
Abstract
Objectives:
To improve national drowning surveillance efforts, we developed and evaluated a definition for unintentional drowning for use in the National Syndromic Surveillance Program’s ESSENCE platform (Electronic Surveillance System for the Early Notification of Community-Based Epidemics) and described drowning-related emergency department (ED) visits from 2019 through 2022 using the new definition.
Methods:
We adapted an unintentional drowning definition from a previous version, which included all drowning-related ED visits regardless of intent (including drowning related to assault and suicide, as well as unintentional drowning). We reviewed a random sample of 1000 visits captured by the new definition of unintentional drowning and categorized visits as likely, possibly, and unlikely to be related to unintentional drowning. We compared monthly drowning-related ED visits from 2020, 2021, and 2022 with monthly drowning ED visits from 2019, overall and by sex and age group.
Results:
A total of 35 431 ED visits related to unintentional drowning (10.71 per 100 000 ED visits) occurred from 2019 through 2022. Most visits (86%) captured by the new definition and manually reviewed were likely related to unintentional drowning. Rates were highest among males (14.04 per 100 000 ED visits) and children aged <1 to 4 years (65.61 per 100 000 ED visits). The number of drowning-related ED visits was higher in May and August 2020, May and June 2021, and May 2022 as compared with the same months in 2019 among people aged 18 to 44 years.
Conclusions:
The definition for unintentional drowning is available in the National Syndromic Surveillance Program’s ESSENCE platform for state and local jurisdictions to use to monitor unintentional drowning-related ED visits in near-real time to inform prevention strategies.
Drowning is the leading cause of death among children aged 1 to 4 years in the United States; >4000 people die from drowning each year. 1 Drowning risk varies by demographic characteristics such as age, sex, race, and ethnicity.1,2 Rates of fatal drowning are higher among males than females. 1 Among people aged ≤29 years, rates of fatal drowning are highest among American Indian/Alaska Native and Black/African American people. 2 The number of fatal and nonfatal drownings also varies by month and geographic location.3-6 Most drowning deaths occur between May and August,3-6 and drowning death rates are highest in Alaska, Hawaii, Louisiana, and Florida. 1
Drowning is preventable. Promising drowning prevention strategies include learning basic swimming and water safety skills, wearing lifejackets, installing and maintaining pool fencing that completely encloses the pool, and encouraging close and constant adult supervision of children in or near water. 3 However, access to interventions may differ by demographic and geographic characteristics. 3 Because of the demographic, seasonal, and geographic variation in drowning, it is important for local and state health departments to have timely data to address drowning risk factors to prevent drownings in their jurisdictions.4-6
Syndromic surveillance is used by public health officials to provide timely, actionable information on disease and injuries at the local and state levels. 7 Syndromic surveillance has been used during public health emergencies, such as the COVID-19 pandemic, to identify increases in emergency department (ED) visits for injuries such as suicide attempts, drug overdoses, intimate partner violence, and child abuse and neglect.8,9 Identifying increases in injuries in near-real time can help inform prevention strategies. For example, after detecting an increase in ED visits related to methanol ingestion from hand sanitizer products in 2020, the Arizona Department of Health and Environment was able to inform health care providers of an increase in methanol poisoning and improve messaging to the public of the dangers of ingesting products containing methanol. 10 Our objective was to develop and validate a definition for unintentional drowning for use in the National Syndromic Surveillance Program’s (NSSP’s) Electronic Surveillance System for the Early Notification of Community-Based Epidemics (ESSENCE) and to use this definition to describe unintentional drowning–related ED visits from 2019 through 2022.
Methods
We obtained data from NSSP’s BioSense platform from 2019 through 2022 through ESSENCE. Approximately 6400 health care facilities from 50 states and the District of Columbia provide information to NSSP on ED visits as soon as 24 to 48 hours after a visit. 7 Information supplied to NSSP includes discharge diagnosis codes, chief complaint terms, and limited demographic data. A drowning definition drafted by Austin Public Health used chief complaint and discharge diagnosis (CCDD) fields to classify ED visits related to drowning. 11 The Austin Public Health definition included drowning of all intents. 11 We reviewed and refined the draft definition to include only initial encounter visits for unintentional drowning because drowning prevention strategies differ for unintentional versus intentional drowning.
