
Abstract
In the United States, molecular HIV epidemiology (MHE) is a key part of the National HIV/AIDS Strategy, which incorporates the evaluation of HIV genetic sequences for cluster detection and response. Data collection for MHE occurs without any requirement for formal consent from patients, which has sparked ethical concerns among community members, ethicists, and advocates. We conducted a rapid review of the current literature on informed consent and MHE to understand the key concerns and recommendations. We searched 4 academic databases and included articles that examined the issue of informed consent in MHE practices. We screened a total of 119 articles and selected 30 articles for inclusion. From these, we extracted data pertaining to concerns and recommendations related to informed consent in MHE, including MHE in the context of both research and surveillance. Our findings revealed 2 main categories of concerns: (1) challenges in obtaining valid informed consent and (2) concerns related to the current lack of consent such as risks of data misuse, privacy violations, and potential stigma. We identified 3 main categories of recommendations: establishing stronger data governance, developing ethical consent practices, and increasing community engagement. A key theme identified was an unresolved contestation about the ethics of using MHE without consent and whether the potential public health benefits of MHE justify concerns about autonomy, privacy, and potential harm. Future directions include the need for empirical research to evaluate the risks and benefits of MHE and the development of practices for meaningful community engagement to ensure ethical and context-sensitive approaches.
Molecular HIV epidemiology (MHE) involves studying HIV transmission patterns within and between communities. 1 As part of clinical care in the United States, genetic testing of HIV is routinely used to detect antiretroviral drug resistance and guide selection of appropriate antiretroviral therapy. 1 Using the genetic sequences derived from drug resistance testing, MHE can provide information about the genetic characteristics and evolutionary history of HIV when sequences are compared across populations. 2 MHE can also be used to track outbreaks through cluster detection and response. Cluster detection and response refers to the identification of HIV and response to communities affected by rapid HIV transmissions (clusters) defined by shared social or sexual networks or geographic location to address gaps in prevention and care. 3 As part of the national strategy to end the HIV epidemic, MHE is used to identify new HIV clusters, enabling rapid response. 4
Like other routinely reported clinical data (eg, CD4 lymphocyte counts), sequences are not explicitly disclosed as being used for public health surveillance.5,6 MHE is generally performed using sequences collected during routine HIV care and reported to state public health systems. Data collection typically occurs without the tested person’s knowledge or consent that the data could also be used for MHE, which is comparable to most public health reuse of clinical data. For example, in the United States, health care providers are mandated to report newly diagnosed cases of tuberculosis to health departments without written authorization from the patient because tuberculosis is considered a substantial threat to public health. 7 However, in the case of MHE, this lack of informed consent has sparked concerns among some community members, ethicists, and advocates.1,6 Unlike other surveillance measures, HIV sequences can be linked across individuals to reconstruct clusters of related infections, which may be misinterpreted as evidence of transmission direction or responsibility, with potential legal and social consequences.
In the context of HIV, these risks heighten ethical sensitivities related to autonomy and privacy. 1 Moreover, the scientific application of MHE is unsettled, with uncertainty about how best to interpret and translate genetic sequence data into effective and acceptable interventions. 8 People living with HIV (PLWH), advocates, and community-based organizations have emphasized that awareness of MHE is limited and that its national rollout occurred with minimal or largely passive community engagement. 1 Together, these factors make MHE ethically distinct and help explain why concerns about consent surface more sharply here than for other forms of routine public health reporting. Informed consent provides an opportunity for individuals to authorize researchers or practitioners to conduct an activity based on their understanding of what the activity entails 9 and is “more than a signature on a piece of paper” 10 because it protect the rights and autonomy of individuals. Therefore, the lack of informed consent in MHE has garnered greater attention in the bioethics literature than have other public health practices that do not obtain consent.
Despite concerns about the lack of informed consent for MHE, few studies have synthesized perspectives on the issue. To address this gap, we conducted a rapid review of the current literature on ethical considerations in informed consent for MHE. We aimed to identify how the topic of consent for MHE has been addressed by public health researchers, community members, clinicians, and other groups affected by HIV. The purpose of the review was to understand the key concerns and recommendations that have emerged from the literature on consent for MHE practices.
