
Abstract
Objectives:
Intimate partner violence (IPV) has short- and long-term health effects, including physical injuries and traumatic brain injury, as well as sexual, reproductive, and mental health issues. However, accessing necessary health care is often challenging for IPV survivors and became even more difficult during the COVID-19 pandemic. We examined access to health care among those affected by IPV during the COVID-19 pandemic to better connect survivors to health and social support services.
Methods:
The Health Resources and Services Administration’s Office of Women’s Health partnered with its Bureau of Primary Health Care, the Administration for Children and Families’ Office of Family Violence Prevention and Services, and the National Domestic Violence Hotline (Hotline) on the 2-year Survivor Health Connection Project. The Hotline administered 2 surveys to its contacts: a 2-question postinteraction survey from March 29, 2021, through September 30, 2022, and a longer focused survey in 2021 and 2022 that measured barriers and restrictions to accessing health care, telehealth safety, and interactions with health care providers.
Results:
Of 9918 respondents to the postinteraction survey, 6173 (62.2%) reported current health needs related to their abusive experience. Nearly half of 242 respondents to the 2021 survey (n = 106, 43.8%) indicated that the frequency or intensity of abuse increased during the COVID-19 pandemic, and 157 of 338 respondents to the 2022 survey (46.4%) reported that their partner had controlled and/or restricted their access to health care. Participants described barriers to accessing health care, including finances, health insurance coverage, and transportation.
Conclusions:
Findings illuminate opportunities to further support the health and social needs of those experiencing IPV, including continued coordination of efforts across health care and social service delivery partners.
Intimate partner violence (IPV) is a public health crisis. One in 2 women and >2 in 5 men in the United States will experience contact sexual violence, physical violence, and/or stalking by a partner in their lifetime. 1 While IPV affects all communities, some face disproportionate risks because of structural and social conditions, including racism. The prevalence of lifetime IPV is higher among non-Hispanic multiracial women (63.8%), non-Hispanic American Indian and Alaska Native women (57.7%), and non-Hispanic Black women (53.6%) than among non-Hispanic White women (48.4%). 1 Transgender, gay, and bisexual women may also experience lifetime IPV at higher rates than cisgender heterosexual women.2,3
The effects of IPV on health and well-being are profound. Nearly 90% (86.8%) of female survivors and 59.6% of male survivors are affected by at least 1 IPV-related effect, including negative health conditions and safety concerns. 1 Common health consequences of IPV are physical injuries, traumatic brain injury, and chronic pain, as well as sexual, reproductive, and mental health issues.1,4 IPV can also contribute to health disparities among survivors and their children. As compared with women in nonviolent relationships, women who experience IPV and their children when exposed to this violence are more likely to experience physical and mental health conditions such as headaches, gastrointestinal problems, depression, anxiety, and posttraumatic stress disorder.5,6 Additionally, when survivors flee violent relationships and seek safety, they are often disconnected and isolated from health services and behavioral health supports.7,8
The COVID-19 pandemic exacerbated the perpetration and severity of relationship violence, highlighting the need to bolster the response to concurring threats to public health.9,10 For example, stay-at-home orders and other closures of regularly accessed spaces and services led to increased isolation and complications in responding to IPV.11,12 Other effects of the pandemic, particularly increases in economic precarity and related stress, contributed to the erosion of protective factors against IPV. 11 Digital health care, including telehealth, was helpful in meeting demand when physical services were halted; however, it is not without access, privacy, and safety issues. 13
Access to information and services offered by local health care providers, behavioral health providers, and advocacy programs is critical for the health and well-being of IPV survivors and their children. Yet, during the COVID-19 pandemic, access to health care and advocacy services was reduced because of facility closures and delays in visits. 10 To improve this access and identify, respond to, and prevent these forms of interpersonal violence and their associated effects during the COVID-19 pandemic and beyond, the Health Resources and Services Administration’s (HRSA’s) Office of Women’s Health partnered with HRSA’s Bureau of Primary Health Care, the Administration for Children and Families’ Office of Family Violence Prevention and Services (Family Violence Prevention and Services Act [FVPSA] Program), 12 and the FVPSA-supported National Domestic Violence Hotline (hereinafter, Hotline) on the 2-year Survivor Health Connection Project (SHCP). 14
The purpose of this collaboration was to connect those experiencing IPV during the COVID-19 pandemic with health services provided by HRSA-supported delivery sites and with social services offered through the Hotline. This project also addressed the following research question: What were the experiences of accessing health care among those who were affected by IPV and contacted the Hotline during the COVID-19 pandemic?