ED visits were considered drowning related if the following International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) 12 codes were included anywhere in the discharge diagnosis field: T75.1, V90, V92, W16 (where the sixth character = 1, except W16.4 and W16.9, where the fifth character = 1), W22.041, and W65-W74; all codes had a seventh character of A or missing to indicate initial encounter (Table). The Austin Public Health definition also included ICD-10-CM codes X37.8 and X38, which describe flood- and storm-related injuries. 11 We removed these codes in the new definition for unintentional drowning because in the national data, they led to the inclusion of visits not related to drowning, and flood-related drowning was captured from chief complaint terms. We also removed the ICD-10-CM code Y21, which is used to describe drowning of undetermined intent. Additionally, we added and removed chief complaint inclusion and exclusion terms from the Austin Public Health definition to detect additional drowning visits missed by the draft definition and to refine the definition to exclude drownings related to suicide or assault (Table). We made decisions about which chief complaint terms to keep or exclude with the goal of maximizing sensitivity. We applied the CCDD fields to the “CC and DD History” fields instead of the CCDD field in ESSENCE. The history fields are updated as more information about ED visits becomes available, thereby allowing the definition to capture additional drowning visits that would be missed in the CCDD field. We refined the “CDC unintentional drowning v1” definition based on feedback from NSSP and 6 local and state health departments, and the definition was added to ESSENCE in June 2022 (Box).
Components of the Centers for Disease Control and Prevention’s unintentional drowning v1 definition, National Syndromic Surveillance Program
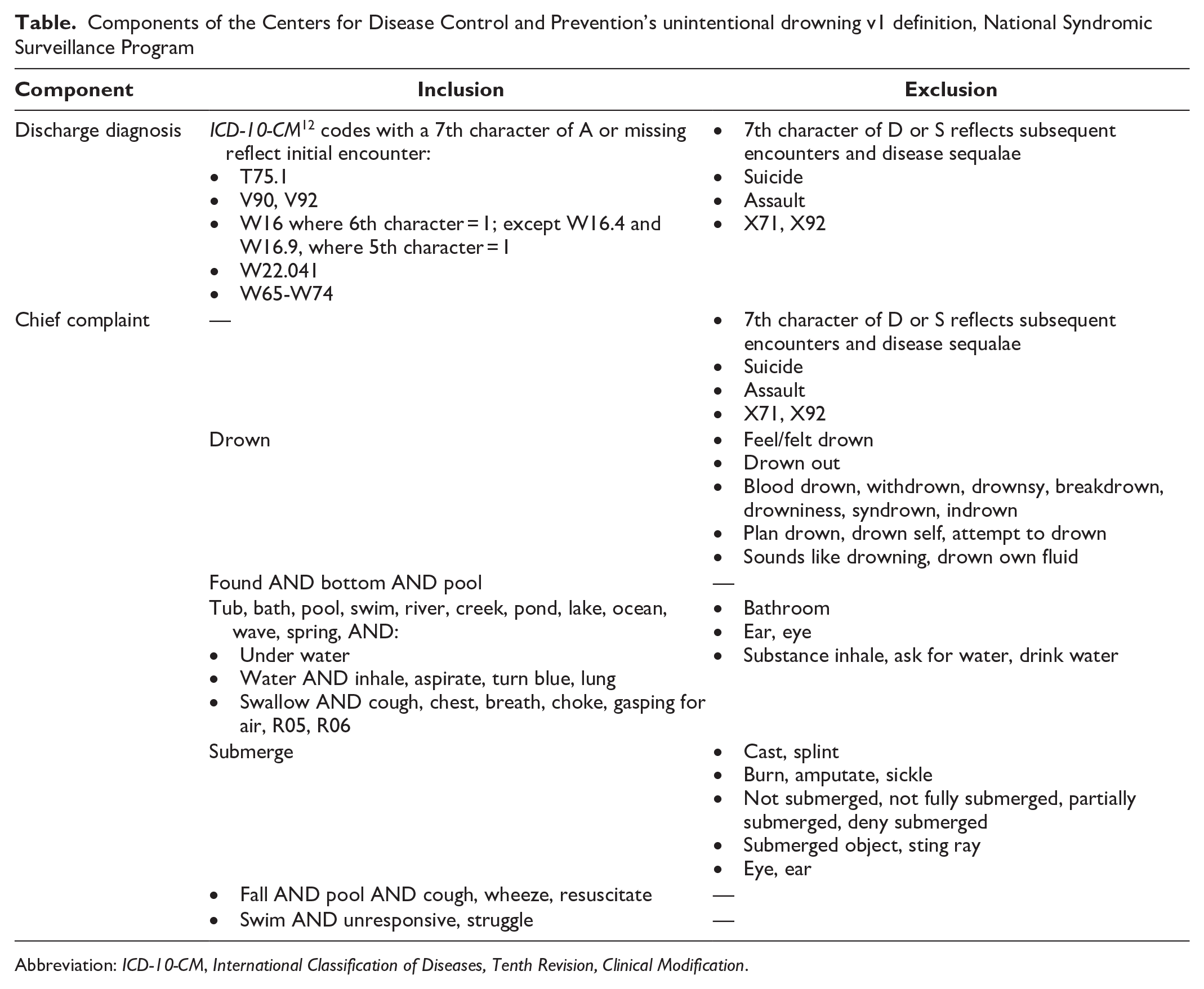
Abbreviation: ICD-10-CM, International Classification of Diseases, Tenth Revision, Clinical Modification.
