
Abstract
Homelessness increases the risk of acquiring an infectious disease. We conducted a systematic review of the literature to identify quantitative data related to infectious diseases and homelessness. We searched Google Scholar, PubMed, and SCOPUS for quantitative literature published from January 2003 through December 2022 in English from the United States and Canada. We excluded literature on vaccine-preventable diseases and HIV because these diseases were recently reviewed. Of the 250 articles that met inclusion criteria, more than half were on hepatitis C virus or Mycobacterium tuberculosis. Other articles were on COVID-19, respiratory syncytial virus, Staphylococcus aureus, group A Streptococcus, mpox (formerly monkeypox), 5 sexually transmitted infections, and gastrointestinal or vectorborne pathogens. Most studies showed higher prevalence, incidence, or measures of risk for infectious diseases among people experiencing homelessness as compared with people who are housed or the general population. Although having increased published data that quantify the infectious disease risks of homelessness is encouraging, many pathogens that are known to affect people globally who are not housed have not been evaluated in the United States or Canada. Future studies should focus on additional pathogens and factors leading to a disproportionately high incidence and prevalence of infectious diseases among people experiencing homelessness.
In 2020, >580 000 people experienced homelessness in the United States 1 and >235 000 people experienced homelessness in Canada. 2 Numerous factors related to homelessness can lead to a greater risk of acquiring an infectious disease among people experiencing homelessness than among the general population. 3 Crowding, as in homeless service sites, can be conducive to transmission of respiratory infections.4,5 Lack of access to hygiene resources can lead to risk for skin and soft tissue infections (SSTIs) 6 and food- and waterborne illnesses. 7 Spending time outdoors carries a risk of exposure to vectorborne disease. 8 Substance use and transactional sex may increase the risk for bloodborne and sexually transmitted diseases. 9 Outcomes among people experiencing homelessness may be exacerbated by underlying medical conditions and limited access to medical care. 10 Despite these factors, quantitative evidence for increased incidence and prevalence of disease among people experiencing homelessness varies. To effectively develop measures to protect the health of people experiencing homelessness, a thorough understanding of the incidence and prevalence of disease is necessary. Recent reviews have provided insight on HIV,11,12 tuberculosis (TB), 13 hepatitis C virus (HCV),12,14 and vaccine-preventable diseases among people who are unhoused. 15 However, infectious diseases other than these have not been extensively reviewed.
We performed a systematic review to understand the availability of quantitative evidence about the incidence, prevalence, or measures of risk for infectious diseases among people experiencing homelessness, excluding HIV and vaccine-preventable infections. These data can provide insight into the risks and data gaps related to infectious diseases and homelessness.
Methods
Study Selection Criteria
We conducted a literature search of Google Scholar, SCOPUS, and PubMed databases (Figure). We included studies that described quantitative prevalence and risk data related to infectious diseases among people who are unhoused. We restricted articles to studies conducted in the United States and Canada and published in English from January 2003 through December 2022.
