
Abstract
Objectives:
The United Kingdom has committed to World Health Organization goals to eliminate hepatitis C virus (HCV) by 2030. Peer-led services (PLS) may enhance health care engagement and treatment outcomes. We compared progression through the HCV care cascade between those tested in a community using PLS (PLS group) with a population tested in drug services (non–PLS group) in England.
Methods:
We extracted data on individuals with HCV-RNA test results from a laboratory surveillance system (2019-2023) and linked them to a national HCV treatment database. We identified individuals tested by the Hepatitis C Trust as having received PLS. We compared differences along the care cascade using the Pearson χ2 test.
Results:
A total of 14 094 individuals in the PLS group (72.9% male; median age, 43 y) and 46 568 individuals in the non–PLS group (70.6% male; median age, 44 y) received a positive HCV-RNA test result. Significantly more individuals from the PLS group than the non–PLS group were linked to treatment (83% vs 51%) and initiated treatment (73% vs 33%; both P < .001). Among those with a treatment outcome, 75% in the PLS group versus 80% in the non–PLS group achieved a sustained virologic response (SVR) (P < .001). Significantly more individuals achieved SVR among those receiving a positive HCV-RNA test result in the PLS group than in the non–PLS group (36% vs 11%; P < .001).
Conclusion:
A key strength in peer-led models lies in linkage to treatment when compared with drug services alone. This finding highlights the importance of ongoing support for peer-led programs helping medically underserved populations living with HCV progress to treatment and achieve elimination.
Keywords
Worldwide, approximately 240 000 deaths are attributed to hepatitis C virus (HCV) each year, with 1 million people acquiring HCV annually. 1 Many countries including the United Kingdom are working toward the World Health Organization (WHO) target to eliminate HCV as a public health concern by 2030, with targets including a 90% reduction in incidence, a 65% reduction in mortality, and treatment coverage of 80%. 2 The United Kingdom has made strides toward meeting these targets since the introduction of direct-acting antivirals, initially through an early access program in 2016 and then more widely starting in 2017, evident in a 57% decrease in HCV prevalence since 2015. 2
Following the introduction of direct-acting antivirals, HCV infection has become curable, and, hence, treatment has become the focus of prevention. In England, from 2015 to 2022, 90 000 people had a positive HCV-RNA test result, and most HCV diagnoses were among people who inject drugs (PWID). 2 To meet WHO elimination targets, evidence-based interventions are necessary to overcome barriers to care for people living with HCV. 3 Low uptake of HCV treatment is a common occurrence in the cascade of care among PWID.4-6 Pathways to HCV elimination include community mobilization, partnership building, and an educational campaign to promote awareness and behavior change.7,8
The involvement of peer-led services (PLS) is recognized as an essential element of HCV treatment support, particularly for medically underserved populations such as PWID. 9 A systematic review of interventions for HCV case finding and linkage to care found that PLS is useful for providing treatment to PWID and people experiencing homelessness but requires careful integration to ensure sufficient removal of organizational barriers to facilitate acceptance of the peer relationship. 10 In London, United Kingdom, a randomized control trial demonstrated that PLS improved engagement with health care services and care pathways among PWID and people experiencing homelessness. 11 Similarly, analyses have demonstrated that across England, treatment areas that have PLS in place see greater treatment initiation and completion than treatment areas that do not have PLS. 12 These findings also mirror studies in Australia and Denmark, where point-of-care testing delivered by peers and PLS into treatment can increase treatment uptake for HCV.13,14 In addition, a recent toolkit designed to increase access to HCV treatment in prisons recommended the involvement of people with lived experience as peers to increase motivation for HCV testing and treatment and to reduce stigma. 15
While it is important to ensure successful progression through the HCV care cascade, there is also a risk of reinfection for those who continue to engage in behaviors that expose a person to HCV. In England, rates of reinfection are highest among people who were currently injecting drugs when initiating treatment and among people who were treated in prison as well as those more recently treated.16,17 Therefore, to prevent reinfection and further risk of disease progression for PWID and people in prison, there is a need to ensure adequate harm reduction information and support during treatment, and people with lived experience may be most suitable to this role.
The objective of this study was to further investigate the role of PLS in supporting people through the HCV care cascade by comparing data on people who received PLS when tested and diagnosed with HCV with data for a similar population of people who accessed drug services and who had no known evidence of receiving PLS.