Centers for Disease Control and Prevention’s unintentional drowning v1 definition, National Syndromic Surveillance Program a
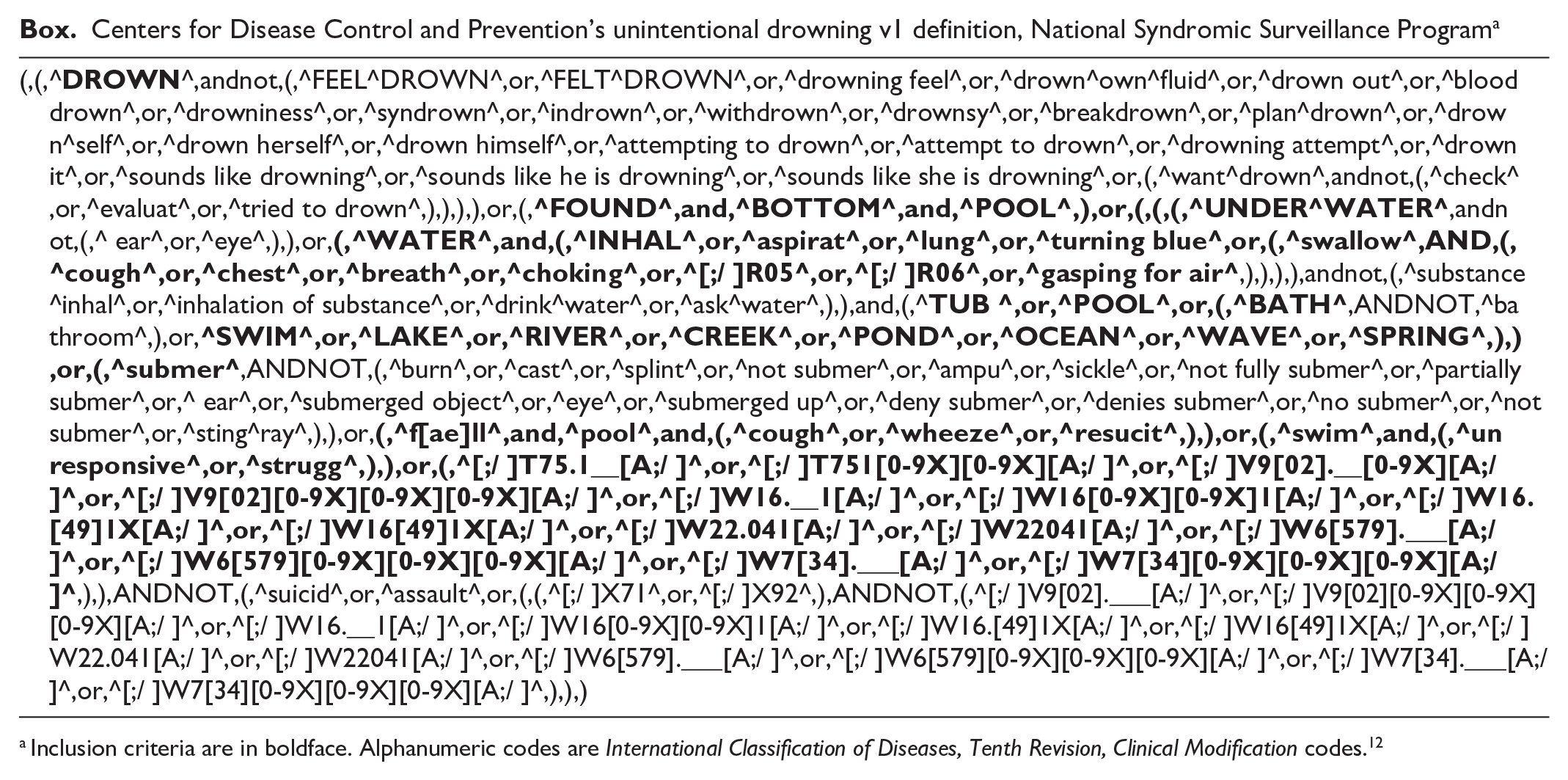
Inclusion criteria are in boldface. Alphanumeric codes are International Classification of Diseases, Tenth Revision, Clinical Modification codes. 12
To evaluate the performance of the unintentional drowning definition, 2 epidemiologists (B.M., T.C.) independently manually reviewed and labeled a random sample of 1000 ED visits in 2019 captured by the unintentional drowning definition as 1 of the following: likely drowning, possibly drowning, and likely not drowning. We labeled visits “likely drowning” if (1) both the discharge diagnosis codes and chief complaint terms included drowning terms or (2) only 1 field was available and it included drowning terms. We labeled visits “possibly drowning” when the discharge diagnosis codes and the chief complaint terms were both available but did not match—for example, when the chief complaint mentioned only limb injuries but the discharge diagnosis field included an unintentional drowning code. We labeled visits “likely not drowning” when chief complaint terms were misspelled or used incorrectly and therefore matched our definition (eg, “drowning in work”). We also coded drowning visits “likely not drowning” that appeared to be subsequent encounters or follow-up visits because they did not meet the inclusion criteria of “initial encounter.” Finally, although we excluded terms and codes related to suicide and assault, some drowning visits appeared to be intentional and were also labeled “likely not drowning.” We compared the categorization of the 1000 ED visits and discussed discrepancies between the reviewers (5.6% of visits; Cohen k = 0.77) until we reached consensus.
We analyzed counts and rates of all unintentional drowning–related ED visits captured by the definition from 2019 through 2022 overall, by sex, and by age group (<1-4, 5-17, 18-44, 45-64, ≥65 y). We calculated rates as the number of drowning-related ED visits per 100 000 ED visits. We analyzed and presented counts alongside rates because of a significant decrease in ED visits in NSSP data (the denominator of the rate) during March and April 2020 as compared with 2019. 