Psychosocial Adaptation
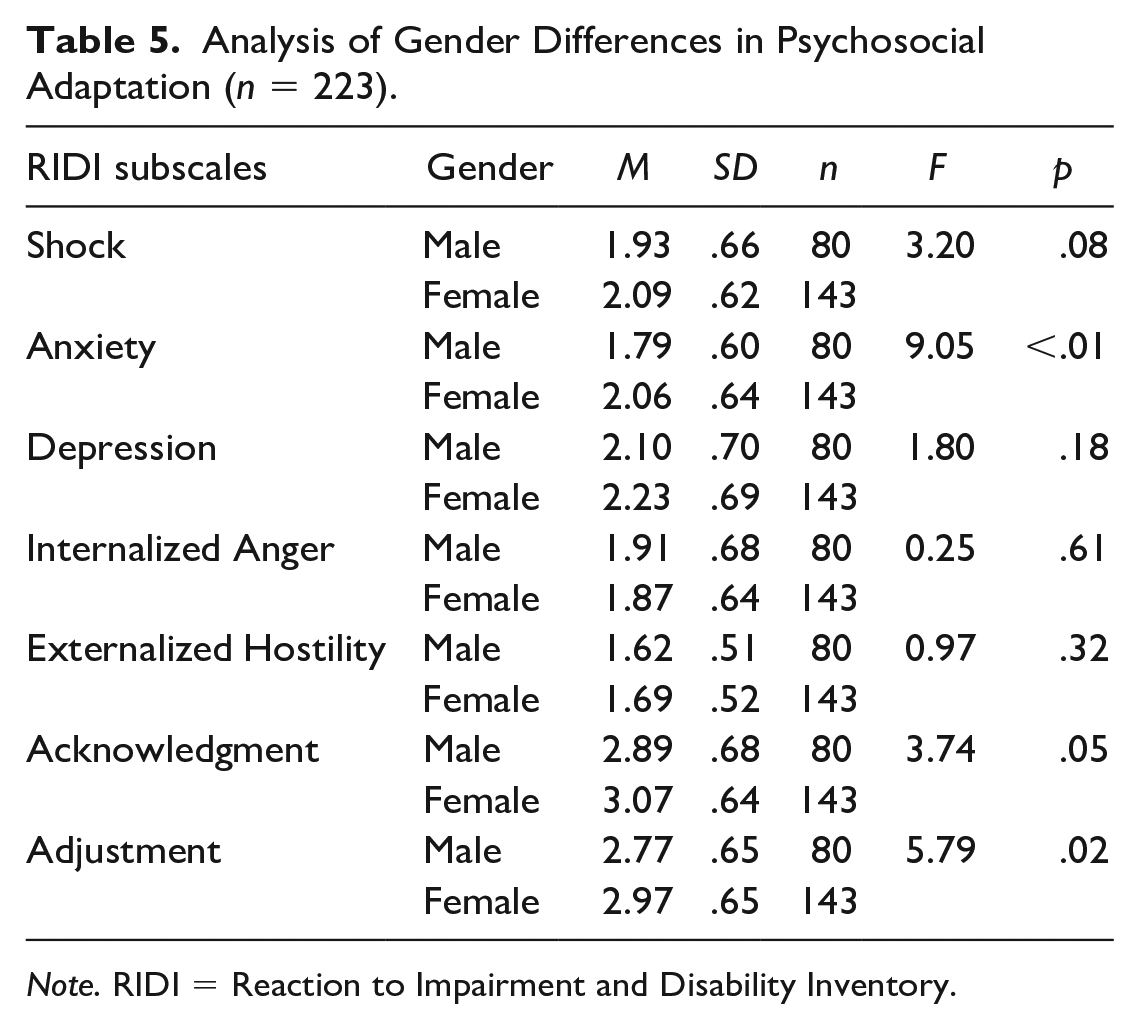
The results of the MANOVA indicated that several variables were significant predictors of the non-adaptive factor in the RIDI (covering the scales of shock, anxiety, depression, internalized anger, and externalized hostility), including sex (F = 5.27, p < .001), age (F = 3.56, p < .01), breathing difficulty (F = 8.05, p < .001), pain (F = 3.70, p < .01), resilience (F = 6.00, p < .001), and avoidance coping (F = 4.89, p < .001; see Table 3). However, only sex (F = 3.34, p = .04), resilience (F = 9.27, p < .001), and active coping (F = 11.07, p < .001) were significant predictors of the adaptive factor (Acknowledgment and Adjustment subscales; see Table 4). The two variables that were predictors of both adaptive and non-adaptive reactions to CID were sex and resilience. Sex did not interact with primary disability in the prediction of non-adaptive or adaptive factors. If only sex is entered as a predictor of RIDI subscales, it is noted that men and women differ mainly on two subscales. Women had significantly higher scores on the Anxiety (F = 9.05, p = .003) and Adjustment (F = 5.79, p = .02) subscales than men (see Table 5).
