
Abstract
Objective:
Fluoride varnish is a prevention measure for dental caries among children, but few studies have assessed its use in medical settings. This study aimed to determine the period-specific and cumulative prevalence of the receipt of fluoride varnish application among children in the medical setting and associated factors.
Methods:
A parent study enrolled 1326 primary caregiver/child dyads in Indiana, Iowa, and North Carolina; conducted 6 child dental examinations with primary caregiver questionnaires; and administered intermediate questionnaires every 4 months during 2013-2022. Responses were combined from 2- or 4-month time periods to determine the 1.5-year cumulative rates for children aged 1 to 9.5 years. Researchers conducted bivariate and multivariable logistic regression analyses to assess factors associated with the receipt of fluoride varnish application only from age 1 to 2.5 years.
Results:
The 18-month cumulative prevalence of the receipt of fluoride varnish application in the medical setting from the child’s age of 1 to 2.5 years was 20.4%, and the prevalence decreased to 12.9%, 6.4%, and 1.9% among children aged 2.5 to 4 years, 6.5 to 8 years, and 8 to 9.5 years, respectively. The following factors were significantly positively associated with fluoride varnish application in the medical setting: Medicaid insured, low annual household income, Duke University study site, child’s frequent consumption of sugary beverages, child enrolled in other public assistance programs, and child’s infrequent dentist visits.
Conclusions:
The prevalence of fluoride varnish application in the medical setting is low. Factors associated with the receipt of fluoride varnish can be targeted to increase caries prevention through the expanded use of fluoride varnish application in the medical setting.
Keywords
Dental caries is the most common chronic childhood disease in the United States, reducing children’s quality of life by causing pain, difficulty eating, trouble sleeping, decreased self-esteem, dissatisfaction with appearance, and/or missed school days.1-3 The 2015-2016 rates of caries prevalence, including untreated cavities, fillings, and/or teeth missing due to caries, were 21% and 51% among children aged 2 to 5 years and 6 to 11 years, respectively, in the United States. 4 Although this situation is unfortunate, fluoride varnish applications offer an effective preventive strategy for caries.5,6 A systematic review of research trials on fluoride varnish demonstrated a mean reduction of 43% in decayed, missing, and filled surfaces of permanent teeth among adolescents and 37% in decayed, missing, and filled surfaces of primary teeth among young children. 7 Fluoride varnish application in the United States must be provided by a dental or medical health care provider.
The Centers for Disease Control and Prevention, US Preventive Services Task Force (USPSTF), American Academy of Pediatrics, and American Academy of Pediatric Dentistry recognize the benefits of fluoride varnish application in preventing cavities and recommend that dental and medical health care providers apply it semi-annually.8–12 Children often do not see a dentist until after the recommended initial visit at age 1 year. 13 Well-child examinations are routine in physician offices, and it is recommended that children see medical providers at least twice a year until age 4 years. 9 In 2021, the USPSTF reaffirmed and modified the 2014 level B recommendation that children receive fluoride varnish applications from medical providers until age 5 years, revised from the original recommendation that went until age 6 years.10,14 The Patient Protection and Affordable Care Act allows for medical health care providers to apply fluoride varnish and receive health insurance reimbursement based on the USPSTF recommendation.15,16
Few studies on the prevalence of fluoride varnish application in medical settings have been published, and data collection methods differ substantially among these studies, contributing to varied prevalence rates.17–21 A 2009-2019 retrospective study found the lowest prevalence rate of medical fluoride varnish applications (0.04%) in family medicine and pediatric clinics at an academic tertiary care center. 17 A cross-sectional study in South Carolina, with data from 2008-2013, reported a 1.6% prevalence rate in medical settings, with higher rates among Black (vs White) children and children aged 1 to 2 years. 18 From 2016 to 2018, private health insurance data from Connecticut, Maine, New Hampshire, and Rhode Island showed a 4.8% prevalence of receipt of medical fluoride varnish, with lower rates as children aged. 19 A prospective longitudinal cohort study of primary caregivers’ reporting of children’s fluoride varnish application from birth to age 2.5 years showed a combined 12.0% prevalence of receipt of fluoride varnish in dental and medical settings, with higher rates among Black (vs White), non-Hispanic (vs White), and Medicaid-insured (vs non–Medicaid-insured) children. 20 A 2015 quality improvement initiative in federally qualified health centers in Colorado showed a 22.9% prevalence of fluoride varnish application in medical settings in children aged 3 to 4 years during a 1-year period. 21
Research evaluating longitudinal data to determine the cumulative prevalence of receipt of fluoride varnish in the medical setting and associated demographic, child, and caregiver factors is lacking. The objectives of this study were to determine (1) the period-specific prevalence of receipt of fluoride varnish application in the medical setting among study children aged 1 to 9.5 years during 20 individual 2- to 4-month periods, (2) the cumulative prevalence of medical fluoride varnish application from age 1 to 9.5 years during four 18-month periods, and (3) the factors associated with the cumulative prevalence of fluoride varnish application in the medical setting from age 1 to 2.5 years.
