
Abstract
After a tumultuous 3 years of pandemic-, political-, and race-related unrest in the United States, the public is demanding accountability to communities of color (defined here as American Indian/Alaska Native, Asian, Black, Native Hawaiian/Pacific Islander, and Hispanic people) to rectify historic and contemporary injustices that perpetuate health inequities and threaten public health. Structural racism pervades all major societal systems and exposes people to detrimental social determinants of health. Disrupting structural racism within public health systems is essential to advancing health equity and requires organized partnerships between health departments and community leaders. As those who are most affected by structural racism, communities of color are the experts in knowing its impacts. This case study describes the King County Pandemic and Racism Community Advisory Group (PARCAG) and its use of an innovative accountability tool. The tool facilitated institutional transparency and accountability in the adoption of community recommendations. PARCAG was influential in shaping Public Health–Seattle & King County’s COVID-19 and antiracism work, with 66 of 75 (88%) recommendations adopted partially or fully. For example, a fully adopted recommendation in May 2020 was to report King County COVID-19 case data by race and ethnicity, and a partially adopted recommendation was to translate COVID-19 information into additional languages. PARCAG members were recruited from a 2019 advisory board on Census 2020 and were adept at shifting to advising on COVID-19 and equitable practices and policies. Organizations that have made declarations that racism is a public health crisis should center the experiences, expertise, and leadership of communities of color in accountable ways when developing and implementing strategies to disrupt and repair the effects of structural racism and efforts to promote and protect public health.
The COVID-19 pandemic serves both as another example of the disproportionate prevalence of morbidity and mortality experienced by racially and ethnically minoritized groups and as a galvanizing call to action to disrupt structural racism.1,2 Structural racism is defined as the totality of ways societies reify and perpetuate racial hierarchy through interconnected systems—housing, education, employment, health care, financing, media, criminal/legal, and public health—that reinforce discriminatory beliefs and allocate resources based on membership in racial and ethnic groups. 3 As part of the 2020 national reckoning with racism and its grounding in US settler colonialism, Public Health–Seattle & King County (PHSKC) joined more than 250 government entities in 40 states in declaring that racism is a public health crisis 4 and committed to centering Black and Indigenous voices in organizational decisions. 5
Public health has historically solicited community input via community advisory boards, most often in the context of academic research.6,7 Community advisory board members are selected based on a shared interest, identity, illness experience, history, language, or culture. 8 Community advisory boards provide infrastructure for community members to voice concerns and priorities that may be missed by researchers, 8 especially given the underrepresentation of racially and ethnically minoritized groups among researchers themselves as a result of structural racism in science, technology, engineering, and math education. 9 Community advisory boards have facilitated mutually beneficial partnerships between academic researchers and communities that increased the cultural relevance of research designed to promote changes in local policies and practices.8,10
To achieve such changes in health policy and practice, the community advisory board model has been adopted by public health departments across the country, including PHSKC. PHSKC has leveraged the community advisory board model to provide the infrastructure for institutional accountability—explaining how its actions support its organizational mission, values, and goals—and to take responsibility for decisions for action or inaction. Accountability is a key feature of the public health accreditation process. 11 In the context of declaring racism a public health crisis, accountability mechanisms need to center ways of disrupting anti-Blackness and anti-Indigeneity among communities as a root-cause approach for antiracism praxis given legacies of settler colonialism that undergird structural racism. 12 However, a description and evaluation of the implementation and impact of community advisory board models, particularly those with an antiracist orientation, are lacking in public health practice settings.
In response to the dual pandemics of racism and COVID-19, PHSKC convened the Pandemic and Racism Community Advisory Group (PARCAG) 13 in March 2020. PARCAG was intended to be a space where community-based organizations (CBOs) led by Black, Indigenous, and other people of color (BIPOC) could come together with PHSKC and other large institutional partners (eg, University of Washington, Microsoft, the Port of Seattle) to advise and problem-solve barriers to racial and ethnic equity in COVID-19 response efforts. PHSKC sought to reduce structural barriers and inaction in the face of need that it feared could surface during the pandemic response if intentional processes were not implemented to counteract institutional racism.14,15 Later, PARCAG agreed to advise PHSKC on 3 operational priorities: workforce diversity, community partnerships and contracting policies, and budget prioritization.
