
Abstract
Objectives:
Treating gender identity as a fixed characteristic may contribute to considerable misclassification and hinder accurate characterization of health inequities and the design of effective preventive interventions for transgender and gender diverse (TGD) adolescents and young adults. We examined changes in how an ethnically and racially diverse sample of TGD adolescents and young adults reported their gender identity over time, the implications of this fluidity on public health, and the potential effects of misclassification of gender identity.
Methods:
We recruited 235 TGD adolescents and young adults (aged 15-24 y) in Los Angeles, California, and New Orleans, Louisiana, from May 2017 through August 2019 to participate in an HIV intervention study. We asked participants to self-report their gender identity and sex assigned at birth every 4 months for 24 months. We used a quantitative content analysis framework to catalog changes in responses over time and classified the changes into 3 main patterns: consistent, fluctuating, and moving in 1 direction. We then calculated the distribution of gender identity labels at baseline (initial assessment) and 12 and 24 months and described the overall sample by age, race, ethnicity, and study site.
Results:
Of 235 TGD participants, 162 (69%) were from Los Angeles, 89 (38%) were Latinx, and 80 (34%) were non-Latinx Black or African American. Changes in self-reported gender identity were common (n = 181; 77%); in fact, 39 (17%) changed gender identities more than twice. More than 50% (n = 131; 56%) showed a fluctuating pattern.
Conclusions:
Gender identity labels varied over time, suggesting that misclassification may occur if data from a single time point are used to define gender identity. Our study lays the foundation for launching studies to elucidate the associations between shifting gender identities and health outcomes.
Research on transgender and gender diverse (TGD) populations—people whose gender identities, expressions, and behaviors are not traditionally associated with their sex assigned at birth—has increased during the past decade. Among an estimated 1.6 million TGD people in the United States, >43% are aged 13-24 years. 1 The diversity that exists among TGD people has been widely accepted, and the many labels that TGD people use to describe their gender identity (eg, nonbinary, gender fluid, genderqueer, two-spirit, gender nonconforming, gender diverse) are commonly used in scientific literature, the popular press, and social media. However, whether for pragmatic or analytic reasons, many researchers treat TGD people as a homogeneous group and gender identity as a static state. Although data reduction is often necessary for quantitative analysis, subsuming all TGD people as a single group obfuscates differences that may contribute to inequities in physical and mental health.
Substantial health inequities exist among TGD people, especially among adolescents and young adults.2-5 As compared with nontransgender adolescents and young adults, transgender adolescents and young adults have higher levels of mental health challenges, such as depression, anxiety, suicidality, and substance use.6-8 Differences in mental health are also shown among TGD adolescents and young adults when comparing people who identify as transgender versus nonbinary. Nonbinary is a gender identity that people use to describe themselves when they do not identify exclusively with the traditional gender binary (man, woman). 9 Newcomb et al 4 reported that young transgender women had significantly fewer depression symptoms than their nonbinary and transgender male counterparts. Rimes et al 3 found that past-year suicidal ideation rates were significantly higher among participants who were nonbinary–assigned male at birth than among those who were nonbinary–assigned female at birth and transgender. Studies have also noted significant differences in life satisfaction, reported childhood sexual abuse, self-harm, help-seeking behavior for depression and anxiety, and domestic abuse or violence between transgender and nonbinary young people.3-5,8 Thus, understanding the drivers of poor health outcomes among TGD adolescents and young adults may require examination of gender subgroups.
Despite the recognition that gender identity is fluid, adaptive, and shaped by complex interactions and experiences during the life course,10-13 most researchers view gender identity through the static lens of cross-sectional data or through participants’ report of gender identity at baseline in longitudinal studies.12,14 Failing to examine gender identity longitudinally leaves researchers unable to describe the fluidity of gender identities, how these identities change over time, and their relationship to physical and mental health outcomes. Relying on a fixed time point for describing gender identity does not capture the changes that may occur within a short time and may lead to misclassification of gender identity. Misclassifying TGD adolescents and young adults can mask important differences in health outcomes in this population and the modifiable risk and protective factors that can be leveraged for tailored prevention efforts.
