
Abstract
The COVID-19 pandemic magnified long-standing health disparities, showing that certain populations are at higher risk for effects of public health emergencies than others. The pandemic response also put demands on the nation’s health departments and stretched their limited resources. In 2021, the Centers for Disease Control and Prevention launched the National Initiative to Address COVID-19 Health Disparities Among Populations at High-Risk and Underserved, Including Racial and Ethnic Minority Populations and Rural Communities (hereinafter, COVID-19 Health Disparities Grant) to reduce COVID-19 health disparities and advance health equity. Health departments in all 50 states, 50 localities, 5 territories, and 3 freely associated states were recipients of approximately $2.25 billion. This study explored the extent to which investments from the COVID-19 Health Disparities Grant, through the allocation of funds across 5 strategies, correspond to reported changes in recipient health departments’ capacity to address the COVID-19 public health emergency and future emergencies as measured in the Health Department and Jurisdiction Capacity Survey in 2023. The survey measured capacity along 4 domains: workforce and human resources, interorganizational relationships, data and informational resources, and governance and planning. In total, 70 of 75 recipients who responded to the survey reported that they began with low capacity in at least 1 capacity domain and advanced their capacity during grant implementation. This study demonstrated the reported value of investments in health departments to build capacity and infrastructure to address health disparities and advance health equity to respond to future public health emergencies.
The COVID-19 pandemic disproportionately affected populations that are medically underserved, including racial and ethnic minority groups and people living in rural communities, which placed these populations at high risk for infection, hospitalization, and mortality. 1 On June 1, 2021, with funding from the Coronavirus Response and Relief Supplemental Appropriations Act, the Centers for Disease Control and Prevention (CDC) awarded approximately $2.25 billion to the health departments (n = 108 health departments) of the 50 states, 50 local jurisdictions, and 8 US territorial and freely associated states (T/FAS) through the National Initiative to Address COVID-19 Health Disparities Among Populations at High-Risk and Underserved, Including Racial and Ethnic Minority Populations and Rural Communities Funding (hereinafter, COVID-19 Health Disparities Grant). 2 The purpose of the grant was to address COVID-19–related health disparities and advance health equity by expanding health department capacity and services to prevent and control COVID-19 infection (or transmission). As such, intended outcomes (abbreviated) for this one-time, 3-year emergency grant were as follows: (1) reduce COVID-19–related health disparities, (2) improve and increase testing and contact tracing, and (3) improve state, local, and T/FAS health department capacity and services to prevent and control COVID-19 infection (or transmission).
Recipients submitted a full application, including a workplan, project narrative, budget, and budget narrative. They were required to complete quarterly reports to CDC, including progress on their activities, expenditures, and reporting of performance measures. Recipients were not required to implement all grant strategies; rather, they selected strategies that best addressed the priorities and needs of communities. Grant strategies were focused on resources and services, data, infrastructure, and partnerships. However, to achieve local outcomes, recipients could also choose to allocate their grant funds to other strategies. The resources and services strategy was designed to expand existing or develop new mitigation and prevention resources and services to reduce COVID-19–related health disparities. The data strategy was intended to increase or improve data collection and reporting to guide an equitable response to the COVID-19 public health emergency. The infrastructure strategy was designed to build, leverage, and expand infrastructure support for COVID-19 prevention and control. The partnerships strategy, which undergirds all other grant strategies, was intended to mobilize partners and collaborators to advance health equity and address social determinants of health associated with COVID-19 health disparities. All grant strategies sought to build infrastructures that address disparities in COVID-19 and health disparities in future pandemic responses. Recipients reported only on the strategies they implemented; however, all recipients were required to report on the partnerships strategy, because strengthening local public health systems was deemed to be crucial to the grant’s success. 3
Purpose
The COVID-19 pandemic brought increased attention to health disparities and placed demands on the nation’s health departments, which necessitated a shift in resource allocations and stretched existing and limited resources to provide services for COVID-19 prevention and mitigation. 4 This case study explored the extent to which health departments used the flexible, strategy-based investment approach of the COVID-19 Health Disparities Grant to build capacity where most needed. Capacity is dynamic and multidimensional and includes tangible and intangible assets and influences (eg, legal authority, governance). 5 For this case study, we conceptualized capacity as the processes and performance of organizations that affect health outcomes and assessed it using the conceptual model of capacity by Meyer et al. 5
Methods
We analyzed 2 data sources: required reports that recipients submitted quarterly to CDC and a survey we administered to recipients. The purpose of the analysis was to assess whether investment allocations of the COVID-19 Health Disparities Grant supported health departments in building capacity to meet the needs of populations at high risk for COVID-19 effects from the beginning of the grant period through the date of survey completion. The analysis focused on the contribution of the grant to changes in capacity rather than attribution because in addition to the COVID-19 Health Disparities Grant, CDC awarded $48.2 billion to states and the District of Columbia and $587.78 million to T/FAS. 6 Where needed, CDC approved a no-cost extension for recipients to accomplish proposed activities through May 31, 2026. Therefore, at the time of analysis, grant funds were not fully expended; as such, results should be interpreted as “findings to date.”
