
Abstract
Objectives:
The number of drug overdoses and drug-related deaths has increased across the United States in recent years. Reports of suspected opioid drug overdoses identified through emergency medical services (EMS) are valuable sources of information for shaping the public health response to drug overdoses. The objective of this study was to describe trends in the number of EMS-reported suspected opioid drug overdose events in South Carolina from 2019 through 2022.
Methods:
We included reports of suspected opioid drug overdoses if they met the definition of nonfatal opioid overdose syndrome in our analysis. We analyzed statewide data reported from EMS agencies to biospatial, Inc, from January 2019 through December 2022 to understand demographic trends for a statewide overdose and response program in South Carolina.
Results:
In 2022, a total of 11 078 suspected opioid drug overdose events, or 216.4 per 100 000 South Carolina residents, were reported by EMS. During the 4-year study period, the number of EMS-reported suspected opioid drug overdoses increased by 82%, with African American people experiencing a 133% increase and White people experiencing a 68% increase. The number of opioid overdoses increased among all age groups during the study period. Approximately 84% of opioid overdoses were reported in urban counties, but rural counties had a higher number of opioid overdose reports per capita than urban counties.
Conclusions:
Monitoring trends in suspected opioid drug overdoses allows decision makers to adjust resources and programs for overdose response and is essential for local coordinated response. Continued monitoring of trends is needed for an equitable response to prevent opioid drug overdoses.
Drug overdoses present a major public health challenge across the United States. Emergency medical services (EMS) are frequently called to the scene of an overdose to provide emergency care and transport people to a hospital if needed. The number of fatal opioid drug overdoses in the United States is increasing because of the adulteration of the nonprescription drug supply by illicitly manufactured fentanyl. 1 However, administration of naloxone by EMS providers, first responders, and laypeople can reverse opioid-induced respiratory suppression and save lives, although not every overdose involves an opioid. 2
EMS reports are used to identify suspected drug overdose events, which can provide near–real-time data about overdoses. The Opioid Emergency Response Team in South Carolina uses EMS data to respond to trends in overdose events across the state. The number and types of EMS responses allow the team to direct resources to counties and towns experiencing a substantial incidence of overdoses or unusual clusters (eg, clusters that indicate a shift in demographic characteristics or use of a novel drug). Community-level EMS data are valuable for understanding a representative geographic and demographic depiction of overdoses, especially compared with emergency department or hospital data, which can be limited because not all people who experience a drug overdose go to a hospital. 3 In addition, the narrative free-text data written by EMS providers can provide additional details about an overdose event that the patient might not remember or report.
The objective of this study was to describe trends in the number of EMS-reported suspected opioid drug overdose events in South Carolina, a state with large African American and rural populations, 2 populations in need of more equitable resource allocation. We also examined trends in naloxone administration during EMS responses to opioid drug overdose events. We sought to characterize these trends in suspected opioid drug overdoses to direct a statewide overdose prevention and response program.
Methods
EMS data are routinely reported from EMS agencies to biospatial, Inc, in partnership with the South Carolina Department of Health and Environmental Control (DHEC) Bureau of EMS and Trauma. EMS agencies are required to report all service encounters to DHEC within 72 hours. We queried these data from the biospatial, Inc, platform under DHEC governance to identify opioid drug overdose response calls during January 2019–December 2022. biospatial, Inc, provides several syndrome definitions for identifying overdose events. For our analysis, we identified opioid drug overdoses as records that met either the Virginia definition or Rhode Island definition of suspected nonfatal opioid overdose syndrome. 4 These definitions are intended to detect events on the basis of the following criteria: primary or secondary impression, naloxone administration and response, and keywords in the EMS narrative (biospatial.io proprietary syndrome definitions, version 2.12; 2022). We restricted our review to 2 types of calls: emergency response calls and intercept calls (when 2 EMS agencies respond to a call and possibly transfer a patient between providers). We extracted data on suspected opioid drug overdoses in January 2023. We excluded events where the patient was deceased on arrival but included events with either a fatal or nonfatal outcome after care. We deduplicated events to remove responses for the same date, time, and location from multiple EMS units.
We reviewed records on suspected opioid drug overdoses for naloxone administration by EMS at the scene or before arrival by a bystander. We assessed trends by month in the number of naloxone administrations recorded for each EMS report. We used population data from the US Census Bureau American Community Survey 5 to determine population denominators. We used descriptive statistics to report the number of EMS-reported suspected opioid drug overdose events by sex (male or female), race (African American, White, or Other [both Hispanic and non-Hispanic]), ethnicity (Hispanic or non-Hispanic of any race), and age (0-17, 18-24, 25-34, 35-44, 45-54, 55-64, and ≥65 years). We grouped Asian, American Indian or Alaska Native, and Native Hawaiian or Pacific Islander people into Other because of small numbers. We excluded records with unknown race from the analysis of racial trends (approximately 2.0% to 2.5% of records annually). We defined urban and rural areas for incident locations by using the 2013 National Center for Health Statistics Urban–Rural Classification Scheme, 6 consistent with data reporting by EMS providers.