Analysis of Predictors of Non-Adaptive Scales of RIDI by General Linear Model MANOVA.
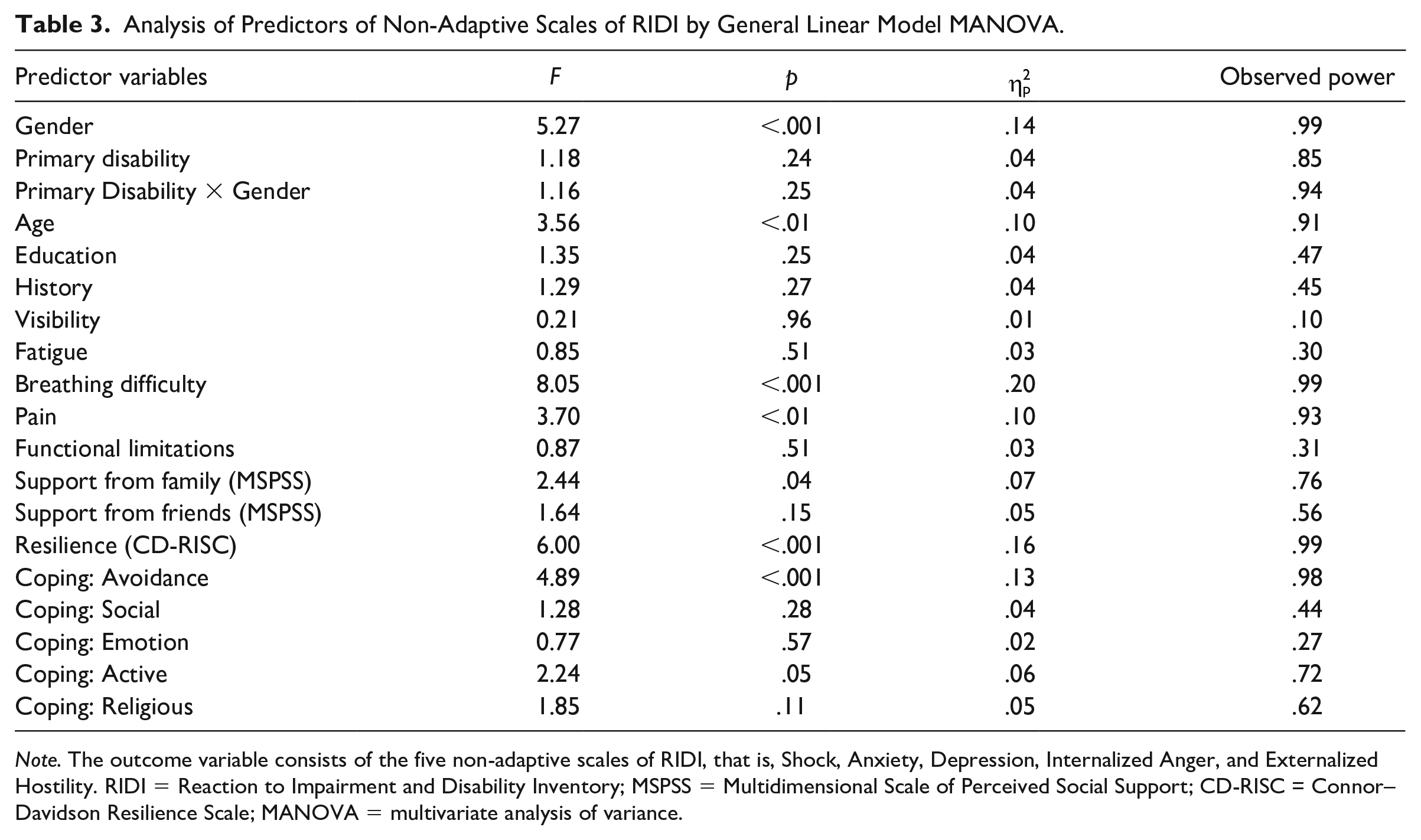
Note. The outcome variable consists of the five non-adaptive scales of RIDI, that is, Shock, Anxiety, Depression, Internalized Anger, and Externalized Hostility. RIDI = Reaction to Impairment and Disability Inventory; MSPSS = Multidimensional Scale of Perceived Social Support; CD-RISC = Connor–Davidson Resilience Scale; MANOVA = multivariate analysis of variance.