Required Quarterly Reports to CDC
We analyzed the most complete and current data available as of May 2024. Recipients entered estimates for funds allocated to grant strategies into a funding allocation table in REDCap version 14.0.24 (Vanderbilt University), a web-based data reporting system hosted by CDC. Recipients were asked to update the table as they adjusted their workplans. The allocation amounts included in this analysis were submitted during February 28, 2022–May 15, 2024, and verified by recipients for accuracy within the prior 2 reporting quarters.
We used the Excel version 2308 (Microsoft Corporation) pivot table function to calculate aggregate sums. We used the pivot table output to calculate minimum and maximum allocations for each strategy both by recipient type and overall. We present allocations to strategies within recipient type groups. We calculated these percentages with the total amount allocated to each strategy for each recipient type (numerator) divided by the total award amount for each recipient type (denominator). We validated the totals included in the funding analysis by using a series of logical checks to ensure consistency, validity, and reliability. This analysis included funding allocation data for all 108 recipients. Not shown in the results are allocations for other strategies and unallocated funds. Recipients allocated $31.76 million to other strategies. At the time of analysis, only 5 recipients had unallocated funds totaling $70.27 million.
Self-Report, Web-Based Survey on Capacity Building
The Health Department and Jurisdiction Capacity Survey, a self-report, web-based survey, was fielded to recipients by NORC at the University of Chicago through a contract with CDC (contract no. GS00G14OADU213). The survey was cleared through the Office of Management and Budget and through CDC. It qualified for a waiver of Paperwork Reduction Act requirements for voluntary data collection related to the COVID-19 public health emergency. 7 The CDC Human Research Protection Office, consistent with CDC policy and federal law, deemed the data collection not research subject to the protection of human subjects. 8 NORC piloted the survey with 6 recipients and administered it to the remaining 102 recipients during September 18–November 10, 2023. The survey focused on recipient capacity-building efforts beginning June 1, 2021, until the date they completed the survey, no later than November 10, 2023. Recipients consented to participate before they could proceed to the survey questions.
To reduce reporting burden on health departments, we used a predesign and postdesign in the survey to assess capacity change. As with other federally funded program evaluations of organizational capacity change, 9 we preferred the predesign and postdesign 10 to the traditional pretest and posttest design because it reduced reporting burden for health department staff who were reporting quarterly, minimized other biases (eg, response shift bias), and reduced missing data by the single-time submission of preinformation and postinformation. The survey used frequently asked questions to encourage survey respondents to work with others in the health department to complete the survey so that final responses would represent numerous perspectives of the average level of capacity across activities.
We prioritized 4 capacity constructs (domains) from the Meyer et al 5 conceptual model for inclusion in the survey: governance and planning, data and informational resources, workforce and human resources, and interorganizational relationships. The selected domains reflect areas where health departments invested grant funds and implemented activities, such as filling workforce vacancies and training gaps to better meet the unique needs of populations in their jurisdictions. For clarity and demonstration purposes, we aligned 1 capacity domain to 1 grant strategy. For example, the workforce and human resources domain assessed changes in hiring, retention, promotion, and training practices to increase workforce diversity. This domain is aligned to the infrastructure strategy, which supported building a sufficient workforce, infrastructure, and capacity critical for providing equitable access to populations disproportionately affected by the COVID-19 pandemic.