Methods
Data were from the parent longitudinal prospective cohort study conducted from 2012 through 2022 to develop a caries risk assessment tool for use by medical providers in medical offices, combining some of the data from the Fontana et al 20 study with new data. Recruitment and main findings are described elsewhere.22,23 The parent study was directed from the University of Michigan, with recruitment and data collection at Duke University, Indiana University, and the University of Iowa. Each university was chosen because it had a primary care practice–based research network. Parent/infant dyads were recruited through diverse medical and dental offices, Special Supplemental Nutrition Program for Women, Infants, and Children clinics, neighborhood centers, and mass email campaigns. The Duke University and Indiana University sites were urban practices serving racially and socioeconomically diverse populations, while the University of Iowa site predominantly serves White urban and rural populations. After each institution obtained institutional review board approval, 1326 primary caregiver/child dyads were enrolled when the children were aged approximately 1 year in 2012-2013. When children were aged 1, 2.5, 4, 6.5, 8, and 9.5 years, primary caregivers completed 52-item questionnaires while children received oral examinations. At each examination and every 4 months afterward, primary caregivers completed 5-item intermediate follow-up questionnaires and were compensated. The 52-item questionnaire included questions about children’s tooth conditions, oral hygiene care, dietary intake, consistency of dental and medical visits, dental and health care insurance, race and ethnicity, feeding behaviors, and birthing method, and primary caregivers’ oral hygiene care, dietary intake, dental and medical insurance, and demographic characteristics as well as the parents’ perceptions of their care for their children’s dental and medical needs. Twenty of these 52 items were chosen based on the scientific literature and biological and behavioral plausibility prior to analysis related to the receipt of medical fluoride varnish after children were aged 1 through 2.5 years.
The series of intermediate follow-up 5-item questionnaires was administered via telephone, email, or letter every 4 months as well as during dental examination visits at the child’s age of 2.5, 4, 6.5, 8, and 9.5 years. Questions addressed primary caregivers’ contact information, whether the child saw a dentist, and follow-up about fluoride varnish application in the dental setting. The main outcome variable was based on the final question, which asked, “Was any fluoride varnish applied during a medical (ie, nondentist) visit since the last intermediate contact or study visit?” Answer choices were yes, no, or unknown.
Statistical Analysis
The “yes” responses were used to determine each of the 20 time period–specific prevalence rates of fluoride varnish (eTable 1 in Supplemental Material). The number of “yes” responses for each possible response count (1-5 responses) was converted to a percentage for each of the 18-month cumulative time periods by dividing the number of “yes” responses by the number of responses with a valid answer (“yes” or “no”; unknowns excluded). These percentages were summed to calculate a dichotomous outcome of “no fluoride varnish application” versus “some fluoride varnish application.” The “some fluoride varnish application” percentage ranged from 20% to 100% for time periods 1 to 4.
Time period 1 included responses from the 5-item follow-up questionnaires at 4 months after the baseline visit, 3 subsequent questionnaires approximately every 4 months, and the second dental visit at age 2.5 years (Figure). Time period 2 included responses every 4 months after the child’s age of 2.5 years until the third dental visit at child’s age of 4 years. Time period 3 included responses every 4 months after the child’s age of 6.5 years until the fifth dental visit at child’s age of 8 years. Time period 4 included responses every 4 months after the child’s age of 8 years until the sixth dental visit at child’s age of 9.5 years.
