
Abstract
Objectives:
State, local, and federal agencies have expanded efforts to address the root causes of overdoses, including health inequity and related social determinants of health. As an Overdose Data to Action (OD2A) technical assistance provider, the Association of State and Territorial Health Officials (ASTHO) conducted the first national needs assessment to understand capacity and technical assistance needs of OD2A jurisdictions in advancing health equity.
Methods:
ASTHO designed and disseminated the OD2A Recipient Health Equity Needs Assessment (RHENA) to 66 OD2A-funded jurisdictions from February to March 2022. OD2A principal investigators and staff were contacted via email and asked to complete the needs assessment within 6 weeks. One coder manually coded open-ended responses, conducted a thematic analysis on the qualitative data, and performed a simple frequency analysis on the quantitative data.
Results:
Fifty-two jurisdictions (78.8%) responded, including 36 states, 12 cities/counties, and 2 territories. Most jurisdictions (n = 46; 88.5%) reported having a formal or informal health equity lead in place. Common barriers included a lack of access to data sources (n = 37; 71.2%), lack of partnerships (n = 20; 38.5%), and lack of funding (n = 14; 26.9%). Respondents reported needing more information sharing among jurisdictions and partner organizations, coaching on best practices, and routine discussions such as peer-to-peer learning sessions.
Conclusion:
Findings suggest that gaps remain in programmatic policies and principles to address inequities in overdose prevention. Results are being used to identify additional technical assistance opportunities, jurisdictional capacity, and approaches to advance health equity.
The drug overdose epidemic is a public health crisis in the United States. Drug overdose–related mortality rates have risen annually; more than 1 million deaths during 2001-2021 were related to drug overdoses. 1 Most drug overdose–related deaths in recent years have involved synthetic opioids, most notably fentanyl. 2 As the drug overdose epidemic has continued, racial and ethnic disparities in drug overdose death rates have become more salient. Data from 2019-2020 showed a significant increase in overdose deaths among non-Hispanic Black (44%) and American Indian and Alaska Native (AI/AN) (39%) populations, while the rate increased by 22% among non-Hispanic White people. 2 For example, in 2020, drug overdose death rates among non-Hispanic Black people (80.9 per 100 000 population) exceeded those of non-Hispanic White people (61.3 per 100 000 population). 2 In addition, substantial racial and ethnic disparities in engagement with prevention strategies, such as naloxone access, use, and training, have been reported among people who use drugs (PWUD) because of access to and use of medical care, despite rapidly increasing rates of overdose among non-Hispanic Black people. 3
The Centers for Disease Control and Prevention (CDC), Division of Overdose Prevention funded the National Association of County and City Health Officials (NACCHO) to investigate the literature available on health equity related to overdose prevention and identify resources designed to guide health departments in addressing drug overdose through a health equity lens. 4 Research suggests that greater emphasis on upstream factors of health inequities could positively affect downstream factors. 4 In addition, most drug overdose literature has focused primarily on racial and ethnic inequities and suggests greater attention is warranted for health inequities within and across other populations, including, but not limited to, PWUD; lesbian, gay, bisexual, transgender, queer, intersex, asexual; adolescent; aging; sex; gender-based; and immigrant populations. 4
Federal, state, and local agencies are important partners in reducing overdose morbidity and mortality rates and addressing the root causes of overdose in the United States. CDC’s commitment to addressing the epidemic led to the launch of a multiyear cooperative agreement, Overdose Data to Action (OD2A), in 2019. 5 OD2A supports jurisdictions implementing strategies to collect and use data to inform drug overdose prevention efforts. Sixty-six state, territorial, and local jurisdictions were funded to track and understand emerging trends that contribute to overdose deaths. The recent increase in overdose death rates among racial and ethnic minority groups highlights a need for efforts to address health inequities in populations with increased death rates and populations historically underserved by health systems or lacking access to care. 6 However, it is unclear what barriers and facilitators exist and what could strengthen the capacity of health departments funded through OD2A to address health equity.
To understand the current health equity capacity and technical assistance needs of OD2A jurisdictions, the Association of State and Territorial Health Officials (ASTHO), a technical assistance provider for OD2A, launched the first national health equity needs assessment for overdose prevention. The needs assessment was created to identify and summarize gaps, technical assistance needs, and jurisdictional capacity among OD2A jurisdictions, including skills, cultural competence, and knowledge, regarding health equity. In addition, the needs assessment identified promising approaches to embed health equity into overdose prevention work. ASTHO and other partners are using these findings to provide technical assistance to enhance prevention and surveillance approaches in applying health equity principles.