We measured self-reported changes in capacity for the 4 domains by asking survey respondents to indicate how their health department’s capacity changed before and during the grant across 4 capacity levels (ie, prefoundational, early, established, and strong; Table 1). The capacity levels corresponded with a State of California Health Equity Self-Assessment tool 11 that was used across state and local health departments. Therefore, the capacity levels were known and familiar to some survey respondents. The survey response rate was 69% (75 of 108). By jurisdiction type, 32 of 50 (64%) state recipients responded, 40 of 50 (80%) local recipients responded, and 3 of 8 (38%) T/FAS recipients responded. The analysis is presented at an aggregate level by jurisdiction type and might not represent the experiences of all recipients in the respondent group. For capacity domains with multiple constructs, we report the constructs with the highest growth.
Health department organizational capacity–level definitions used in the COVID-19 Health Disparities Grant evaluation’s Health Department and Jurisdiction Capacity Survey administered to grant recipients, United States, September–November 2023 a
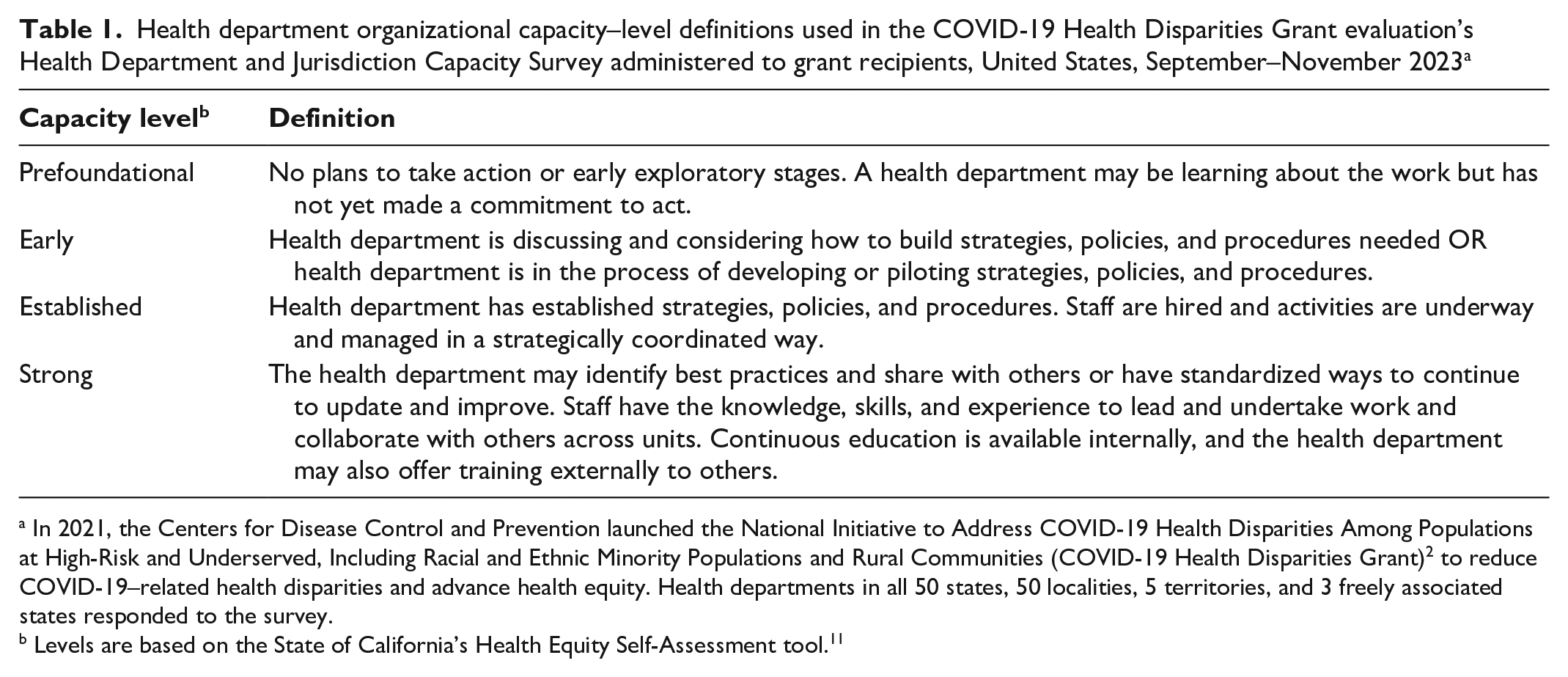
In 2021, the Centers for Disease Control and Prevention launched the National Initiative to Address COVID-19 Health Disparities Among Populations at High-Risk and Underserved, Including Racial and Ethnic Minority Populations and Rural Communities (COVID-19 Health Disparities Grant) 2 to reduce COVID-19–related health disparities and advance health equity. Health departments in all 50 states, 50 localities, 5 territories, and 3 freely associated states responded to the survey.