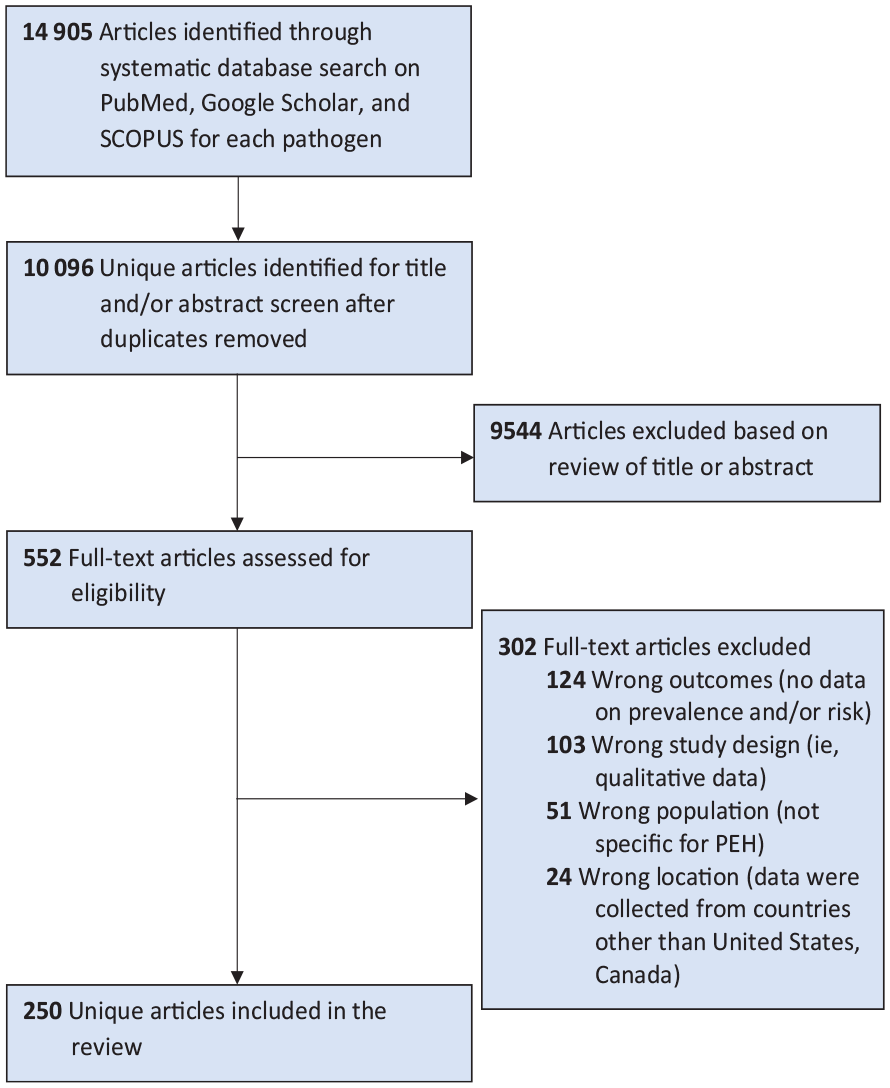
PRISMA flowchart of study selection of infectious diseases among PEH from the United States and Canada, January 2003–December 2022. Abbreviations: PEH, people experiencing homelessness; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
We excluded most vaccine-preventable infections because a systematic review of these infections was recently published. 15 We also excluded articles describing HIV incidence and prevalence alone because HIV and homelessness have been well documented.11,12 However, we included articles describing HIV and HCV coinfection or other sexually transmitted infection (STI) coinfection, as well as TB and HCV infections, because we found no systematic reviews that quantified disease risk for these pathogens among people experiencing homelessness for our review period (2003-2022) or in the same locations (United States and Canada) at the time of our literature search. We followed the PRISMA protocol (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 16
Search Strategy
We used the following search terms for each pathogen: ([homeless*] OR [roofless] OR [houseless] OR [unhoused] OR [unsheltered]) AND pathogen.
Two screeners (C.J.W. and M.M.S., A.A.M. and C.K.L., or C.S.S. and E.M.M.) independently screened titles and abstracts from each database for relevance. They compiled titles and abstracts in a spreadsheet and removed duplicates. A third investigator (either C.J.W. or A.A.M.) resolved any disagreements that could not be resolved between the screeners. Two investigators (C.J.W. and M.M.S.) independently assessed the full texts of relevant abstracts. We did not perform a meta-analysis. Per the guidelines of the Centers for Disease Control and Prevention Institutional Review Board, this study was exempt from board assessment because this project did not involve primary human data or participants.
Results
Our searches returned 14 905 records. After we removed duplicates, we screened 10 096 titles and/or abstracts and reviewed 552 full texts. After review, 250 articles met inclusion criteria, of which 216 were conducted in the United States, 32 in Canada, and 2 in both (Table, eTable 1 in Supplemental Material).