After 6 months of advising, PARCAG called for greater transparency about whether and how its recommendations were being adopted by PHSKC and what the rationales for those decisions were. PARCAG called for the adoption of antiracism principles in group functions as well as in PHSKC operations. In response, PHSKC staff developed a tool to document whether PARCAG recommendations were fully adopted, partially adopted, or not adopted; who in the health department made the decision; and what their rationale was. Many community partnership frameworks advise institutions to communicate transparently with community partners, but case studies demonstrating how to implement this type of communication are limited.16,17
Purpose
The purpose of this case study was to describe the implementation of an explicitly antiracist community advisory board model and document its processes for antiracist transparency, accountability, and trust-building. The PARCAG model and the accountability tool align with Public Health 4.0 practice, when politically engaged researchers, practitioners, and CBOs work together to respond to structural racism as a root cause of poor health. 18
Methods
Setting
PHSKC is a large metropolitan health department with more than 1400 employees serving the Seattle area in King County, Washington (population 2.3 million). 19 The median annual household income is $99 158, and 18% of the population is living at <200% of the federal poverty level. 20 County demographic characteristics are rapidly shifting—people of color (defined in this article as American Indian/Alaska Native, Asian, Black, Native Hawaiian/Pacific Islander, and Hispanic people) compose 47% of residents overall, and they represent 61% of residents aged <18 years and only 28% of people aged >64 years. 20 Across all ages, 53% of residents are non-Hispanic White, 21% are Asian, 11% are Hispanic, 7% are non-Hispanic Black, 7% are multiracial, 1% are Native Hawaiian/Pacific Islander, and 1% are American Indian/Alaska Native. 20 Almost one-third (30%) speak a language other than English at home, and 17% of adults have a disability. 20
PARCAG Leadership and Function
PARCAG comprised representatives from 25 organizations, with overrepresentation of BIPOC-led CBOs. Most members were drawn from an advisory board convened in 2019 to inform and advise King County about Census 2020 outreach. They were community leaders who brought perspectives and relationships with historically undercounted populations, such as Hispanic, non-Hispanic Black, and Pacific Islander groups.21,22 Members included representatives of county and city governments, philanthropy, and social services CBOs. Health care partners were convened in a different coalition, the Northwest Healthcare Response Network (https://nwhrn.org). PARCAG focused on Black and Indigenous community priorities and representation while uplifting people with identity intersections (eg, queer people of color, people of color with disabilities) to ground group discussions in the wisdom and experiences of those facing systemic marginalization in public health.
From March 5 through September 10, 2020, meetings were convened virtually for 1 hour on a weekly basis. PHSKC staff set agendas to disseminate information about COVID-19 and to consult with community groups about how to customize mitigation strategies. After the first 6 months, BIPOC leaders asked that PARCAG adopt a shared leadership model to center community voices in determining the group’s purpose and function. In August 2020, PARCAG established a steering committee of 5 community leaders and 1 PHSKC staff member. The majority-BIPOC steering committee set agendas, facilitated meetings, invited speakers, and developed strategy. From September 2020 through February 2022, the steering committee met biweekly, alternating with biweekly full PARCAG meetings. Steering committee members were compensated $3600 per year for their time and expertise. With a community-led steering committee, a substantial shift in power took place and a forum for PHSKC and community co-creation was created. The steering committee and PARCAG were supported by PHSKC staff who took notes, organized virtual meetings, disseminated materials, and posted slides and notes online. 13
PARCAG Accountability Tool
The accountability tool tracked health department implementation of community recommendations about COVID-19 mitigation strategies and antiracist organizational policy changes. The tool was based on a decision-tree flowchart and was informed by policy change frameworks that identify who has the authority to act on an issue and document whether community recommendations were acted on in full, in part, or not at all.23,24 The tool provided a systematic way for PHSKC staff to document PARCAG recommendations, staff and steering committee next steps, who had the authority to make a policy decision, what the decision was, and whether staff reported the decision back to PARCAG (Figure). PARCAG made recommendations within 4 domains: (1) the health departments’ COVID-19 prevention and mitigation efforts; (2) the department’s organizational goals to use more equitable processes in workforce, contracting, and budgeting; (3) PARCAG’s internal processes and norms; and (4) institutional antiracism activities among PHSKC and other organizational partners (Table).