Levels are based on the State of California’s Health Equity Self-Assessment tool. 11
Outcomes
Allocation of Funds
Recipients allocated funds across 4 grant strategies inclusive of the range of all nonzero allocations for each strategy by recipient type totaling $2.145 billion. T/FAS recipients’ highest-to-lowest funded strategies were resources and services (32%), infrastructure (31%), partnerships (20%), and data (15%) (Table 2). T/FAS recipients often linked funding for activities under different strategies together to build infrastructure. Local health department recipients’ highest-to-lowest funded strategies were partnerships (33%), resources and services (28%), infrastructure (24%), and data (12%). Local activities funded under the partnerships strategy included support for community coalitions and health equity zones (eg, Rhode Island’s Health Equity Zone Initiative 12 ) and direct services provided with or through partners. State recipients’ highest-to-lowest funded strategies were partnerships (35%), infrastructure (30%), resources and services (16%), and data (13%). State activities funded under the partnerships strategy included forming, expanding, reestablishing, or continuing community advisory groups. States also used grant funds to mobilize and compensate community-level programs, including programs designed for rural communities. Because of the availability of other funds for data modernization, 13 recipients used COVID-19 Health Disparities Grant funds under the data strategy to engage communities in new ways to improve data quality and update data systems. Improvements included changing what data are collected, developing dashboards, and sharing data with community leaders.
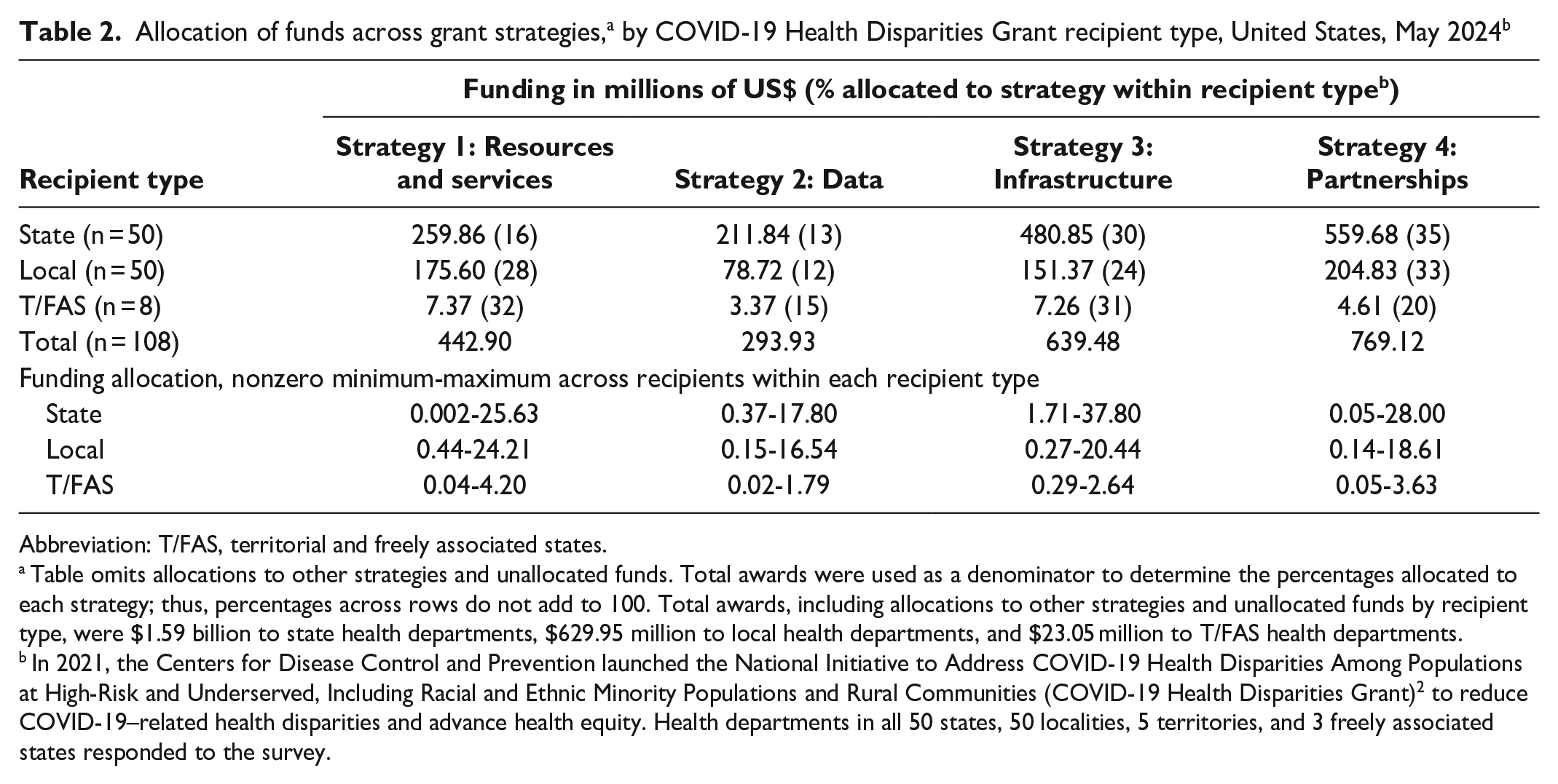
Abbreviation: T/FAS, territorial and freely associated states.
Table omits allocations to other strategies and unallocated funds. Total awards were used as a denominator to determine the percentages allocated to each strategy; thus, percentages across rows do not add to 100. Total awards, including allocations to other strategies and unallocated funds by recipient type, were $1.59 billion to state health departments, $629.95 million to local health departments, and $23.05 million to T/FAS health departments.