13 Previous studies of NSSP data during the COVID-19 pandemic found that analyzing counts and rates of injury-related ED visits provides context to (1) whether changes in rates were the result of increases or decreases in the number of injury-related ED visits specifically or (2) whether changes were driven by decreases in people seeking care from EDs during the pandemic.8,9 We compared differences in 3-year rates among demographic groups using z tests. We conducted tests of independence between the monthly numbers and rates of drowning-related ED visits in 2020, 2021, and 2022 as compared with 2019 by fitting a Poisson log-linear model and adjusting for multiple comparisons using Bonferroni adjustments. We fit separate models to analyze data overall, by sex, and by age group. We fit models using SAS studio version 3.8 (SAS Institute Inc). We used data quality filters in the analysis to include EDs that consistently reported (coefficient of variance <35) to NSSP and provided informative discharge diagnosis codes (informative ≥65% on average each week). Using these data quality filters limited our analysis to 61.9% of EDs (2342/3783) reporting visits to NSSP each week from 2019 to 2022. Institutional review board approval was not required. The Centers for Disease Control and Prevention (CDC) considers data from NSSP public health surveillance to not involve human subjects research.
Results
Validation of Unintentional Drowning Definition
Among the sample of 1000 drowning-related ED visits that were captured by the unintentional drowning definition and manually reviewed, 860 (86.0%) were likely related to an initial unintentional drowning. An additional 95 (9.5%) ED visits captured by the definition were possibly related to an initial unintentional drowning. For example, “V92.09XA” in the discharge diagnosis field and “abrasion to forearm” in the chief complaint field were possibly related to an unintentional drowning because the discharge diagnosis field contained the ICD-10-CM code V92, which indicates drowning due to a fall off a watercraft, but the chief complaint field does not include drowning-related symptoms. Additionally, 45 (4.5%) ED visits were likely not related to an initial unintentional drowning—for example, those related to intentional drowning (eg, attempted to drown cousin) and those in which drowning-related terms were used to describe other conditions (eg, drowning in sleep, acid reflux).