Few studies, to our knowledge, have focused on changes in gender identity labels over time. However, cohort studies such as the HIV Prevention Trials Network 061 study—also known as the BROTHERS study (Broadening the Reach of Testing, Health Education, Resources, and Services), which enrolled adults aged 18-68 years—have provided preliminary evidence of shifts in gender identity over time. 14 At baseline, most participants in the sample (93.7%) identified as men; yet, at 12-month follow-up, the number of participants who identified as a man significantly decreased, with a concurrent increase in the number of participants who identified as women. When data were controlled for age, the changes remained significant, suggesting that changes in gender identity reporting occur throughout the life course. Diamond and Butterworth 15 reported fluidity and multiplicity in gender identity during a 10-year period for 4 adult participants assigned female sex at birth from a larger study on sexual identity development. We did not find a single study that examined fluidity of gender identity among a sample of diverse, multiracial adolescents and young adults, the developmental period during which such changes might be expected.
To develop tailored prevention programs, we must be able to describe the fluidity of gender identities and how these identities change over time. This critical area merits attention and additional research, considering the unprecedented increases in antitransgender legislation and violence that further threaten the health and well-being of TGD adolescents and young adults in the United States, 16 which is occurring in parallel to the increase in young people embracing TGD identities. 1 The main objective of our study was to recognize and examine the fluidity in gender identities that is common among TGD adolescents and young adults and consider the implications of this fluidity in gender identities for health and prevention efforts. We documented changes in gender identity labels in a racially and ethnically diverse sample of 235 TGD adolescents and young adults from New Orleans, Louisiana, and Los Angeles, California; we conducted quantitative content analysis to identify discernible patterns of change; and we conducted quantitative data analysis to provide a more nuanced understanding of this fluidity.
Methods
Participants
We recruited 1727 adolescents and young adults aged 15-24 years from clinics, community-based agencies, and social media from New Orleans and Los Angeles for an HIV prevention and treatment intervention study from May 2017 through August 2019. 17 We assessed participants at 4-month intervals during 24 months; at each assessment, participants selected their gender identity and sex assigned at birth. We provided 9 response options for gender identity: genderqueer, gender nonconforming, female/woman, male/man, nonbinary, transgender female/woman, transgender male/man, two-spirit, and write-in option. We had a write-in option to allow participants to express their identity using their own words (eg, pangender, questioning, nonbinary feminine, trans/nonbinary, nonbinary woman). We limited sex assigned at birth to binary options (male, female). A team of trained research assistants conducted the research activities—all of whom identified as part of the LGBTQ+ community (lesbian, gay, bisexual, transgender, queer or questioning, or another diverse gender identity) and mirrored the demographic characteristics of the participants.
The University of California Los Angeles Institutional Review Board (no. 16-001674-AM-00006) and Tulane University Review Board (no. 1033876) approved the study protocol. All participants provided informed consent (or child assent) to participate in the studies.
To create the analytic dataset, we identified participants who selected at least once, across all time points, any TGD identity label or binary gender (eg, man) that did not correspond to their sex assigned at birth (eg, female). We then excluded participants who had <3 time points of data, resulting in a dataset of 235 TGD participants. Among the sample, 66% provided responses at ≥5 time points and 43% provided responses across all 7 time points.
We used responses to gender identity and sex assigned at birth to classify participants. In so doing, we noted that some participants did not choose the transgender identity label, even though their binary gender identity did not correspond to their sex assigned at birth. Instead, these participants defined themselves as a man, not a transgender man, or as a woman, not a transgender woman. In contrast to many researchers who group people within the transgender category regardless of the participants’ self-selected gender identities, we labeled this group “binary gender diverse” and classified them as woman–binary gender diverse or man–binary gender diverse.
Analysis
Because participants’ responses to the gender identity and “sex assigned at birth” items could be treated as quantitative data, we used a quantitative content analysis framework to guide our analytic approach. Quantitative content analysis is a systematic approach for categorizing or recategorizing qualitative data such that they can be described quantitatively. 18 For our analysis, we content analyzed the qualitative responses for gender identity and sex assigned at birth to elucidate patterns of change over time and then conducted quantitative analysis on the patterns that we constructed. The analytic team, which included racial and ethnic minority and LGBTQ+ young adults (M.A.O., D.H.S.W.), brought their lived experiences to the quantitative content analysis process.
