
Abstract
Keywords
One in 5 people in the United States had a sexually transmitted infection (STI) on any given day in 2018, and STIs acquired that year amounted to nearly $16 billion in direct medical costs. 1 The incidence of gonorrhea in the United States increased from 123.0 cases per 100 000 people in 2015 to 188.4 cases per 100 000 people in 2019. 2 The Centers for Disease Control and Prevention estimated nearly 68 million STI cases in the United States in 2018. Of this total, 26 million cases were new STIs acquired in that year. 1 As of 2016, about 2.4 million people had hepatitis C and 850 000 people had hepatitis B in the United States. 3
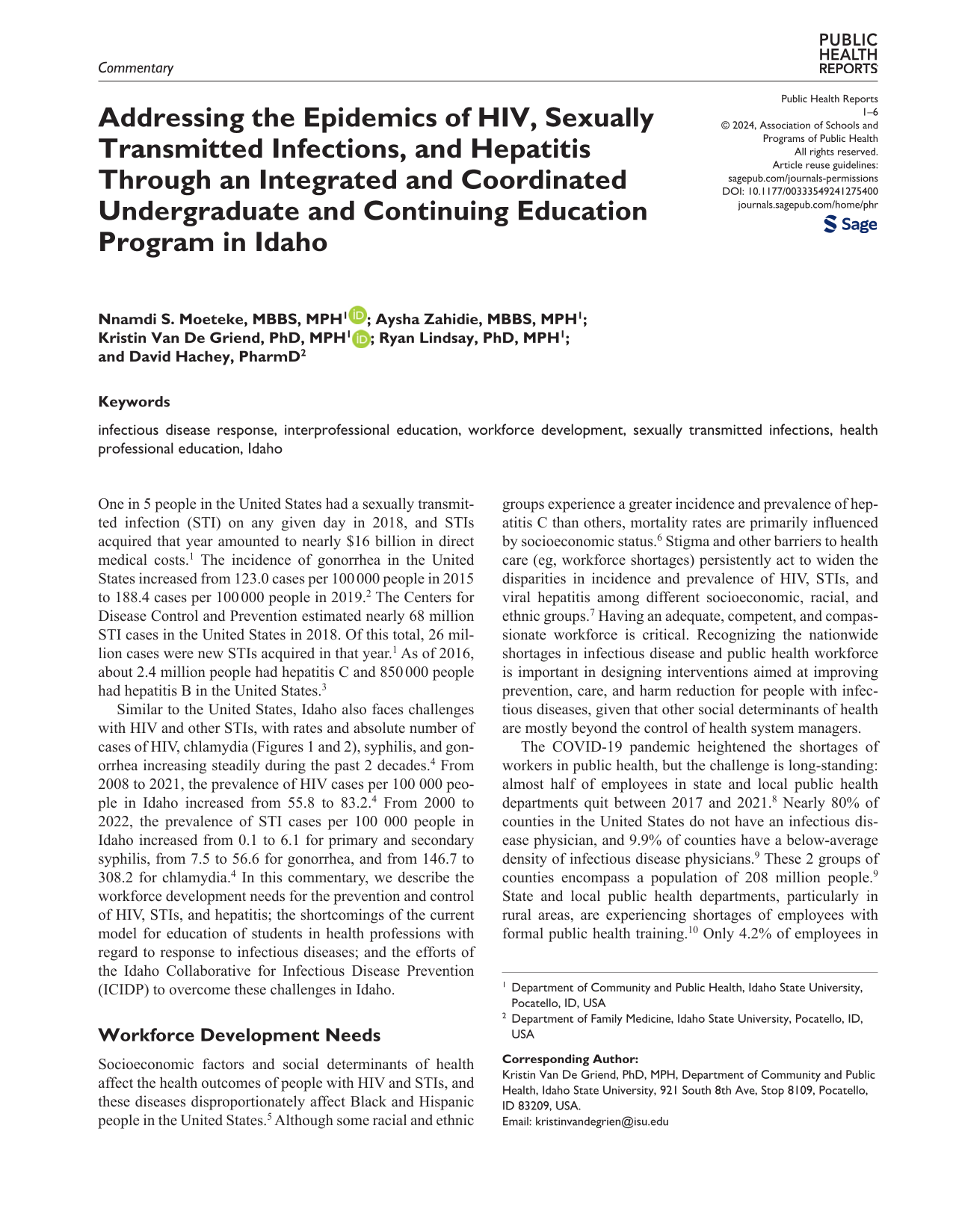
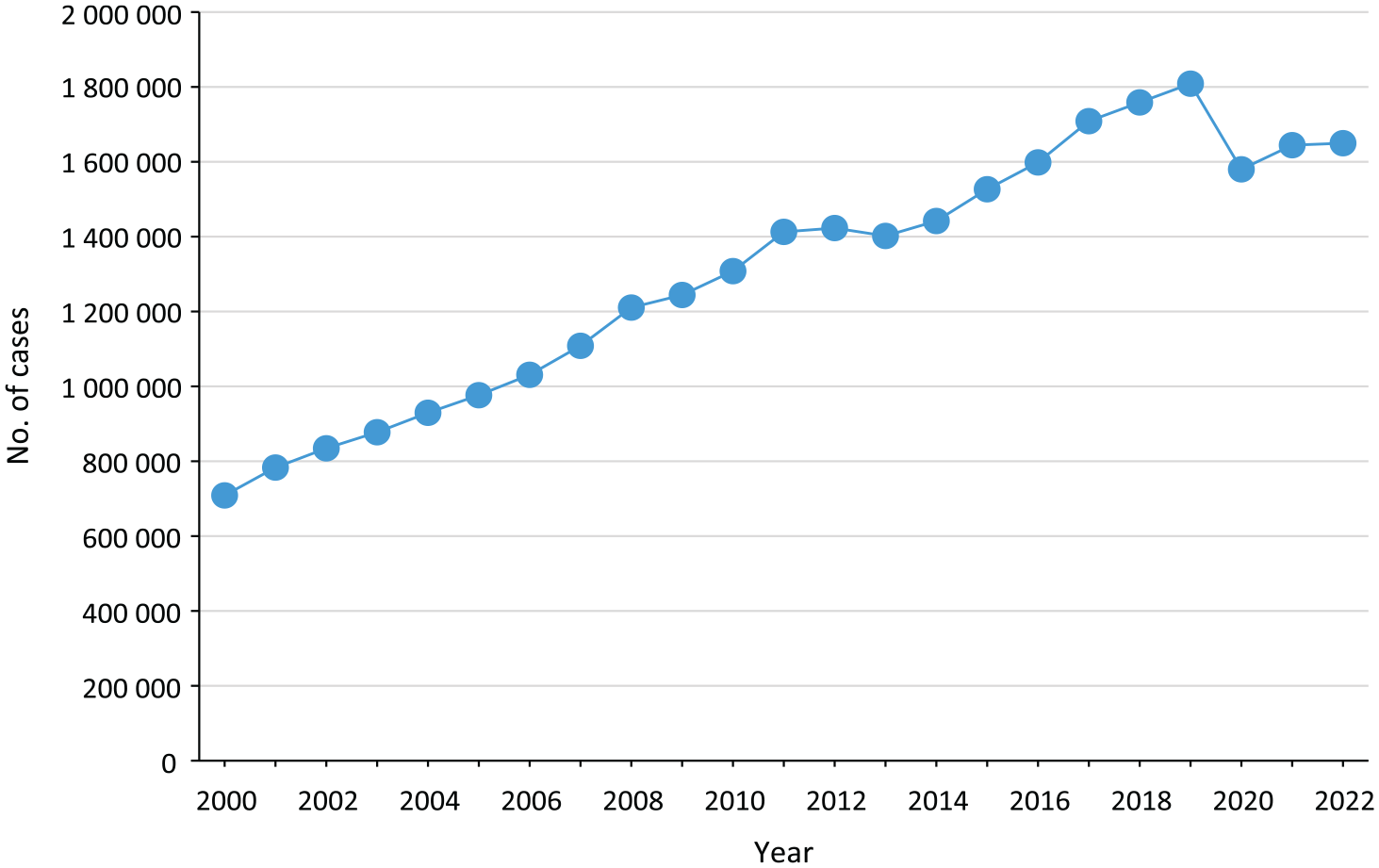
Similar to the United States, Idaho also faces challenges with HIV and other STIs, with rates and absolute number of cases of HIV, chlamydia (Figures 1 and 2), syphilis, and gonorrhea increasing steadily during the past 2 decades. 4 From 2008 to 2021, the prevalence of HIV cases per 100 000 people in Idaho increased from 55.8 to 83.2. 4 From 2000 to 2022, the prevalence of STI cases per 100 000 people in Idaho increased from 0.1 to 6.1 for primary and secondary syphilis, from 7.5 to 56.6 for gonorrhea, and from 146.7 to 308.2 for chlamydia. 4 In this commentary, we describe the workforce development needs for the prevention and control of HIV, STIs, and hepatitis; the shortcomings of the current model for education of students in health professions with regard to response to infectious diseases; and the efforts of the Idaho Collaborative for Infectious Disease Prevention (ICIDP) to overcome these challenges in Idaho.