Description of Unintentional Drowning–Related ED Visits
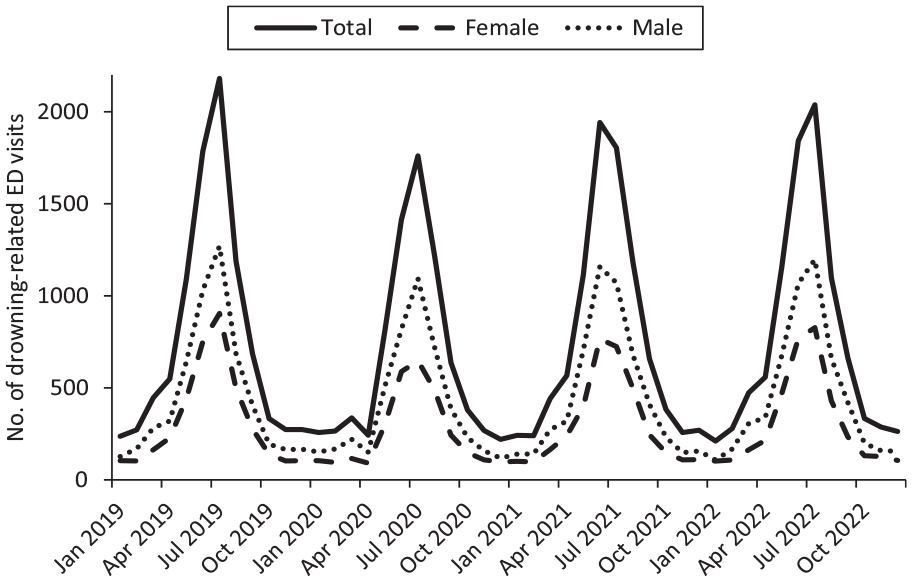
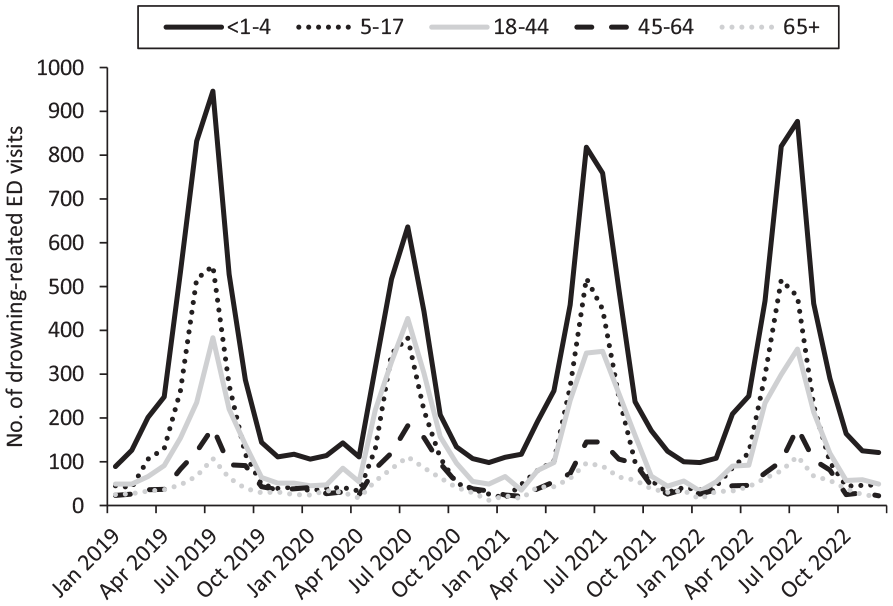
From 2019 through 2022, a total of 35 431 ED visits related to unintentional drowning occurred (10.71 per 100 000 ED visits; eTable 1 in Supplemental Material). Males had a higher rate of drowning-related ED visits than females (14.04 vs 7.84 per 100 000 ED visits) (eTable 2 in Supplemental Material). Children aged <1 to 4 years had the highest rates of drowning-related ED visits (65.61 per 100 000 ED visits) followed by children aged 5 to 17 years (24.47 per 100 000 ED visits). Overall and across sex and age groups, monthly rates of drowning-related ED visits peaked in July each year, except among all groups in 2021 and among children and adolescents aged 5 to 17 years in 2022, when rates peaked in June (Figures 1 and 2).