Methods
Data Systems
We extracted data on testing and diagnosis from the Sentinel Surveillance of Blood Borne Virus (SSBBV) surveillance system. SSBBV began in 2002 18 and collects hepatitis A to E, HIV, and human T-lymphotropic virus testing data from 43 participating laboratories across England and includes demographic characteristics (age, sex, ethnicity) and the service conducting the test. SSBBV has a large coverage of blood-borne virus (BBV) testing conducted in drug services in England (>90%). 18 In addition to laboratories, information on community testing, such as testing from the Hepatitis C Trust (HCT; www.hepctrust.org.uk), is also fed into SSBBV. A unique identifier differentiates people who use a National Health Service (NHS) number, identification number (hospital, sexual health, drug treatment), and/or a combination of name, soundex (phonetic algorithm for indexing names), and date of birth, which is applied across the whole SSBBV dataset (including HCT data).
Information on people who have a positive HCV-RNA test result and are referred for HCV treatment are entered by operational delivery networks (ODNs) into the Arden & GEM clinical system (the National Hepatitis C Patient Registry and Treatment Outcome System). 19 Information on individuals includes demographic, clinical (disease stage, hepatocellular carcinoma, fibroscan result, comorbidities), and risk information (exposure route, injecting drug use status) as well as details on treatment initiation (treatment start date, outcomes). Data are deduplicated and linked to SSBBV using a combination of NHS number, date of birth, and name.
The Peer-Led Program
The HCT provides HCV awareness, education, testing, and peer support to marginalized and excluded populations who are at increased risk of HCV acquisition (PWID, people who have been in prison, people who experience homelessness, people who have migrated from another country). About 120 paid staff and more than 100 peer volunteers with lived experience provide community and peer support in all 24 ODNs that are responsible for HCV treatment in England; they are integrated into hepatitis C care pathways, prisons, and drug-testing services. The program is largely funded through the NHS England HCV elimination program and uses a peer-led approach that involves staff and volunteers who have relevant lived experience including HCV, homelessness, and/or injecting drug use. This support is routinely offered to people diagnosed with HCV, in particular where people have previously faced barriers to accessing health care. HCT peers actively participate in multidisciplinary team meetings, where HCV treatment and therapies are reviewed and approved alongside clinicians. These services are generally provided as per patient needs, usually several meetings during pretreatment and then once a week while on treatment for patients with higher needs or once a month for patients with less need. Peers work with patients referred by drug services, community nursing teams, or emergency department settings when traditional pathways to treatment engagement have been unsuccessful. In addition, they identify patients through intensive outreach efforts, particularly among populations experiencing homelessness.
The peers provide services such as appointment reminders, travel support or reimbursement, medication delivery, and a personal connection throughout the treatment journey, acting as a support mechanism and mentor from testing and diagnosis to treatment completion and sustained virologic response (SVR). This approach takes a holistic view, aiming to reduce the stigma around testing and diagnosis. Discontinuation from the PLS is determined by the patient, and support can continue beyond their HCV treatment, including providing preventative harm-reduction strategies for those who engage in injecting drug use, such as retesting, needle and syringe programs, and naloxone. HCT peers also provide continued support for those with advanced liver disease, such as attending ultrasound appointments.
The Cascade of Care
We extracted data pertaining to individuals tested for HCV-RNA from 2019 through 2023 from SSBBV and linked to treatment data (January 1, 2019, through August 31, 2024) to compare outcomes along the HCV care cascade. People who were tested for HCV-RNA by the HCT were labeled as receiving PLS and were compared with people who were tested in drug treatment services, where people were not known to have received PLS. Those who were tested in drug treatment services but had not been tested by HCT were grouped as no known PLS (non-PLS). Drug services were used as a comparison group because a large proportion of individuals with a positive HCV-RNA test result were PWID. 2 We obtained information on engagement in drug use for those in the PLS group by examining previous testing history in drug services and drug use information at treatment engagement, because all those tested in the non-PLS group were tested in drug services and, therefore, were assumed to be engaging in or had engaged in drug use.
We compared 6 outcomes along the cascade of care between those receiving and not receiving PLS. We also investigated the total movement through the care cascade for those with patient-identifying information (hereinafter, identifiers) and HCV reinfection after successful treatment for HCV. If an individual was not included in the numerator at a given stage, then that individual did not advance to the subsequent stage of the care cascade. Unless otherwise stated (eg, SVR), the denominator used was the numerator of the previous step in the care cascade.