This activity was reviewed by the Centers for Disease Control and Prevention (CDC) and was conducted consistent with applicable federal law and CDC policy (eg, 45 CFR part 46, 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
Results
In 2022, a total of 11 078 suspected opioid drug overdose events, or 216.4 per 100 000 South Carolina residents, were reported by EMS, which was an overall increase in incidence of 82% from 2019. Overall, adults aged 25 to 34 and 35 to 44 years most commonly experienced an opioid overdose (Figure 1). The number of opioid drug overdose events increased during the study period in each age group, notably 155% among those aged 0 to 17 years and 123% among those aged 35 to 44 years. Males represented 62.8% of opioid overdoses in 2019 and 66.1% in 2022.
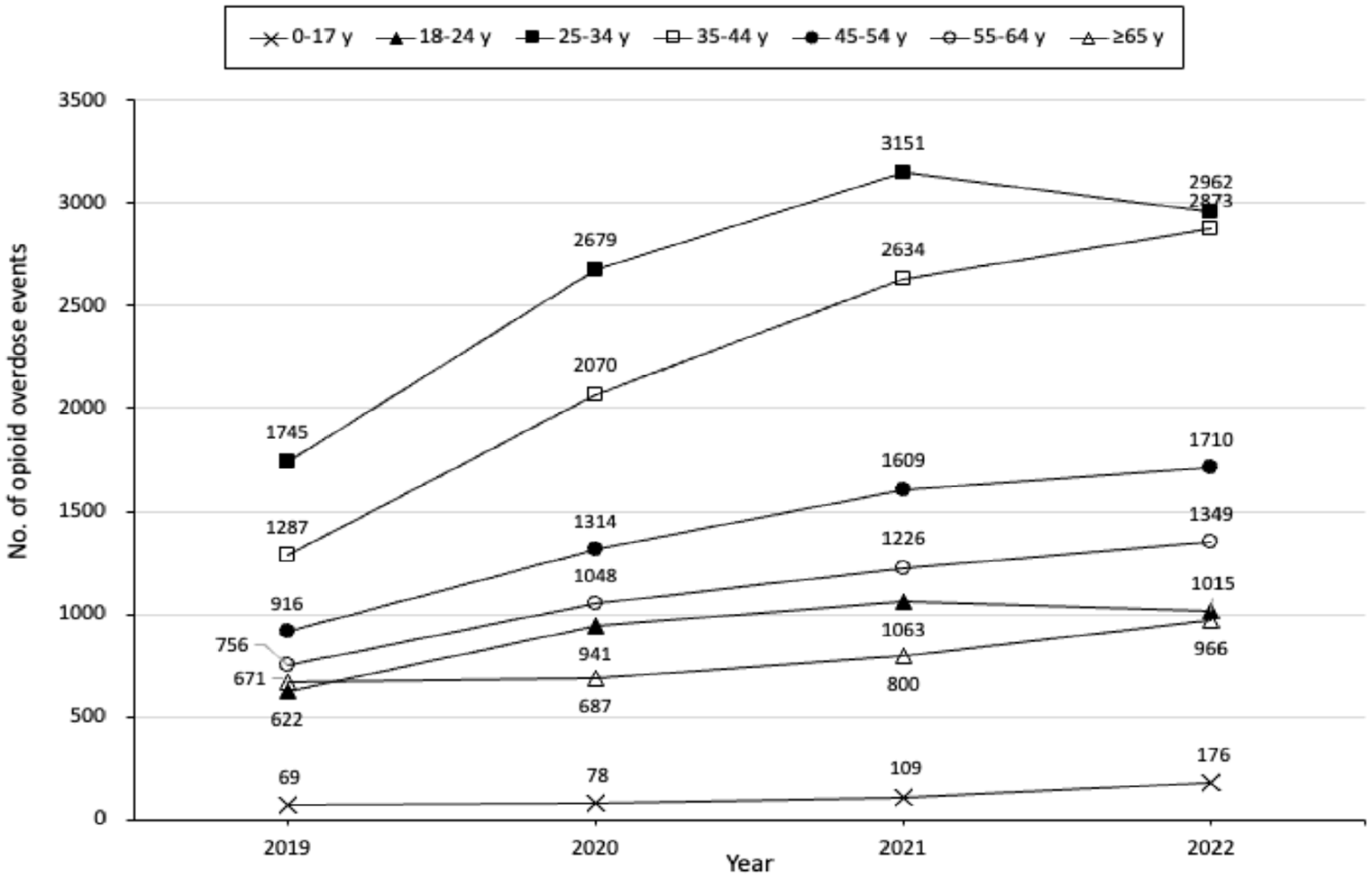
Number of suspected opioid drug overdose events reported by emergency medical services (EMS), by age group, South Carolina, 2019-2022. Data source: biospatial, Inc, in partnership with South Carolina Department of Health and Environmental Control Bureau of EMS and Trauma.