Project partners were uniquely positioned to support this collaboration. HRSA is the primary federal agency charged with improving health outcomes by providing equitable health care to people who are geographically isolated and economically or medically vulnerable, serving 30.5 million US patients in 2022. FVPSA is the federal funding stream ensuring that IPV shelter and supportive services are available for IPV survivors and their children, such as provision of training and technical assistance to the advocates and programs that serve them. FVPSA-funded domestic violence shelters and programs serve 1.3 million survivors annually. The Administration for Children and Families’ Office of Family Violence Prevention and Services has administered FVPSA funding since 1996. FVPSA funding is the primary federal funding stream for the Hotline, which operates as the only national 24-hour domestic violence hotline that provides compassionate support, life-saving resources, and safety planning. 15 In 2021, the Hotline received 620 193 calls, texts, and chats, for an average of nearly 1700 daily. 16
Methods
Survey Development
To better understand the experiences of accessing health care among those who were affected by IPV and contacted the Hotline during the COVID-19 pandemic, the SHCP developed a postinteraction survey of anonymous users of the Hotline using SurveyMonkey. The survey contained 2 questions: “Do you have current health (physical, mental, or emotional) needs related to your abusive experience?” and “How comfortable would you be in sharing your experience with abuse with your health care provider (if you have or were to have one)?” We collected data from March 29, 2021, through September 30, 2022.
Using SurveyMonkey, the project team also developed a health care accessibility–focused survey (hereinafter, focused survey) of anonymous users of the Hotline, with 11 questions in English and Spanish: 2 open-ended questions on barriers to accessing health care and comfort in contacting health care providers; 5 single-select questions focused on restrictions to accessing health care, interactions with health care providers, telehealth safety, and experiences of abuse during COVID-19; 1 open-ended question on types of assistance needed to address needs; and 3 demographic questions on gender, age, and race and ethnicity. The project team administered the first round of the focused survey from June 23 through August 1, 2021 (eTable 1 in the Supplement).
The COVID-19 pandemic exacerbated preexisting vulnerabilities in health systems, such as limited resources and workforce shortages, as well as health care worker burnout, stress, and mental health challenges. 17 While the effects of the COVID-19 pandemic on health care systems differed throughout 2021 and 2022, many of the effects on the workforce were cumulative and will persist after the pandemic. Because of this cumulative effect, we emphasized maintaining questions on restrictions to accessing health care and interactions with health care providers between survey rounds and included more open-ended questions in the 2022 focused survey to better understand the barriers to accessing health care that were reported in the 2021 focused survey.
In 2022, the project team updated the focused survey to include 11 questions in English and Spanish. Questions from the 2021 survey that remained the same were 3 demographic questions and 3 single-select questions on restrictions to accessing health care, interactions with health care providers, and telehealth safety. Responses to the 2021 open-ended questions informed response categories for 2 single-select questions on barriers to accessing health care and comfort in contacting health care providers. Two new single-select questions covered knowledge of finding low-cost health care and barriers to using health insurance. One new open-ended question asked participants to describe barriers to using health insurance. The second round of the focused survey ran from July 1 through August 28, 2022 (eTable 2 in the Supplement).
Survey Participants and Analysis
Participants in the postinteraction and focused surveys were anonymous users of the Hotline. We did not collect personally identifiable information from participants; therefore, respondents remained anonymous. The project team recruited participants via a link on the Hotline’s website, through the Hotline’s English and Spanish social media posts, with a digital referral link, and by telephone. Participation was voluntary and participants could stop the survey at any time. The Hotline ran descriptive statistics for the postinteraction and focused surveys using SQL Server and visualized survey results using Tableau (Tableau Software LLC). Data collection for this project constituted a routine project monitoring activity; therefore, HRSA determined that institutional review board approval was not required.
Results
Postinteraction Survey
Of 9918 respondents to the postinteraction survey, 6173 (62.2%) reported current health needs related to their abusive experience during COVID-19, and 3908 of 9063 respondents (43.1%) indicated that they would be somewhat likely or extremely likely to share their experience of abuse with their health care provider.