Analysis of Predictors of Adaptive Scales of RIDI Using General Linear Model MANOVA.
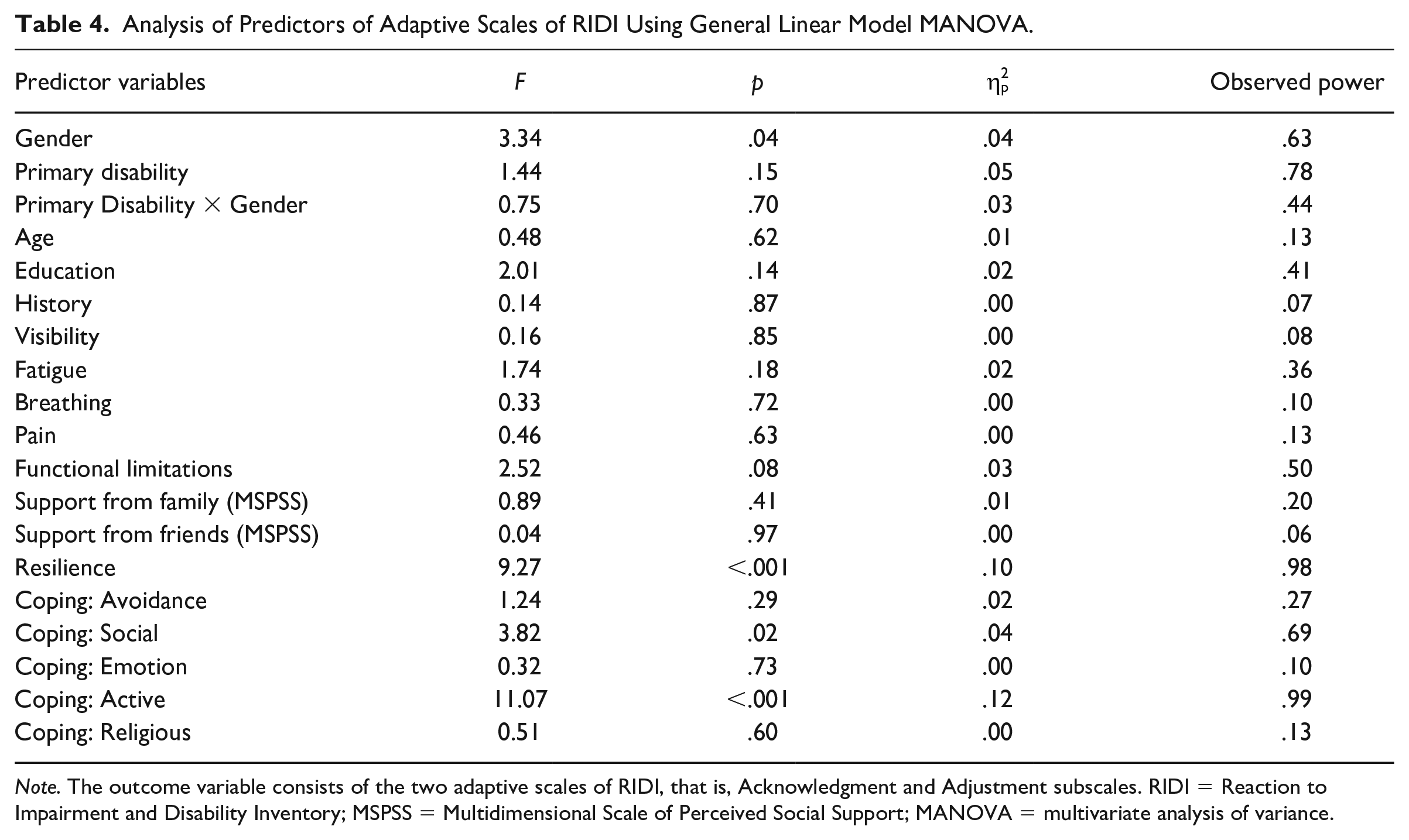
Note. The outcome variable consists of the two adaptive scales of RIDI, that is, Acknowledgment and Adjustment subscales. RIDI = Reaction to Impairment and Disability Inventory; MSPSS = Multidimensional Scale of Perceived Social Support; MANOVA = multivariate analysis of variance.