HCV-RNA positive with identifiers
We included individuals who had a positive HCV-RNA test result with identifiers, such as forename, surname, date of birth, or NHS number (health care identifier), from SSBBV from 2019 through 2023. The denominator included those who had a positive HCV-RNA test result.
Linked to treatment
We defined linked to treatment as individuals who had a positive HCV-RNA test result with identifiers in SSBBV from 2019 through 2023 and were linked based on forename, surname, date of birth, or NHS number to the National Hepatitis C Patient Registry and Treatment Outcome System (data until August 2024). Doing so indicates an ODN is aware of a patient in need of treatment and has created a record of that patient.
Initiated treatment
We defined initiated treatment as individuals who had a positive HCV-RNA test result with identifiers in SSBBV from 2019 through 2023 and were linked to the National Hepatitis C Patient Registry and Treatment Outcome System data until 2024 and had a treatment start date.
Treatment outcome
We defined those with a treatment outcome as those who initiated treatment in SSBBV during the study period and had a treatment outcome (SVR, breakthrough, nonresponse, relapse, and lost to follow-up) reported. Treatment outcome is reported by the clinical team, where SVR reflects an RNA negative test result 12 weeks after treatment completion.
Sustained virologic response
We defined SVR as individuals who initiated and completed treatment in SSBBV during the study period and had an SVR reported as their treatment outcome or a negative HCV-RNA test result ≥96 days after treatment start. The denominator excludes people who died before an SVR result could be identified.
Total cascade
We calculated the proportion of people who moved through the cascade of care for PLS and non-PLS groups. The numerator was people who achieved SVR, and the denominator was those who had a positive HCV-RNA test result with sufficient identifiers to link, excluding those who died before treatment could start.
Reinfection
HCV reinfection was defined using 3 previously published criteria. 16 Briefly, an individual was identified as experiencing an HCV reinfection if they had a positive HCV-RNA test result or a subsequent treatment period ≥196 days after initial treatment start, where HCV clearance was evident. We included only those who initiated treatment prior to 2024 in the denominator for reinfection to ensure sufficient time for reinfection to occur.
Statistical Analysis
To understand the differences in the cascade of care between people in the PLS group and non–PLS group, we conducted Pearson χ2 tests using Stata version 18E (StataCorp).
Public Engagement
The PLS program by HCT is designed by people with lived experience of HCV. It is therefore an example of community-led public health practice. The data were then shared with the UK Health Security Agency (UKHSA) for analysis and reporting, and the HCT peer-led program group was involved in the reporting, interpretation, and dissemination of findings.
Ethics
Laboratory testing data are collated and processed by UKHSA as part of national surveillance of HCV. The dataset is covered by the United Kingdom’s government Health Service (Control of Patient Information) Regulation 2002 (regulation 3 and 7), which makes provisions for the recognition, control, and prevention of communicable diseases and other risks to public health. Therefore, ethical approval from participants was not needed as per UKHSA’s Research and Ethics Governance Board, but appropriate Caldicott approval was obtained for linkage between databases.
Results
A total of 60 662 people were tested by either the HCT (PLS) or drug services (non-PLS) group from 2019 through 2023. Among those receiving PLS, 14 094 individuals had a positive HCV-RNA test result, of whom 72.9% (n = 10 273) were male and the median (IQR) age was 43 (37-49) years (Table). In the non–PLS group, 46 568 individuals had a positive HCV-RNA test result, of whom 70.6% (n = 32 870) were male and the median (IQR) age was 44 (38-51) years.