We created a dataset in Microsoft Excel with responses to the gender identity and “sex assigned at birth” items at each time point. Through a preliminary review of responses, we inductively developed a codebook to identify the patterns of change. During weekly meetings, we discussed and revised codes until we reached consensus that the patterns were meaningful and accurately represented the data. We identified 3 patterns, each with more nuanced subpatterns:
Consistent: same gender identity over time
Fluctuating: different gender identities with no discernable pattern
Moving in 1 direction: initially reporting 1 gender identity, then reporting a different gender identity, and remaining consistent in the later identity
Two independent coders (M.A.O., D.H.S.W.) categorized participants into the patterns. The first coder was a cisgender Latinx queer man who has conducted research with LGBTQ+ communities for >5 years, and the second coder was a transfeminine Black researcher, student, and artist centering community engagement and care through their practice. For cases in which the coders disagreed on the classification of participants, the research team convened and reviewed each case until consensus was reached. The coders had 71% agreement.
In addition to the patterns of change, we were interested in further exploring the changes in distribution of gender identities over time. We focused exclusively on participants who provided 3 time points of information at 1-year intervals: at baseline (initial assessment), 12 months, and 24 months (n = 146). For this analysis, we did not include the entire sample to make sure that changes in distribution were not due to missingness at any given time point. We calculated the distribution of gender identity labels for each of the 3 time points and described the overall sample by age, race, ethnicity, and study site.
Results
Of the 235 TGD participants in our sample, 64 (27%) were assigned female sex at birth, 90 (38%) were Latinx, and 80 (34%) were non-Latinx Black or African American. Their median age was 21 years at baseline. Most (n = 158; 69%) were from Los Angeles, and the remainder were from New Orleans.
