
Abstract
In 2021, the US government undertook Operation Allies Welcome, in which evacuees from Afghanistan arrived at 2 US ports of entry in Virginia and Pennsylvania. Because of the rapid evacuation process, the US government granted evacuees an exemption to a Centers for Disease Control and Prevention (CDC) requirement in place at that time—namely, that air passengers present a negative SARS-CoV-2 viral test result or documentation of recovery from COVID-19 before they boarded international flights bound for the United States. This study describes cases of SARS-CoV-2 infection detected among 65 068 evacuees who arrived at the 2 ports of entry in August and September 2021. Because evacuees were a population at increased risk for infection with diseases of public health concern, CDC staff helped coordinate on-site and on-arrival testing, visually observed evacuees for signs and symptoms of communicable disease, and referred evacuees for further evaluation and treatment as needed. CDC staff used antigen or nucleic acid amplification tests at the ports of entry to evaluate evacuees aged ≥2 years without documentation of recent SARS-CoV-2 infection. CDC staff isolated evacuees with confirmed SARS-CoV-2 infection and quarantined their close contacts, consistent with CDC guidance at the time, before evacuees rejoined the repatriation process. Of 65 068 evacuees, 214 (0.3%) were confirmed as having SARS-CoV-2 infection after port-of-entry testing. Cases of measles, varicella, pertussis, tuberculosis, hepatitis A, malaria, leishmaniasis, and diarrheal illness were also identified. Although the percentage of SARS-CoV-2 infection was low in this evacuated population, communicable disease detection at US ports of entry, along with vaccination efforts, was an important part of a multilayered approach to mitigate the transmission of disease in congregate housing facilities and into US communities.
In August 2021, under the direction of the US Department of Homeland Security, the Centers for Disease Control and Prevention (CDC) joined Operation Allies Welcome (OAW). 1 OAW was a multiagency US government humanitarian mission that coordinated the safe resettling of evacuees from Afghanistan (including special immigrant visa holders and parolees and other Afghan nationals) and the repatriation of a portion of evacuees who were US citizens and lawful permanent residents. After leaving Afghanistan, the evacuees temporarily stayed at various overseas locations (transit locations) before they arrived by plane at 2 US ports of entry: Washington Dulles International Airport and Philadelphia International Airport.
To expedite the transportation of evacuees to the United States, on August 15, 2021, CDC granted a blanket humanitarian exemption to its order, in effect at that time, that required all international air passengers aged ≥2 years to show either proof of a negative SARS-CoV-2 viral test result collected within 3 days before boarding a US-bound flight or proof of recent recovery from COVID-19 as defined in the order. 2 Under the order, a humanitarian exemption could be granted if the following criteria were met: (1) “exigent circumstances where emergency travel [was] required to preserve health and safety” and (2) “predeparture testing [could not] be accessed or completed before travel.” For OAW, this exemption to the order was contingent on all eligible evacuees from Afghanistan receiving SARS-CoV-2 viral testing immediately upon their arrival to the United States, the subsequent isolation of any evacuees with confirmed SARS-CoV-2 infection, and quarantine of identified close contacts before evacuees could continue their travel in the United States by commercial transportation. 3
Purpose
Few data exist describing communicable disease concerns or mitigation measures taken during rapid evacuation of populations who might later be housed in congregate settings after arrival. This case study describes the evacuees from Afghanistan who were diagnosed with SARS-CoV-2 infection and other communicable diseases of public health concern at 2 US ports of entry during the initial phase of OAW in August and September 2021.
Methods
The evacuation flights began arriving at Dulles International Airport on August 17, 2021, and at Philadelphia International Airport on August 28, 2021 (phase 1). On September 14, 2021, CDC issued a directive for a pause in OAW flights when staff detected cases of measles among the evacuees from Afghanistan. 4 CDC recommended the removal of the predeparture testing exemption on September 20, 2021, 5 when SARS-CoV-2 testing capacity became available at the designated transit locations. Flights resumed on October 5, 2021 (phase 2).