Studies that quantified the risk of infectious diseases, by pathogen, among PEH from the United States and Canada, January 2003–December 2022 a
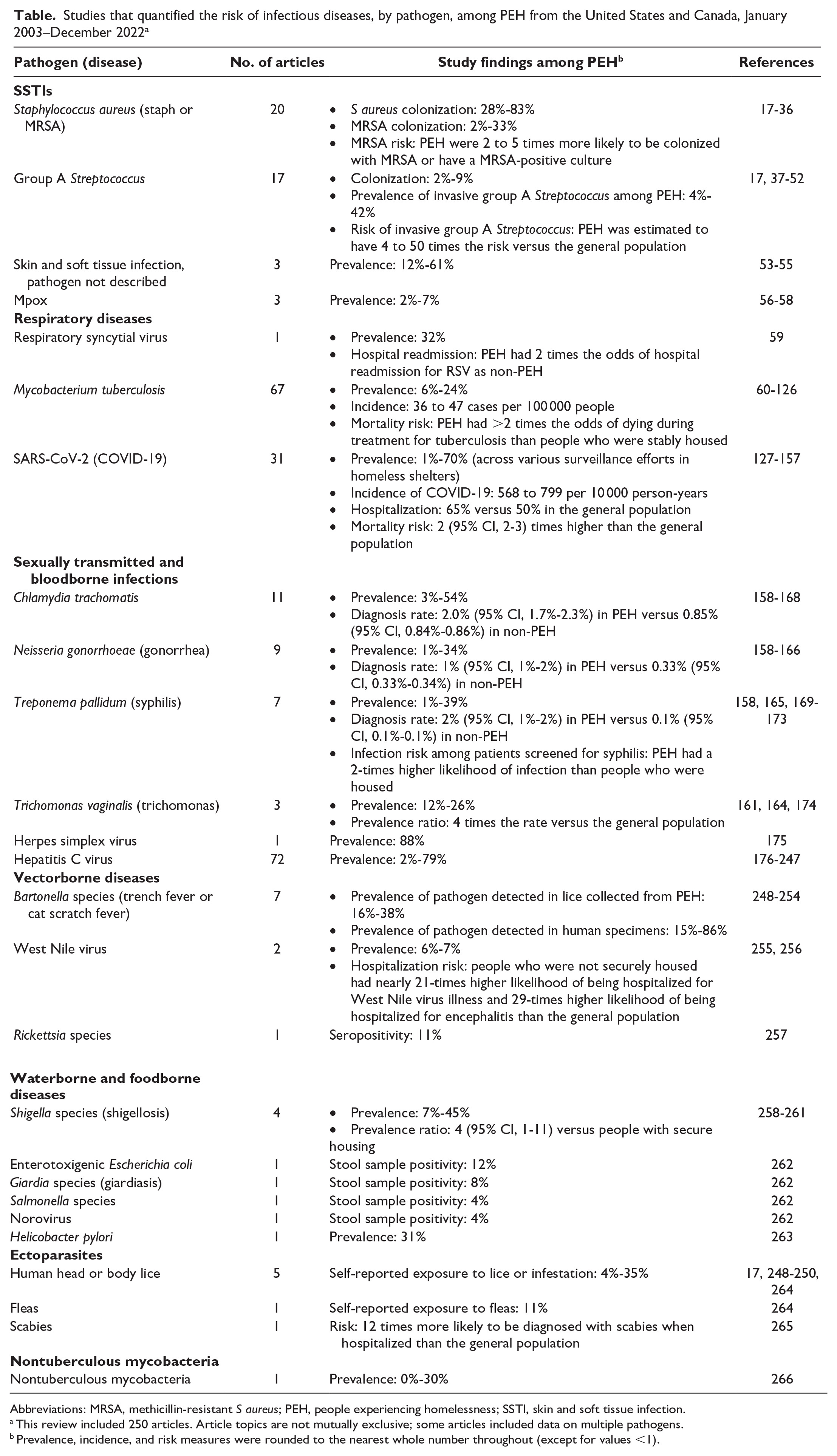
Abbreviations: MRSA, methicillin-resistant S aureus; PEH, people experiencing homelessness; SSTI, skin and soft tissue infection.