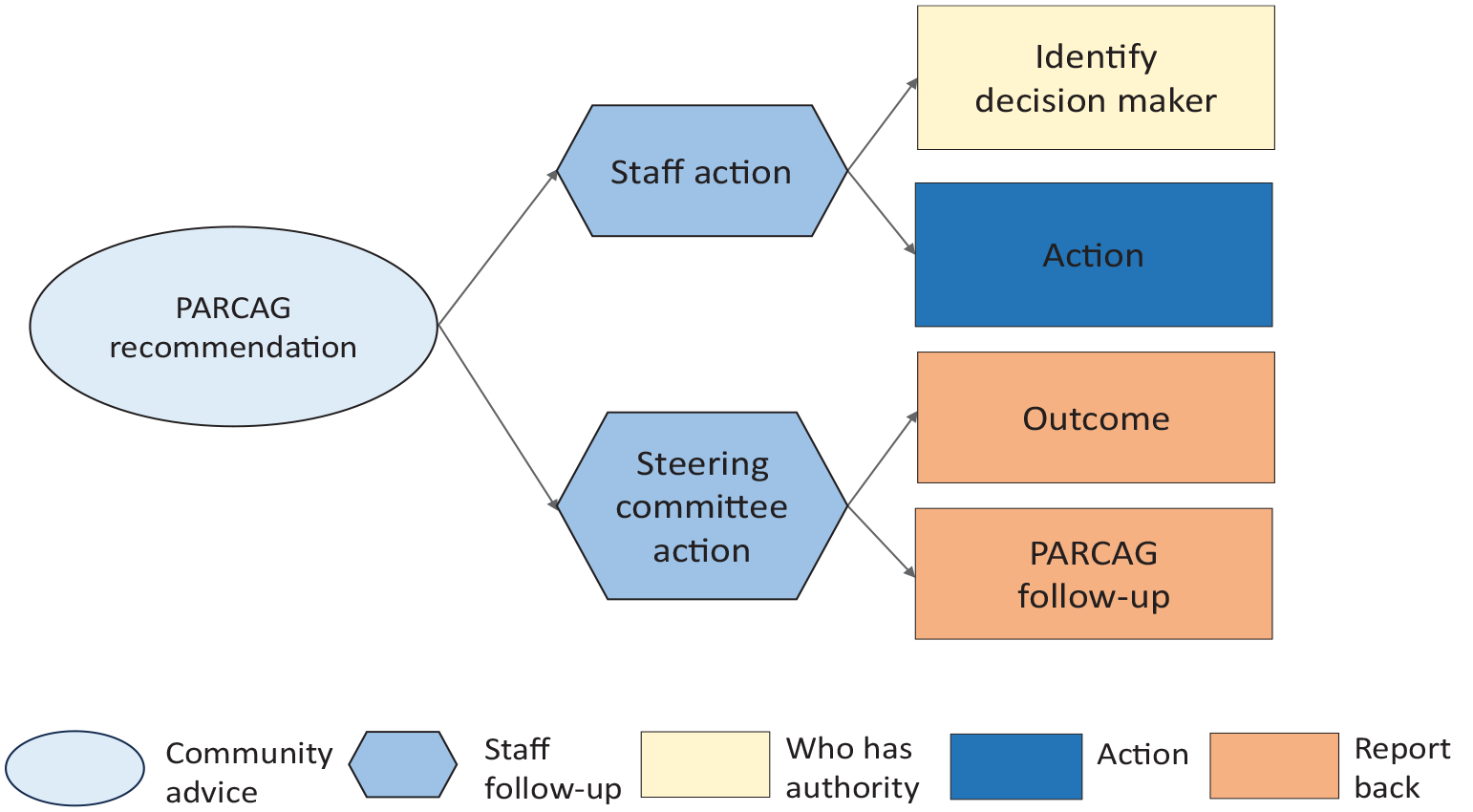
Flowchart to track Pandemic and Racism Community Advisory Group (PARCAG) recommendations and their adoption using an accountability tool, King County, Washington, 2021.