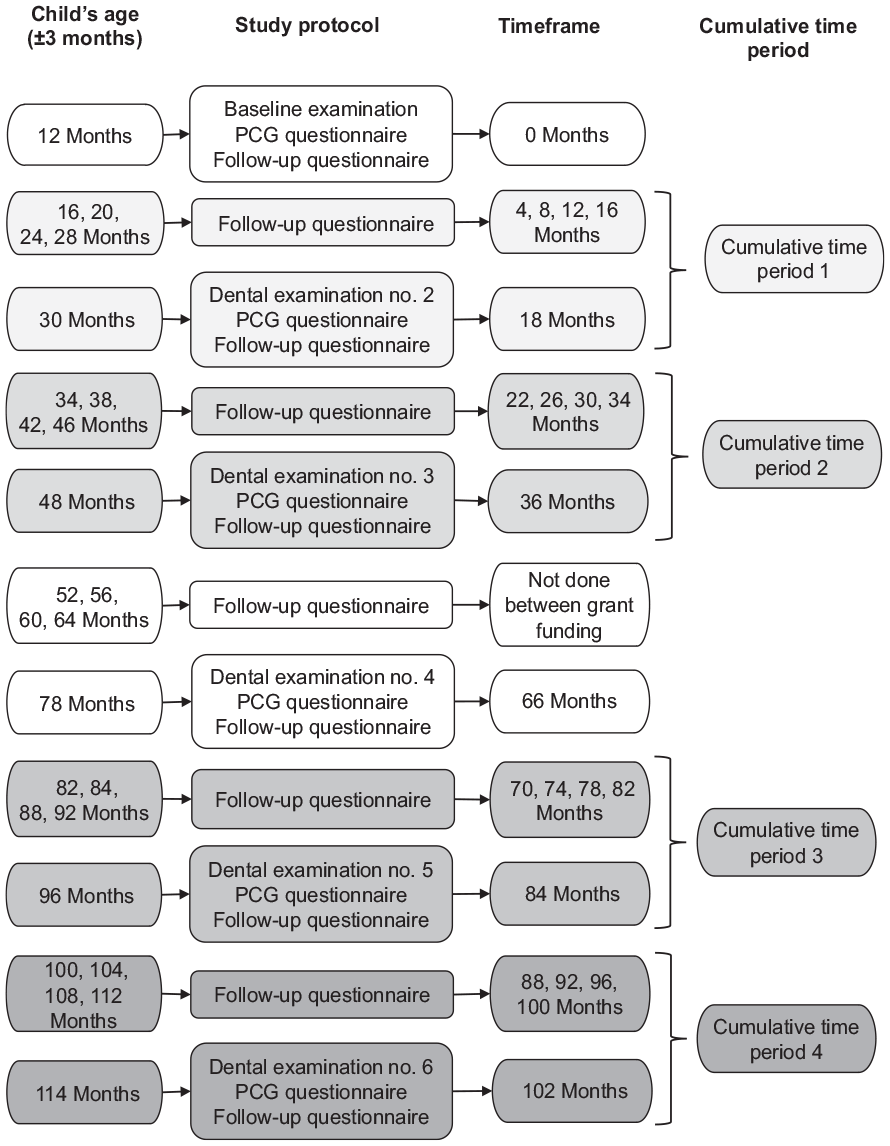
Child’s age, study protocol, study time frame, and cumulative time periods for a study on the receipt of fluoride varnish application among children in the medical setting, Indiana, Iowa, and North Carolina, 2013-2022. Abbreviation: PCG, parent/caregiver.
Descriptive analyses included response rates, time period–specific and cumulative prevalence of medical setting fluoride varnish application, and child and primary caregiver factors at the study’s second dental visit. Bivariate and multivariable logistic regressions evaluated the associations of the 20 demographic, dental experience, oral hygiene care, dietary, nondietary behavioral, and other miscellaneous factors from the second dental visit 52-item questionnaire completed at children’s age of 2.5 years with the cumulative prevalence of receipt of medical fluoride varnish during time period 1. The researchers completed bivariate logistic regressions and used the Wald χ2 test to determine significance, with significance set at P ≤ .05. An overall P value indicates whether the predictor variable as a whole is significant, and the P value indicates whether specific categories are significantly different from the reference category. The researchers used variable selection with backward elimination using the Akaike information criterion (AIC) for model comparison to determine the most parsimonious model. 24 The model with the lowest AIC score and all models within 2 units of the lowest AIC value were considered roughly equivalent. The authors used SAS version 9.4 (SAS Institute Inc) for descriptive, bivariate logistic regression, and multivariable logistic regression analyses.
Results
At baseline (age 1 y), 1326 children had dental examinations, and their primary caregivers completed a 52-item questionnaire. At the child’s age of approximately 2.5, 4, 8, and 9.5 years, 1062, 985, 576, and 510 children, respectively, had oral examinations, and their primary caregivers completed intermediate follow-up questionnaires. Among the 1062 children at the second dental examination, 50.8% were White, 33.9% were Black, and 12.8% were Hispanic; the annual household income for 15.9% of respondents was ≥$100 000 and for 11.7% of respondents was ≤$5000; and 54.1% were enrolled in Medicaid.