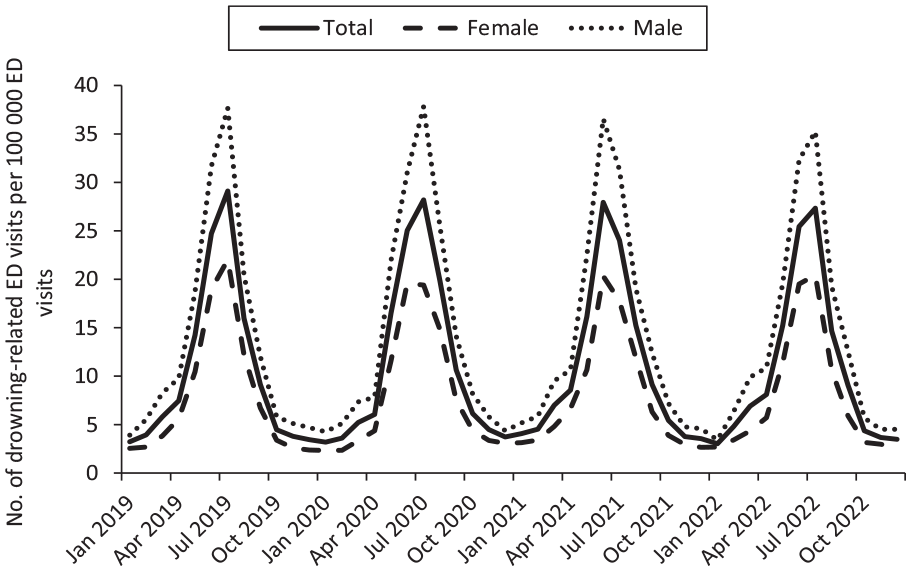
Monthly ratea of unintentional drowning–related EDb visits, overall and by sex, NSSP, United States, 2019-2022. Abbreviations: ED, emergency department; NSSP, National Syndromic Surveillance Program.
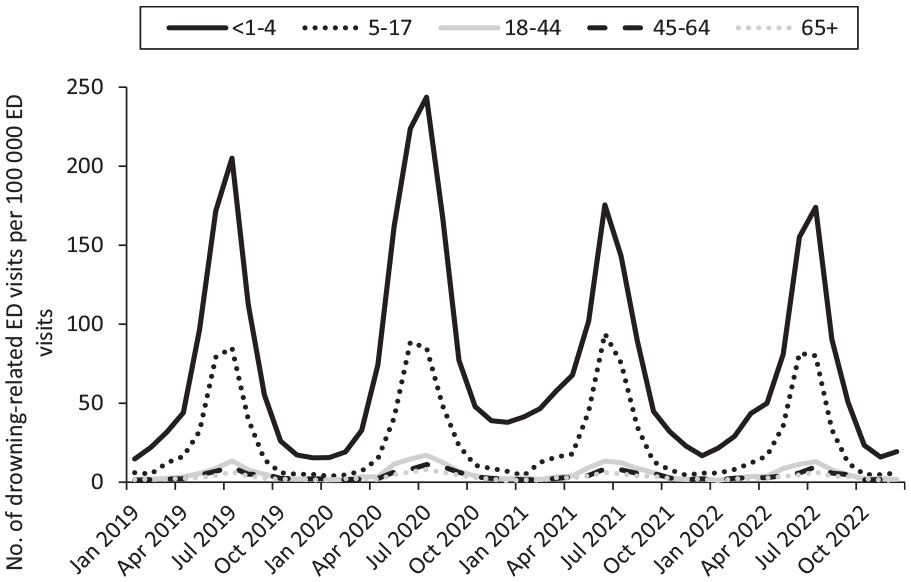
Monthly ratea of unintentional drowning–related ED visits,b by age group, NSSP, United States, 2019-2022. Abbreviations: ED, emergency department; NSSP, National Syndromic Surveillance Program.