Focused Surveys
Of respondents to the 2021 (N = 242) and 2022 (N = 262) focused surveys who shared demographic information, most identified as female, White, and aged 25 to 45 years (Table 1).
Characteristics of contacts of the National Domestic Violence Hotline who responded to focused surveys on accessing health care among those affected by IPV during the COVID-19 pandemic, United States, 2021 and 2022

Abbreviation: IPV, intimate partner violence.
More than half of respondents to the 2021 focused survey (52.5%; n = 127) reported that their partner had been abusive and had controlled and/or restricted their access to health care, as compared with 46.5% (n = 157) of respondents to the 2022 focused survey. Similar to the 2021 survey, most respondents to the 2022 survey (53.0%; n = 179) responded that their health care provider spent time or talked with them without their partner present. Of respondents to the 2022 survey who affirmed that their partner controlled or restricted their access to health care, 27.4% (43 of 157) stated that their health care provider did not spend time or talk with them alone. During both survey rounds, more respondents indicated that telehealth appointments were safe (49.6% [120 of 242] in 2021 and 59.5% [201 of 338] in 2022) than unsafe. However, among the quarter of respondents in the 2022 survey whose health care providers did not spend time with them alone, the percentage reporting that virtual appointments were safe decreased from 59.5% (201 of 338) to 50.6% (41 of 81) (Table 2). Challenges with telehealth safety during the pandemic were expressed by 1 participant who shared that virtual appointments are “only safe when he’s gone at work. But even then, there are cameras that can overhear me.”
Health care access during the COVID-19 pandemic among contacts of the National Domestic Violence Hotline responding to focused surveys, United States, 2021 and 2022

Three respondents to the 2021 survey responded yes and no to this question, and these responses were coded as invalid.
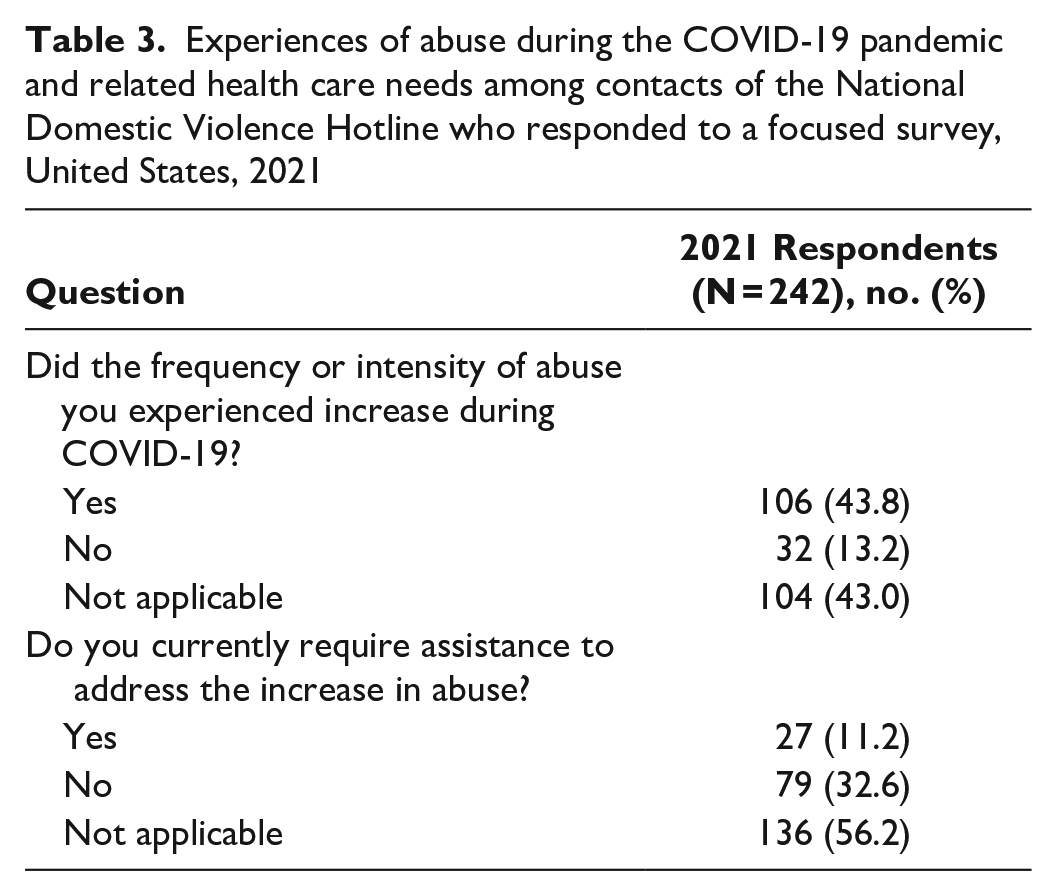
Of 106 respondents to the 2021 focused survey who affirmed that the frequency or intensity of abuse increased during the COVID-19 pandemic, 25.5% (n = 27) reported that they currently required assistance to address this increase in abuse (Table 3).