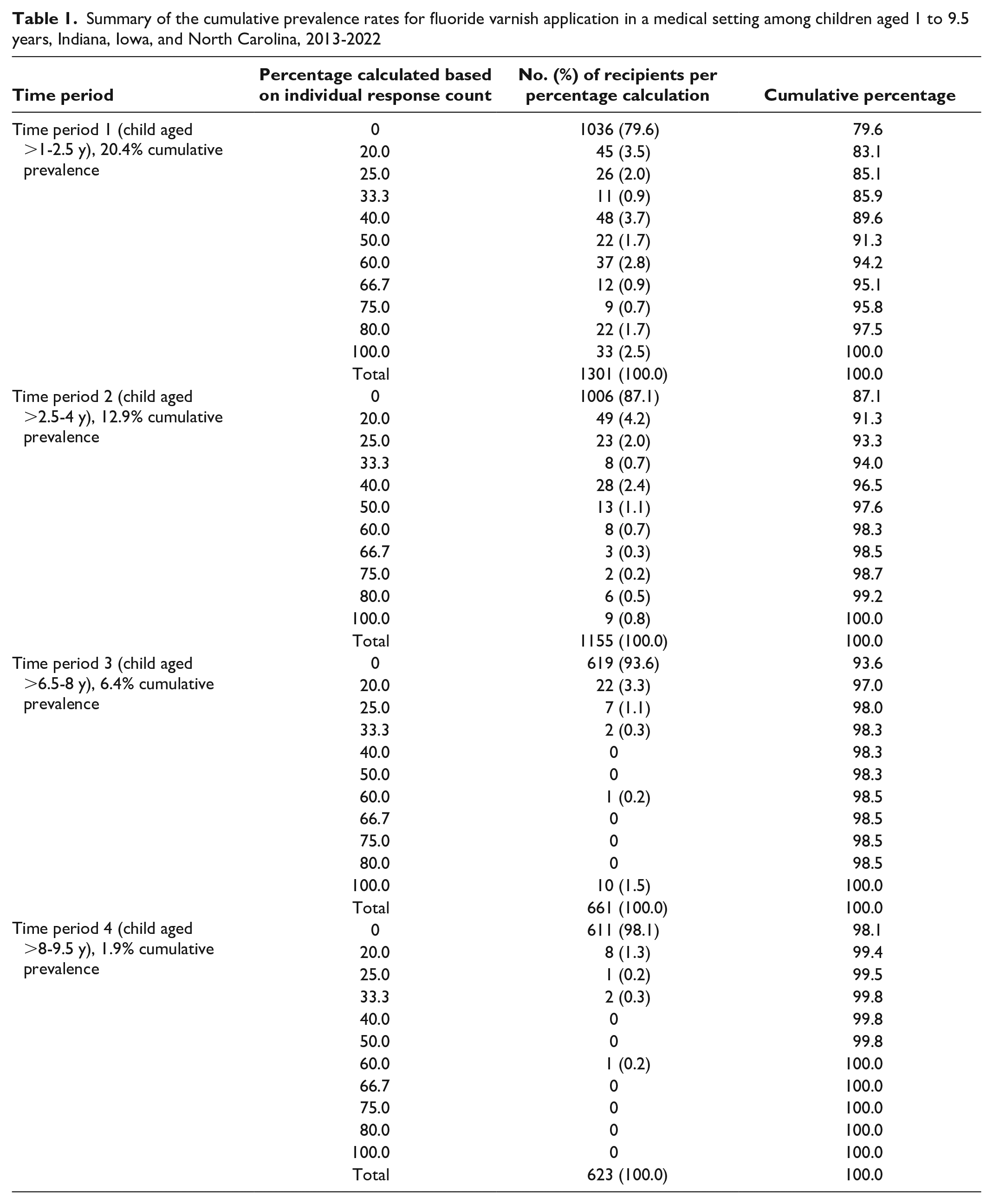
At the first 4-month intermediate follow-up contact, 1257 of 1325 (94.9%) primary caregivers responded, with 136 (11.6%) reporting their child had received fluoride varnish application in the medical setting (eTable 1 in Supplemental Material). Each time period had 5 short time period–specific prevalence rates. For time period 1, the time period–specific prevalence rates ranged from 5.2% to 13.1%. The time period–specific prevalence rate ranges were 4.3% to 5.3% for time period 2, 0.7% to 1.8% for time period 3, and 0.2% to 0.7% for time period 4. The cumulative prevalence rates were 20.4% for time period 1, 12.9% for time period 2, 6.4% for time period 3, and 1.9% for time period 4 (Table 1).
Summary of the cumulative prevalence rates for fluoride varnish application in a medical setting among children aged 1 to 9.5 years, Indiana, Iowa, and North Carolina, 2013-2022
Ten factors were significantly associated with children’s receipt of any fluoride varnish application in the medical setting during cumulative time period 1 (Table 2). Child factors associated with higher odds of children’s receipt of medical fluoride varnish from age 1 to 2.5 years included being Black or multiracial, having a daily habit of falling asleep while nursing or drinking something other than water, frequency of child’s consumption of sugary beverages, and being enrolled in Medicaid and/or other public assistance programs. Primary caregiver factors associated with higher odds of children’s receipt of medical fluoride varnish were having an annual household income of ≤$79 999, primary caregiver’s weekly or more frequent consumption of sugary beverages, and primary caregiver’s perception that they took excellent care of their child’s teeth. In addition, the Duke University study site was a factor associated with higher odds of the child’s receipt of fluoride varnish application in the medical setting. The primary caregiver factor associated with lower odds of children’s receipt of fluoride varnish in the medical setting was the primary caregiver’s twice-yearly dentist visits.