In 2021, the Centers for Disease Control and Prevention launched the National Initiative to Address COVID-19 Health Disparities Among Populations at High-Risk and Underserved, Including Racial and Ethnic Minority Populations and Rural Communities (COVID-19 Health Disparities Grant) 2 to reduce COVID-19–related health disparities and advance health equity. Health departments in all 50 states, 50 localities, 5 territories, and 3 freely associated states responded to the survey.
Capacity Change
Most recipients (71 of 75; 95%) self-reported beginning with prefoundational or early capacity across at least 1 of the 4 capacity domains, and 93% (70 of 75) self-reported advancing from low capacity to at least 1 capacity level higher during grant implementation (Figure). Fifty-four recipients self-reported advancing from low capacity to established or strong capacity. Sixteen recipients self-reported beginning with low capacity in any domain and remaining at low capacity at the time of data collection. Finally, the minimum and maximum number of recipients who self-reported starting and remaining at high capacity (established or strong), including those who self-reported progressing from established to strong capacity, were 8 and 17, respectively. Most local health departments reported advances in capacity in the interorganizational relationships (30 of 38) and governance and planning (24 of 37) domains. This finding aligns with their top 2 funded strategies: partnerships and resources and services.
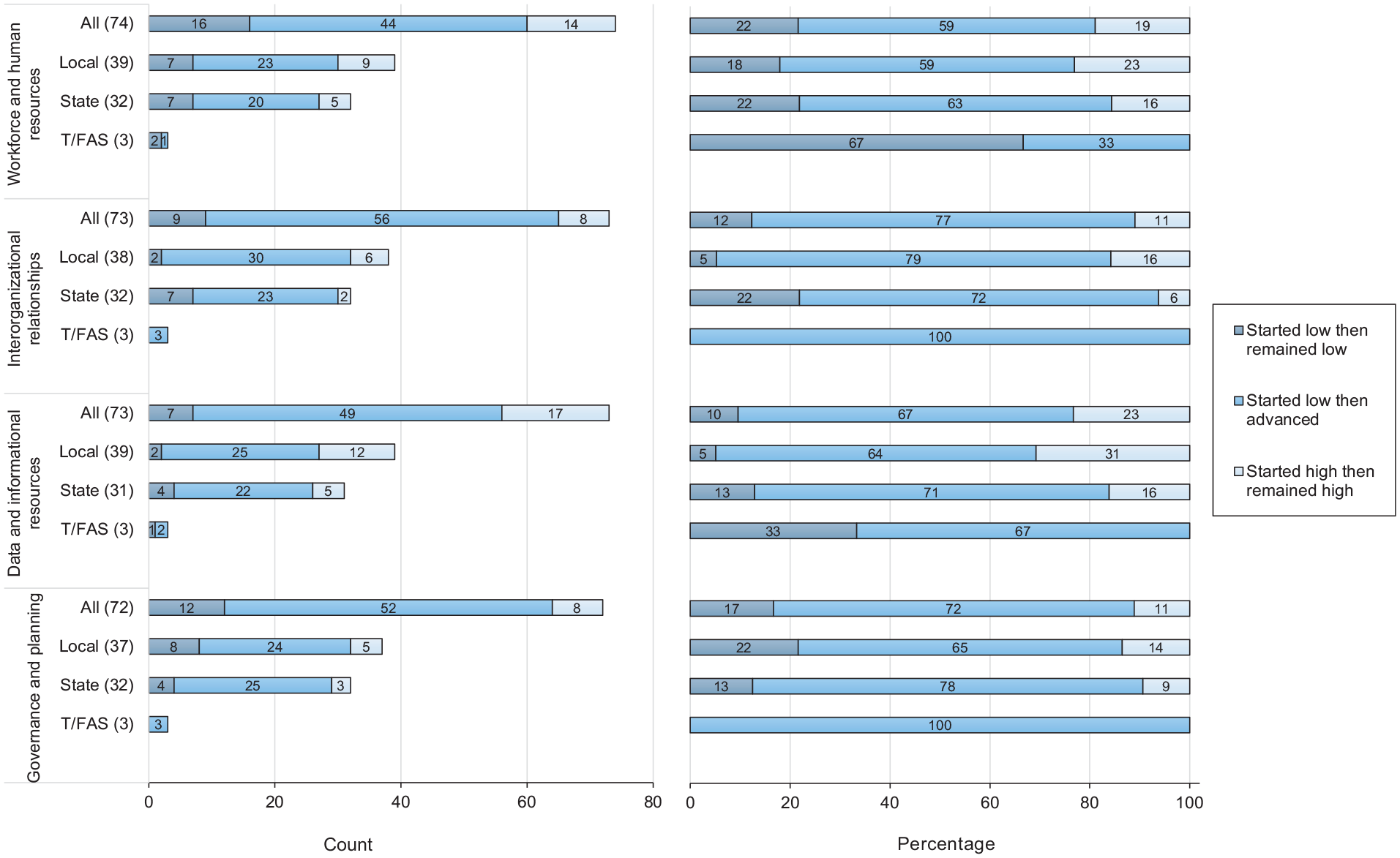
Capacity change from before COVID-19 Health Disparities Grant funding (June 1, 2021) to the time of the survey (November 10, 2023), by domain and recipient type. The label “started low then remained low” means capacity in the domain started at the prefoundational and early capacity stages at time 1 and remained in those stages at time 2. The label “started low then advanced” means capacity in the domain began in the prefoundational and early capacity stages at time 1 and advanced to either established or strong capacity at time 2. The label “started high then remained high” means capacity in the domain started at established or strong at time 1 and ended in the same stage in time 2 or advanced from established at time 1 and ended strong at time 2. The Centers for Disease Control and Prevention launched the National Initiative to Address COVID-19 Health Disparities Among Populations at High-Risk and Underserved, Including Racial and Ethnic Minority Populations and Rural Communities (COVID-19 Health Disparities Grant) 2 to reduce COVID-19–related health disparities and advance health equity. Health departments in all 50 states, 50 localities, 5 territories, and 3 freely associated states responded to the survey. Abbreviation: T/FAS, territorial and freely associated states.
Most state health departments reported advances in capacity in governance and planning (25 of 32; 78%) and interorganizational relationships (23 of 32; 72%) (Figure). The governance and planning domain is seemingly not aligned with where state health departments allocated the most funding (partnerships and infrastructure strategies). However, that activity in this domain (eg, updating emergency operation procedures to focus on health equity) supports expanding resources and services to reduce health disparities. In total, 78% (25 of 32) of state health departments reported either advancing capacity or starting and remaining at high capacity for the workforce and human resources domain. All T/FAS departments reported advances in capacity for the governance and planning (3 of 3) and interorganizational relationships (3 of 3) domains. We observed an association between this finding and their highest funded strategy (resources and services). No T/FAS departments reported starting and remaining in high capacity for any domain. Also, no recipient in any category reported regressing to a lower stage of capacity during grant implementation.