Experiences of abuse during the COVID-19 pandemic and related health care needs among contacts of the National Domestic Violence Hotline who responded to a focused survey, United States, 2021
Of respondents to the 2022 focused survey, finances and health insurance coverage were the greatest barriers to accessing health care. Finances were reported by 53.0% (179 of 338) and health insurance coverage by 37.6% (127 of 338) (Figure). When asked to describe barriers, several participants shared how partner control influenced their access to health care. One respondent stated, “When I was w[ith] my abuser, he cut off access to my phone. He would also steal my car and money so I wouldn’t have been able to get to appointments.” Barriers to health insurance coverage were another challenge, with 1 participant stating, “After I left him, he cancelled my insurance without telling me, leaving me without insurance for months until I found out.” An additional barrier expressed by several participants centered on patient autonomy over their health appointments. One Hotline user shared, “My ex came with me into the exam room. I could not freely discuss problems including injuries after surgery caused by him.” Challenges in accessing mental health services and the reduced availability of mental health services due to COVID-19 were commonly cited barriers in the 2021 and 2022 focused surveys, as exemplified by 1 respondent to the 2022 survey: “Due to the increased COVID-19 demand in mental health resources, many counselors’ schedules are full.”
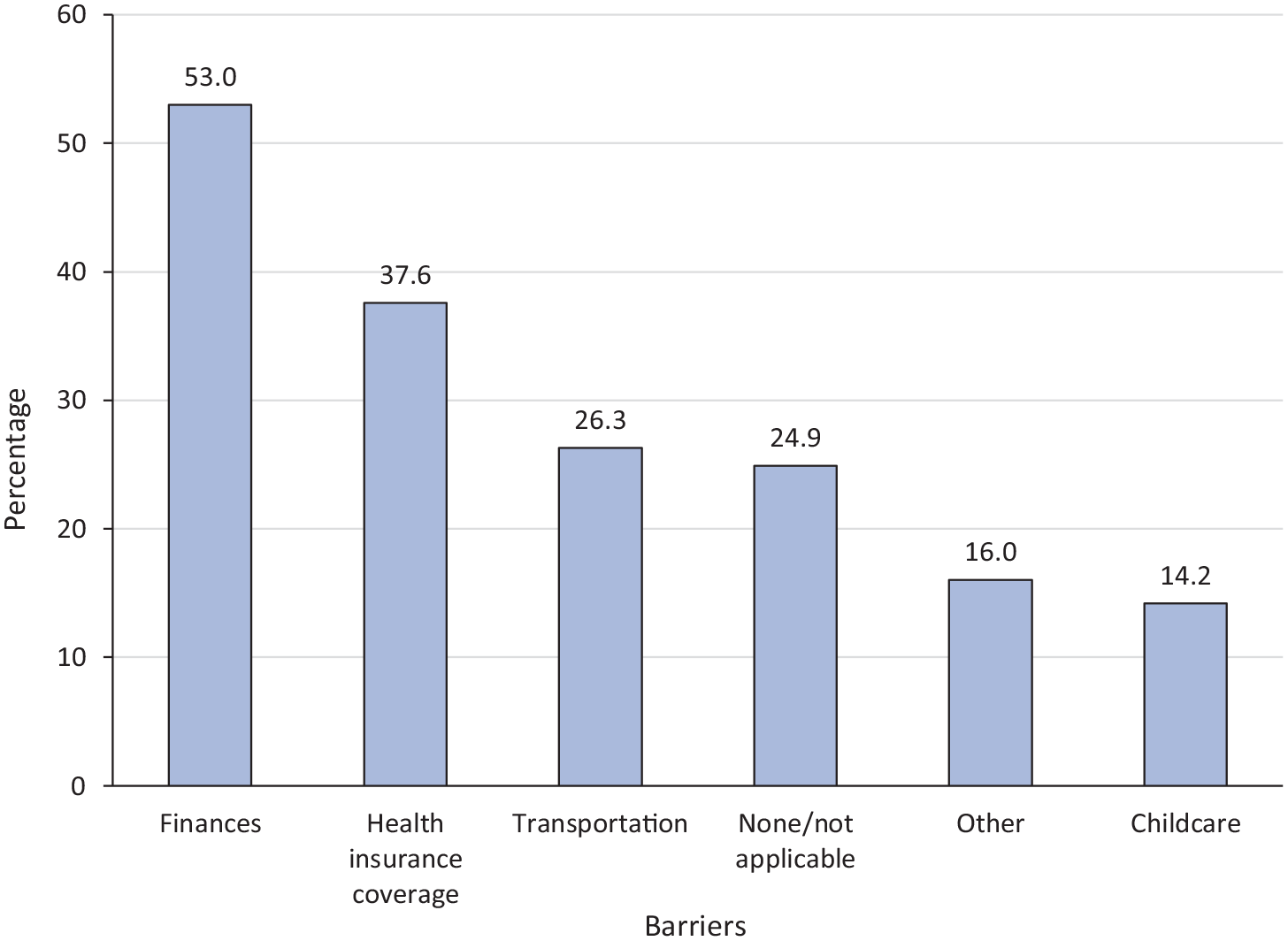
Barriers to accessing health care during the COVID-19 pandemic among contacts of the National Domestic Violence Hotline who responded to a focused survey (N = 338), United States, 2022.
More than half of 279 respondents to the 2022 focused survey said that they would feel more comfortable contacting a health care provider when they felt that the provider would believe them (68.8%; n = 192), trauma-informed care was practiced (66.7%; n = 186), they could trust the staff (62.0%; n = 173), and there was a guarantee of confidentiality (59.5%; n = 166). The importance of leveraging these facilitators to care was expressed by 1 respondent to the 2021 survey: “What has made me comfortable was finding care that didn’t judge me and was exceedingly compassionate and trauma informed.”