Overall and by sex, monthly rates of drowning-related ED visits were similar in 2020, 2021, and 2022 as compared with 2019, except for August 2020, October 2020, and June 2021, when rates overall and among males were higher than in the same months in 2019. Rates among males were also higher in May 2021 than in May 2019. Among males and females, rates of drowning-related ED visits were lower in July 2021 than in July 2019 (Figure 1), and the number of drowning-related ED visits was lower from April 2020 through July 2020 and in July 2021 than in the same months in 2019 (Figure 3).
Monthly count of unintentional drowning–related EDa visits, overall and by sex, among EDs consistently reporting to NSSP, United States, 2019-2022. Abbreviations: ED, emergency department; NSSP, National Syndromic Surveillance Program.
Rates of drowning-related ED visits among children aged <1 to 4 years were higher from April 2020 through April 2021 and lower in July and August 2021 and July and August 2022 than in the same months in 2019 (Figure 2). However, the number of drowning-related ED visits was lower among children aged <1 to 4 years from April through July 2020, in September 2020, and in July 2021 than in the same months in 2019 (Figure 4). Among children and adolescents aged 5 to 17 years, rates of drowning-related ED visits were higher in September 2020 and February and May 2021 than in these same months in 2019, and the number of ED visits was lower from March 2020 through July 2020 and in January 2021 than in the same months in 2019. Among adults aged 18 to 44 years, rates of drowning-related ED visits were higher from May through August 2020 and in October 2020, May and June 2021, and May 2022 than in the same months in 2019. Additionally, the number of drowning-related ED visits among adults aged 18 to 44 years was higher in May, June, and August 2020, as well as May and June 2021 and May 2022, than in the same months in 2019.
Monthly count of unintentional drowning–related EDa visits, by age group, among EDs consistently reporting to NSSP, United States, 2019-2022. Abbreviations: ED, emergency department; NSSP, National Syndromic Surveillance Program.
Discussion
Most ED visits captured by the CDC unintentional drowning v1 definition were likely related to unintentional drowning. However, the definition did capture some ED visits where it was challenging to determine if they were truly related to unintentional drowning; it also captured a small number of ED visits that may have been related to intentional drowning or subsequent ED visits for drowning. The unintentional drowning definition was designed to maximize sensitivity, so it is expected that some of the visits captured by the definition may not be true unintentional drowning–related ED visits. Rates of drowning-related ED visits were highest among males, among children aged <1 to 4 years, and during summer months. These demographic trends are consistent with other reports.3,14
The number of drowning-related ED visits was lower among children aged <1 to 4 years from April through July 2020 than during these months in 2019. However, the rate of drowning-related ED visits among this age group was higher from April 2020 to April 2021. The higher rates of drowning-related ED visits among this age group may have been driven by the significant decrease in overall ED visits (the denominator of the rate) that occurred in NSSP data during the beginning of the COVID-19 pandemic (March and April 2020), particularly among children. 13 The largest declines in ED visits among children were for influenza and other respiratory conditions, otitis media, nausea and vomiting, abdominal pain, and fever. 13 Notably, while the number of drowning-related ED visits and all ED visits among children decreased during the early months of the pandemic, the number of drowning-related ED visits decreased to a lesser extent than overall ED visits. This finding could suggest that parents felt that some of the previously mentioned conditions could be addressed in primary or urgent care settings during the COVID-19 pandemic but that drowning-related visits may be more severe, requiring treatment in the ED. Among adults aged 18 to 44 years, the number of drowning-related ED visits was higher in May, June, and August 2020, and rates of drowning-related ED visits were higher from May through August 2020 than during these months in 2019. Given that drowning death rates increased 44% among people aged 20 to 24 years and 29% among people aged 25 to 29 years from 2019 to 2020, 14 it is not surprising that drowning-related ED visits may also have increased in this age group.