Pandemic and Racism Community Advisory Group (PARCAG) recommendations to Public Health–Seattle & King County, by type and level of adoption, March 2020 through February 2022
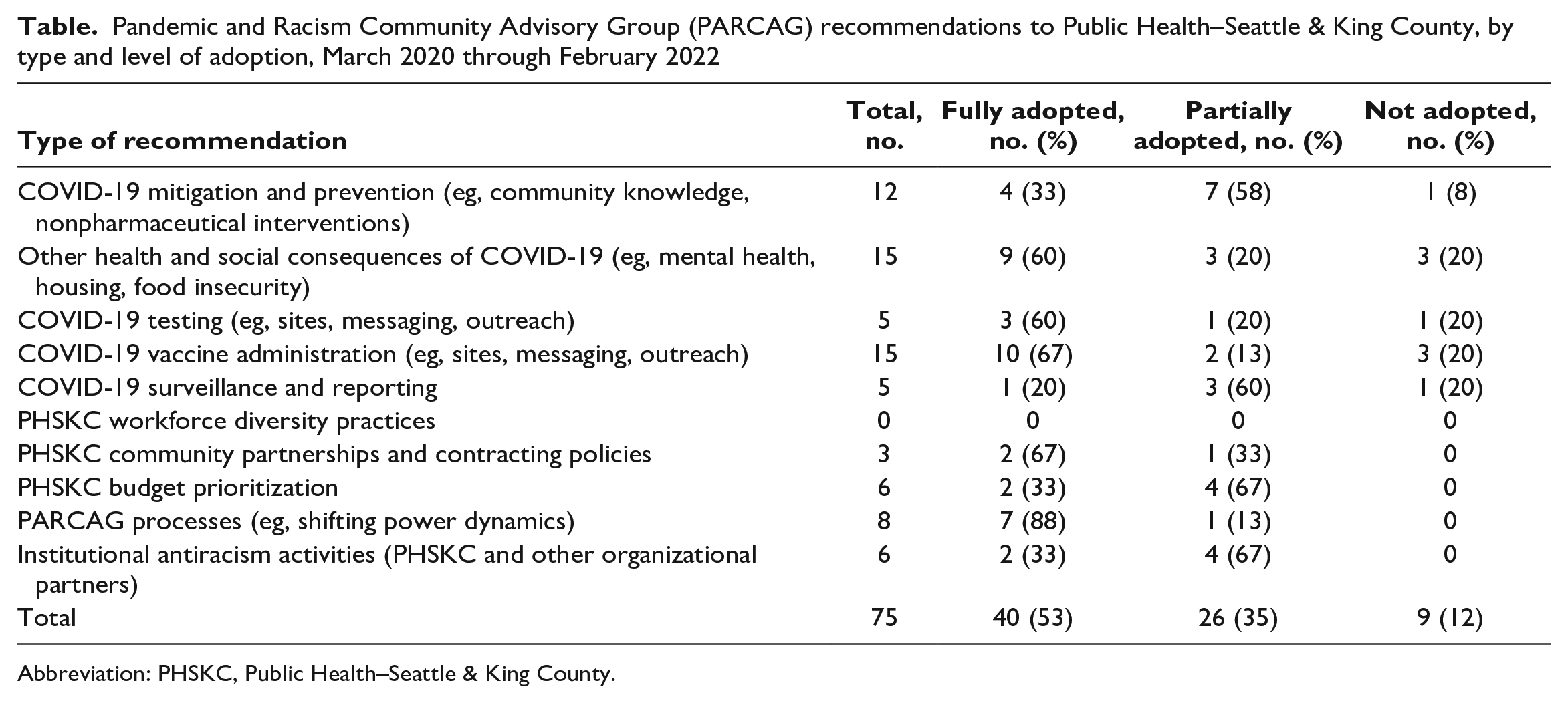
Abbreviation: PHSKC, Public Health–Seattle & King County.