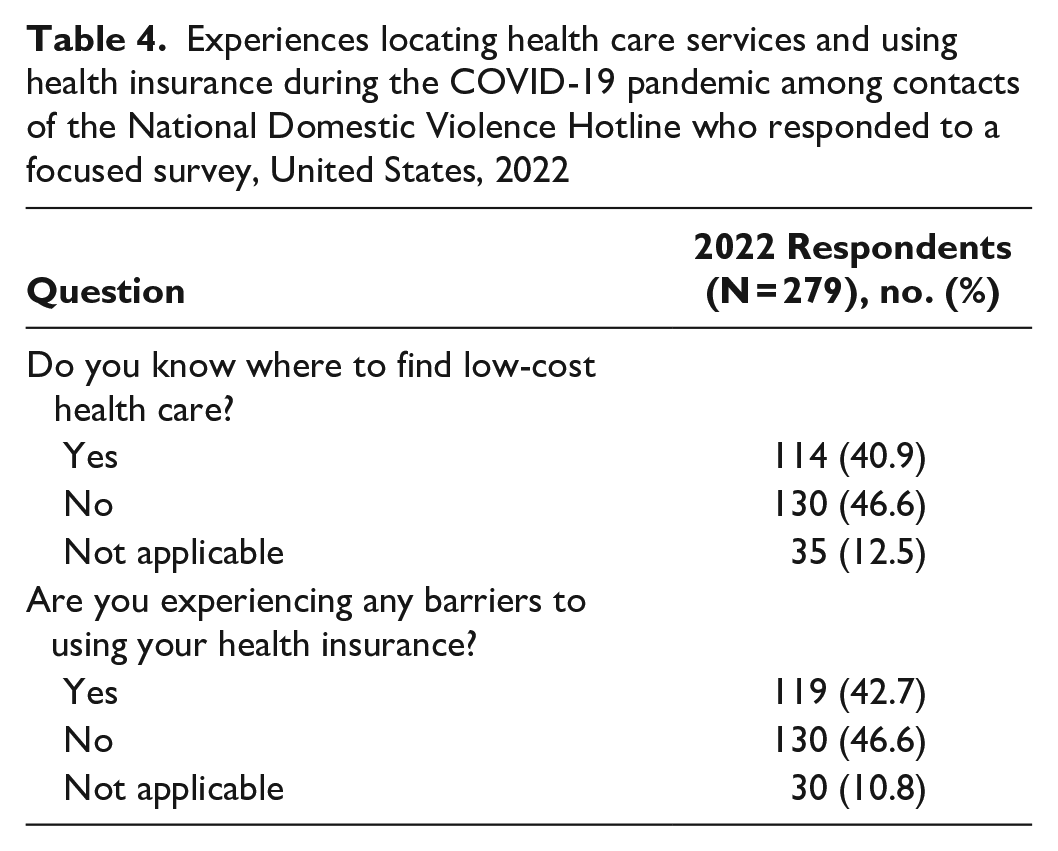
More of the 279 respondents to the 2022 focused survey (46.6%; n = 130) reported that they were not experiencing barriers to using their health insurance as compared with those who indicated not experiencing those barriers (42.7%; n = 119). However, those experiencing barriers shared challenges in locating health care providers who accepted their health insurance and challenges navigating health insurance networks. One respondent said, “Nowhere close takes my insurance, so have to drive 2+ hours away to find a doctor.” Challenges in using Medicaid were expressed by a participant who stated, “Medicaid is only accepted by few places, and even less are accepting new patients.” Finally, almost half of respondents to the 2022 survey (46.6%; n = 130) did not know where to find low-cost health care (Table 4).
Experiences locating health care services and using health insurance during the COVID-19 pandemic among contacts of the National Domestic Violence Hotline who responded to a focused survey, United States, 2022
Discussion
These findings illuminate opportunities to address the social, physical, health, and well-being needs of those experiencing IPV during future public health emergencies and normal operations, and they reveal experiences of accessing health care among those who were affected by IPV during the COVID-19 pandemic. The finding from this project—namely, that partners who used violence controlled and/or restricted access to health care during the pandemic—aligns with common control tactics, such as coercive control and isolation, which is especially alarming considering the disruption to health care and support services caused by the pandemic. The increase in frequency and intensity of abuse during the COVID-19 pandemic, along with the assistance needed to address the increase reported in this study, highlights the additional strain that the COVID-19 pandemic