Among racial groups, African American people experienced a 133% increase and White people experienced a 68% increase in opioid overdoses from 2019 to 2022. People of Hispanic ethnicity represented a low proportion of total opioid overdoses (2.8%, data not shown) but experienced a 325% increase in opioid overdoses from 2019 to 2022, whereas non-Hispanic people experienced a 79% increase during the same period (data not shown). Fewer numbers of opioid overdoses among White males were reported in 2022 than in 2021 (Figure 2). Other racial and sex groups saw sequential annual increases in opioid overdoses during the study period.
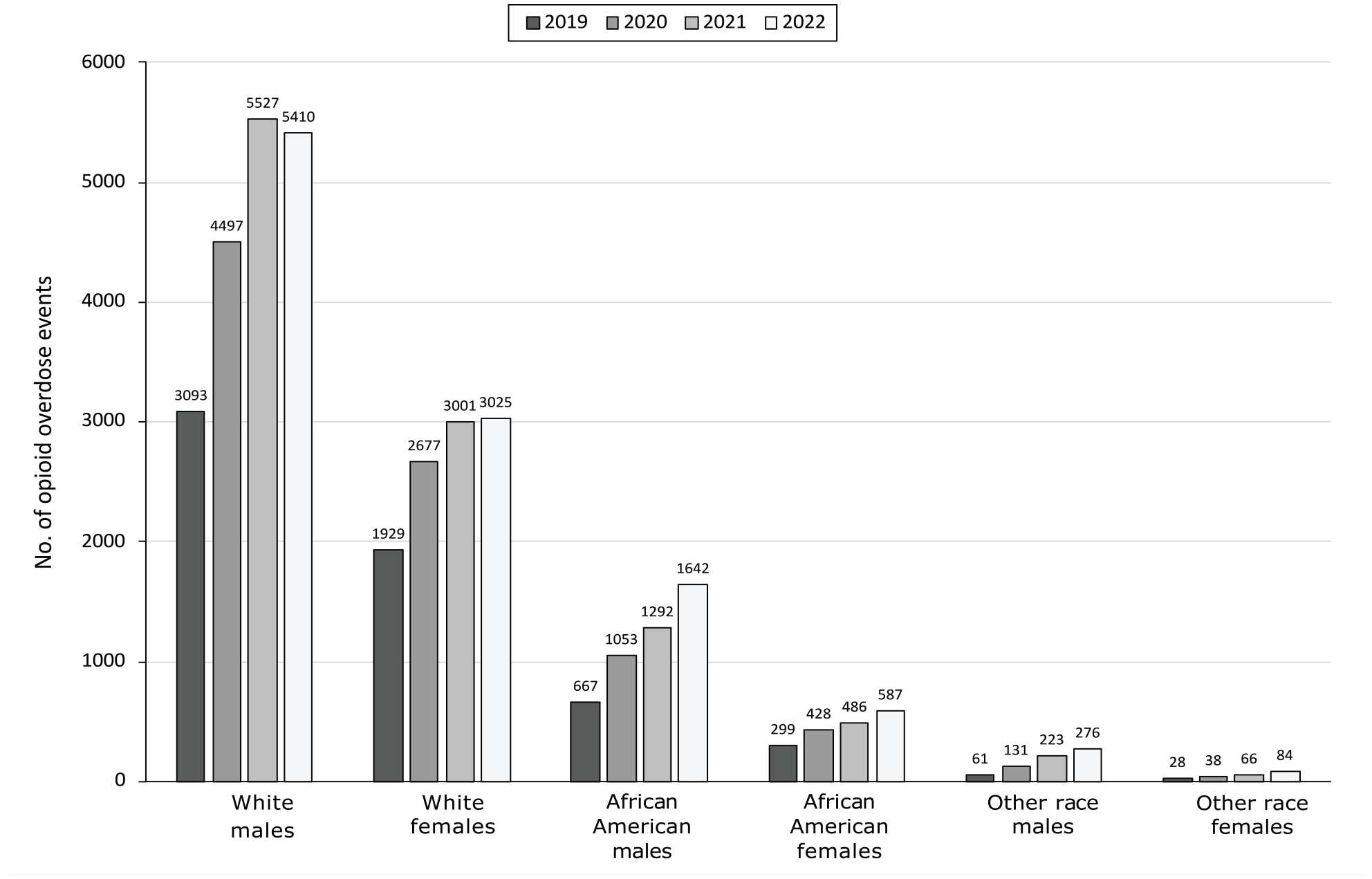
Number of suspected opioid drug overdose events reported by emergency medical services (EMS), by race and sex, South Carolina, 2019-2022. “Other” race includes Asian, American Indian/Alaska Native, Native Hawaiian or Pacific Islander, and other racial groups that had too few counts to report individually. All racial categories include both Hispanic and non-Hispanic ethnicity. Data source: biospatial, Inc, in partnership with South Carolina Department of Health and Environmental Control Bureau of EMS and Trauma.