This review included 250 articles. Article topics are not mutually exclusive; some articles included data on multiple pathogens.
Prevalence, incidence, and risk measures were rounded to the nearest whole number throughout (except for values <1).
Skin and Soft Tissue Infections
Twenty articles were included for Staphylococcus aureus (eTable 2 in Supplemental Material).17-36 S aureus colonization prevalence ranged from 28% to 83% among samples of people experiencing homelessness.17-20 Methicillin-resistant S aureus (MRSA) colonization ranged from 2% to 33% within sample populations where most participants were experiencing homelessness.21-23 People experiencing homelessness were 2 to 5 times more likely to be colonized with MRSA or have a MRSA-positive culture23-25 among MRSA cases versus controls who had methycilin-susceptible S aureus 25 and among people living with HIV who reported being unhoused versus those who were housed.23,24 Risk factors for MRSA colonization included recent hospitalization or antimicrobial use, injection drug use, manipulation of infected skin (squeezing, cutting, popping), and sharing personal items (towels, clothes, razors).22,26,27
Seventeen articles related to group A Streptococcus among people experiencing homelessness were included17,37-52: 14 studies provided data on invasive group A Streptococcus (iGAS) disease and 3 provided data on colonization (eTable 3 in Supplemental Material). Colonization among people experiencing homelessness ranged from 2% to 9%.46,48,52 People experiencing homelessness were estimated to have 4 to 50 times the risk of iGAS as compared with the general population.17,42 Studies showed yearly increases of iGAS cases among people who were unhoused and greater odds for cluster-associated isolates than noncluster isolates among people experiencing homelessness.37,40
Three articles were included that did not differentiate the etiologic agent of SSTIs53-55 and showed a self-reported prevalence of 12% to 61% for SSTIs in the previous month among people experiencing homelessness (eTable 4 in Supplemental Material).
In articles related to mpox (formerly monkeypox) among people who were unhoused (eTable 5 in Supplemental Material), 2 studies reported that the prevalence of probable or confirmed mpox cases or detection of antiorthopoxvirus antibodies ranged from 2% to 7%.56,57 In a study of severe manifestations of mpox, 23% of hospitalized case patients were experiencing homelessness. 58
Respiratory Diseases
One study on respiratory syncytial virus (RSV) showed that 32% of adult patients with RSV were experiencing homelessness and that people experiencing homelessness had 2 times the odds of hospital readmission for RSV when compared with people not experiencing homelessness (eTable 6 in Supplemental Material). 59
Sixty-seven articles on TB were included in our review (eTable 7 in Supplemental Material).60-126 Outbreak investigations and retrospective medical record or surveillance system reviews were the most common study type. In San Francisco, California, from 1993 through 2005, 14% of TB cases were among people experiencing homelessness. 109 In addition, in a review of latent TB screening records, patients experiencing unstable housing were 5 times more likely to test positive than those who had stable housing. 90 US National Tuberculosis Surveillance System data showed that 6% of reported cases of TB were among people experiencing homelessness, 93 similar to a study in New York City, which found that 7% of TB cases were among people who were unhoused. 112 The annual incidence of TB disease among people experiencing homelessness from 2006 through 2010 ranged from 36 to 47 cases per 100 000 people, representing 10 times the incidence of the general population. 93 Mortality attributable to TB among people experiencing homelessness was assessed in studies from New York City and Texas, which showed that people experiencing homelessness had >2 times the odds of dying during treatment for TB than people who were stably housed.67,71 People experiencing homelessness also had greater frequency of resistant TB strains than people who were stably housed. 75
For COVID-19, 31 articles were included (eTable 8 in Supplemental Material).127-157 In a surveillance study of 8728 people hospitalized for COVID-19 in 99 counties across the United States, 2% of cases were among people who were unhoused. 136 In homeless shelters, the prevalence of SARS-CoV-2 ranged from about 1% in overall asymptomatic individuals where tests were performed for surveillance 137 to as high as about 70% of shelter clients and 17% of shelter staff during a shelter outbreak.141,147 People experiencing homelessness were also >20 times more likely to be admitted to the hospital, had 65% higher hospitalization rates, and had 2 to 5 times the mortality risk when compared with the general population.133,134,145