Characteristics of people with hepatitis C virus who received care from peer-led services and non–peer-led services, England, 2019-2023 a
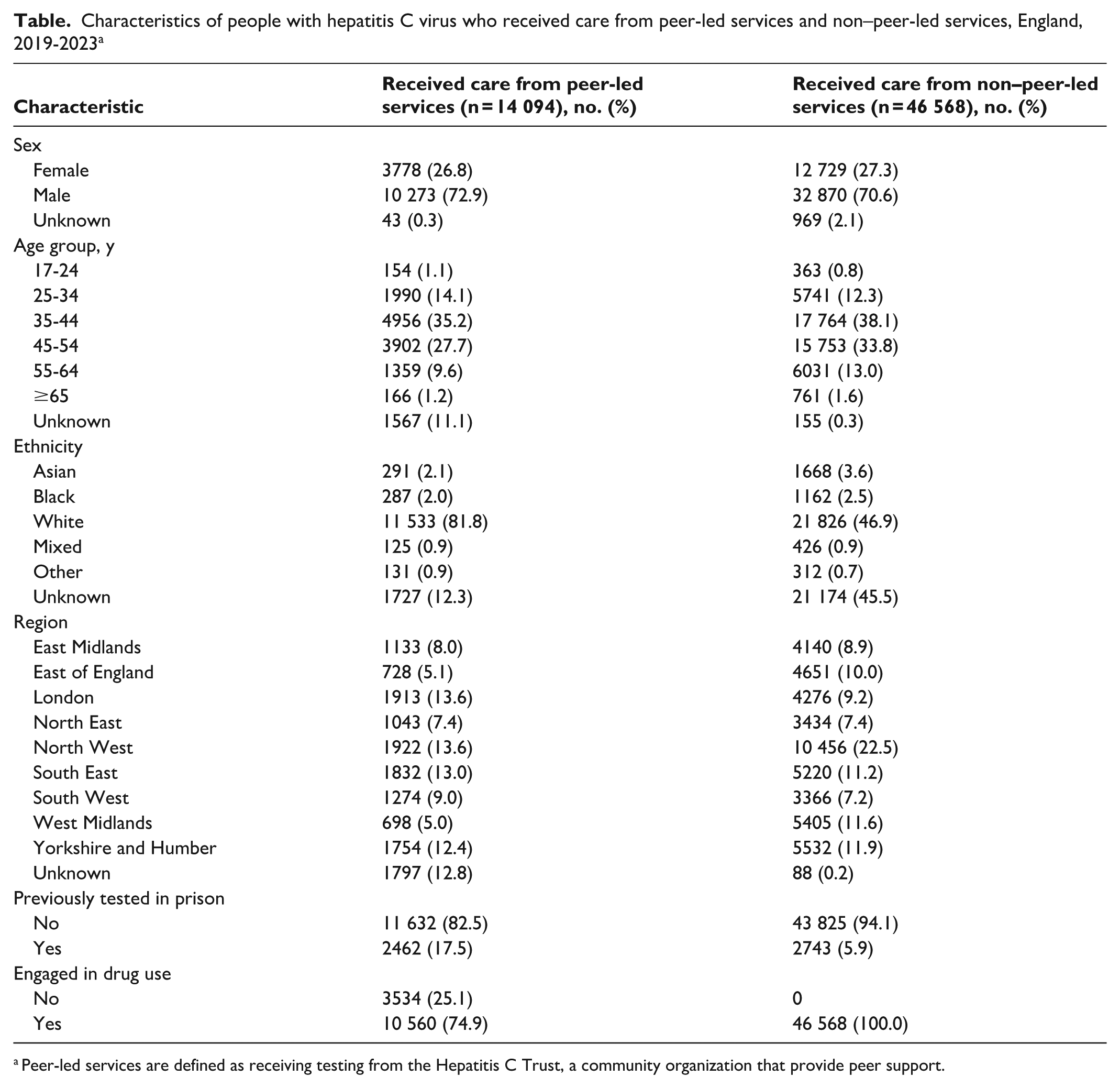
Peer-led services are defined as receiving testing from the Hepatitis C Trust, a community organization that provide peer support.
A higher proportion of the PLS group than the non–PLS group had ethnicity reported (87.7% [n = 12 367] vs 54.5% [n = 25 394]) (Table). Where ethnicity was reported, a high proportion of both groups reported being of White ethnicity (93.3% [11 533 of 12 367] vs 85.9% [21 826 of 25 394]). A higher proportion of people in the PLS group than in the non–PLS group had been previously tested in prison (17.5% [2462 of 14 094] vs 5.9% [2743 of 46 568]).
We found a significantly higher proportion of people who had a positive HCV-RNA test result with identifiers among the PLS group (72.6%; 10 238 of 14 094) compared with the non–PLS group (35.4%; 16 471 of 46 568) (P < .001) (Figure). Among those with sufficient identifiers, the PLS group had a higher proportion of linkage to treatment (83.0%; 8500 of 10 238) than the non–PLS group (51.0%; 8403 of 16 471) (P < .001). Of those who linked to treatment, a higher proportion of people in the PLS group (72.9%; 6199 of 8500) compared with the non–PLS group (33.5%; 2812 of 8403) (P < .001) initiated treatment. Among those who initiated treatment, we found no significant difference in the reporting of an outcome between those in the PLS group (82.3%; 5102 of 6199) and the non–PLS group (83.4%; 2346 of 2812).