When stratifying age groups by race and sex, we observed notable differences over time (Table). From 2019 to 2022, African American males aged 35 to 44 years had a 202% increase in opioid overdoses, although White males in the same age group had a 106% increase. From 2019 to 2022, African American females aged 25 to 34 years had a 186% increase in opioid overdoses, and White females aged 25 to 34 years had a 49% increase in opioid overdoses. From 2019 to 2022, African American males aged ≥65 years had a 116% increase in opioid overdoses, whereas White males aged ≥65 years had a 56% increase in opioid overdoses.
Number of suspected opioid drug overdose events reported by emergency medical services (EMS), by sex and race, South Carolina, 2019-2022 a
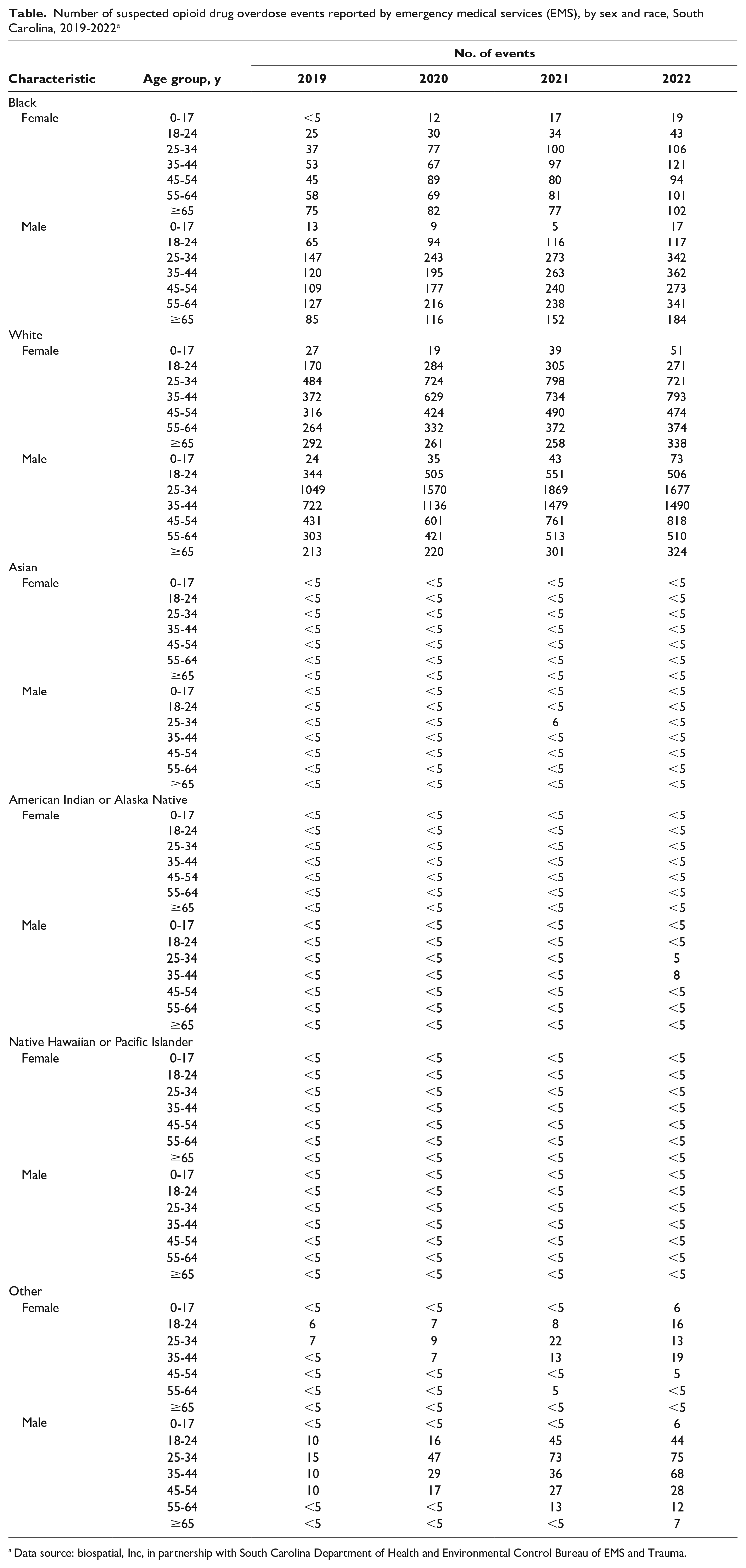
Data source: biospatial, Inc, in partnership with South Carolina Department of Health and Environmental Control Bureau of EMS and Trauma.