During phase 1, from August 17 through September 10, 2021, staff from CDC, other governmental agencies, and state and local health partners visually observed evacuees from Afghanistan who arrived from overseas locations to the 2 US ports of entry for signs and symptoms of communicable disease (eg, presence of rash or lesions, fever, shortness of breath, coughing) and documented the symptoms on an intake form. Staff administered rapid SARS-CoV-2 viral testing to all evacuees aged ≥2 years arriving from Afghanistan at the 2 ports of entry (including US citizens, lawful permanent residents, special immigrant visa holders and parolees, and other Afghan nationals). Local and state health departments, with the support of a contracting agency, initially performed SARS-CoV-2 viral testing; an interagency group subsequently coordinated SARS-CoV-2 viral testing.
Before specimen collection, evacuees completed a standard intake form (with the assistance of an interpreter), which had questions on demographic characteristics (date of birth/age, sex, and citizenship), symptom status, and COVID-19 vaccination status. Staff administered a rapid SARS-CoV-2 antigen test (BinaxNOW COVID-19 Antigen Card; Abbott) to asymptomatic evacuees aged ≥2 years who did not have documentation of having recovered from SARS-CoV-2 infection during the previous 90 days. Based on CDC’s guidance in place at the time for the use of SARS-CoV-2 antigen tests in congregate living settings, staff administered a confirmatory rapid nucleic acid amplification test (NAAT; ID NOW COVID-19 test [Abbott] or Accula SARS-CoV-2 test [Thermo Fisher Scientific]) to evacuees with a SARS-CoV-2 antigen–positive result. Staff at Dulles International Airport administered only the rapid NAAT to evacuees who reported symptoms on intake that were consistent with COVID-19, including children aged <2 years not routinely tested. Staff at Philadelphia International Airport, because of concerns about limitations in symptom reporting and interpretation of the reported symptoms, administered an initial SARS-CoV-2 antigen test with the confirmatory NAAT to symptomatic evacuees. In rare cases, in compliance with local health department requirements, staff tested evacuees who exhibited symptoms with only a SARS-CoV-2 antigen test. However, staff considered a confirmed case to be only an evacuee who tested positive for SARS-CoV-2 with an NAAT.
Staff at the 2 ports of entry transferred evacuees with confirmed SARS-CoV-2 infection and their close contacts to temporary isolation and quarantine staging areas at the ports of entry. Because of the inherent mixing of the evacuees, both at the transit location and during the long international flights throughout the OAW mission, ascertaining other potentially exposed evacuees was challenging. Therefore, a “close contact” was defined as a family member or other evacuee who traveled with the evacuee with confirmed SARS-CoV-2 as a unit throughout the evacuation process.
Using an interpreter, CDC staff interviewed evacuees with confirmed SARS-CoV-2 infection and their identified close contacts to assess their medical history and COVID-19 vaccination history (documented or self-reported) and to confirm any reported COVID-19–related symptoms. CDC staff also provided recommendations to evacuees on how to prevent SARS-CoV-2 transmission. After the interview, in coordination with the US Department of State, US Department of Homeland Security, US Department of Defense, and local or state health departments, CDC staff used noncommercial transport to transfer evacuees with confirmed SARS-CoV-2 infection and their close contacts from the airport to a nearby location to complete their isolation and quarantine periods before evacuees rejoined the repatriation process (Figure 1).