Number of cases of chlamydia in the United States, 2000-2022. Data source: Centers for Disease Control and Prevention. 4
Number of cases of chlamydia in Idaho, 2000-2022. Data source: Centers for Disease Control and Prevention. 4
Workforce Development Needs
Socioeconomic factors and social determinants of health affect the health outcomes of people with HIV and STIs, and these diseases disproportionately affect Black and Hispanic people in the United States. 5 Although some racial and ethnic groups experience a greater incidence and prevalence of hepatitis C than others, mortality rates are primarily influenced by socioeconomic status. 6 Stigma and other barriers to health care (eg, workforce shortages) persistently act to widen the disparities in incidence and prevalence of HIV, STIs, and viral hepatitis among different socioeconomic, racial, and ethnic groups. 7 Having an adequate, competent, and compassionate workforce is critical. Recognizing the nationwide shortages in infectious disease and public health workforce is important in designing interventions aimed at improving prevention, care, and harm reduction for people with infectious diseases, given that other social determinants of health are mostly beyond the control of health system managers.
The COVID-19 pandemic heightened the shortages of workers in public health, but the challenge is long-standing: almost half of employees in state and local public health departments quit between 2017 and 2021. 8 Nearly 80% of counties in the United States do not have an infectious disease physician, and 9.9% of counties have a below-average density of infectious disease physicians. 9 These 2 groups of counties encompass a population of 208 million people. 9 State and local public health departments, particularly in rural areas, are experiencing shortages of employees with formal public health training. 10 Only 4.2% of employees in state and local public health departments have a degree in public health. 11 Fewer than 30% of local public health departments had an epidemiologist before the pandemic, 12 implying that many infectious disease roles are filled by members of staff from other fields. The limited access to well-trained professionals in infectious diseases and HIV care in many communities continues to hinder the health care system’s capacity to tackle the challenges posed by HIV, STIs, viral hepatitis, and other epidemic-prone infectious diseases. 13 Idaho is mostly rural, and only 9 of its 44 counties are urban. 14 All but 2 counties in Idaho are federally designated as geographic or population-group health professional shortage areas. 15 Some people who work as communicable disease intervention specialists do not have a college degree (L. Hudson, MN, RN, and T. Maxwell, BSN, RN, South Central Public Health District, oral communication, April 18, 2023). These workforce challenges adversely affect prevention, care, and harm reduction efforts for HIV, STIs, and viral hepatitis across Idaho.
Current Education Models on Infectious Disease for Students in Health Professions
Infectious diseases continue to pose challenges with increasing demands on health professionals, and health care systems worldwide are struggling to keep up with ever-new infectious disease threats. 16 Sexual health education, including HIV and STI learning opportunities for students in health professions, has not kept pace with these challenges, with institutions of higher education graduating an underprepared workforce.17 -22 For example, in a survey of pharmacy schools, 78% of schools (29 of 37) provided 10 or fewer hours of classroom education related to HIV. 20 Static curricula can lead to insufficient adaptation to local needs, a narrow technical focus without a broad contextual understanding, and nonalignment of competencies with population health goals. 16 Institutions of higher learning are not structured to be responsive to the increasing incidence and prevalence of infectious disease and the demands on health systems. 16 In a recent survey of health sciences students in a university in Idaho, more than 60% had a negative attitude toward people living with HIV/AIDS, and one-third had a low level of willingness to provide care for these patients. 23 Attempts to rectify these inadequacies have been hampered to some extent by a siloed approach to education, which fosters a systemic lack of collaboration and poor teamwork. Institutional and instructional inadequacies regarding infectious disease may worsen the inequity in care in health systems by aggravating shortages and maldistribution of public health professionals. 16 Students in health professions are more likely to consider a career related to infectious disease if they are trained and feel well-prepared for work in this area. 24
Addressing inadequacies in curricula is needed to mitigate the effects of infectious diseases in medically underserved communities. Although workers in different health professions have unique and complementary abilities, bringing their abilities together is of utmost importance for effective patient-centered and population-based care and prevention. Task sharing and shifting are often needed during epidemics and in workforce shortage areas—an impossible feat when the training of students in each health profession is done in isolation and without interdisciplinary communication and cooperation.
16
To improve health outcomes through the services rendered by the workforce, the professional educational subsystem must design new instructional and institutional strategies that emphasize mutual learning and joint solutions.
16
The Lancet Commission on the Education of Health Professionals for the 21st Century, which was set up in 2010 to develop strategies to prepare students in health professions for present and future challenges of health systems, advocated for interdependence in education and transformative learning.