Sexually Transmitted and Bloodborne Infections
Eighteen articles assessed ≥1 pathogen that can cause STIs, such as Chlamydia trachomatis (n = 11 articles),158-168 Neisseria gonorrhoeae (n = 9 articles),158-166 Treponema pallidum (causative agent of syphilis) (n = 7 articles),158,165,169-173 Trichomonas vaginalis (n = 3 articles),161,164,174 and herpes simplex virus (n = 1 article). 175 Chlamydia prevalence ranged from as low as 3% to as high as 54% (eTable 9 in Supplemental Material).159,168 Gonorrhea prevalence ranged from as low as 1% to as high as 34% (eTable 10 in Supplemental Material).159,162 In San Francisco, California, 28% of people who were experiencing homelessness or unstable housing and were living with HIV tested positive for chlamydia or gonorrhea, as opposed to 13% of people living with HIV who were stably housed. 160 Women who had experienced homelessness before incarceration in correctional facilities in Rhode Island had approximately double the risk of STIs as compared with women who had not experienced homelessness before incarceration. 164 Rates of positive tests for chlamydia or gonorrhea were higher among women than among men (11% of women, 5% of men). 163
In a study of 23 cases of congenital syphilis in Indiana, 39% were among children of mothers who were experiencing homelessness or unstable housing (eTable 11 in Supplemental Material). 172 In surveillance studies, the prevalence of syphilis was 1%.165,173 Among women experiencing homelessness or unstable housing, the prevalence of T vaginalis ranged from 12% to 26%, as opposed to 3% among the general population (eTable 12 in Supplemental Material).161,164,174
The only study included for herpes simplex virus was a cross-sectional study exploring herpes simplex virus type 2 among women experiencing homelessness that showed a prevalence of 88% for immunoglobulin G antibodies specific to the virus (eTable 13 in Supplemental Material). 175
Hepatitis C Virus
For HCV, 72 articles were included in the review (eTable 14 in Supplemental Material).176-247 The most common study types were retrospective medical record reviews and prospective cohort studies. There were also numerous randomized controlled trials of antiviral treatment or intervention-based observational studies that explored HCV treatment initiation, retention, and completion. Fifteen studies estimated the odds of having a history of homelessness among people with HCV or the odds of people experiencing homelessness to have a positive HCV diagnostic test result.176,183,190,192,199,208,210,212,216,223-225,228,229,232 Of the 15 studies, 10 showed significant associations between homelessness and a positive HCV status or test result.176,183,190,192,212,216,223-225,232 An additional 13 articles examined the association between homelessness and linkage to care, initiation of direct-acting antiviral treatment, or sustained viral response to treatment.182,184,189,193,196,198,200,209,211,214,218,222,238
The prevalence of HCV varied widely depending on the study population, ranging from 2% to 79%.188,206 Intravenous drug use and sharing injection equipment were prominent risk factors for HCV infection among people who were securely housed and people who were not securely housed, in addition to HIV and HCV coinfection, birth cohort or age, alcohol and other substance use disorders, history of mental illness, and history of sex work.183,190,192,199,208,210,212,216,223-225,228,229
Vectorborne Diseases
Two studies evaluated Bartonella-infected lice carried by people who were unhoused,248,249 and 5 studies evaluated Bartonella infection among people who were not securely housed (eTable 15 in Supplemental Material).250-254 DNA extracted from lice gathered from people experiencing homelessness showed that 16% to 38% were carrying Bartonella quintana.248,249 The prevalence of B quintana among people experiencing homelessness or reports of homelessness ranged from 15% to 86%.251-253
Two studies provided data on West Nile virus (WNV) (eTable 16 in Supplemental Material). One study showed that 7% of participants were seropositive for WNV. 255 The other study showed an increased risk of hospitalization for WNV among people who were not securely housed, with an almost 21-times higher likelihood of being hospitalized for WNV illness and 29-times higher likelihood of being hospitalized for encephalitis than the general population. 256