Methods
We conducted a rapid review of published academic literature on the topic of informed consent for MHE in public health research and surveillance. A rapid review is a streamlined and accelerated form of conducting reviews wherein certain components of a systematic review are simplified to shorten the process.11,12
Inclusion and Exclusion Criteria
Inclusion criteria were limited to original studies or conference proceedings that addressed the issue of consent in MHE and were published as articles in academic journals. We also included reviews, editorials/commentaries, policy briefs, and empirical and conceptual studies addressing consent in MHE. We excluded MHE studies that did not address the topic of consent, study protocols, and studies that were not published in the English language. Publication dates ranged from 2009 through 2023.
The authors’ subject knowledge and Medical Subject Headings (MeSH) terms guided the development of search terms that we used to identify articles for this review. A librarian at the University of North Carolina at Chapel Hill assisted in selecting appropriate MeSH terms. The final search string used was: (“molecular HIV epidemiology”[tiab:~1] OR “molecular HIV surveillance” OR “HIV surveillance”) AND (“HIV”) AND (“consent” OR “informed consent” OR “consent waiver”). We tailored the search string for each database search. We searched 4 databases: PubMed, EBSCOhost, Global Health, and Global Health Archive. We also searched the references of articles selected for inclusion to identify additional articles for potential inclusion. We used Covidence (Veritas Health Innovation Ltd), a systematic review software, to review the articles.
Data Extraction and Analysis
After identifying articles through database searches, 2 reviewers (U.O. and S.R.) independently screened titles and abstracts for inclusion. They then reviewed the full texts using predefined criteria and recorded reasons for exclusion—most commonly, a lack of focus on consent. The reviewers resolved discrepancies collaboratively. Final selections proceeded to the next step of data extraction, which included study type, publication year, location, authors, population, and whether MHE was discussed in the context of research and surveillance (Table 1). We also extracted concerns and recommendations related to informed consent in MHE.
Data extraction from key contributing articles included in a rapid review of literature (N = 30) published from 2009 through 2023 on informed consent in molecular HIV epidemiology
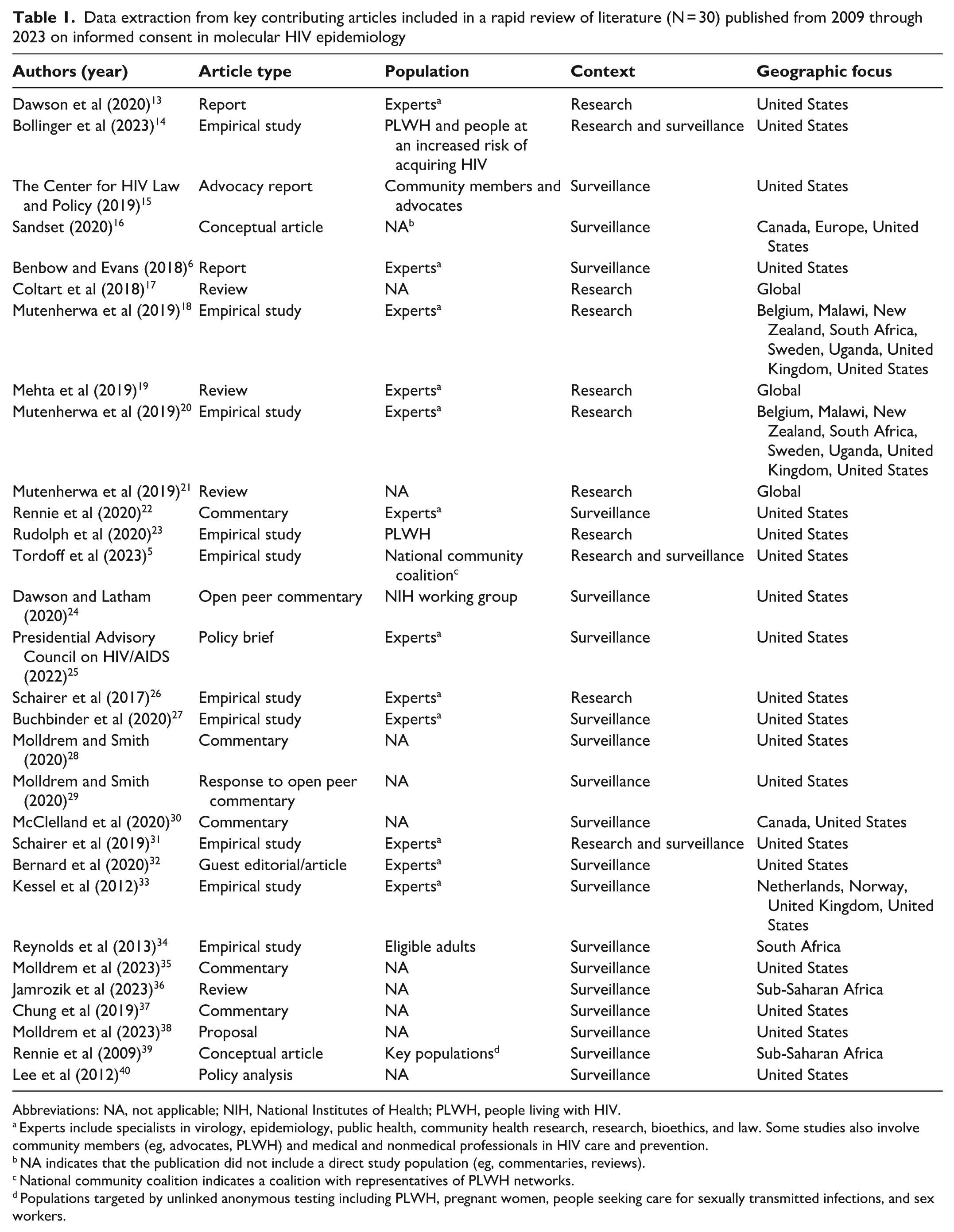