placed on health care and social support services for IPV. During future public health emergencies, including pandemics, health care and social service partners can promote messaging of programming and existing resources available to those who may be experiencing IPV. Coordination of efforts across federal partners, including those engaged in health care, behavioral health, and social service delivery, is crucial to maximize existing resources that support these efforts.
The COVID-19 pandemic also emphasized existing disparities in health outcomes and access to health care, especially among those at risk of and experiencing relationship violence. For example, the challenges in using Medicaid during the pandemic shared by 1 survivor, particularly in finding health care providers who were accepting new patients, may have been exacerbated by pandemic-associated workforce shortages. Additional reported barriers to accessing health care, including finances, health insurance coverage, and patient autonomy, may have been exacerbated by the stressors placed on the health care system by the COVID-19 pandemic. However, this study did not study causation of barriers. These barriers underscore the need to connect patients experiencing IPV to wraparound services, a collaborative multidisciplinary process that provides holistic services to meet the physical health, behavioral health, and social support needs of IPV survivors during future emergencies and in general practice. For example, to address health insurance coverage barriers that IPV survivors may be experiencing, health professionals and domestic violence advocates can connect survivors to existing national and local health insurance coverage resources. While affordable service options exist—including those at HRSA-supported settings, such as health centers that offer services on sliding-fee scales and do not turn away anyone regardless of ability to pay—nearly half of respondents to the 2022 focused survey did not know where to find low-cost health care. This finding introduces an opportunity to strengthen promotion of HRSA-supported services and other local resources.