Of 235 TGD participants, 77% (n = 181) changed their identities at least once and 17% (n = 39) changed their identities ≥2 times (Table 1). We found a fluctuating pattern in 56% (n = 131), with the most prevalent fluctuation being from a transgender to binary gender diverse identity with no discernible pattern (20%, n = 47). Among 50 participants who moved in 1 direction, 28 initially reported cisgender identities and consistently cited a TGD identity at the end of their participation in the study.
Patterns in gender identity reporting among 235 TGD adolescents and young adults aged 15-24 years, Los Angeles, California, and New Orleans, Louisiana, 2017-2019 a
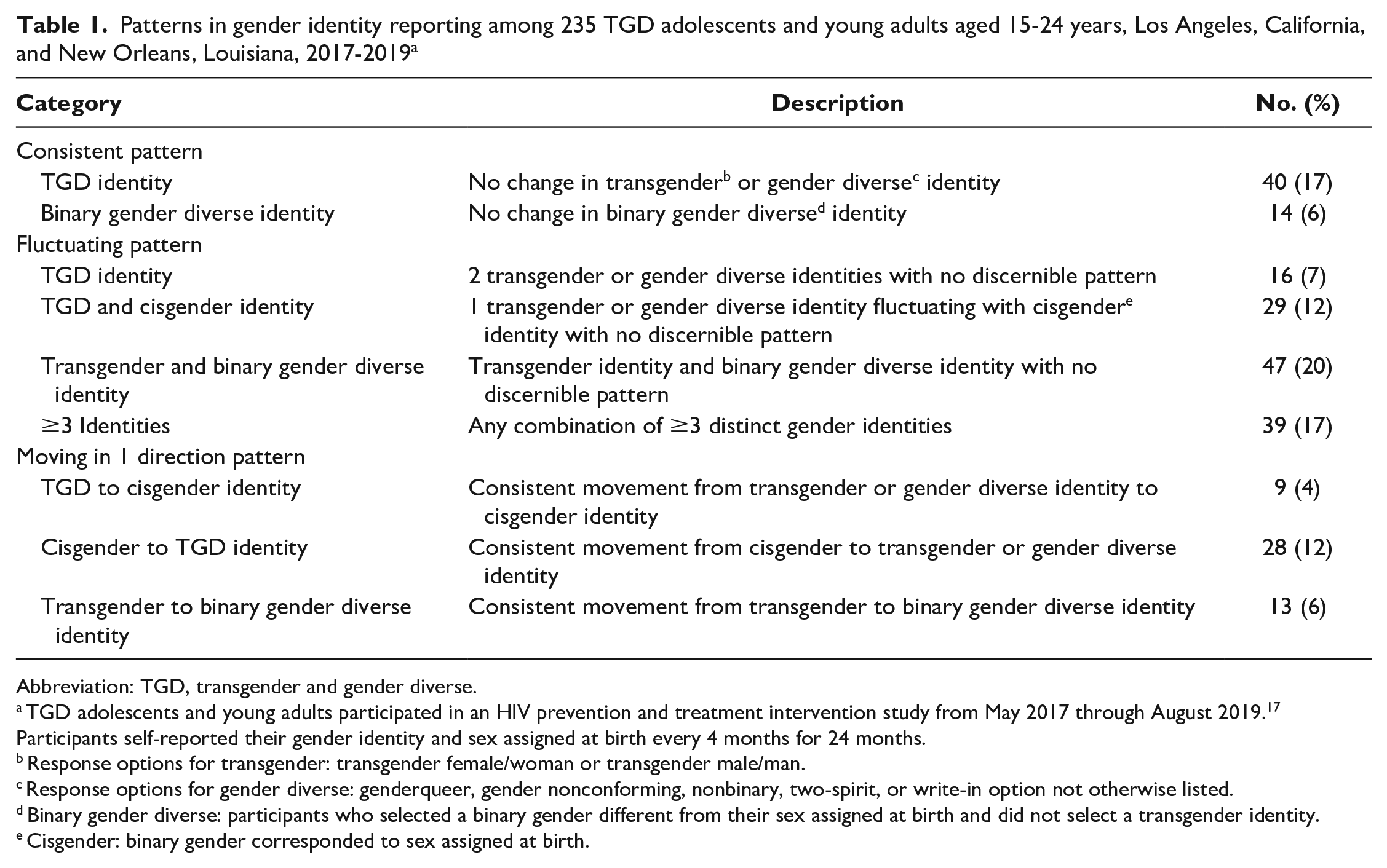
Abbreviation: TGD, transgender and gender diverse.
TGD adolescents and young adults participated in an HIV prevention and treatment intervention study from May 2017 through August 2019. 17 Participants self-reported their gender identity and sex assigned at birth every 4 months for 24 months.
Response options for transgender: transgender female/woman or transgender male/man.
Response options for gender diverse: genderqueer, gender nonconforming, nonbinary, two-spirit, or write-in option not otherwise listed.
Binary gender diverse: participants who selected a binary gender different from their sex assigned at birth and did not select a transgender identity.
Cisgender: binary gender corresponded to sex assigned at birth.
With regard to the distribution of gender identity labels among participants who reported data at baseline and at 12 and 24 months, at baseline 22% (n = 31) identified as cisgender, 37% (n = 54) as transgender, and 15% (n = 22) as binary gender diverse (Table 2). The proportion who selected nonbinary and other gender diverse identities was comparable from baseline (27%; n = 39) to 24 months (31%; n = 45), but the number of participants who reported cisgender identities from baseline (22%; n = 31) to 24 months (14%; n = 20) decreased. The proportion of binary gender diverse participants increased from baseline to 24 months (15% vs 33%), but the proportion who identified as transgender decreased from baseline to 24 months (37% vs 23%).
Distribution of TGD identities reported at baseline and at 12- and 24-month assessments in a sample of adolescents and young adults aged 15-24 years, Los Angeles, California, and New Orleans, Louisiana, 2017-2019 a