Abbreviations: NA, not applicable; NIH, National Institutes of Health; PLWH, people living with HIV.
Experts include specialists in virology, epidemiology, public health, community health research, research, bioethics, and law. Some studies also involve community members (eg, advocates, PLWH) and medical and nonmedical professionals in HIV care and prevention.
NA indicates that the publication did not include a direct study population (eg, commentaries, reviews).
National community coalition indicates a coalition with representatives of PLWH networks.
Populations targeted by unlinked anonymous testing including PLWH, pregnant women, people seeking care for sexually transmitted infections, and sex workers.
Categorization of Articles
We categorized the articles based on whether they discussed MHE in the context of public health surveillance, research, or both. Those categorized as discussing MHE in the context of research examined MHE as a scientific tool to study HIV transmission dynamics and clusters. These studies were intended for research purposes to inform broader scientific understanding (eg, estimate changes in HIV transmission) and to highlight the impact of interventions and policies on various populations. 41 Articles categorized as discussing MHE in the context of surveillance—the continuous, systematic collection, analysis, and interpretation of health-related data seeks to inform the public health response 42 —focused on using MHE to monitor and guide public health response. We categorized articles that addressed both concepts or had overlap between research and surveillance applications as both research and surveillance.
Ethical Considerations
This study was a rapid review of existing published literature and did not involve direct interaction with human participants or collection of human data. Therefore, ethical approval was not required.
Results
The database search yielded 95 articles, and other sources identified 24 articles, for a total of 119 articles. We exported the articles to Covidence to screen the titles and abstracts and assess them for eligibility, which resulted in removing 1 duplicate article and excluding 66 articles. Upon screening the full texts of the remaining 52 articles, we excluded 22: 18 lacked consent-related content, 2 were not MHE specific, and 2 were duplicates. We included a total of 30 articles in the final review for data extraction and synthesis (Figure). We also present the results of the review by summarizing the major concerns (Table 2) and key recommendations (Table 3) surrounding informed consent for MHE.