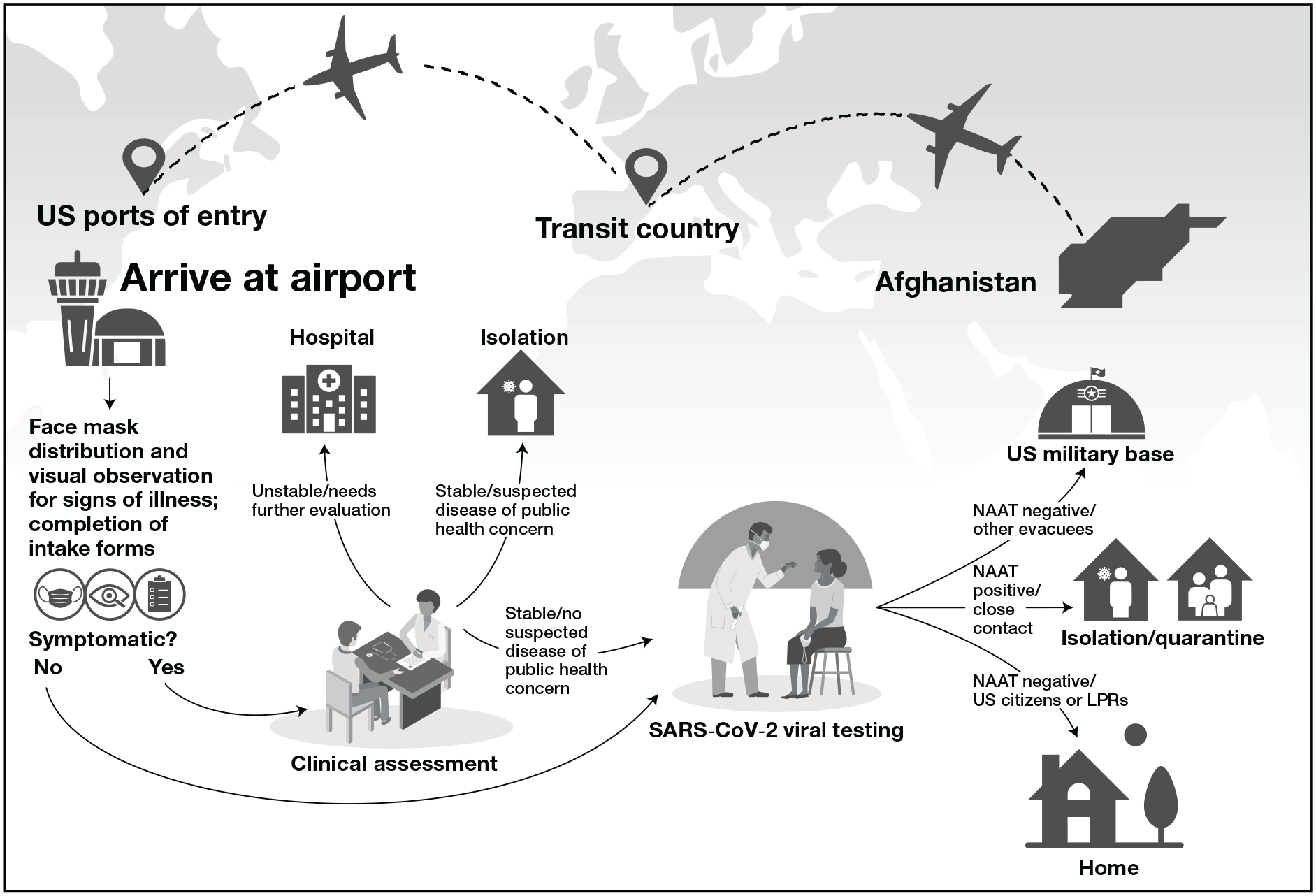
Intake process of evacuees arriving from Afghanistan at 2 US ports of entry, Washington Dulles and Philadelphia international airports, during Operation Allies Welcome, August 17–September 10, 2021. Other evacuees were special immigrant visa holders and parolees. Abbreviations: LPR, lawful permanent resident; NAAT, nucleic acid amplification test.
On-site deployed CDC staff entered data collected from the standard intake form and the case interviews into the secure Port Health Activity Reporting System online database, which is used to record CDC public health activities at ports of entry. Deidentified data were extracted from the Port Health Activity Reporting System and entered into a secure Research Electronic Data Capture form that could be accessed only by a small number of project staff.
On-site clinicians assessed evacuees who needed additional medical evaluation or care unrelated to a communicable disease of public health concern, or they oversaw transfer of evacuees to a hospital for additional assessment. Staff encouraged the use of face masks throughout the intake process and provided them, when appropriate, to all evacuees aged ≥2 years. Many evacuees arrived wearing face masks, although staff noted that some evacuees had likely been using the same face mask for more than the duration of its intended use. Therefore, staff provided new face masks to evacuees aged ≥2 years who were wearing ones that appeared old or soiled.