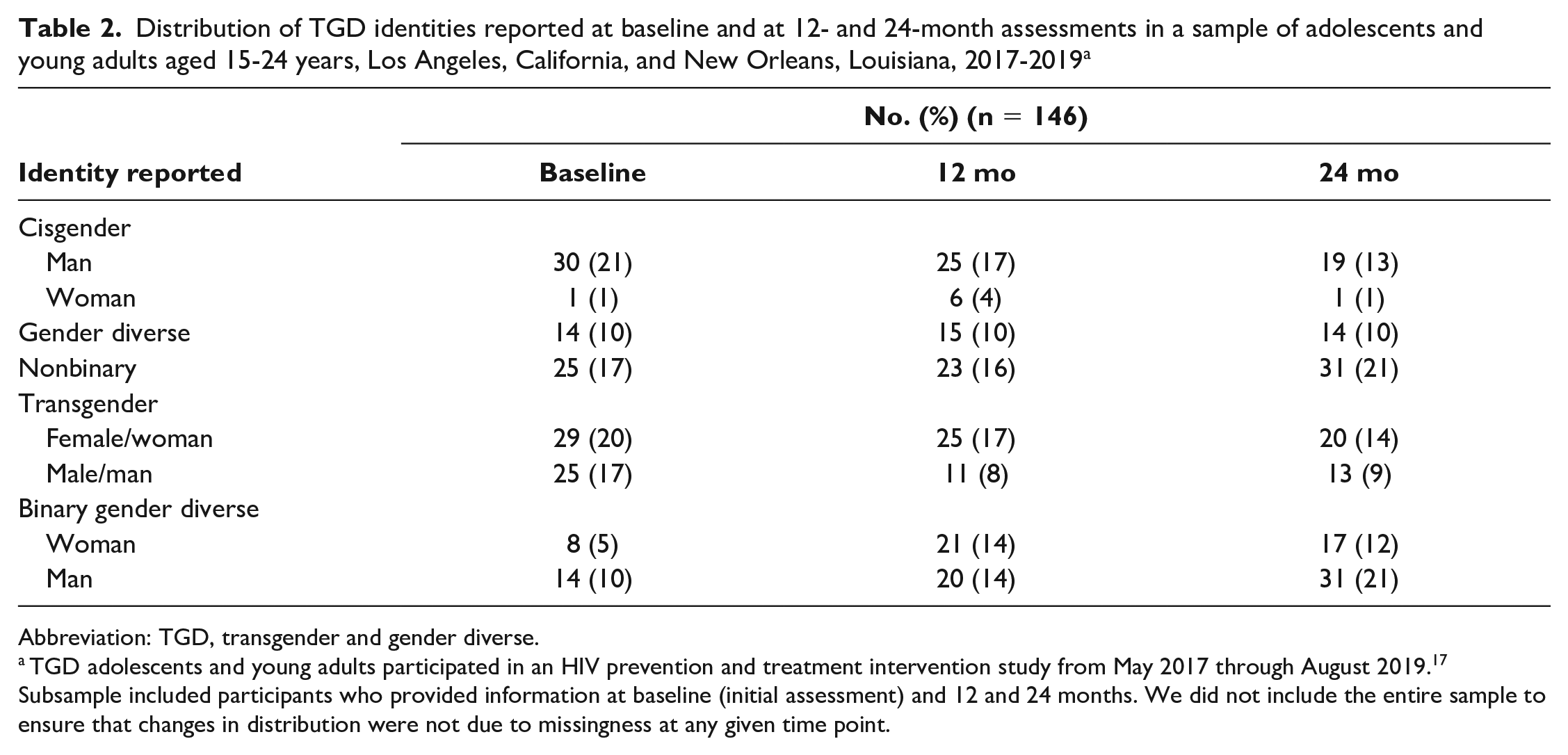
Abbreviation: TGD, transgender and gender diverse.
TGD adolescents and young adults participated in an HIV prevention and treatment intervention study from May 2017 through August 2019. 17 Subsample included participants who provided information at baseline (initial assessment) and 12 and 24 months. We did not include the entire sample to ensure that changes in distribution were not due to missingness at any given time point.
Discussion
To our knowledge, this study is one of the first to show 3 distinct patterns of gender identity reported in a diverse population of TGD adolescents and young adults. The considerable variation in gender identity in our study supports prior work suggesting that gender identity can change in a short period. 14 Our findings also suggest that using any single time point as a fixed marker for gender identity can result in misclassification, which could have dire implications for accurately characterizing health disparities among TGD young people.
Tordoff et al 19 explored the effect of misclassification bias among TGD respondents in the 2014-2016 Behavioral Risk Factor Surveillance System survey. Because the survey interviewers assessed sex assigned at birth based on the participants’ voice at the time, many who reported a transgender or gender nonconforming identity received anatomically incorrect questions pertaining to their reproductive health (eg, Papanicolaou testing, pregnancy). The study estimated that 30% of transgender men and women were misclassified. Furthermore, prevalence estimates for pregnancy among transgender men and all reproductive health estimates for gender nonconforming participants varied considerably, even with a small degree of misclassification bias. In our study, we explored misclassification longitudinally. More than 75% of the sample reported ≥1 change in gender identity; thus, had we used baseline data to label TGD participants, we would have omitted 59 participants (25%) who identified as TGD in follow-up assessments. These changes in identity highlight the importance of including, as well as examining, gender identity longitudinally and the potential effect of misclassification in characterizing health disparities among TGD people.