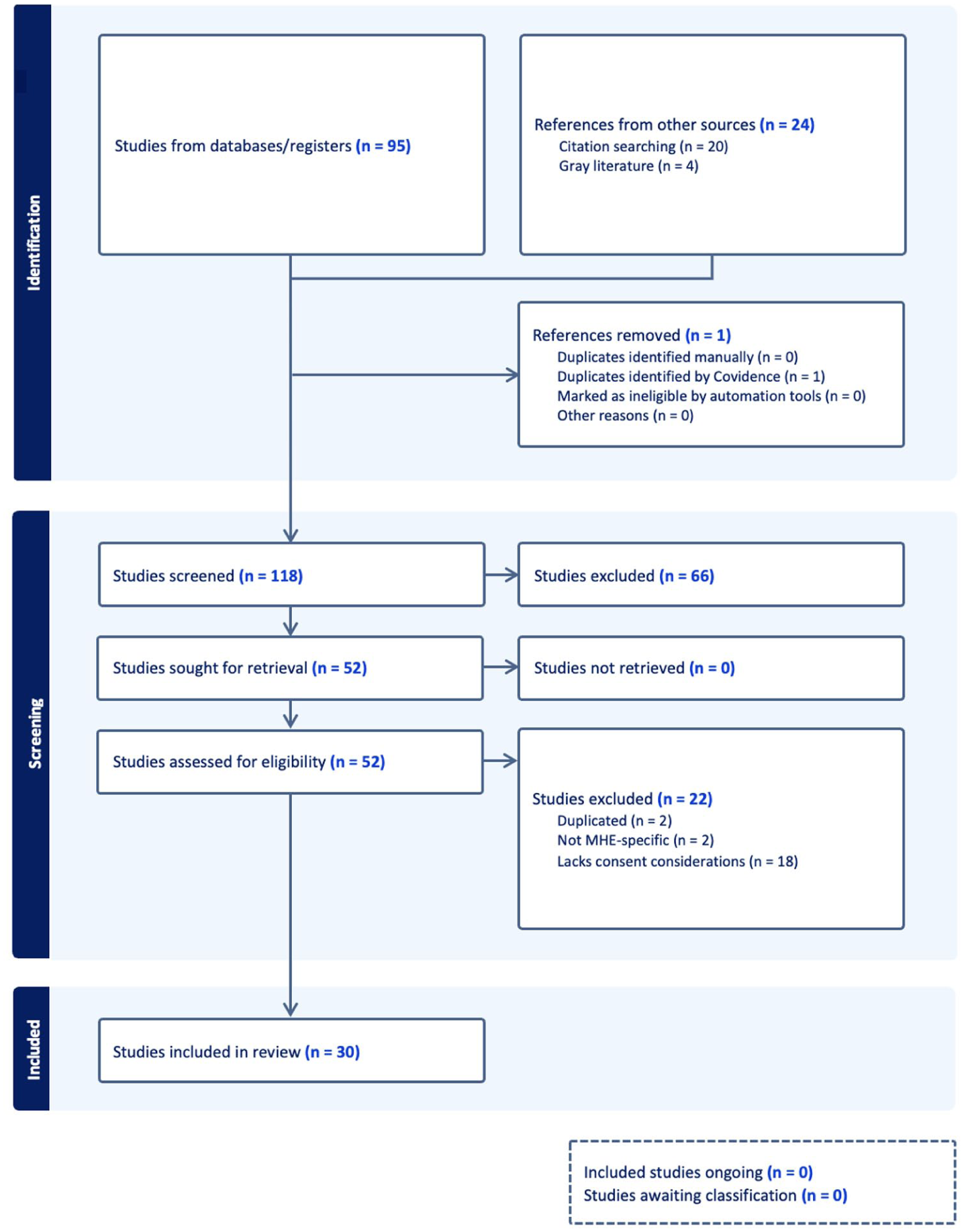
PRISMA flow chart of study selection for the rapid review of informed consent in molecular HIV epidemiology. Abbreviations: MHE, molecular HIV epidemiology; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
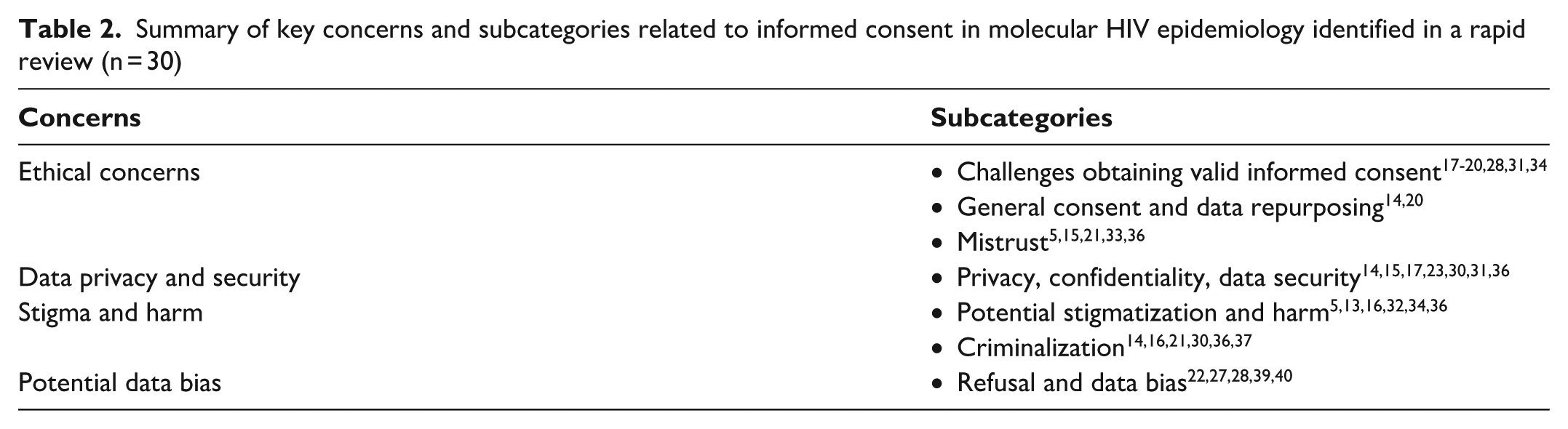
Summary of key concerns and subcategories related to informed consent in molecular HIV epidemiology identified in a rapid review (n = 30)
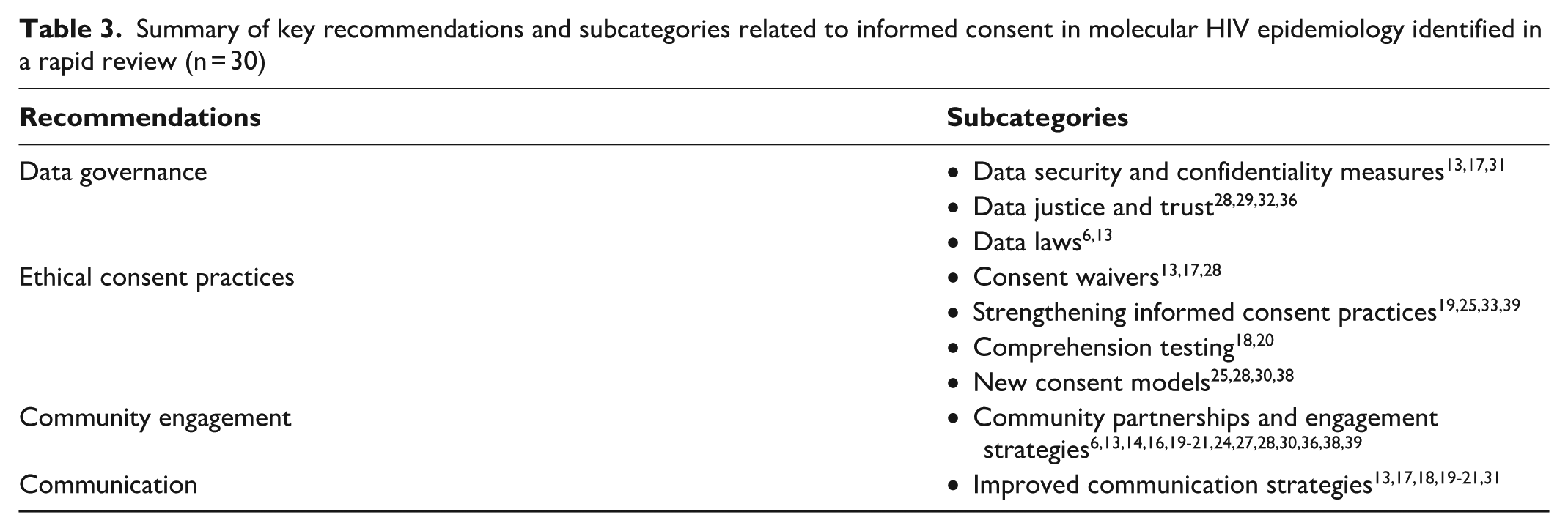
Summary of key recommendations and subcategories related to informed consent in molecular HIV epidemiology identified in a rapid review (n = 30)
Study Details
Among the 30 included articles, 10 were empirical studies,5,14,18,20,23,26,27,31,33,34 7 were commentaries (including a response to a commentary),22,24,28,29,30,35,37 and 3 were reports.6,13,15 The remaining articles consisted of policy briefs, reviews, and conceptual articles. Some studies involved community members (eg, advocates, PLWH) and medical and nonmedical professionals in HIV care and prevention.5,6,13-15,18-20,22,25-27,31-33,39 Commentaries, policy briefs, and conceptual articles focused primarily on issues surrounding MHE in the context of surveillance. Geographically, most (n = 19) articles were focused on the United States. Some (n = 5) articles focused on the United States and other countries. Eight articles examined global or multicountry contexts, spanning regions across Africa, Europe, and North America. Of the 30 articles, 19 examined the topic of MHE consent in the context of surveillance, 8 in the context of research, and 3 in the contexts of both research and surveillance.
Concerns Identified