Implementing health equity principles in overdose prevention provides an opportunity to distribute resources and understand community assets to support jurisdictional needs more equitably, thereby decreasing disparities in overdose and improving health outcomes. By prioritizing and infusing health equity principles throughout agency and partner activities and policies, a broader approach and wide-ranging impact could be realized. 7 Infusing health equity principles in the work is particularly done through supporting data and evidence to improve implementation of evidence-based interventions. Many of these interventions involve at least 1 of the following components: increasing coordination, collaboration, and integration to reduce barriers and expand access to care and treatment among all populations; reducing stigma among health care providers, peers, and the community; and implementing policies to reduce stigma.
Based on a review of the literature and gaps identified, we summarized and updated a national snapshot of health equity capacity and technical assistance needs among health departments working to prevent overdose deaths and described potential strategies to overcome barriers to addressing health equity.
Methods
ASTHO designed the OD2A Recipient Health Equity Needs Assessment (RHENA) to collect data from OD2A-funded jurisdictions in 4 domains: (1) health department capacity and readiness to incorporate health equity into their work, (2) identification of staff knowledge and gaps, (3) program planning and development, and (4) partner engagement. The assessment was deemed a nonresearch activity through ASTHO’s designated internal project review process; therefore, institutional review board review was not required.
The OD2A RHENA was informed by several existing health equity needs assessments, best practices, and lessons learned, including the Racial Equity Tools resource, 8 the Bay Area Regional Health Inequities Initiative, 9 a Health Equity at Work Skills Assessment from the National Association of Chronic Disease Directors, 10 the Community Health Assessment and Group Evaluation Action Guide, 11 and ASTHO’s Public Health Assessment resource. 12 The assessment questions used in the analysis can be found in the Supplement.
From February through March 2022, ASTHO fielded the OD2A RHENA through the Qualtrics XM platform to all 66 recipients funded under OD2A to understand the current health equity capacity and technical assistance needs of funded recipients. OD2A principal investigators and staff were contacted via email and asked to complete the needs assessment within 6 weeks. Only 1 response per jurisdiction was accepted, and it was up to the discretion of the staff to decide who had input. Some jurisdictions had the principal investigator complete the entire assessment, while others included the principal investigator and other OD2A program staff. To ensure anonymity, the assessment did not collect demographic information other than location because the focus was on jurisdictional rather than individual capacity to implement efforts.
Email reminders were sent every 2 weeks during the open period to increase the response rate. The assessment contained 45 questions (Supplement). Question design included Likert scales, open-text responses, and multiple-choice questions. Respondents were required to submit answers to all quantitative questions; however, answering qualitative or open-ended questions was optional.
Canary Health, an ASTHO consultant, conducted a thematic analysis on May 3, 2022, to identify key themes in the qualitative data and performed a simple frequency analysis on quantitative data. The analysis was guided by an interest in understanding the current landscape of jurisdictional capacity to integrate health equity into their activities, while recognizing that more semantic levels of data may need to be analyzed for potential technical assistance opportunities. 13
One coder, a Canary Health consultant, manually coded open-ended responses using Microsoft Excel version 2206 Build 16.0.15330.20260 (Microsoft Corp). The coder grouped similar responses by words and topics of the responses used to identify key themes within each qualitative question. This grouping was less theoretical than inductive, due to the nature of the data and the interest in analyzing it to support health agency capacity rather than to prove a theory.
Results
Of all 66 recipients funded under OD2A who received a survey, ASTHO received 52 responses (78.8%). Responses were received from 36 states, 12 cities/counties, and 2 territories. Respondents were geographically dispersed among the West (n = 7), Midwest (n = 9), Southwest (n = 3), Southeast (n = 11), and Northeast (n = 8) regions.
Of the 52 respondents, 46 (88.5%) indicated that they had a formal health equity entity (ie, a health equity officer, program lead, or workgroup) in place or in progress and 3 (5.8%) reported having an informal health equity lead in place (eg, a point of contact for diversity, equity, and inclusion within a health department or program office) (Table 1).