Analysis of Gender Differences in Psychosocial Adaptation (n = 223).
Note. RIDI = Reaction to Impairment and Disability Inventory.
Modeling the Predictors of Psychosocial Adaptation and Mental Well-Being
In preparation for SEM, a correlation matrix was generated to check the relationships among the key variables in the study (see Table 6). Figure 2 shows the fitted path model from SEM. All the paths in the model were significant, indicating the relationship between the hypothesized variables. As suggested by the modification indexes, some covariance was added between support from family and friends and among the five health-related factors. Adding all these covariances together leads to an increase in the overall model fit. The overall model fit was good (comparative fit index [CFI] = .89, root mean square error of approximation [RMSEA] = .089). All background and health-related variables contributed significantly to resilience, coping, and mental well-being. Resilience contributed more to non-adaptive reactions than adaptive reactions; it also contributed significantly and directly to mental well-being. Both resilience and coping contribute to a reduction in non-adaptive reactions and an increase in adaptive reactions. Adaptive reactions contributed to mental well-being positively while non-adaptive reactions contributed negatively. A goodness-of-fit index lower than .08 can be regarded as an acceptable fit (Kline, 2016).
Correlations Among Key Variables Included in the Structural Equation Modeling.
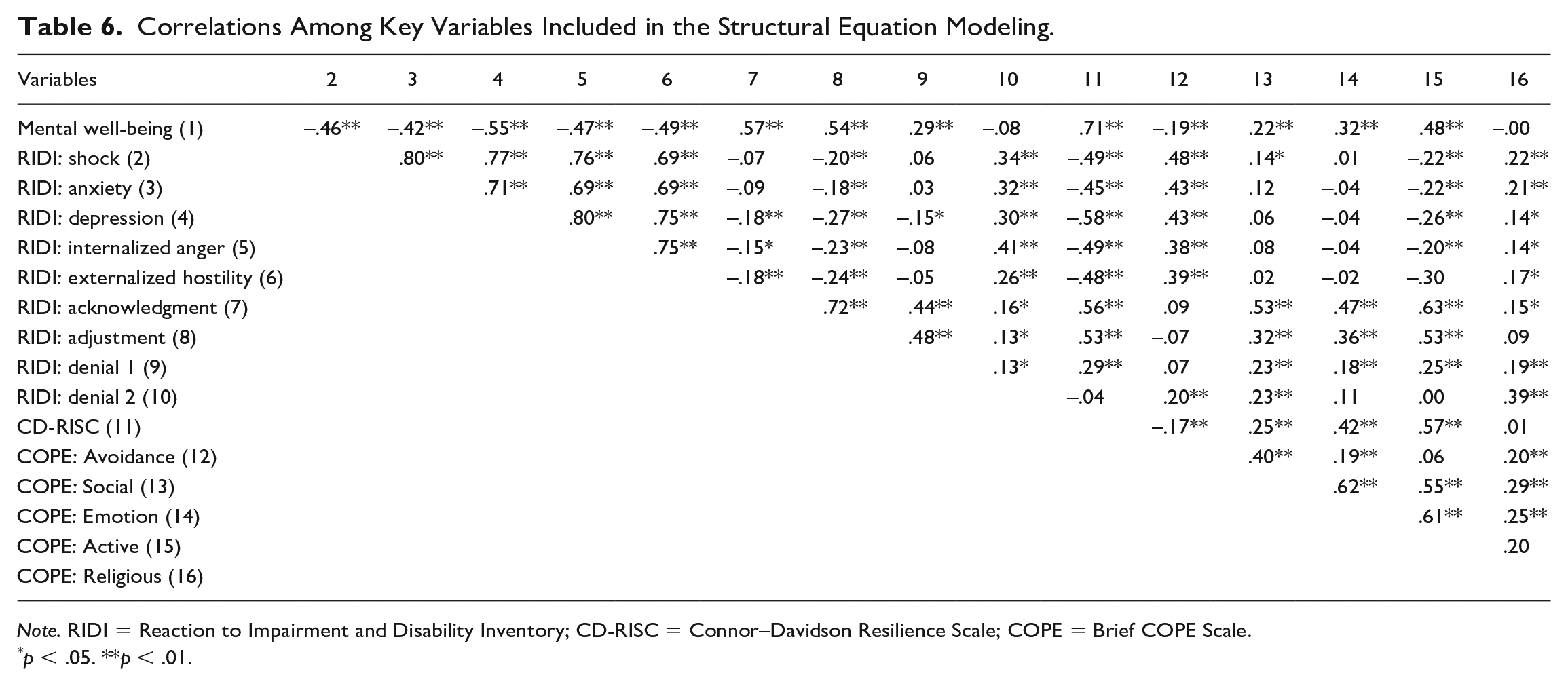
Note. RIDI = Reaction to Impairment and Disability Inventory; CD-RISC = Connor–Davidson Resilience Scale; COPE = Brief COPE Scale.