We extracted and synthesized a summary of the ethical concerns related to consent for MHE. Two important challenges emerged from the literature. First, the articles frequently discussed the challenge of obtaining valid informed consent. Most studies found that the complexity of phylogenetic concepts and difficulty in explaining them, sometimes in vernacular languages, often impeded true informed consent—defined as consent given with a full understanding of the conditions, risks, and benefits associated with what one is consenting to do.18,20,28 Articles also highlighted that sometimes even researchers and clinicians lacked sufficient understanding of MHE concepts and their risks and benefits, further complicating the comprehension process necessary for valid consent.18,20,26 For example, some articles described a disconnection between patients’ beliefs of their understanding of the request and physicians’ belief in their capability to explain the request, both of which could be subjective. 43 Another concern was that the collection of MHE data could pose risks to privacy and autonomy, including situations in which legally vulnerable populations (eg, incarcerated people with constrained ability to refuse participation) may be unable to provide valid consent. In addition, MHE practices may disproportionately affect groups marginalized through criminalization or heightened surveillance and generate downstream social harms such as stigma.21,44,45 Another concern was that providing a mechanism to obtain informed consent for MHE would give way to refusals to participate. 22 This emerged in the context of informed consent for MHE as a public health practice, in which refusals could lead to the collection of biased data and inaccurate epidemiological mapping by capturing the information of only willing participants. 22
The second challenge raised in the literature was related to the overall lack of informed consent. These concerns focused on the lack of informed consent and resulting lack of explanation to participants about the potential risks associated with the collection of MHE data. Potential risks include the misuse of data, particularly when samples collected for clinical purposes are later repurposed for surveillance without explicit consent. 18
The literature also identified concerns related to violations of privacy due to the nature of HIV sequences, which can make individuals vulnerable when linked to transmission clusters. Issues related to data breaches and misuse of MHE data are particularly salient in contexts in which populations subject to legal constraints, such as undocumented migrants, may face deportation, imprisonment, or stigmatization if identified through cluster analyses. 17 Without informed consent, individuals and communities may also be unaware of how their data could be used in ways that carry social risk, such as the potential for stigmatization or harm.5,13,14,16,32,36 These risks are heightened in contexts in which HIV is criminalized. Although the directionality of transmission cannot be established with certainty through phylogenetic analysis, the absence of informed consent and disclosure about data use contribute to fears of criminalization.15,21,30-32
Recommendations Identified
Our review revealed 3 main categories of recommendations in the literature to address ethical concerns related to consent for MHE: (1) establishing stronger data governance, (2) developing ethical consent practices, and (3) increasing community engagement.