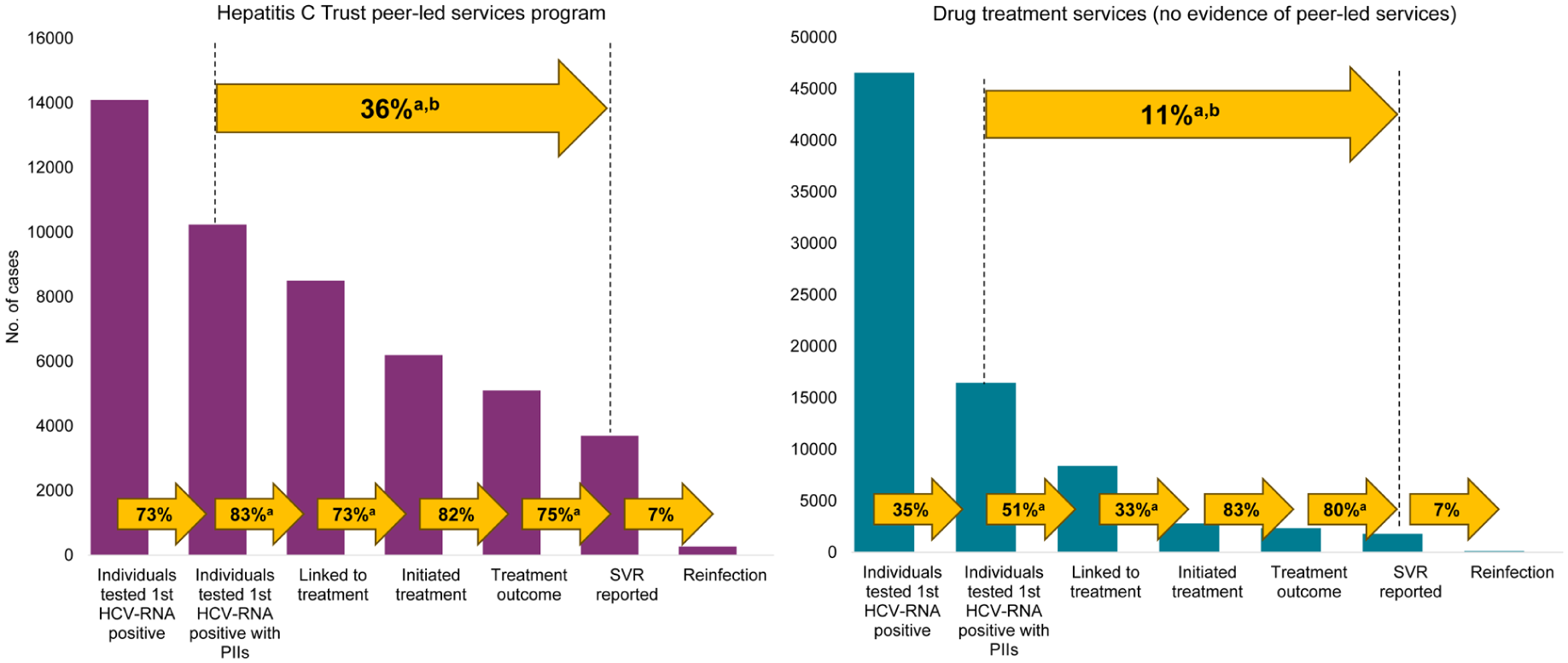
A comparison of the HCV cascade of care between (A) people who received peer-led services (PLS) through the Hepatitis C Trust and (B) those tested in a drug service with no known evidence of PLS, England, 2019-2023. Data exclude people who died before treatment could commence. Data source: Sentinel Surveillance for Blood Borne Viruses, 18 combined with data from the National Hepatitis C Treatment Registry and Reporting System. Abbreviations: HCV, hepatitis C virus; HCV-RNA, hepatitis C virus ribonucleic acid; PII, patient identifying information. Individuals tested first HCV-RNA positive with PIIs, linked to treatment, initiated treatment, and with sustained virologic response (SVR) reported were significant at P < .001.