Lessons Learned
These findings highlight important lessons learned. First, the COVID-19 Health Disparities Grant awards and flexible allocation of funds supported health departments in building capacity to address COVID-19–related health disparities and advancing health equity. Almost all recipients reported that they improved their capacity for at least 1 domain where they started with low capacity. It is important to note, however, that the results indicate a temporary increase in capacity. Future studies should explore the sustainability of these improvements.
Second, ensuring that health departments have the resources needed to meet future demands during public health emergencies and sustain the efforts that were started or continued under the grant is important for advancing health equity. Grants with flexible allocation of funds, such as CDC’s Public Health Infrastructure Grant, 14 have the potential to advance or sustain efforts begun with the COVID-19 Health Disparities Grant.
Third, opportunities remain to improve health department and jurisdiction capacity in equitable hiring and recruitment processes and build on advances developed by using grant funds. Opportunities would include developing pathway programs for high school, college, and university students to fill temporary opportunities and provide on-the-job training for students in either public health or health-related fields. Representative workforces are important for health departments to effectively serve communities. 15
Fourth, ensuring health departments have the necessary capacity to manage flexible, partner-focused awards is crucial to a strong public health infrastructure that is equipped to advance health equity, address health disparities, and rapidly respond to future public health emergencies.
This study had several limitations. One limitation was the use of self-reported data to measure funding allocations and capacity change. The other funding data, expenditure data, are also self-reported and do not disaggregate funding by strategy. 16 Neither allocation data nor expenditure data are typically collected for research or evaluation purposes and are not independently validated. The allocation data capture plans to spend funds but not how funds are ultimately expended. Still, it is the best available proxy for expenditure data because it allows analysis to disaggregate funds by strategy, which conceptually aligns with the grant and the purpose of this case study. Allocation data are commonly used in the literature as a proxy for recipient expenditures.17,18 A second limitation was the potential risk for social desirability bias because the survey for this study, although administered by a contractor, was funded by CDC, the funding agency for this grant.
Although the capacity change data were self-reported, the survey design limited the potential for self-report bias by placing items about more specific capacity before the predesign and postdesign questions. This decision provided respondents with examples of capacity built during grant implementation that they could reference and use to support recall and rankings. The self-reported capacity-level items were paired with other, more specific survey items that could be used to contextualize and conceptually validate the self-reported changes in capacity. The predesign and postdesign may have introduced inflationary bias if respondents overstated a positive change in capacity. However, the variability in reported change, including recipients reporting starting and remaining at low capacity across domains, provides some confidence that, despite the risk, the predesign and postdesign was preferrable for reducing reporting burden.
The findings from this study establish that investments through the COVID-19 Health Disparities Grant increased capacity that assisted health departments in their response to the public health emergency. The lessons learned are important considerations for health departments for ongoing and future responses to public health threats and emergencies.
Footnotes
Acknowledgements
The authors acknowledge the following contributors: Nishchala S. Kodali, MS, Alda Tsang, MPH, and Jimmy Minh Huynh, BS (DRT Strategies), supported dataset development for the funding allocation table data and supported management of the overall REDCap reporting system; Nancy Habarta, MPH (CDC), led strategic planning for the overall grant evaluation, including conceptualizing evaluation questions; Hannah McMillan, MPH, Kai Young, PhD, and Cassandra Frazier, MPH (CDC), also contributed to evaluation question development; Cassandra Frazier, MPH, supported development of the final survey instrument, including providing a scale already in use in public health departments that was used for the capacity question; Arielle Shiver, MPH (CDC), reviewed the survey and supported coordination of the survey pilot with recipients; Alycia Bayne, MPH (NORC), provided leadership to her team at NORC; Lauren Isaacs, MPH, MSW, Anu Neupane, MS, and Nina Crowley, MA, MSW (NORC), contributed to survey development, administration, data validation, and analysis; Teresa Tufte, MPH, MSW (NORC), supported survey development, administration through Qualtrics, and analysis; April Bankston, BA, provided programmatic review and feedback that improved the final instrument and support provided to recipients during survey administration; and Angela Shelton, MSPH (CDC), reviewed the instrument and provided input on survey design.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.