For greater clarity, we intentionally created a separate label, binary gender diverse, to classify the participants who selected a binary gender different from their sex assigned at birth. When recoding gender variables, many researchers create a composite group combining participants who self-identify as transgender and those we classified as binary gender diverse. Anecdotal reports suggest that people who are binary gender diverse may be qualitatively different from those who self-identify as transgender. They may not identify with the transgender community and navigate the world differently, 20 as noted by Lindqvist et al. 13 Furthermore, their physical and mental health needs may differ, which has implications for public health researchers and practitioners interested in etiologic and intervention research among TGD adolescents and young adults. Binary gender diverse people are understudied. Our literature review did not yield a single study that independently examined the needs of this group, highlighting the necessity for tailored research.
The 3 distinct patterns of gender identity labeling that emerged during our qualitative analysis are interesting. We did not have a priori expectations. The 3 patterns seemed to reflect the explorations typical during adolescence and emerging adulthood. 21 Among our participants, 23% were classified in the consistent pattern, suggesting that they zeroed in on 1 gender identity label during the study period. More than 50% were classified in the fluctuating pattern, which suggests that they were exploring the fit of different gender identity labels. In contrast, adolescent and young adult participants who were classified in the “moving in 1 direction” pattern appeared to be making strides toward defining their gender identity (ie, they selected the same gender identity during the last 2 assessments).
We present these patterns to illustrate the fluidity and range of identities that TGD adolescents and young adults may use to describe themselves during a relatively short period, not as a commentary on gender identity development. The development of gender identity is a complex and dynamic process that is influenced by the interplay among psychosocial and biological factors. 13 Simply reporting the labels that TGD adolescents and young adults use to describe their gender identity while illustrating fluidity does not accurately reflect the process. The fact that some participants may have identified as cisgender at least once does not necessarily mean that they are not TGD. Gender identity changes occur throughout the life course, and identifying as cisgender at the final study visit does not imply that a participant’s “gender journey” has ended. Gender journeys are complex, and the fluctuations that we reported reinforce the need for gender-affirming care (1) to support TGD adolescents and young adults as they explore their gender identities and (2) to ensure that they are affirmed in the process. Mixed-methods studies are needed to provide an understanding of how changes in gender identity labels relate to gender identity development and how these changes influence the health and well-being of TGD young people.
Limitations
Our study had some limitations. First, our convenience sampling, imbalanced representation of sex assigned at birth (73% assigned male sex at birth), and restricted age range limited generalizability to the broader TGD community. Second, the surveys were interviewer administered, introducing the potential for data entry errors and social desirability bias. Although our interviewers were well-trained and experienced members of the community and data collection occurred in safe, private, and welcoming environments, participants may have been unwilling to disclose gender identities truthfully. Therefore, some degree of self-reporting bias may have occurred. Third, to simplify the coding process, we combined the least selected identity labels into the gender diverse category (eg, gender nonconforming, two-spirit), which may have caused us to miss more nuanced patterns of change. Fourth, only 2 response options were provided for sex assigned at birth, which may have excluded intersex individuals or led to misclassification. For the gender identity item, participants could select just 1 response. Thus, the variation in gender identity reporting that we observed may have been artifactual because participants may have identified with all of the labels but were allowed to select only 1 per assessment point. Fifth, we examined gender identity for just 24 months and had no data on gender identity labels before enrollment and after study completion. The patterns that we identified may have varied had we been able to include gender identity labels outside of the study period. Lastly, we did not collect data to contextualize these changing patterns, which limited our ability to interpret the meaning of these observed changes.
Conclusion
Despite the increase in the number of young people embracing more diverse gender identities, the process of gender identity fluidity and its consequences for the health and well-being of TGD young people are not well understood. Public health researchers and practitioners have the tools and methods to make substantial advances in this understudied area of inquiry. By empirically documenting shifting patterns of gender identity labels among TGD young people, our study lays the foundation for launching studies to elucidate the associations between shifting gender identities and health outcomes, data that are critical for the development of preventive interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Institute on Minority Health and Health Disparities Mentored Research Scientist Career Development Award (K01MD016813) and a Eunice Kennedy Shriver National Institute of Child Health and Human Development grant funded through an Adolescent Medicine Trials Network for HIV/AIDS Interventions (U19HD089886).