Establishing stronger data governance
Data governance refers to data approval processes, access laws, and other considerations that guide data use. 46 Recommendations in this category focused on enhancing data security and confidentiality, data justice and trust, and data laws.13,28 Specific strategies included implementing data use agreements for HIV sequence data sharing, particularly in research,13,17 and strict security measures to prevent the unauthorized use of data. 17 For example, Dawson et al 13 called for empirical research to assess the risks of data breaches and reidentification and the development of effective deidentification methods and data security measures. They also recommended evaluating data use agreements to determine how well they prevent the unauthorized use or secondary transfer of HIV sequence data. 13 Coltart et al 17 called for governance plans that address safety, confidentiality, and the unauthorized use of phylogenetic data. In addition, Molldrem and Smith 28 recommended a broader paradigm shift toward HIV data justice, in which engagement with PLWH and affected communities, legal reform, and ethical frameworks work together to ensure that data governance respects individual rights and community trust.
Developing ethical consent practices
The second category of recommendations focused on establishing or improving ethical informed consent. Strategies included using consent waivers, enhancing participant understanding, and developing new consent models that balance ethical considerations with public health needs.13,25,30 Others emphasized testing comprehension to ensure valid consent is obtained, overlapping with calls for improved communication via community engagement.17,20 Molldrem and Smith 28 recommended context-specific consent practices tailored to sociocultural and economic realities. Additional recommendations included enhancing transparency related to data collection, its purpose, and the potential consequences of MHE data use; general notification of ongoing surveillance; and more research to define MHE risks and benefits.20,24,27,33
Increasing community engagement
The third category of recommendations pertained to community engagement to advance the public’s understanding of surveillance efforts in lieu of specific informed consent. Suggested strategies included tailoring communication and dissemination strategies to ensure accessibility, such as designing communication materials that avoid technical terms, especially for complex concepts such as HIV phylogenetics.13,17 Community engagement was also considered key to strengthening informed consent by fostering trust, increasing awareness, and supporting context-specific approaches to consent.17,19,20,24 Collaborative partnerships with community members could help with the development of consent protocols that address local concerns and increase participant buy-in, thereby protecting trust in public health. 18 The literature further highlighted the use of empirical studies to engage communities and build informed consent frameworks that reinforce trust and ethical data practices.16,21,36
Discussion
We conducted a rapid review of the published literature on informed consent in MHE to determine how the issue of informed consent, or lack thereof, has been addressed in both research and surveillance. We identified several key themes in the ethical concerns and recommendations presented in the literature. Broadly, these themes are centered on whether informed consent should be obtained and, if so, the best approach for obtaining it. The necessity of informed consent in MHE is a contentious ethical issue, reflecting broader tensions between individual rights and public health priorities. Our findings revealed variation in perspectives, highlighting the challenges associated with achieving consensus.
A key theme identified in the literature was an unresolved contestation over whether the potential public health benefits of MHE justify compromising individual autonomy and privacy. Some public health practitioners and researchers prioritized the rapid identification of transmission clusters as a public good, while others emphasized that bypassing consent undermines trust and exposes populations subject to stigma, criminalization, or other social harms to disproportionate risk.30,37,45 This contestation underscores why discussions of governance are essential. Rather than abstract calls for governance, our synthesis suggests concrete measures, such as independent data access committees, clear data use agreements restricting repurposing, and community advisory boards, to operationalize accountability. These mechanisms could help address concerns about misuse while maintaining the public health utility of MHE. Importantly, this contestation reflects the broader debate about whether public health benefit can justify compromising autonomy. 44 These ethical tensions have real consequences for groups subject to stigma or criminalization, such as PLWH, and for those whose access to health services may be constrained by incarceration. Recognizing this contestation and making it a central focus of governance and engagement efforts is critical to the future of MHE.