Bivariate logistic regression analysis results of factors associated with receipt of fluoride varnish application in the medical setting for children aged 1 to 2.5 years, Indiana, Iowa, and North Carolina, 2013-2015 (N = 1062)
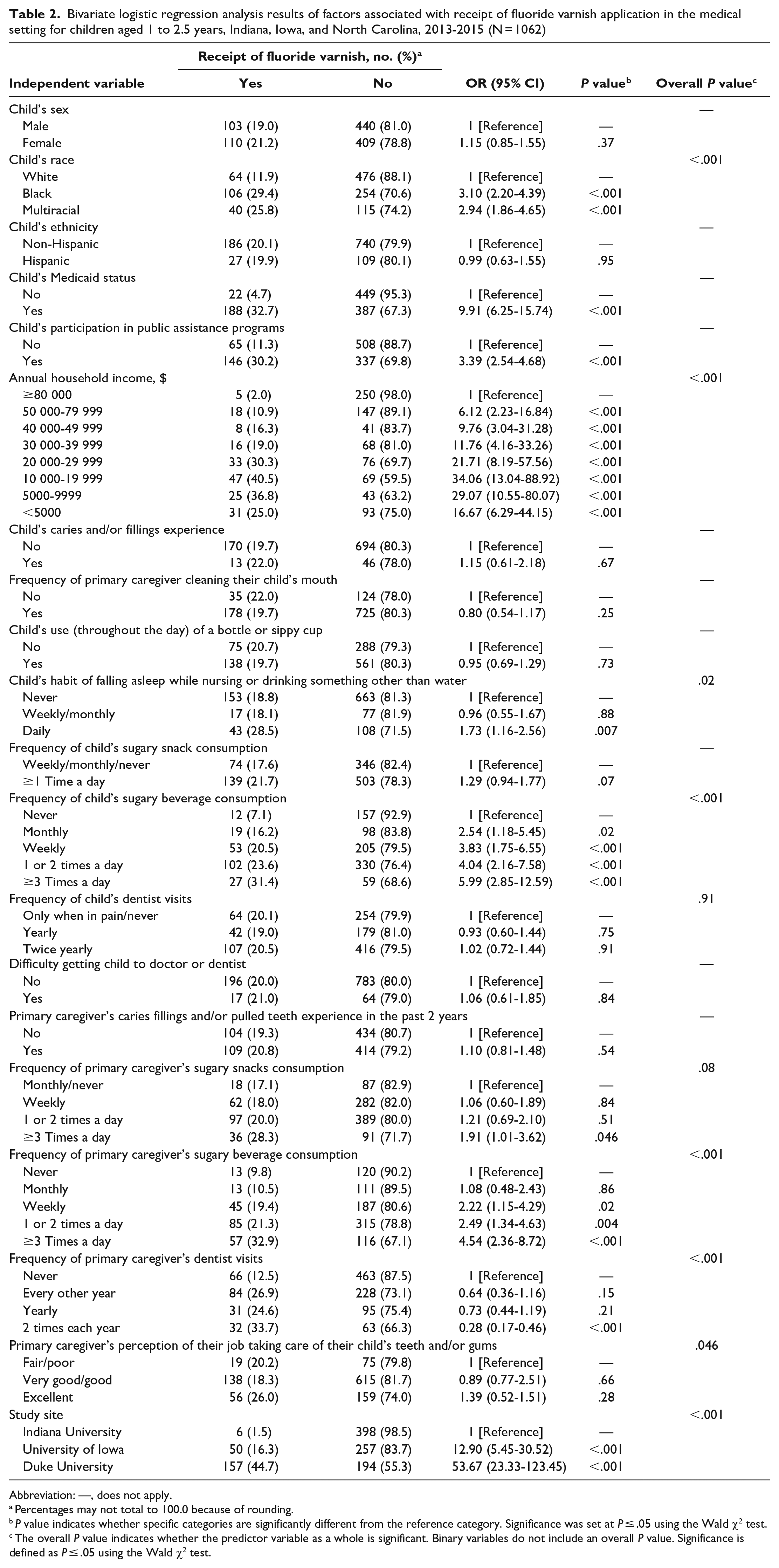
Abbreviation: —, does not apply.
Percentages may not total to 100.0 because of rounding.
P value indicates whether specific categories are significantly different from the reference category. Significance was set at P ≤ .05 using the Wald χ2 test.
The overall P value indicates whether the predictor variable as a whole is significant. Binary variables do not include an overall P value. Significance is defined as P ≤ .05 using the Wald χ2 test.