One article on rickettsial disease met inclusion criteria (eTable 17 in Supplemental Material). Among 176 people experiencing homelessness, 11% had detectable antibodies to Rickettsia typhi or Rickettsia prowazekii. 257
Water- and Foodborne Diseases
Four articles described shigellosis outbreaks among people experiencing homelessness (eTable 18 in Supplemental Material).258-261 In 1 article that described an outbreak of 105 cases of shigellosis, 43% of cases were among people who were unhoused, and heavy rain was identified as a contributing factor to Shigella transmission. 258 People experiencing homelessness had an increased prevalence of shigellosis in an outbreak setting (prevalence ratio = 4; 95% CI, 1-11) and higher rates of hospitalization when compared with case patients who did not report homelessness.258,260
Among the articles reviewed for Escherichia coli (eTable 19 in Supplemental Material), Giardia (eTable 20 in Supplemental Material), Salmonella (eTable 21 in Supplemental Material), and norovirus (eTable 22 in Supplemental Material), no studies quantified the relative risk for these diseases among people experiencing homelessness. However, 1 study surveyed open defecation near homeless service sites and found that 12% of stool samples collected at these sites were positive for enterotoxigenic E coli, 8% were positive for Giardia species, 4% were positive for norovirus, and 3.8% were positive for Salmonella. 262
One study on Helicobacter pylori was included (eTable 23 in Supplemental Material). In a study on seroprevalence of H pylori among 100 people experiencing homelessness, rates were similar to the general population, at around 31%. 263
Ectoparasites
Five studies described the risk of ectoparasites.17,248-250,264 These studies quantified the prevalence of ectoparasites among people experiencing homelessness, with estimates ranging from 4% to 35% for lice and 11% for fleas (eTable 24 and eTable 25 in Supplemental Material). For scabies, people experiencing homelessness were 12 times more likely to be diagnosed with scabies when hospitalized than the general population (eTable 26 in Supplemental Material). 265
Nontuberculous Mycobacteria
Among people with a history of homelessness, 1 study reported that up to 30% presented with 1 of 8 nontuberculous Mycobacteria species (eTable 27 in Supplemental Material). 266
Pathogens With No Data
We did not identify articles on Campylobacter species, Listeria species, Yersinia species, Clostridium difficile, Cryptosporidium, or multidrug-resistant Enterobacteriaceae despite evidence of these infections among people experiencing homelessness in other countries, particularly in Europe.267,268 Articles pertaining to infection with Legionella species, Burkholderia species, or Human parvovirus B19 among people experiencing homelessness were not identified. Despite reported exposure to vectors by people who are unsheltered, 264 no published data in the United States or Canada were identified for Borrelia, Ehrlichia, or Anaplasma species. Our search also did not yield any articles discussing the epidemiology of other zoonotic infections, such as Brucella, Coxiella, or Streptobacillus species, among people experiencing homelessness.
Discussion
We identified increased incidence, prevalence, and measures of risk of infectious diseases among people experiencing homelessness for nearly every included pathogen. Although HIV, TB, and HCV have been well documented among people experiencing homelessness, 14 we showed many additional infectious diseases that caused a high incidence and prevalence of disease among people experiencing homelessness. Information was lacking for some infectious disease categories, such as food-, water-, and vectorborne illnesses. Understanding available data and gaps in the literature is necessary to develop inclusive infectious disease prevention programs that can reach people experiencing homelessness.
SSTIs and ectoparasites were more common among people experiencing homelessness than among the general population in nearly all included articles. Barriers to accessing hygiene facilities and proper wound care and injection drug use are reported risk factors for SSTIs among people experiencing homelessness.20,21,32,34,41 Therefore, increasing access to hygiene facilities and substance use treatment could prevent SSTIs among people who are not securely housed.