Health equity facilitators and barriers reported among Overdose Data to Action (OD2A) recipients in 52 US jurisdictions, February 2022 a
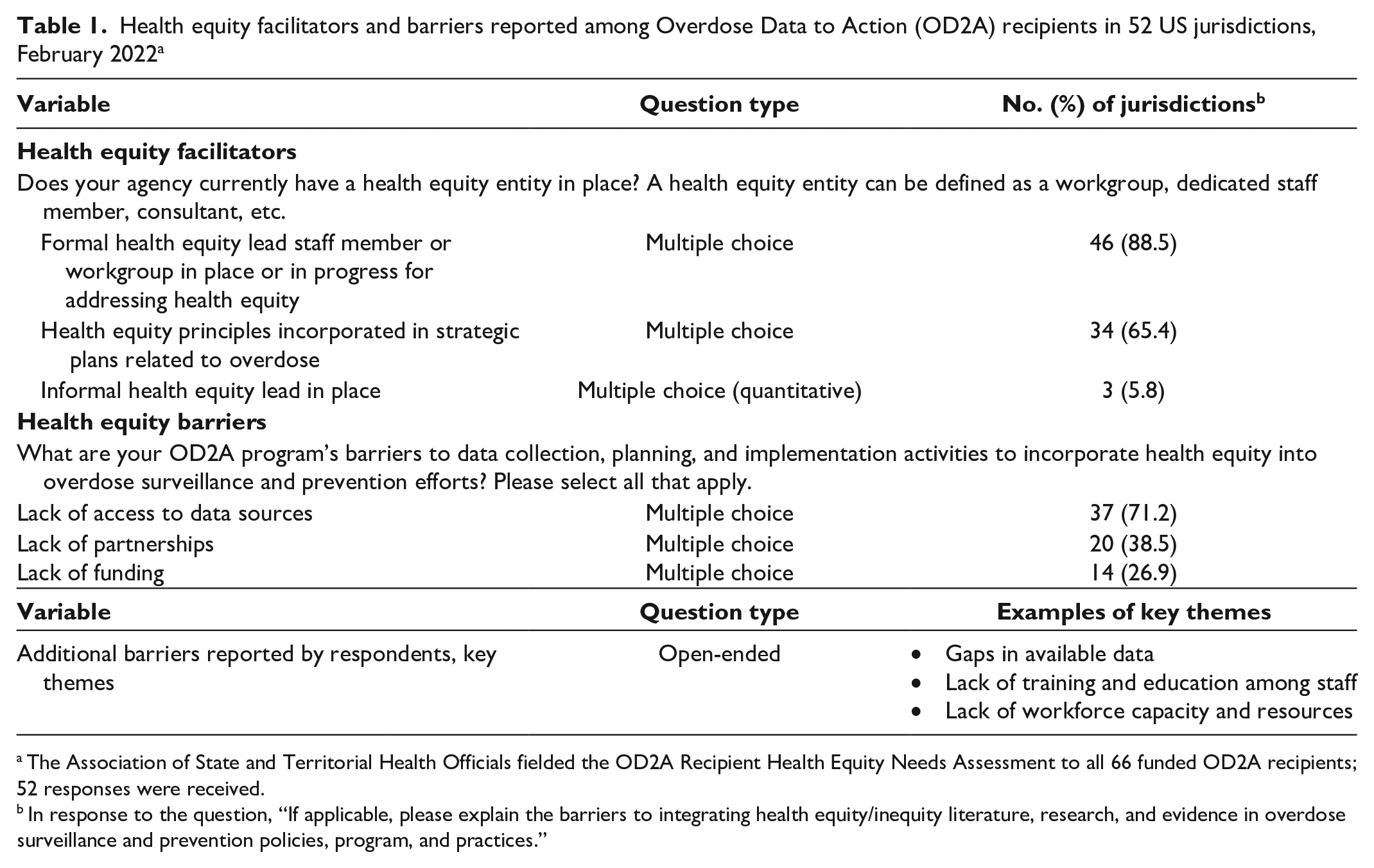
The Association of State and Territorial Health Officials fielded the OD2A Recipient Health Equity Needs Assessment to all 66 funded OD2A recipients; 52 responses were received.
In response to the question, “If applicable, please explain the barriers to integrating health equity/inequity literature, research, and evidence in overdose surveillance and prevention policies, program, and practices.”