In addition, the diversity of needs for those experiencing violence during public health emergencies such as the COVID-19 pandemic are immediate (eg, transportation, childcare, health insurance coverage) and prolonged (eg, managing chronic health conditions, accessing and maintaining safe housing and economic support). One avenue to meet these ongoing needs is strengthening health care providers’ ability to connect patients to social support services and serve their patients with trauma-informed care, not only during normal operations but also within public health emergencies such as the COVID-19 pandemic, to build trust and support survivors in their health care decisions. 18 More than two-thirds of respondents to the 2022 focused survey reported that the use of trauma-informed care would increase their comfort when contacting health care providers for support. Although not examined in our study, the COVID-19 pandemic may have challenged the ability of health care settings to maintain trauma-informed practices. 19 An important aspect of trauma-informed care is spending time with patients alone so that they may discuss experiences of violence without their partner present, should patients choose to disclose this information. 20 However, nearly one-quarter of respondents to the 2022 focused survey stated that their health care provider did not spend time with them alone. These findings offer an opportunity to strengthen training and technical assistance for health care providers across disciplines on trauma-informed care and to support patients who have experienced relationship violence.
As an example of technical assistance, project partners provided the Hotline with resources to integrate information about health and behavioral health into their safety planning framework and referral processes for survivors. One such resource is the HRSA Find a Health Center tool, 21 an interactive map that allows users to search for local, comprehensive, primary and preventive health care services. These resources led to operational changes to Hotline advocate workflows that increased capacity to connect contacts to high-quality affordable health care. Another platform to connect IPV survivors to health care is a set of new webpages on the Hotline’s website linking to the HRSA Find a Health Center tool.22,23
Limitations
This study had several limitations. First, the project team administered the postinteraction and focused surveys only to users of the Hotline; therefore, survey data were missing perspectives of those who experienced violence during the study period but did not use the Hotline. Nonusers of the Hotline may have unique challenges to locating health care services or unique barriers in accessing health care. Second, most respondents to the focused survey identified as White and female. However, people in racial and ethnic minority groups, medically underserved communities,24,25 and gender-diverse communities are typically affected by experiences of IPV at a higher rate and face more barriers when seeking health care and other support services than people who are not in these groups and communities. Future data collection efforts would benefit from a more deliberate attempt to diversify participant identities and experiences.
Conclusion
The COVID-19 pandemic contributed to the increase in availability of telehealth services, including services to people experiencing IPV. As advances in telehealth continue, SHCP findings suggest that telehealth for IPV support may be a safe option for some patients. Implications of these findings reinforce the importance of investing in the workforce and technological infrastructures of health centers, domestic violence programs, sexual assault programs, and culturally specific organizations to ensure that they can provide digital and telehealth services for survivors and their children during future public health emergencies and in general practice. However, these organizations should consider the safety and security risks for people experiencing IPV and develop strategies to increase the safety and security for IPV survivors and their families. Increased technical assistance may be needed to develop such strategies. The SHCP emphasizes the importance of not only health care and advocacy partnerships but also technology infrastructures to support the safety, health, and well-being of millions of domestic violence survivors seeking help across the country.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241291496 – Supplemental material for Survivor Health Connection Project: Understanding Experiences of Accessing Health Care Among Those Affected by Intimate Partner Violence During the COVID-19 Pandemic
Supplemental material, sj-docx-1-phr-10.1177_00333549241291496 for Survivor Health Connection Project: Understanding Experiences of Accessing Health Care Among Those Affected by Intimate Partner Violence During the COVID-19 Pandemic by Ellen Hendrix, Jane Segebrecht, Kris Thomas, Tracy Branch and Shawndell Dawson in Public Health Reports
Footnotes
Acknowledgements
The authors thank the leadership and staff at the Health Resources and Services Administration’s Office of Women’s Health and Bureau of Primary Health Care, as well as the Administration for Children and Families’ Office of Family Violence Prevention and Services and Family Violence Prevention and Services Act Program, for their contribution to the development, implementation, and monitoring of the project. The authors also thank Sala Fuchs, Marty Hand, MSPA, Celbrica Tenah, MS, Rosemary Estrada-Rade, MSOL, and the survey team at the National Domestic Violence Hotline for their contributions to the management and evaluation of the project.
Authors’ Note
The views expressed in this publication are solely the opinions of the authors and do not necessarily reflect the official policies of the US Department of Health and Human Services, the Health Resources and Services Administration, or the Administration for Children and Families, nor does mention of the department or agency names imply endorsement by the US government.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Intra-departmental Delegation of Authority of the Further Consolidated Appropriations Act, 2020, HR 1865, Public Law No 116-94.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.