Data Sources and Analysis
We counted and analyzed PARCAG recommendations and health department actions by reviewing meeting agendas, presentation slides, and meeting notes from March 2020 through February 2022. We grouped recommendations into the 4 domains and classified these as fully adopted, partially adopted, or not adopted. A fully adopted recommendation was one in which all aspects were adopted and no part of the recommendation was left unaddressed. In partially adopted recommendations, some but not all aspects were implemented. We categorized recommendations as not adopted if no action related to the recommendation was taken by the public health department. These documents are publicly available and do not include personal identifiers of PARCAG members. 25 The University of Washington Institutional Review Board considered this study not human subjects research because of the lack of interaction with or collection of identifiable information about human subjects and because the case study was conducted as part of public health quality improvement activities at PHSKC. All data included in the article are available elsewhere. 25
Outcomes
In the first 2 years of PARCAG’s operation (early 2020 to early 2022), PHSKC convened 56 PARCAG meetings and the advisory group made 75 recommendations (Table). Most of the recommendations (n = 52; 69%) focused on COVID-19 mitigation and prevention, and about one-third (n = 23; 31%) addressed the 3 other domains of PARCAG priorities.
In the first year (March 2020 through February 2021), PARCAG made 47 recommendations—25 (53%) were fully adopted, 15 (32%) were partially adopted, and 7 (15%) were not adopted. Two of the fully adopted recommendations were to use simple graphics, less text, and more videos in COVID-19 information materials and to report King County COVID-19 case data by race and ethnicity. A partially adopted recommendation was to translate COVID-19 information into more languages, which the health department did for 5 languages; PARCAG recommended using 6 more. Another partially adopted recommendation was to acknowledge and act on the mental health effects of the pandemic. Mental health effects were acknowledged in public health communications, but the health department and county government were not able to fully meet the demand for services. PARCAG recommendations that were not adopted included fully meeting requests for hand sanitizer, subsidizing housing on a scale proportional to need, providing early vaccine access to members of the racial and ethnic groups that had the highest rates of COVID-19, and requiring antiracism training for health care providers before they administered COVID-19 vaccines. These recommendations were not adopted because of supply-chain issues or because they were seen by decision makers as outside of PHSKC’s decisional authority.
In its second year, from March 2021 through February 2022, PARCAG made 28 more recommendations—15 (54%) were fully adopted, 11 (39%) were partially adopted, and 2 (7%) were not adopted by PHSKC. Fully adopted recommendations included holding vaccination events in community settings, prioritizing community funding in a CDC grant application, and modifying a vaccine verification ordinance so that identification cards would not be required. PARCAG also recommended that vaccine verification implementation be delayed by 6 weeks for small businesses and that instructions for reporting discrimination be included in signage; these suggestions were adopted. Partially adopted recommendations included distributing home test kits to some CBOs that requested them but not having enough supply to meet all requests, reporting more categories of race and ethnicity but with a 1-year implementation delay, and providing advice on some aspects of PHSKC’s 2-year budget but not on all of it. PARCAG recommendations to clarify a chart of COVID-19 cases and to prioritize vaccine administration to Pacific Islander communities due to past harms and disproportionate prevalence of COVID-19 were not acted on, due to lack of time for epidemiologists to revise the chart and lack of agreement within the department about whether to offer vaccines first to specific racial and ethnic groups. Outreach by Pacific Islander staff through Pacific Islander CBOs was undertaken to promote vaccinations in this group.
These decisions were communicated to PARCAG members during the meetings and online through the accountability tool for major recommendations. PARCAG members said they appreciated the transparency from the department about why recommendations were or were not adopted, and they communicated these decisions and rationales to their networks.
Walk-through of the Accountability Tool With a Specific Recommendation
In March 2021, the accountability tool was used to document and report back how PARCAG discussions shaped a statement of principle about how to deliver COVID-19 vaccines in racially, geographically, and socioeconomically equitable ways. PARCAG advised removing barriers that deter access; using an inclusive process in planning, implementation, and evaluation; and being intentionally antiracist and accountable. 25 These recommendations were fully adopted. PARCAG-created values were used to develop 7 principles that vaccine sites run by PHSKC and health care system partners followed in 2021 and 2022. The principles included focusing on the groups that were the most affected by COVID-19 infections by age, race, and geography; working with community leaders and trusted messengers at the vaccination sites; making appointment registration a simple process in multiple languages and in accessible ways for people with disabilities; staying open after work and on the weekends; hosting community vaccine events; and arranging no-cost transportation when needed. 26
Lessons Learned
Several lessons were learned during 2 years of PARCAG convenings that can inform accountability tool revisions and use of the tool by others.