Common barriers reported by jurisdictions included a lack of access to data sources (n = 37; 71%), lack of partnerships (n = 20; 38%), and lack of funding (n = 14; 27%) (Table 1). One respondent stated that “barriers in overdose surveillance include a gap in available data that impact health equity. Baseline data [are] needed to better understand needed improvements” (Table 2). Another respondent stated, “The real barrier would be the lack of information or education on health equity in general.” In reference to low workforce capacity, 1 respondent stated, “Barriers to providing health equity services include not a large enough workforce focused on health disparities.” Resistance to address health inequities due to factors such as the political landscape and competing priorities were also reported by respondents as barriers. Respondents reported a lack of sufficient health equity and cultural competency resources, education, and technical assistance as barriers to fully understanding the concepts and methods to incorporate health equity and cultural competency into their work. Despite jurisdictions having health equity representatives and a strong commitment to addressing health equity and issues related to the social determinants of health, analyses indicated that only 65% of respondents included these principles into their strategic plans related to overdose (Table 1).
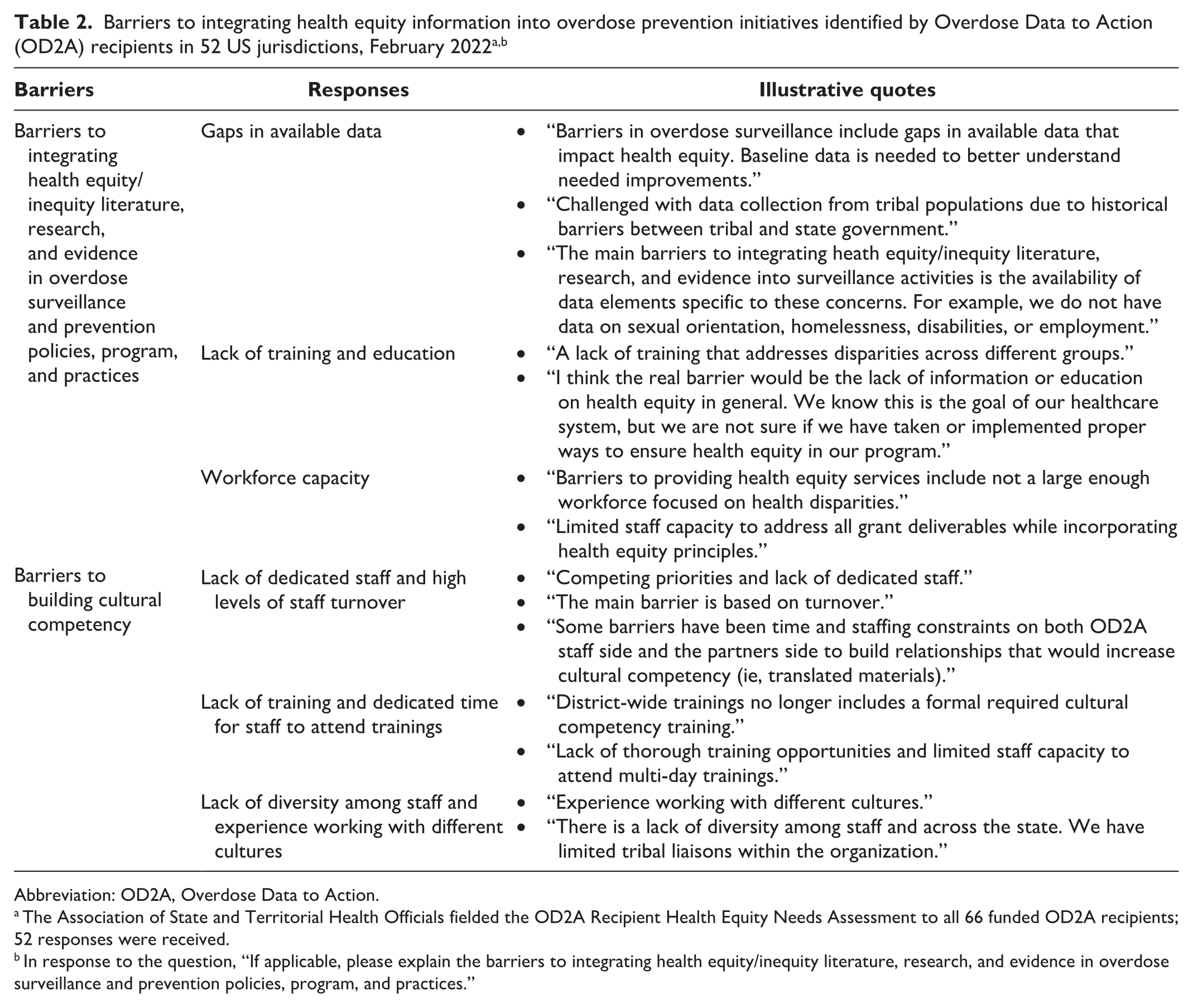
Abbreviation: OD2A, Overdose Data to Action.