Homelessness was also associated with risk of respiratory diseases such as TB and COVID-19. During our literature search, a systematic review of literature on global COVID-19 among people experiencing homelessness had been published. 269 The most common strategies reported for COVID-19 infection prevention and control were rapid testing, expansion of noncongregate shelters, bed rearrangements to increase distancing, and reduction of staff turnover. In a systematic review of TB, the most common recommendation to reduce TB transmission was to improve ventilation systems in shelters. 270 Such practices could be considered when implementing prevention measures for respiratory diseases among people who are not securely housed, given that staying in a shelter, sharing a room with others, and staying in a place with high rates of resident turnover are reported risk factors for COVID-19,129,146,150,157 while distancing measures are protective. 141
People experiencing homelessness showed an increased risk of STIs as compared with people who were stably housed. A review of global HIV, HCV, or HIV-HCV coinfection identified a heightened risk of infections among people experiencing unstable housing or recent homelessness. 12 The experience of homelessness affected initiation, retention, and completion of HCV treatment. Similarly, a systematic review of HIV conducted in the United States and Canada concluded that a lack of stable, secure, or adequate housing is a substantial barrier to consistent and appropriate HIV medical care, access and adherence to antiretroviral medications, and sustained viral suppression and creates a risk of continued transmission. 11 These findings, among others, 111 support a need for integrating sexual health care at homeless service sites.
Although food-, water-, and vectorborne illnesses represented more than one-third (n = 9) of the number of identified pathogens with published literature for people experiencing homelessness (n = 25), they accounted for only 8% (n = 19) of the 250 articles. These topics remain understudied for this population but are a growing concern, as evidenced by a recent outbreak of locally acquired malaria in the United States, where 3 of 8 patients were experiencing homelessness. 271 Lack of access to water, sanitation, and hygiene continues to be a contributing factor for illness among people experiencing homelessness. 270
This review builds on existing knowledge about vaccine-preventable diseases. A review of vaccine-preventable diseases concluded that people experiencing homelessness have high rates of vaccine-preventable diseases but low rates of vaccination; in addition, the amount of available data on vaccination is scarce. 15 Work has been done to determine effective strategies to increase vaccination among people experiencing homelessness. Several successful strategies include having nurse-led vaccination clinics, having vaccination events in convenient locations, and offering no-cost vaccines or providing incentives. 272 The use of evidence-based methods to ensure that people experiencing homelessness have access to vaccines could address the disparities reported in vaccine coverage and disease rates.
This review had several limitations. Our search focused on studies performed in the United States and Canada, which limits the global generalizability of the results. The list of pathogens and conditions may not fully represent the number of organisms and conditions affecting people who are experiencing homelessness. Despite these limitations, our review showed that research is needed in a variety of other emerging infectious diseases, given the environmental exposure, overcrowding, and sanitation issues encountered by people experiencing homelessness.
Current knowledge gaps could be addressed through improved collection of clinical, surveillance, and research data on infectious diseases among people experiencing homelessness. The Centers for Disease Control and Prevention outlines useful considerations when ascertaining housing status and provides sample data systems that currently include a measure of homelessness. 273 Including people who are not securely housed more readily in public health data collection can promote equity by quantifying the risks associated with homelessness, informing public health prevention measures that can reach people experiencing homelessness, and improving connection and retention in treatment.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241228525 – Supplemental material for Infectious Diseases Among People Experiencing Homelessness: A Systematic Review of the Literature in the United States and Canada, 2003-2022
Supplemental material, sj-docx-1-phr-10.1177_00333549241228525 for Infectious Diseases Among People Experiencing Homelessness: A Systematic Review of the Literature in the United States and Canada, 2003-2022 by Caroline J. Waddell, Carlos S. Saldana, Megan M. Schoonveld, Ashley A. Meehan, Christina K. Lin, Jay C. Butler and Emily Mosites in Public Health Reports
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Contributions
Drs Waddell and Saldana contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided this supplemental material to give readers additional information about their work. The material has not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.