16
According to the Commission, Instructional reforms should: adopt competency-driven approaches to instructional design; adapt these competencies to rapidly changing local conditions drawing on global resources; promote interprofessional and transprofessional education that breaks down professional silos while enhancing collaborative and non-hierarchical relationships in effective teams; exploit the power of information technology for learning; strengthen educational resources, with special emphasis on faculty development; and promote a new professionalism . . . that develops a common set of values around social accountability.
16
Competency is the consistent and thoughtful application of communication, expertise, clinical reasoning, emotional awareness, values, and reflection in everyday practice to promote the well-being of the individual and the population served. 25 A competency-based approach is a system in which crucial health problems are specified, knowledge and skills needed by graduates to address these challenges are identified, and the curricula are structured to bring about these competencies. 16 Infectious disease outbreaks often necessitate the mobilization and redeployment of health professionals from various branches of clinical health care to public health response. Competency-based education is critical for such flexibility and adaptability and allows for innovation in times of crisis. 26 Similar to other aspects of health care, dealing with infectious diseases will always be about teamwork. As such, interprofessional education should be integrated into health professional training before and after graduation, as part of a continuum of learning. 16 Having curricula that emphasize competencies for teamwork will prepare health professionals to fit into the combined actions of various professionals, which is vital for good practice and health system performance. 16 These reforms are expected to increase the performance of health systems and improve equity in care, with improved outcomes for patients and populations. 16 The Lancet Commission posited that favorable conditions for these reforms and outcomes must first be created. These conditions entail engagement with leaders at all levels in relevant sectors (including the academic and professional communities) and considerable expansion of investments in health professional education.
Idaho’s Integrated and Coordinated Undergraduate and Continuing Education Program
In June 2022, Idaho State University (ISU) and the HIV, STI, and Hepatitis Section of the Division of Public Health in the Idaho Department of Health and Welfare (IDHW) partnered to start ICIDP with 2 goals: (1) to develop and implement an interdisciplinary curriculum geared toward building the capacity of Idaho’s workforce to respond to infectious diseases and (2) to enhance workforce development and interdisciplinary partnerships. The vision of ICIDP is to build and maintain a compassionate workforce in Idaho with the capacity to effectively address prevention, harm reduction, and care for people with HIV, STIs, viral hepatitis, and other communicable diseases, particularly in medically underserved communities. The mission is to be Idaho’s leading multidisciplinary consortium engaged in building interprofessional partnerships and enhancing workforce development in infectious diseases, through education, training opportunities, and research. ISU and IDHW modeled ICIDP on the framework of the innovative approaches highlighted by the Lancet Commission—interprofessional education, use of technology to improve learning, and lifelong continuing education for health professionals.27,28 To this end, ICIDP seeks a coordinated infectious disease response by fostering a common language among all health professionals, with everyone having a population health and equity orientation and an understanding of their actual or potential role as health professionals.
As a first step, ISU and IDHW established a leadership team of 4 faculty members with broad expertise in infectious disease to oversee ICIDP. The team made presentations at health-related academic and research forums at ISU (such as the Division of Health Sciences interprofessional education grand rounds) and held meetings with ISU deans, department chairs, and faculty members to obtain their support for the project. These meetings aided the team in mapping curricula across health-related undergraduate and continuing education programs at ISU. The team obtained and reviewed syllabi from undergraduate and continuing education courses to identify strengths and gaps in training on infectious disease across health sciences programs. In this review, the team found deficiencies in content related to infectious disease response and how to collaborate with other health professions.