The Association of State and Territorial Health Officials fielded the OD2A Recipient Health Equity Needs Assessment to all 66 funded OD2A recipients; 52 responses were received.
In response to the question, “If applicable, please explain the barriers to integrating health equity/inequity literature, research, and evidence in overdose surveillance and prevention policies, program, and practices.”
Respondents also identified several technical assistance needs (Table 3). Respondents suggested that program leads could facilitate information sharing among jurisdictions and partner organizations to support opportunities to learn from work in the field. They indicated a need for coaching on best practices and the need for routine discussions such as peer-to-peer learning sessions or community of practice calls. One respondent indicated a need for opportunities to “share examples of how other jurisdictions effectively incorporate/operationalize health equity into their programming.” Finally, respondents highlighted access to information, resources, and education about health equity and cultural competence as an important need to help staff fully comprehend and integrate health equity into their work.
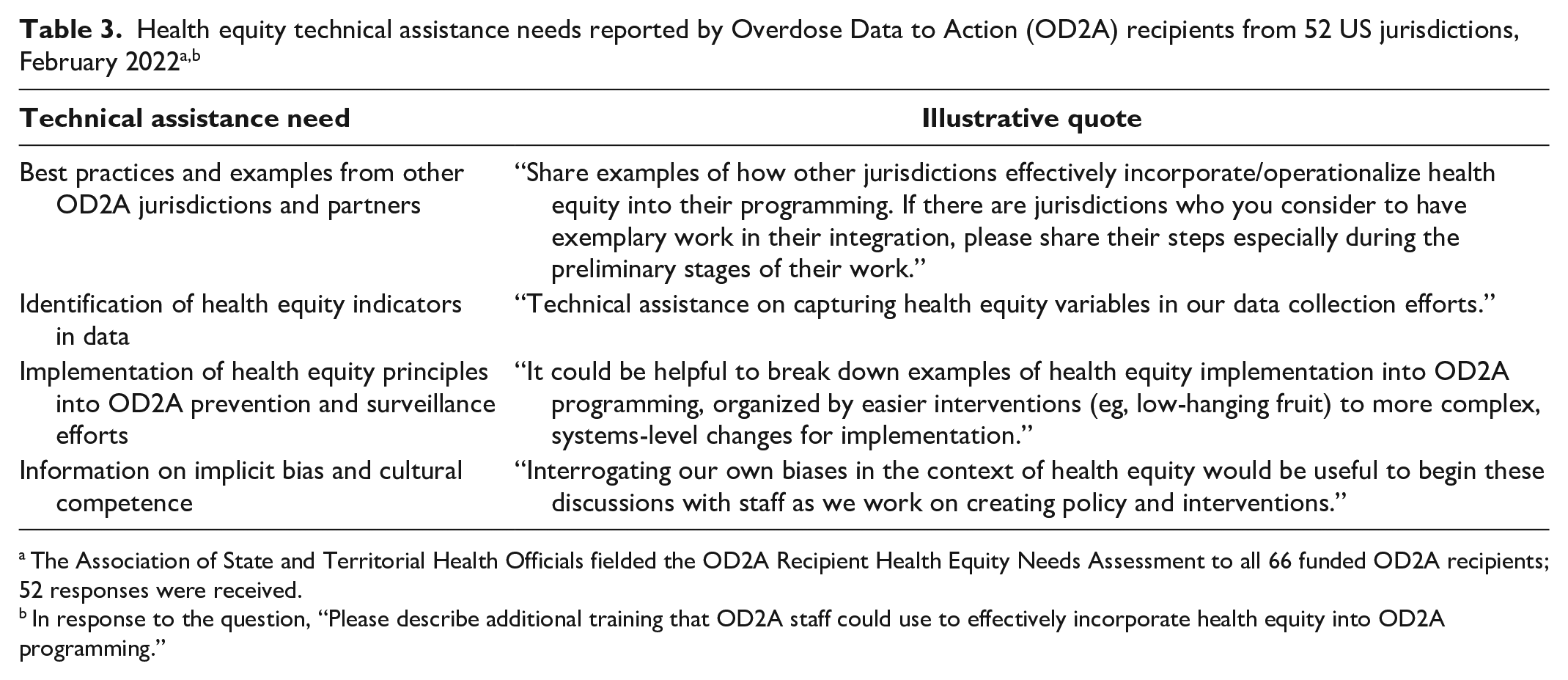
The Association of State and Territorial Health Officials fielded the OD2A Recipient Health Equity Needs Assessment to all 66 funded OD2A recipients; 52 responses were received.