The number of EMS-reported suspected opioid drug overdose events varied by time in urban and rural communities (data not shown). In 2022, 84.4% of opioid overdose responses occurred in urban communities (ie, counties with ≥250 000 residents). In these communities, opioid overdoses increased by 78.4% from 2019 to 2022. Opioid overdoses in rural counties increased by 106% from 2019 to 2022. In 2022, 15.6% of opioid overdoses occurred in rural counties, and 13.6% of South Carolinians resided in 1 of the 20 rural counties as of 2020.
The number of EMS-reported suspected opioid drug overdose events in which naloxone was administered, either by EMS or before arrival, increased from a mean (SD) of 455 (60) administrations per month in 2019 to 755 (60) administrations per month in 2022 (data not shown). The steepest increase occurred from February 2020 to May 2020, from 375 to 823 administrations per month.
Discussion
Nonfatal opioid overdoses resulting from drug use in South Carolina have increased across the state since 2019. This finding is especially noteworthy among racial and ethnic minority groups and for rural communities; these groups have experienced a disproportionate increase in suspected opioid drug overdoses that can be overshadowed if trends are considered only in aggregate. Monitoring weekly trends along with longer patterns—disaggregated when possible—can help decision makers in real time. This monitoring might assist in directing short- and long-term resources, particularly to address racial and ethnic differences in treatment access 7 and longer emergency response times in rural communities. 8 Allowing communities to engage with shared data across various health, public safety, treatment, and recovery partners is essential for local coordinated response. The rapid increase in overdose reports involving fentanyl and contamination of the drug supply continues to present a public health threat and a challenge in overdose prevention and response.9,10 Use of rapidly available public health data such as EMS reports is urgently needed to tailor overdose response strategies.
The decrease in opioid drug overdose events in 2022 among White males is an encouraging signal, but unfortunately that signal was not reported across all populations. This observed decrease also indicates that evidence-based strategies to reduce overdoses and save lives should be adopted widely and focused on achieving equitable gains. Expanding harm reduction services (eg, syringe service programming, fentanyl test strips, low-barrier buprenorphine, peer recovery specialists, access to naloxone, overdose prevention education) that reach and are representative of communities that are experiencing increases in overdoses remains a priority. EMS, often regarded as community providers, can be a nimble and versatile partner in providing referrals and increasing access to care, particularly if other service organizations are not able to operate in sparsely populated areas or fully meet a community’s needs. 11 Through EMS agencies and community paramedics, SC DHEC and the South Carolina Department of Alcohol and Other Drug Abuse Services continue to promote interventions such as leave-behind naloxone, post-overdose outreach, and access to treatment to those who experience an overdose.
Limitations
This study had several limitations. First, EMS reports undercount suspected opioid drug overdose incidents because 911 is not called for every overdose, especially for overdoses among people in racial and ethnic minority groups. 12 Second, demographic information recorded by EMS might not reflect how a person self-identifies. Third, reports of naloxone administration can contain errors or be incomplete, particularly when naloxone is administered by laypeople, before EMS or other first responders arrive. Nevertheless, EMS reports are single-source data that, when combined with hospital, prescription, mortality, and qualitative data from people with lived experience, can help provide a complete picture of this public health challenge and opportunities to meet community needs.
Conclusion
The use of EMS response data for monitoring trends in opioid overdose events allows policy makers and public health officials to prioritize communities experiencing a high incidence of overdose events. In South Carolina, the increase in the number of opioid overdoses has disproportionately affected rural and racial and ethnic minority populations. Using real-time overdose event data to direct resources may assist in achieving equitable reductions in opioid overdoses.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.