This project was reviewed by CDC, deemed not research, and was conducted consistent with applicable federal law and CDC policy (eg, 45 CFR part 46; 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
Outcomes
From August 17 through September 10, 2021, 65 068 evacuees entered the United States from Afghanistan and were processed at either Dulles International Airport (52 822 evacuees) or Philadelphia International Airport (12 246 evacuees). During phase 1 of OAW, 214 of 65 068 evacuees (0.3%) from Afghanistan had positive NAAT results for SARS-CoV-2 (Figure 2). Among the 214 evacuees from Afghanistan with confirmed SARS-CoV-2 infection, 14 (7%) were US citizens or lawful permanent residents, and 200 (93%) were Afghan residents. Most evacuees with COVID-19 did not report severe symptoms, and none required hospitalization for COVID-19. Three children aged <2 years who presented with symptoms at intake tested positive for SARS-CoV-2 by NAAT. Among evacuees with confirmed SARS-CoV-2 infection, the median age was 24 (range, 0-81) years, 132 (62%) were male, and 81 (38%) reported being partially or fully vaccinated for COVID-19 (Table). The median number of close contacts for each evacuee from Afghanistan with confirmed SARS-CoV-2 infection was 2 (range, 0-19).
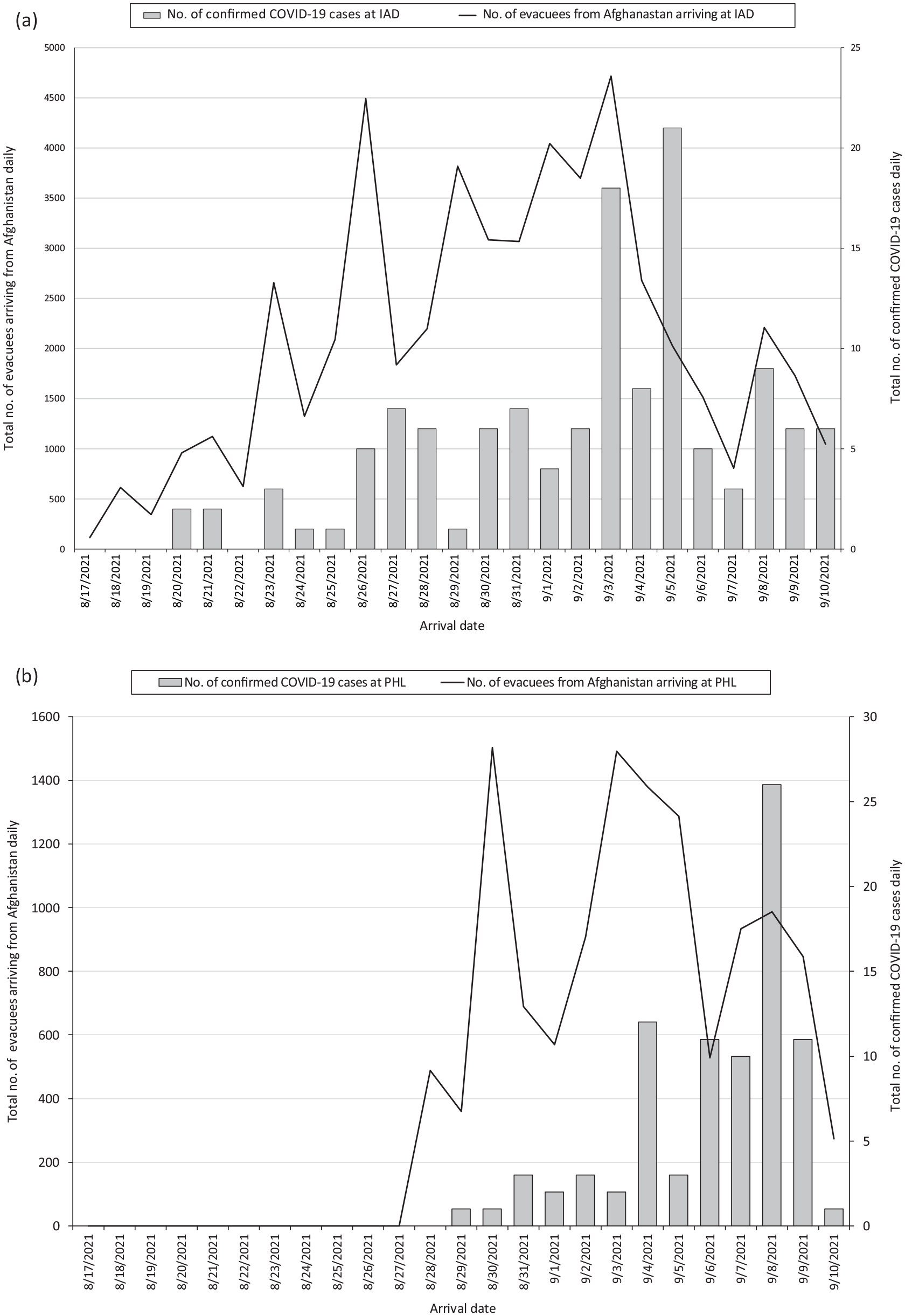
Daily number of evacuees from Afghanistan testing positive for SARS-CoV-2 on arrival and total number of evacuees from Afghanistan arriving daily at 2 international airports during Operation Allies Welcome, August 17–September 10, 2021: (a) Washington Dulles and (b) Philadelphia. Only confirmed COVID-19 cases are indicated (ie, evacuee had a positive SARS-CoV-2 molecular test or nucleic acid amplification test result). The number of evacuees arriving from Afghanistan each day is an estimate and is not equivalent to the number of evacuees from Afghanistan who were tested daily. Abbreviations: IAD, Washington Dulles; PHL, Philadelphia.