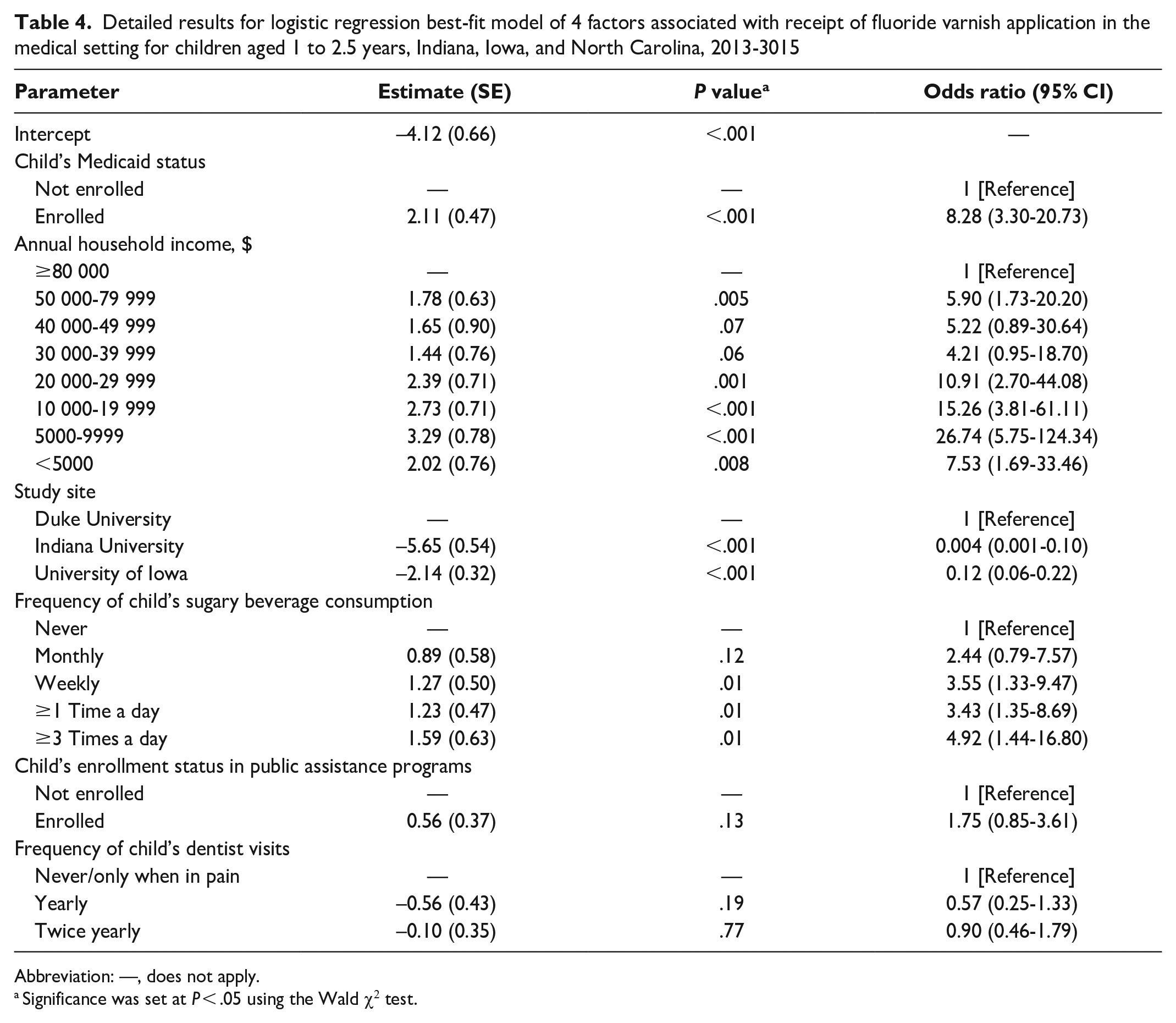
Following the backward elimination, stepwise multivariable logistic regression analysis showed 4 models that best fit the data, with model 1 having the lowest AIC of 391.08 (Table 3). However, all models within 2 units of the lowest AIC model were not substantially different from each other. The researchers retained 6 variables in at least 1 of the 4 best models: child’s Medicaid-enrolled status, annual household income, study site, child’s frequency of sugary beverage consumption, child’s enrolled status in other public assistance programs, and frequency of child’s dentist visits (Table 4). All 4 models showed that children’s enrollment in Medicaid, lower annual household income, and the Duke University study site were factors associated with children’s significantly higher odds of receipt of medical fluoride varnish application. Children’s more frequent consumption of sugary beverages was associated with children’s higher odds of receipt of medical fluoride varnish application in models 1, 2, and 4; children’s enrollment in other public assistance programs was associated in models 1 and 4; and child’s infrequent dentist visits was associated in model 4.