Even if informed consent is deemed necessary for MHE, our findings show substantial challenges related to ensuring that consent is truly informed, with recommendations for improving comprehension, communication, and trust as central to establishing informed consent. Without adequate understanding, obtaining truly informed consent often presents a challenge. This challenge raises a call for standardizing an approach to ensuring that people understand the risks, benefits, and overall scope of MHE. Some articles addressed the issue of disclosure and understanding and described how it goes beyond participants’ understanding of MHE concepts: it also relies on researchers’ knowledge levels and their ability to explain concepts to participants and community members.20,21 For example, Schairer et al 26 found that both lay and professional individuals struggled to grasp the nuanced risks and implications of MHE, which calls into question the veracity of informed consent in this process. Our findings suggest that challenges related to informed consent in MHE are not only logistical but also epistemic, shaped by gaps in understanding on both sides of the consent encounter. In other words, consent risks becoming symbolic if neither participants nor researchers can fully articulate the implications of phylogenetic analyses.
Beyond individual consent, meaningful community engagement also emerged as a crucial but underdeveloped response to the challenges identified. 1 Engagement must go beyond passive consultation and must involve communities in shaping how MHE data are used, governed, and explained. Specifically, community engagement can help address comprehension gaps by developing plain language educational materials in collaboration with community advocates, mitigating mistrust through advisory boards that include disproportionately affected groups, and reducing fears of misuse by ensuring transparency related to secondary data use. 1 However, community engagement is not a substitute for informed consent; it is a complementary mechanism that creates space for dialogue about acceptable data use, acknowledges the concerns around surveillance, and helps generate forms of collective legitimacy that individual consent alone cannot achieve.
Collectively, our findings suggest that any consent processes for MHE, if considered appropriate, must be ethically robust and responsive to persistent communication challenges and community concerns. As MHE continues to expand in scope and use, it is essential to develop context-sensitive and transparent approaches to obtaining consent and raising community awareness of MHE to ensure that public health benefits do not come at the expense of individual rights or public trust.
Limitations
This review had 2 limitations. First, it focused primarily on informed consent in the context of MHE. Thus, while several of the articles included in this review highlighted other concerns, we focused primarily on the issues related to informed consent, possibly limiting the generalizability of findings to other ethical aspects of MHE. Second, the articles included in this review were primarily focused on the United States, which may not fully capture perspectives from other regions, particularly in low- and middle-income countries.
Future Directions and Implications
MHE is an important tool in both research and public health. Recognizing the ethical concerns related to its use without informed consent and fostering dialogue on how to address these concerns can help researchers and public health professionals navigate the ethical landscape of MHE practice and use. Building on the synthesis of this review, we recommend key steps to address the ethical complexities of MHE. First, more empirical research is needed to assess the risks and benefits of MHE, particularly as they relate to informed consent. Such research is critical for evaluating whether and how individuals can meaningfully consent to MHE. It should also aim to show how MHE can balance public health surveillance needs with the protection of individual rights. Second, meaningful community engagement is crucial to ensure that MHE practices align with local values and are context sensitive. Finally, integrating these ethical considerations and recommendations into policy frameworks and developing context-specific guidelines could play a crucial role in balancing the goals of MHE and public health.
Footnotes
Acknowledgements
The authors acknowledge the support of the Health Sciences Library at the University of North Carolina at Chapel Hill in developing the literature search strategy for this review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support for the research, authorship, and/or publication of this article from the National Institute of Allergy and Infectious Diseases, National Institutes of Health (grant no. R01AI135970). The content is solely the responsibility of the authors and does not necessarily represent the views of the National Institutes of Health.