Demographic characteristics and vaccination status for evacuees from Afghanistan with positive nucleic acid amplification test results for SARS-CoV-2 at arrival at Washington Dulles and Philadelphia international airports during Operation Allies Welcome, August 17–September 10, 2021 a

Only confirmed COVID-19 cases are indicated (ie, evacuee had positive SARS-CoV-2 molecular test result or nucleic acid amplification test result).
Close contact was defined as a family member or other evacuee who traveled with the evacuee with confirmed SARS-CoV-2 infection throughout the evacuation process.
Vaccination status and vaccine type were based on documentation or self-report.
Vaccines other than those listed here and if the vaccine type was unknown.
During the screening process, staff at ports of entry identified 2 cases of measles, in addition to cases of varicella, pertussis, extrapulmonary tuberculosis (no cases of infectious pulmonary tuberculosis), hepatitis A, malaria, leishmaniasis, and diarrheal illness.
Lessons Learned
The rate of confirmed SARS-CoV-2 infection among evacuees identified at the 2 US ports of entry was low (0.3% of all arriving evacuees during phase 1 of OAW) as compared with the rate in the United States at that time (9.8%). 6 This low percentage was consistent with the results of SARS-CoV-2 viral testing of evacuees from Afghanistan performed at the Spanish border. From August 19 through August 27, 2021, of the 1499 rapid SARS-CoV-2 viral tests performed at Spain’s port of entry, only 1 evacuee (0.07%) had positive SARS-CoV-2 antigen test and NAAT results. 7 Similarly, 14 days before evacuation, Afghanistan’s 7-day rolling average SARS-CoV-2 incidence was 12.61 cases per 1 million people as compared with 231.03 cases per 1 million people in the United States. 8 Full or partial COVID-19 vaccination of the evacuee population may have mitigated transmission among evacuees before arrival. These data were not fully captured because of the nature of the evacuation; many evacuees arrived with incomplete or no documentation of prior vaccination during the reported period. Evacuees often recalled that they had been vaccinated but could not recall the name of the vaccine or the specific date of vaccination.
On September 14, 2021, after the detection of measles among evacuees, CDC issued a directive to pause incoming flights; initiate mass vaccination campaigns for measles, mumps, and rubella and varicella at the overseas and domestic housing locations; and quarantine all evacuees for 21 days postvaccination. 4 After the pause, all evacuees had routine SARS-CoV-2 testing before departure to the United States. After flights resumed on October 5, 2021, no new measles or COVID-19 cases were identified among evacuees. By October 15, 2021, 98% of eligible evacuees at the domestic and overseas locations had been vaccinated against measles. 4
After the predeparture testing exemption was removed and during the pause of the OAW flights, if staffing and resources were available, some of the transit locations provided Johnson & Johnson COVID-19 vaccine to adult evacuees from Afghanistan. At a minimum, all eligible evacuees received vaccines for measles, mumps, and rubella and varicella. When the evacuation flights restarted on October 5, 2021 (only to Philadelphia International Airport), mass testing on arrival at US ports of entry was not performed for all evacuees because predeparture testing was available. The evacuees would not have been able to board their flights to the United States without proof of either a negative SARS-CoV-2 viral test result within 3 days before boarding or documentation of having recovered from COVID-19. Only evacuees who reported COVID-19 symptoms upon arrival to the port of entry received a rapid SARS-CoV-2 NAAT based on an assessment by on-site clinical staff after this time. No evacuees tested positive for SARS-CoV-2 at the port of entry after the OAW flights resumed; in February 2022, CDC deactivated the OAW response. In addition, age-eligible evacuees from Afghanistan were required to get fully vaccinated after arrival with a primary series of a COVID-19 vaccine if they had no documented prior vaccination.