Logistic regression best-fit models of factors associated with receipt of fluoride varnish application in the medical setting for children aged 1 to 2.5 years, Indiana, Iowa, and North Carolina, 2013-2015 a
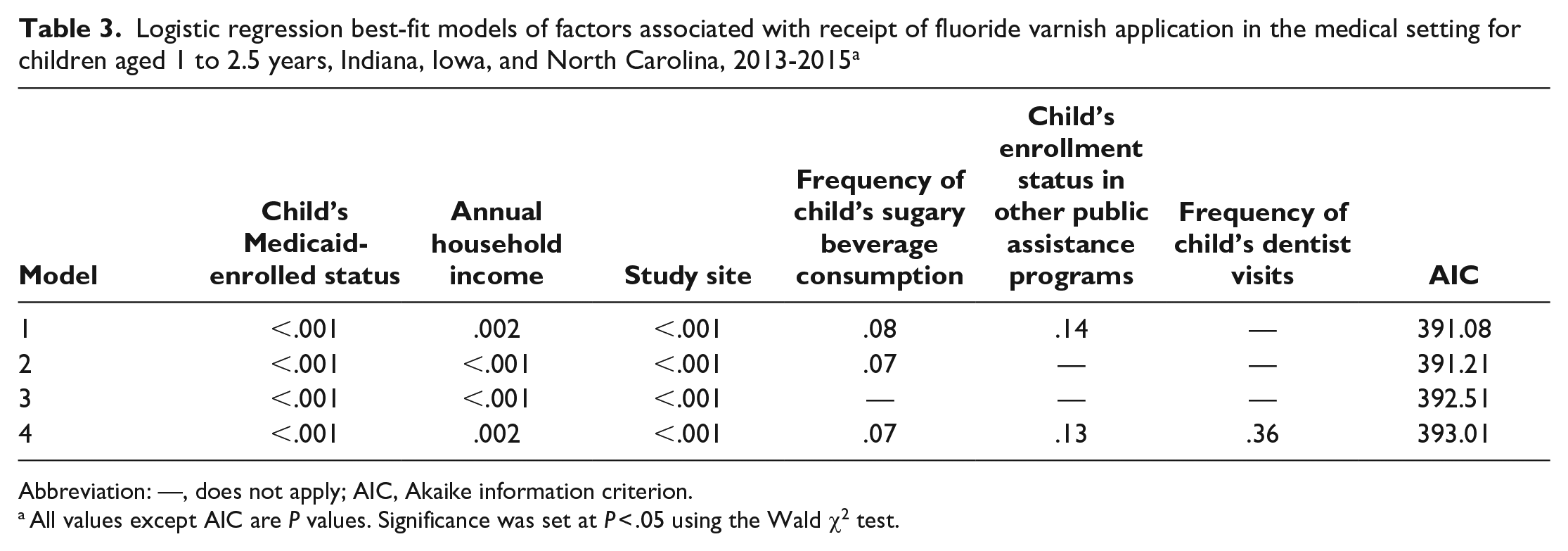
Abbreviation: —, does not apply; AIC, Akaike information criterion.
All values except AIC are P values. Significance was set at P < .05 using the Wald χ2 test.
Detailed results for logistic regression best-fit model of 4 factors associated with receipt of fluoride varnish application in the medical setting for children aged 1 to 2.5 years, Indiana, Iowa, and North Carolina, 2013-3015
Abbreviation: —, does not apply.
Significance was set at P < .05 using the Wald χ2 test.
Discussion
The approximately 4-month time period–specific and cumulative prevalence rates of receipt of medical fluoride varnish application were unique to this study and decreased substantially as children aged from approximately 1 to 9.5 years. The highest cumulative prevalence of medical fluoride varnish application was during time period 1 at 20.4%, when the children were approximately aged 1 to 2.5 years, with decreasing cumulative prevalence during each successive time period. This finding is consistent with previous research that showed the highest rates of medical fluoride varnish application were among younger children, with lower rates as the children aged.17,19,20 One reason for the lower prevalence of medical fluoride varnish application as children aged could be due to lack of reimbursement for medical providers after a certain age. At the time of data collection, the USPSTF recommended fluoride varnish application by medical providers until age 6 years, which probably contributed to the decrease in prevalence as children aged.