p < .05. **p < .01.
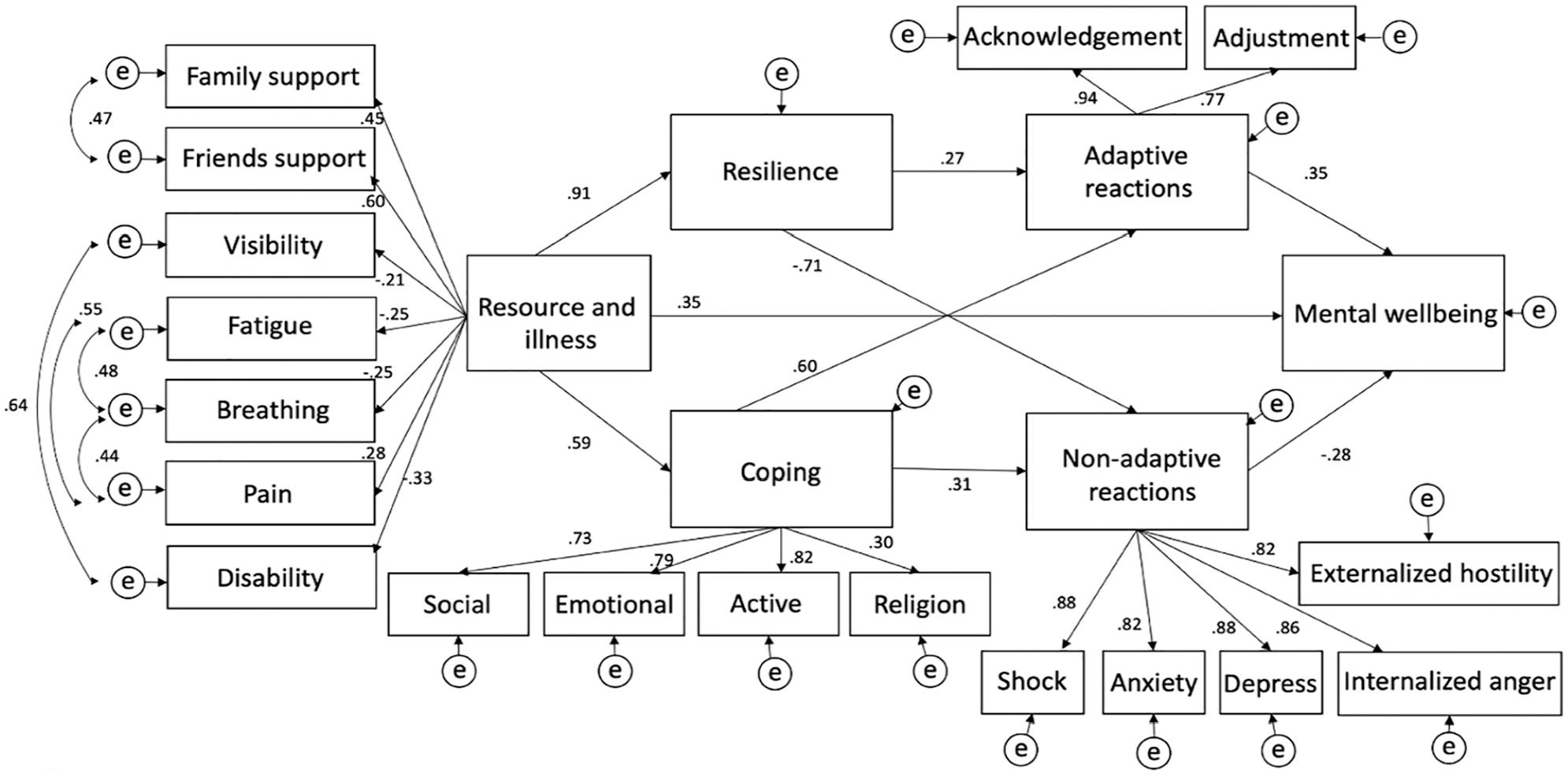
Fitted SEM on predictors of psychosocial adaptation among people with CID.