PARCAG was an influential community advisory board model. During 2 years, 88% of its 75 recommendations pertaining to PHSKC’s COVID-19 and antiracism work were adopted partially or fully. The accountability tool enabled PHSKC to inform BIPOC community leaders about their influence and acknowledge their expertise in guiding PHSKC actions. One limitation of the implementation was that data related to the attributions for PHSKC decisions were not explicitly collected (ie, no analysis was conducted to determine whether the health department would have made a particular decision in the absence of a PARCAG recommendation).
PARCAG benefited in unanticipated ways from building on a Census 2020 advisory board. Many organizations committed to Census outreach had long-held inclusive and antiracist values. They were skilled at advising the health department on equitable COVID-19 outreach and antiracist organizational changes. With an equity and social justice ordinance in place since 2010, King County local government and its community partners had many years’ experience and training in antiracist organizational practices.27,28 These shared experiences helped form a shared foundation of language and values for PARCAG work.
Working side-by-side and co-creating health promotion strategies with communities requires a prioritization of equity, 29 which means that public health entities need to change business-as-usual processes characterized by White-dominant organizational practices. 30 Antiracist organizational practices include welcoming new ideas, refocusing practice dialogue on racial equity, including people affected by structural racism in decision-making, power-sharing, and promoting a culture that values bidirectional and race-conscious learning. 31 PARCAG members and staff revisited group norms frequently and made adjustments to prioritize and reprioritize racial equity.
One weakness of the advisory group practice was that it did not adopt a specific antiracism framework at its launch. Promoting an antiracist orientation to group function and dynamics is not easy, and PARCAG’s progress could have been facilitated by its adoption of an antiracist framework to ground group norms. All members needed to interrogate their own positionality and regularly reflect on their engagement. Steering Committee members needed to amplify and reinforce antiracism in group norms to facilitate active engagement by all members. Group composition needed to reflect intersectional identities while still acknowledging the primacy of racism. To address the effects of structural racism in the local context, the steering committee committed to centering the priorities and experiences of descendants of enslaved Africans as well as American Indian, Alaska Native, Native Hawaiian, and Pacific Islander communities. Representation of these groups within PARCAG was difficult to achieve consistently. Strategies to address these issues could be an important additional component of subsequent versions of the accountability tool.
The accountability tool was designed to summarize PARCAG recommendations, and refinements are needed to create and deepen processes to ensure it continues to be used for all recommendations, aligns PHSKC accountability with PARCAG priorities, and collects additional data on how and why recommendations were adopted, along with their effects. Evaluating outcomes stemming from PARCAG recommendations could strengthen community confidence in public health at a time when public mistrust is high. Conducting this evaluation during the COVID-19 recovery affords the opportunity to assess community effects of more proactive approaches to promote public health and health equity.
Prioritizing communities affected by structural racism holds the promise of better public health policies and implementation. PARCAG community leaders became important creators and advocates of public health measures adopted by PHSKC from 2020 through 2022. Their recommendations reflected the values and practices of PARCAG members’ communities.
Declarations that racism is a public health crisis are calls for antiracist public health transformation. 4 This transformation of past public health practice should include routine use of frameworks, processes, tools, and systems of accountability that engage communities disproportionately burdened by structural racism and the health inequities it perpetuates. The use of an accountability tool by PARCAG and PHSKC is an effort to provide transparency and accountability for a health department’s actions to the BIPOC communities it serves. Processes like this can contribute to the deepening of relationships, trust-building, and long-term collaboration that are the foundations for a culture of health for organizations and communities alike.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Centers for Disease Control and Prevention (CDC-RFA-OT21-2103, National Initiative to Address COVID-19 Health Disparities among Populations at High-Risk and Underserved, Including Racial and Ethnic Minority Populations and Rural Communities).