This study was also notable for showing the prevalence of medical fluoride varnish application among children from 3 states with various types of state and private health insurance. In previous analyses with the same study cohort, Fontana et al 20 evaluated the same children from 3 states with various types of state and private health insurance but assessed the combined receipt of medical and dental fluoride varnish application. Other studies focusing on medical fluoride varnish application assessed only the prevalence of fluoride varnish application among children from either various locations19,20 or with various health insurance types,17,20,21 with 1 study evaluating a single location and health insurance type. 18
The authors found no significant association between children’s receipt of fluoride varnish application in the medical setting from age 1 to 2.5 years and sex, which is similar to the results of previous studies.18–20 Multivariable analysis results showed that receipt of fluoride varnish was more likely at the Duke University site than at the Indiana University and University of Iowa sites, a finding similar to the findings of Geissler et al, 19 who found significant differences in rates among different states. The higher rate at Duke University could be a result of the statewide Into the Mouth of Babes program, which has advocated for fluoride varnish treatment in the medical setting statewide since 2001. 25 In addition, Iowa and North Carolina began reimbursing for fluoride varnish application among children until age 3 and 3.5 years, respectively, in the early 2000s, whereas Indiana University did not start until 2017. 26
Bivariate logistic regression indicated several factors that were positively associated with medical fluoride varnish application: child’s Medicaid enrollment, lower annual household income, child’s frequent consumption of sugary beverages, child’s enrollment in other public assistance programs, and child’s infrequent dentist visits. Fontana et al 20 found similar bivariate associations in either 1 or 2 states in their previous study with the same cohort, focusing on children at age 1 year. The current study extends those findings, showing similar associations for children aged 1 to 2.5 years in the medical setting across 3 sites. In addition, our study identified an association between medical fluoride varnish application and the study site, which was not previously reported by Fontana et al. 20
Contrary to previous studies, multivariable analysis did not show higher rates of medical fluoride varnish application for children who were Black, who frequently went to sleep while nursing or drinking nonwater beverages from a bottle or sippy cup, whose primary caregiver frequently drank sugary beverages, and whose primary caregivers had infrequent dental checkups.18,20 However, bivariate regression analyses did associate these factors with higher odds of receipt of fluoride varnish in the medical setting. The higher rates of receipt of fluoride varnish application among Black children align with the findings of previous studies.18,20 Training for medical providers on fluoride varnish application, including educational sessions, online modules, and protocols, has been linked to an increase in the prevalence of fluoride varnish in the medical setting. 27 Medical providers’ receipt of education on caries risk factors may have affected their decisions to apply fluoride varnish to Black children more frequently than to White children. Several factors of children and primary caregivers were associated with children’s receipt of medical fluoride varnish application from age 1 to 2.5 years, suggesting that medical providers may consider caries risk factors in determining whether to apply fluoride varnish. However, findings showed that many children at high risk for caries, such as those of Hispanic ethnicity or with previous caries experience, had not received this preventive measure.
The use of a caries risk assessment tool designed for medical providers to assess young children’s caries risk could help physicians to better focus on oral health and, thus, could result in a higher prevalence of fluoride varnish application in the medical setting. More research is needed to better understand the patterns of the use of fluoride varnish application in the medical setting as well as health care provider, child, primary caregiver, family, community, and health care institution factors associated with its use. An increase in the use of fluoride varnish application in the medical setting could help to reduce caries among children in the United States, especially among children who are least likely to see a dentist at a young age.
Strengths and Limitations
This study had several strengths. Strengths of this study included its prospective longitudinal design, which allowed the calculation of the cumulative prevalence of receipt of fluoride varnish application in the medical setting through consecutive periods, which was not found in the previous literature17–21; a large initial sample size, which allowed for attrition over time; and a high retention of primary caregiver/child dyads, 28 which resulted in substantial sample sizes remaining for analyses with data from the 52-item questionnaires. The intermediate follow-up questionnaires administered approximately every 4 months to primary caregivers allowed for frequent contact with the subject dyads, resulting in a reduction in recall bias because of the shorter intervals between questioning and improved retention of study subjects.
The analysis in this study included multivariable logistic regression modeling instead of bivariate analyses as conducted previously by Fontana et al. 20 The use of stepwise regression with AIC for model comparison allowed for model parsimony and inclusion of predictor variables based on model fit instead of the use of P values to guide variable selection. The advantage of this modeling approach was that it helped to retain predictor variables that improve model fit but might not otherwise be included because of reliance on only the P value.
This study also had several limitations. First, this study used a volunteer, convenience sample with people who were compensated for participation. Second, the researchers collected data via a self-reported survey, which can be associated with recall bias, social desirability bias, the Hawthorne effect, and variability in interpretation of survey questions. Third, the researchers recruited participants from 3 tertiary care centers across multiple states, which could have introduced selection bias.
Conclusion
The prevalence of receipt of fluoride varnish application in the medical setting from age 1 to 9.5 years was low and declined with age. Both child and primary caregiver factors were associated with the receipt of medical fluoride varnish from age 1 to 2.5 years. These factors could be used to develop methods to improve the prevalence of medical fluoride varnish application. Higher rates of application of fluoride varnish to children in the medical setting could have important caries-preventive effects, resulting in decreased caries prevalence among children in the United States.
Supplemental Material
sj-docx-1-phr-10.1177_00333549251346012 – Supplemental material for Prevalence of Receipt of Fluoride Varnish Application in the Medical Setting and Associated Factors Among Children in Indiana, Iowa, and North Carolina, 2013-2022
Supplemental material, sj-docx-1-phr-10.1177_00333549251346012 for Prevalence of Receipt of Fluoride Varnish Application in the Medical Setting and Associated Factors Among Children in Indiana, Iowa, and North Carolina, 2013-2022 by Mary C. Tandon, Steven M. Levy, John J. Warren, Shareef M. Dabdoub, Jeanette Daly, Barcey T. Levy, Martha Ann Keels, Anderson T. Hara and Margherita Fontana in Public Health Reports®
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health (NIH)–National Institutes of Dental and Craniofacial Research–DE021412 and NIH Clinical and Translational Science Awards grants: TR002553 (Duke University), TR000006 (Indiana University), TR001356 (University of Iowa), and TR000433 (University of Michigan).
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.