Discussion
The study demonstrated that all hypothesized background and adjustment process variables contributed to psychosocial adaptation and mental well-being. There are several important observations. First, the results of the MANOVA indicated that only certain variables predicted the non-adaptive and adaptive reactions during psychosocial adaptation. Sex and resilience were the only common variables that were significant predictors of both adaptive and non-adaptive reactions to CID. This result is in accordance with the findings of previous studies that have found that women tend to perform better than men with psychosocial adaptation to CID. In this study, women not only had significantly higher acknowledgment and adjustment scores than men but also had higher anxiety scores than men. These differences may be associated with other sex-based differences with regard to social support, coping, spirituality, and coping strategies (Clinciu & Cazan, 2014; di Pilla et al., 2016; Jacobs-Lawson et al., 2010; Nicholas, 2000). The importance of resilience in the psychosocial adaptation to CID has been highlighted in many studies and reviews (Cal et al., 2015; Kim et al., 2016; Kools et al., 2008; White et al., 2008). Resilience correlates negatively with depression, anxiety, and somatization, and can even influence the course of illnesses (Cal et al., 2015). Many researchers and practitioners in rehabilitation have advocated the development of strength-based programs to build resilience among people with CID (Stuntzner & Hartley, 2014; White et al., 2008).
Second, the MANOVA results supported that avoidance coping significantly predicted non-adaptive reactions while active coping predicted adaptive reactions. This is consistent with a wealth of previous studies that focused on how coping strategies are linked to emotional adjustment and stress management in a wide range of illnesses and disabilities (Livneh, 1999a, 1999b; Livneh & Martz, 2014; Wong et al., 2019). Third, two health-related factors—breathing difficulty and pain—significantly predicted non-adaptive reactions. This result is consistent with the predictions of health-related coping theories. Chronic pain, breathing difficulty, or fatigue are commonly experienced by people with chronic illnesses (such as fatigue in diabetes or breathing difficulty in chronic obstructive pulmonary disease) and disabilities (such as pain in SCIs or RA), and can significantly elicit non-adaptive coping (Jensen et al., 2011).
Fourth, as we used SEM to test an overall conceptual model of psychosocial adaptation, we found that all hypothesized variables contributed significantly to psychosocial adaptation and mental well-being. All path coefficients were significant and the directions of the relationships were consistent with our hypotheses. For instance, all health-related factors are negatively associated with the latent variable of the client’s background, while social support variables are positively associated with the latent variable of resources and health-related factors. Another example is that adaptive and non-adaptive behaviors are linked positively and negatively, respectively, with mental well-being.