Enhancing Workforce Development and Interdisciplinary Partnerships
The leadership team established partnerships with groups outside of ISU, which included relevant members of staff of all 7 public health districts in Idaho, various bureaus in the Division of Public Health at IDHW, health care organizations, and communities, to explore needs and enhance workforce development possibilities. The team discussed ICIDP’s proposed training modules and their learning objectives with partners and sought ideas on ways to improve content and design learning outcomes to meet partners’ personnel needs. Based on the curricular mapping and input from health sciences faculty and partners across the state, the team built learning content at the beginner–intermediate level for the following modules:
i. Foundations of Public Health
ii. Epidemiology Essentials
iii. Infectious Disease 101
iv. HIV, STI, and Viral Hepatitis Prevention, Harm Reduction, and Care
v. Disease Outbreak Response
vi. Fundamentals of Disease Intervention: STI Contact Tracing and Partner Services
vii. Idaho Infectious Disease Resources
viii. Rural Health and Health Equity: Assets and Challenges
ix. Diversity, Inclusion, and Cultural Humility
x. Communicating With Compassion
ICIDP provides the 10 modules free of charge through the online learning management system of ISU’s Division of Continuing Education and Workforce Training. Participants receive a micro-credential (and a digital badge that is shareable on social media) after they complete each module. For participants who finish all 10 modules, ICIDP awards a professional certificate. Furthermore, ICIDP plans to host a statewide collaborative meeting on HIV, STI, and hepatitis thrice a year. The meetings will bring together clinicians, public health practitioners, academics, community-based organizations, people living with HIV, community members, and other relevant individuals and organizations. Less than 5 months after the ICIDP launched the modules on November 27, 2023, more than 100 participants enrolled. People who have enrolled include community health workers and other health professionals from health care institutions, including the tribal health services, staff members of IDHW and 6 of Idaho’s 7 public health districts, and university students in health degree programs. The School of Nursing at ISU has made all 10 modules part of the requirements for its course “NURS 4200 Population Health Nursing.” These actions demonstrate considerable acceptance by the relevant academic and professional communities, including leaders of ISU’s health-related programs and Idaho’s public health districts. ICIDP’s leadership team is currently building 5 modules at an advanced level that will be used for continuing education by health care practitioners.
Theoretical Underpinnings of ICIDP
Educational interventions should be predicated on well-articulated theoretical frameworks. 29 A useful theory for structuring and explaining or predicting the delivery of an interprofessional education program is Mezirow’s transformative learning theory. This theory focuses on adult learning and is recognized as an essential component of professional development.30 -32 Mezirow proposed that the mindset of adult learners can be modified by new information that leads to critical reflection and review, unlike the learning experience of children, which is characterized by persistence in applying old understanding to new situations. As such, an adult’s worldview is changed the more they learn, and this disposition helps adults grasp new concepts and ideas that lead to a transformation to what they should believe and understand in the prevailing circumstances. Mezirow’s theory transcends the simple acquisition of knowledge and dives into the ways that learners consciously make meaning of their lives and understanding.30,31 New perspectives have to appeal to learners both logically and emotionally to challenge their previous position.30,31
Wenger’s theory of communities of practice has been increasingly emphasized for performance improvement in various sectors. 33 According to Wenger, “communities of practice are groups of people who share a concern or a passion for something they do and learn how to do it better as they interact regularly.” 33 These communities are formed when people in a common domain of human endeavor come together for collective learning. 33 Learning could be intentional or an incidental outcome of these interactions. 33 Not every community is a community of practice; the latter must have 3 key features: the shared domain of interest, the community in which members engage in joint activities and share information, and a shared repertoire of resources for their practice. A community of practice is cultivated by developing these 3 elements in parallel. 33 The repertoire of resources for practice can be developed through activities such as problem solving, requesting information, seeking experience, visiting other members for observational learning, sharing technical resources, fostering coordination and synergy, discussing developments, and identifying gaps in competence. 33
Evaluation Plan
After the conclusion of the ICIDP in December 2024, the leadership team will evaluate the program by using predefined outcome measures. The leadership team will measure the success of the program by improvements, from baseline to the end of the program, in knowledge, supportive attitude, and confidence about infectious disease prevention, harm reduction, and care. The team is also interested in whether and to what extent the needs of state partners were met, the number of interdisciplinary training events and their level of attendance (along with outcomes from participant evaluations before and after these events), and the number of practicum and internship opportunities created. The team has already developed measurement tools and has started assessing some of these variables.
Conclusion
Building public health competencies across the health workforce is crucial for overcoming the ever-new challenges posed by HIV, STIs, viral hepatitis, and other infectious diseases. Coordination of efforts across professions has never been as necessary as it is today. 34 ICIDP is demonstrating the importance and feasibility of an integrated and coordinated education program to build the capacity of Idaho’s health workforce. ICIDP is providing an innovative platform to prepare Idaho for current epidemics or a future pandemic and may serve as a model for designing and structuring interprofessional education and training on infectious disease prevention and response across the United States.
Footnotes
Ethical Statement
This article does not involve human data or participants; therefore, institutional review board assessment was not necessary per the policy of the Office of Science and Medicine at the US Department of Health and Human Services, Office of the Assistant Secretary for Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Idaho Collaborative for Infectious Disease Prevention and this publication were made possible by the Centers for Disease Control and Prevention’s PS19-1901, Strengthening STD Prevention and Control for Health Departments (STD PCHD), through the Idaho Department of Health and Welfare (subgrant no. HC291200).
Disclaimer
The contents of this article are solely the authors’ responsibility and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Idaho Department of Health and Welfare.