Drowning surveillance data have been used in jurisdictions to inform prevention strategies. For example, data on drowning deaths from child death reviews conducted in Washington State from 1999 to 2003 were used to launch a drowning prevention campaign, increase lifeguard staffing, implement a lifejacket loaner program, work with state officials to enforce pool fencing codes, and draft legislation to prohibit swimming in dangerous waterways. 15 If the increase in the rates of drowning-related ED visits among adults aged 18 to 44 years in 2020 had been detected by using syndromic surveillance in near-real time, this increase could have led health departments to implement timely interventions to decrease the number of drowning-related ED visits in this age group during the early months of the COVID-19 pandemic. Drowning-related deaths among adults most often occur in natural water, such as lakes, rivers, and oceans. 3 Drowning prevention strategies could have included (1) reminding swimmers about the dangers of swimming in natural water settings without the presence of lifeguards, 16 the dangers of swimming or boating while under the influence of alcohol, 17 and the importance of wearing a lifejacket when boating or swimming in natural water 18 ; (2) increasing lifeguard staffing; and (3) providing or increasing the number of lifejacket loaner stations. 15 Drowning rates among adults aged 18 to 44 years continued to be higher in May and June 2021 and May 2022 than in the same months in 2019. The unintentional drowning definition was added to the ESSENCE platform in June 2022 and is now available for health departments to use to monitor drowning-related ED visits in their jurisdictions in near-real time to help inform timely drowning prevention interventions in the future.
Limitations
This study had several limitations. First, NSSP is a convenience sample of EDs willing to participate and is not nationally representative. Approximately 76% of EDs in the United States participated in NSSP at the time of our analysis (July 2023), 7 and we used data from 61.9% of those EDs on average each week. EDs that participate in NSSP and those that consistently provide information to NSSP might differ from EDs that do not participate. Second, we did not describe the rates and numbers of drowning-related ED visits by race and ethnicity because of inconsistent reporting of these variables from 2019 through 2022. Data on race and ethnicity in NSSP improved during the study period. State and local health departments may want to consider describing drowning-related ED visits by race because some racial and ethnic groups have higher rates of drowning than others. 2 Third, because the goal of this definition was to maximize sensitivity, the ICD-10-CM code T75.1 was included in the definition even though this code could be used to indicate intentional and unintentional drowning. Although we excluded visits where T75.1 was used in conjunction with intentional drowning codes or where the chief complaint field mentioned suicide, self-harm, or assault, it is possible that some of the ED visits containing only the T75.1 code were intentional.
Fourth, although we were able to identify 4.5% of visits captured by our definition that were unlikely to be related to unintentional drowning, we were not able to measure the true drowning-related visits that our definition may have missed. Jurisdictions may consider comparing ED medical record reviews with syndromic data in their jurisdictions to determine how often drowning-related visits are missed by the unintentional drowning definition. Fifth, although data on drowning-related ED visits are available in near real time, we limited our analysis to 2022 so that we could report seasonal trends throughout each year. State and local health departments may want to consider monitoring trends in drowning-related ED visits in near real time in their jurisdictions to best inform prevention strategies.
Conclusion
Consistent with other sources of data, rates of ED visits related to unintentional drowning were highest among children aged <1 to 4 years and among males and were most likely to occur during the summer months, peaking in June or July. Drowning-related ED visits among adults aged 18 to 44 years were higher during the summer months in 2020 and 2021 than during the same months in 2019. State and local health departments can use the CDC unintentional drowning v1 definition available in ESSENCE to monitor trends in ED visits related to unintentional drowning in near-real time to inform drowning prevention strategies.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241249675 – Supplemental material for Syndromic Surveillance of Emergency Department Visits Related to Unintentional Drowning, United States, 2019-2022
Supplemental material, sj-docx-1-phr-10.1177_00333549241249675 for Syndromic Surveillance of Emergency Department Visits Related to Unintentional Drowning, United States, 2019-2022 by Briana Moreland, Tessa Clemens and Nimi Idaikkadar in Public Health Reports®
Supplemental Material
sj-docx-2-phr-10.1177_00333549241249675 – Supplemental material for Syndromic Surveillance of Emergency Department Visits Related to Unintentional Drowning, United States, 2019-2022
Supplemental material, sj-docx-2-phr-10.1177_00333549241249675 for Syndromic Surveillance of Emergency Department Visits Related to Unintentional Drowning, United States, 2019-2022 by Briana Moreland, Tessa Clemens and Nimi Idaikkadar in Public Health Reports®
Footnotes
Acknowledgements
The authors acknowledge Zachary Stein, MPH, syndromic surveillance analyst and ICF contractor to the Division of Health Informatics and Surveillance, Center for Surveillance, Epidemiology, and Laboratory Services, Centers for Disease Control and Prevention, and David Zane, MS, Zoe Thompson, MPH, Ashley Hawes, MPH, and Jeff Taylor, MPH, current and former employees of Austin Public Health, for providing initial drafts of a drowning definition and their help in validating the unintentional drowning definition.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.