Among those with a treatment outcome, the PLS group had a slightly lower SVR rate (74.9%; 3698 of 4939) than the non-PLS group (79.8%; 1807 of 2264) (P < .001) (Figure). Among those who received a positive HCV-RNA test result and had sufficient identifiers to link, significantly more people moved through the cascade of care and had an SVR reported in the PLS group (36.1%; 3698 of 10 238) than in the non–PLS group (11.0%; 1807 of 16 471) (P < .001). The proportion experiencing an HCV reinfection captured in surveillance after SVR was similar between the PLS group (7.4%; 272 of 3669) and the non–PLS group (7.3%; 131 of 1798).
Discussion
This study assessed the impact of a peer-led program compared with a non–peer-led approach on the HCV care cascade. Overall, support from peers was associated with better outcomes across the care cascade, from linking individuals to treatment to initiating treatment and progressing through the care cascade to achieving SVR. These findings highlight a key strength of the peer-led model in connecting individuals to treatment. An advantage of peer-led programs is their ability to engage with people at risk of, or diagnosed with, hepatitis C and provide individualized care to those facing complex challenges. Our findings mirror those of previous studies from England11,12 and internationally13,14 that highlighted the role of PLS in increasing people’s engagement in care and completing treatment.
Peers target early engagement, provide education, and help patients attend their appointments. They help bridge the gap between health care professionals and the care population by advocating for individuals and helping them navigate the health care system. Our results show the effectiveness of a peer-led program in supporting patients through the HCV care cascade, resulting in improved outcomes for people living with HCV. We found that the proportion of patients with an SVR reported was significantly lower among the PLS group than the non–PLS group (75% vs 80%). It is important to note that the proportion with an SVR for both groups was lower than what is seen nationally (87%) 2 and lower than the WHO goal of 90% diagnosed and cured. 20 Across the entire care cascade, in the PLS group, 64% of patients with a positive HCV-RNA test result were without an SVR compared with 89% in the non–PLS group. However, the rate of SVR achievement may be lower than what is seen nationally given that those receiving PLS services may have previously disengaged from care and have multiple competing psychosocial needs. In addition, despite the difference of 5 percentage points in SVR achievement between the non–PLS group and the PLS group (75% vs 80%), the dramatically greater success the PLS group had in linkage to treatment (83% vs 51%) resulted in a greater number of people in the PLS group (vs the non–PLS group) who were being treated and cured.
Further research is needed to explore how ongoing PLS can sustain long-term patient engagement and harm-reduction interventions to prevent reinfection and to characterize the techniques of PLS that enable behavior change. The proportion of individuals experiencing HCV reinfection was similar between those receiving and not receiving PLS. Whether someone is currently injecting drugs when initiating treatment or receiving treatment in prison is the biggest predictor of HCV reinfection, 16 which may help explain why we found no significant difference between the 2 groups, because a higher proportion of people who had been tested in prison were in the PLS group. Peer workers also reach PWID who are not engaged with drug treatment services and, therefore, are at an elevated risk of HCV reinfection after treatment. In England, integrating PLS in prisons that provide opt-out testing has been successful, with 97% of those diagnosed being treated in one study. 21 It is, therefore, crucial to identify which clients benefit the most from peer involvement and to understand the broader health and social benefits of this approach.
Limitations
This study had several limitations. First, we could not guarantee that those in the non–PLS group did not receive other forms of peer support or incentives outside the HCT and, therefore, were unknown to the researchers. Second, because of the high proportion of those engaging in or previously engaged in drug use in the sample (100% of non-PLS and 75% of PLS), it was not possible to control for drug use along the care cascade in relation to the PLS group. In addition, those in the PLS group who did not have evidence of drug use may have less engagement in health services and, therefore, fewer opportunities for this information to be included in health records, although these individuals may still be engaging in drug use. Despite these limitations, we found a significant difference in linkage to treatment between the 2 groups, therefore demonstrating the usefulness of the HCT PLS program compared with what people would have received otherwise when tested in drug services.
Conclusion
This study demonstrated the importance of PLS in linking individuals to treatment and aiding people through the cascade of care for HCV. To achieve HCV elimination by 2030, the need for PLS may become even more important because individuals who still need treatment may have multiple health and social care needs. It is also important to further understand the role of peers in preventing HCV reinfection, given the importance of minimizing HCV reinfection to achieve HCV elimination goals, as well as reducing impact on individuals’ physical health.
Footnotes
Acknowledgements
The authors acknowledge the work of the Hepatitis C Trust peer-led workers who made this analysis project possible and provided the data for analyses.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.