In response to the question, “Please describe additional training that OD2A staff could use to effectively incorporate health equity into OD2A programming.”
Discussion
Although many OD2A jurisdictions have begun to address and incorporate health equity principles into their overdose initiatives, findings suggest that gaps remain in programmatic policies and principles, specifically, workforce capacity, data access to inform implementation efforts, and resources to address inequities in overdose prevention.
Building Workforce Capacity
Our findings indicate that recipients intended to incorporate health equity principles into overdose prevention strategic plans. Having dedicated health equity staff could help advance health equity, but based on needs assessment results, not all recipients have a lead entity in place; increasing the public health workforce with health equity experts or champions is an area of opportunity. This point is in alignment with the NACCHO environmental scan that found having quality staff with health equity expertise working in drug overdose prevention was an important resource and deemed a promising practice by health departments. 6 Consistent with building health equity workforce capacity as a strength, another study posited that health department practitioners who rated their work unit with a strong commitment to health equity also rated smaller gaps in skills, and those that perceived their work unit as actively working toward advancing health equity believed their leaders to be high quality and effective at change management. 14 Collaboration with health equity champions and building workforce capacity may help with sustainability and could be an area of opportunity to invest resources.
Improving Data Infrastructure
Jurisdictions could use data to identify population health disparities to demonstrate the importance of integrating health equity efforts. However, most respondents reported lack of access to data sources to identify social determinants of health indicators as a primary barrier for planning and implementing health equity efforts. Continued CDC funding presents the opportunity for state and local health departments to build their data infrastructure to surveil priority populations and encourages localities to implement their own community needs assessment with health equity fundamentally interwoven. According to an environmental scan conducted by NACCHO, respondents from health departments reported access to data as a “valuable and near-universal resource to inform programming and policy-making.” 6 The importance of data access noted in the environmental scan coincides with improved data collection as a priority to reduce morbidity and mortality by building overdose tracking into existing surveillance systems or linking information systems to create dashboards. 15 Building data infrastructure is an important way to capture evidence of the long-standing health disparities and inequities that exist in communities. Through key partnerships, barriers to enhanced data access, surveillance, and data quality among OD2A recipients can be reduced. Recently, CDC and OD2A jurisdictions have been working to gain access to multiple data sources and create key performance measures to provide more access and create linkages to data on the social determinants of health.
Enhancing Technical Assistance
Many recipients were grappling with other barriers, including lack of health equity educational trainings, resources, and integration methods. These findings reflect similar barriers and needs found in the literature pertaining to health departments implementing health equity efforts. Sokol et al 16 conducted key informant interviews with local health departments in North Carolina and found that all respondents stated health equity was the aim of their organizational work, but several surmised that “understanding of health equity was limited across the organization.” Thus, health departments and others may benefit from knowledge and training on how to incorporate health equity in policies, programs, and practices. Such findings could inform the creation of various technical assistance resources specific to the needs of OD2A recipients. Given what we have learned from the needs assessment results and literature, health equity and cultural competence could be advanced through concerted efforts of alleviating barriers, addressing gaps, and providing technical assistance for overdose initiatives.
Limitations
One strength of our study was the high response rate and the wide range of domains in the assessment. However, our review had several limitations. First, while our review covered a broad range of domains and topics, it did not dive deeply into several of the domains. Additional assessments may further build on our understanding of the gaps identified during analysis. Second, only 1 coder analyzed the data. The use of more than 1 coder would have ensured better interrater reliability. Third, we used Microsoft Word and Excel to analyze data, but more rigorous approaches such as the Rapid and Rigorous Qualitative Data Analysis (RADaR) method could have been implemented. 17 Lastly, while the needs assessment was fielded to all OD2A-funded jurisdictions, including 2 territories, no territories responded to the assessment. In the future, data collection on gaps identified with a focus on a more contextual understanding of jurisdictional needs from local and state recipients may provide additional insight.