However, while the fit of the SEM is acceptable, and despite modifications and re-fitting, it still falls slightly short of the standard of a good model fit. This insufficiency of the model fit could be due to several reasons. First, it is possible that important predictors were not included. In particular, RIDI had one more factor (denial), which we were unable to fit into the SEM. Studies of the factorial structure of the RIDI (Antonak & Livneh, 1991; Livneh et al., 2006) have indicated that the Denial subscale has two subscales, which might be termed “magical cure and disappearance of illness” and “bargaining and conditional recovery.” These two Denial subscales were found to be correlated with both adaptive and non-adaptive reactions to CID and were found to exert differential but substantial impacts on both adjustment and maladjustment (Livneh et al., 2006). However, it is not possible to maintain a non-recursive model for testing if we add the Denial subscales into the hypothesized model. Second, several demographic variables were excluded from the data analysis. This was due to various reasons. While we found sex-based differences in psychosocial adaptation in the MANOVA, we did not have a sample large enough to split the data for testing separate models for men and women. In addition, the variables of age and history correlated substantially and neither variable loaded significantly on the latent variable of the resources and health-related factors. In short, we cannot fully examine the impact of several background factors on SEM. Third, avoidance coping was significantly associated with the RIDI’s non-adaptive scales but this path was dropped and became insignificant in the SEM. The paths for social, emotional, active, and religious coping remained significant in SEM. In further research, researchers could try to use the variable of coping flexibility instead of including a range of coping strategies as predictors of psychosocial adaptation. Coping and cognitive flexibility are essential for choosing appropriate behavioral coping responses and they both exert significant effects on the adjustment to stressful life changes (Cheng et al., 2014; Dajani & Uddin, 2015). Fourth, the modeling of predictors of psychosocial adaptation in this study is mainly based on a model of adaptive and non-adaptive reactions and how coping variables affect mental well-being. Future research could incorporate positive psychological constructs such as hope, optimism, meaning-making, and posttraumatic growth (Livneh & Martz, 2016; Martz & Livneh, 2016), in the modeling of psychosocial adaptation, which could bring about new findings and perspectives in rehabilitation counseling.
Study Limitations
There are several limitations to the design and implementation of the study, which could affect the validity of the findings. First, the participants were mainly recruited from community-based rehabilitation settings and self-help groups. They tended to be older and had a long history of illness and multiple disabilities or illnesses. Many came from low-income families and were retired, homemakers, or volunteers. In particular, the distribution of the history of illness was skewed, and the majority (67.4%) of participants had an illness history of 5 years or more. Illness coping and identity can evolve over time (Oris et al., 2018). The profiles of the participants could have an impact on the study results. Second, we were unable to include people with more severe disabilities and illnesses who may have communication difficulties (e.g., some people with stroke, brain injuries, or developmental disabilities). Although we did prepare to read the questionnaires to these participants, it was decided that they would not participate in the study.
Third, the COVID-19 pandemic, which started in early 2020, may have affected the study results. During the initial months of the pandemic (February–May 2020), some of the research questionnaires were completed online, while others were completed using hard copies. While the majority of questionnaires (about 70%) were received by mail by January 2020, about 30% of the data were received during a period of lockdown and limited community mobility. The emotional adjustment of participants could be partially affected by their emotional adjustment to the lockdown and social distancing policies imposed during this period. As the pandemic progressed, we discontinued data collection by May 2020 to ensure the completion of the project within the planned time framework. The final sample size of 224 was slightly smaller than the planned size of 240. Nevertheless, when we checked the observed power of key analyses, for example, general linear models, we found that the sample size was adequate for the analysis of the predictors of the RIDI’s adaptive and non-adaptive scales.
Conclusion
Resilience, coping strategies, and sex were the significant predictors of psychosocial adaptation among people with CID in China. Health-related factors (pain and breathing difficulty) are important predictors of non-adaptive emotional reactions but not adaptive reactions. Women experience higher levels of anxiety during psychosocial adaptation although their overall adjustment is better than that of men. The study also used SEM to test a conceptual model that was hypothesized based on the theories of health-related coping and psychosocial adaptation. All the proposed variables, including background variables of social support and health-related factors, contributed significantly to the adjustment process variables of resilience and coping, which in turn affected psychosocial adaptation and mental well-being. The fair model fit of the SEM indicates that some important predictor variables may not have been included. Most of the results on the predictors of psychosocial adaptation resemble those of studies conducted in non-Chinese contexts. Cultural influences did not appear to be a significant factor in predicting psychosocial adaptation among people with CID in China.
Footnotes
Acknowledgements
The authors thank all the self-help groups and their members who participated in this study, including the 1st Step Association, Direction Association for the Handicapped, Hong Kong Epilepsy Association, Hong Kong Neuro-Muscular Disease Association, Hong Kong Parkinson’s Disease Association, and Yin Hong Club. They also thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is funded by the Faculty of Health and Social Sciences, The Hong Kong Polytechnic University (Project Code ZVNB).