Interpretation of these data is limited by several factors. First, although predeparture testing was not required during the initial phase, some evacuees from Afghanistan reported being tested for SARS-CoV-2 while en route at 1 of the temporary transit locations; however, data were incomplete on when this testing was conducted and with what frequency or regularity. It is assumed that evacuees who had tested positive for SARS-CoV-2 during this in-transit testing would have remained at the transit location to complete their isolation and were therefore not included, during their infectious period, among evacuees who arrived during phase 1 of OAW. Thus, the positivity rate among those directly evacuating Afghanistan during OAW (ie, those housed temporarily and tested at the transit location) may have been higher than the positivity rate among those who subsequently arrived in the United States. Second, the use of antigen tests as the initial screening test may have missed asymptomatic evacuees who might have been positive for SARS-CoV-2 by NAAT only. Yet, data detailing evacuees’ time in transit were not available for analysis. Third, the demographic data of all evacuees from Afghanistan who arrived at the 2 US ports of entry during phase 1 of OAW were limited and are not presented here.
OAW was one of the largest resettlement efforts in the United States within the last 40 years, with >124 000 people evacuated from Afghanistan, in July and August 2021, for subsequent repatriation and resettlement in the United States and elsewhere. 9 During future outbreaks, testing and vaccination entry requirements may be considered a priority intervention when recommended as part of public health guidance for travelers. Testing and vaccination requirements may also be considered before travel to the United States or upon arrival when combined with additional mitigation measures for infected travelers and their close contacts. Implementing such measures may not only limit transmission risk in congregate housing settings but may also mitigate further spread of infection once evacuees are integrated into US communities if implemented early in the course of an outbreak.
Footnotes
Acknowledgements
The authors thank the deployers, public health staff, and federal agencies who assisted with Operation Allies Welcome. The authors also thank CDC staff with the National Center for Emerging and Zoonotic Infectious Diseases, especially leadership in the Division of Global Migration Health, and Miguel Ocaña, MD, and Jennifer Torres, MSHS, with the CDC Port Health Stations in Washington, DC, and Philadelphia. The authors acknowledge and thank Mindy C. Barringer, AA (CDC), for creating the graphics used for ![]() . The authors thank Sheila Roy, MD (CDC), for presenting this work at the 2023 North American Refugee Health Conference. The authors acknowledge the support of eTrueNorth, the Virginia Department of Health, the Virginia Department of Emergency Management, and the City of Philadelphia Department of Public Health. The authors also thank Herbert Wolfe, PhD (Department of Homeland Security), for his tireless support of CDC’s efforts at the ports of entry during this mission and beyond. Finally, the authors thank all of the nongovernmental organizations, volunteers, and communities who supported the Operation Allies Welcome mission.
. The authors thank Sheila Roy, MD (CDC), for presenting this work at the 2023 North American Refugee Health Conference. The authors acknowledge the support of eTrueNorth, the Virginia Department of Health, the Virginia Department of Emergency Management, and the City of Philadelphia Department of Public Health. The authors also thank Herbert Wolfe, PhD (Department of Homeland Security), for his tireless support of CDC’s efforts at the ports of entry during this mission and beyond. Finally, the authors thank all of the nongovernmental organizations, volunteers, and communities who supported the Operation Allies Welcome mission.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hannah Lawman, PhD, contributed to this study in her own capacity, not on behalf of Novo Nordisk.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. In addition, mention of any specific products does not constitute an endorsement of those products by the authors or their employers.