Public Health Implications
This needs assessment was an attempt to fill a gap in understanding the needs, barriers, and capacity of health departments to implement health equity. Needs assessments are valuable methods to measure capacity and readiness to implement health equity–related public health activities. The results identified prominent barriers, facilitators, and gaps to addressing and integrating health equity efforts in overdose prevention, which is a strength of the needs assessment. Findings can be leveraged to provide future technical assistance and inform practical implications for the field of overdose prevention that extend beyond ASTHO and CDC efforts.
The findings of the needs assessment will help identify opportunities for ASTHO, CDC, and other partners to provide technical assistance to increase health agency capacity and support integration of health equity principles into their existing and future OD2A activities. A deeper contextual understanding of each recipient could inform tailored technical assistance efforts, but knowledge on how to reach this understanding is a cyclical process. Oftentimes public health entities may use the same evidence-based interventions on all populations, but research has shown that it is more effective to tailor intervention strategies based on populations at increased risk for a condition rather than implementing a single intervention for all populations. 18 For example, interventions can incorporate culturally appropriate practices and traditions based on the unique needs and differences of individuals in racial and ethnic minority groups. 4 Although current OD2A program staff have begun to glean this information through frequent communication with recipients and findings from programmatic data, additional support and tailored actionable technical assistance efforts are needed that can be addressed by local, state, national, and federal organizations.
To begin addressing these needs, national and federal organizations can work to:
Enhance and increase workforce training opportunities to educate staff about health equity and cultural competence to increase knowledge and understanding.
Provide coaching to local and state health departments on best practices for health equity implementation by having one-on-one opportunities and technical assistance consultations to assist jurisdictions with aligning their needs.
Include more opportunities for jurisdictions to capture health equity indicators during funding announcements. CDC has recently funded 2 new opportunities, Overdose Data to Action in States 19 and Overdose Data to Action: Limiting Overdose Through Collaborative Actions in Localities, 20 to provide more funding opportunities to state and local health departments. These efforts align with a recommendation from the literature to explicitly communicate that health equity is a stated priority, 6 reiterating health equity as a new standard and the importance of using data to address health inequities.
Increase collaboration, facilitate new partnerships, and support more community-led organizations and partners to bridge a gap in health equity work to better access priority populations.
Enhance and increase training opportunities to educate staff about health equity and cultural competence to increase workforce knowledge and understanding.
Encourage peer-to-peer learning by creating communities of practice, peer-to-peer sharing, and cross-jurisdictional collaborations. Subject matter experts and health agencies with strong health equity principles can be identified.
Create more resources, such as health equity toolkits, and redistribute existing materials to help guide jurisdictions on implementation of health equity efforts.
State and local public health departments can continue to work toward incorporating health equity by:
intentionally expanding health equity efforts by identifying populations at increased risk of drug overdose,
encouraging their jurisdictions to gather more health equity data in their work, and
increasing access to needed data sources in their public health departments by creating memoranda of understanding that would allow local health departments to have direct access to their own data.
Overall, OD2A-funded jurisdictions have undertaken substantial efforts to address the social determinants of health and overcome health inequities in overdose prevention, but more tools, resources, training, and technical assistance can help implement the work.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241239905 – Supplemental material for Implementing a Needs Assessment to Advance Health Equity in Overdose Prevention and Surveillance Initiatives
Supplemental material, sj-docx-1-phr-10.1177_00333549241239905 for Implementing a Needs Assessment to Advance Health Equity in Overdose Prevention and Surveillance Initiatives by Tiffany R. Winston, Minda Reed, Marissa Roberts, Aashna Panjwani, Jennifer Farfalla, Victoria Pless, Ayana Miles, Cherie Rooks-Peck and Natasha L. Underwood in Public Health Reports
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Association of State and Territorial Health Officials.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Development of this article was in partnership with the Centers for Disease Control and Prevention’s National Center for Injury Prevention and Control, Division of Overdose Prevention and the Association of State and Territorial Health Officials.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.