
Abstract
Objectives:
Surveillance systems for unexplained deaths that might have an infectious etiology are rare. We examined the Minnesota Department of Health Unexplained Deaths and Critical Illnesses of Possible Infectious Etiology and Medical Examiner Infectious Deaths (UNEX/MED-X) surveillance system,—a system that expanded postmortem surveillance for infectious diseases during the COVID-19 pandemic by leveraging standard (medical examiner [ME]) and expanded (mortuary) surveillance to identify COVID-19–related deaths.
Methods:
MEs, coroners, or morticians collected postmortem swabs from decedents with an infectious prodrome or with SARS-CoV-2 exposure before death but with no known recent infectious disease testing. The Minnesota Department of Health Public Health Laboratory used nucleic acid amplification, viral culture, and standard algorithms to test specimens collected postmortem for SARS-CoV-2, influenza virus, and other infectious pathogens. We reviewed UNEX/MED-X data from March 2, 2020, through December 31, 2021, and characterized decedents by location of swab collection (ie, ME or mortuary).
Results:
From March 2, 2020, through December 31, 2021, the UNEX/MED-X surveillance system received samples from 182 decedents from mortuaries and 955 decedents from MEs. Mortuary decedents were older than ME decedents (median age, 78 vs 46 y). Seventy-three mortuary decedents (40.1%) and 197 ME decedents (20.6%) had SARS-CoV-2 detections. The UNEX/MED-X system identified 212 COVID-19–related deaths, representing 2.0% of total COVID-19–related deaths in Minnesota. Eighty-nine decedents (42.0%) were from racial and ethnic minority populations, representing 6.1% more COVID-19–related deaths among people from racial and ethnic minority populations than would have been detected without this surveillance system.
Practice Implications:
Expanded and standard UNEX/MED-X surveillance builds capacity and flexibility for responding to emerging public health threats. Similar programs should be considered elsewhere as resources allow.
Mortality surveillance is used to track characteristics of those dying to provide insights into health threats encountered when living. 1 Understanding the causes of death can uncover health disparities, inform policy decisions, improve outbreak and disaster response efforts, and inform development of interventions to save lives. 1 Surveillance for unexplained deaths and critical/(life-threatening) illnesses can provide opportunities to monitor emerging disease trends and expand the understanding of causes of death. Since 1995, the Minnesota Department of Health (MDH) has conducted surveillance for unexplained deaths and critical illnesses that might have an infectious etiology. The Unexplained Deaths and Critical Illnesses of Possible Infectious Etiology (UNEX) program initially began as part of the Emerging Infections Program in Minnesota, Connecticut, Oregon, and parts of California in collaboration with the Centers for Disease Control and Prevention (CDC) Infectious Disease Pathology Branch.2,3 As of April 2023, Minnesota was the only state still operating an UNEX program. In 2006, MDH expanded surveillance of deaths from infectious diseases by initiating the Medical Examiner Infectious Deaths (MED-X) surveillance program, based on the New Mexico MED-X program. 4 MED-X prioritizes unexplained deaths in decedents aged <50 years regardless of having infectious disease hallmarks, although decedents are sometimes included regardless of age at death (eg, decedent has no obvious cause of death). 5 These 2 complementary surveillance systems—collectively known as the UNEX/MED-X programs—supplement routine surveillance for infectious diseases and mortality surveillance in Minnesota. 2
UNEX/MED-X relies on collaborations among public health professionals, clinicians, pathologists, infection control professionals, medical examiners (MEs), and coroners. The goals of the UNEX/MED-X system are to (1) identify novel and newly emerging pathogens, (2) identify deaths attributable to known pathogens presenting as sudden unexplained deaths, (3) monitor epidemiologic features of fatal infections, and (4) improve pathology-based diagnostics. In Minnesota, coroners and MEs have jurisdiction over all sudden or unexpected deaths and those that may result from any factor other than natural disease processes, including deaths of people not seen by a physician within 120 days of death. 6 Unexplained deaths and critical illnesses (possibly because of an infectious cause) in a previously healthy person must be reported by MEs and coroners to MDH within 1 working day. 7 MEs and coroners, in accordance with universal precautions as required by Minnesota statutes, 8 collect and submit autopsy swabs to UNEX/MED-X for standardized infectious disease testing.
During an emerging pathogen epidemic, the investigation of deaths that occur outside traditional settings is important to determine if deaths occurring in the community are the result of the novel pathogen. 8 When the COVID-19 pandemic began in early 2020, the MDH Public Health Laboratory (PHL) was initially the only SARS-CoV-2 testing facility in Minnesota. After the first identification of a positive SARS-CoV-2 test result in Minnesota in March 2020, MDH partnered with mortuaries (ie, funeral establishments, as defined in the Minnesota statutes 9 ) to expand postmortem UNEX/MED-X surveillance (Figure). Because of a limited supply of testing materials, COVID-19 testing in Minnesota was initially prioritized for hospitalized patients, health care workers, and people living in congregate settings 10 until testing was widely available. Deaths among residents at skilled nursing facilities increased during April 2020,11,12 before widespread SARS-CoV-2 testing was available. The limited testing capacity and overwhelmed health care systems gave rise to concerns that COVID-19–related deaths might be missed; thus, MDH partnered with mortuaries to increase testing capacity through postmortem testing, leveraging UNEX/MED-X while Minnesota public health and clinical laboratories were scaling up testing capacity. Minnesota reached its target testing capacity of 20000 tests per day on June 29, 2020. 13 The expanded UNEX/MED-X surveillance meant that postmortem nasopharyngeal swabs could be collected at mortuaries for infectious disease testing of decedents who did not receive an autopsy, which increased the capacity of postmortem testing before and after SARS-CoV-2 testing was widely available. Our objective was to describe findings from standard (ME) and expanded (mortuary) UNEX/MED-X postmortem surveillance during the COVID-19 pandemic.
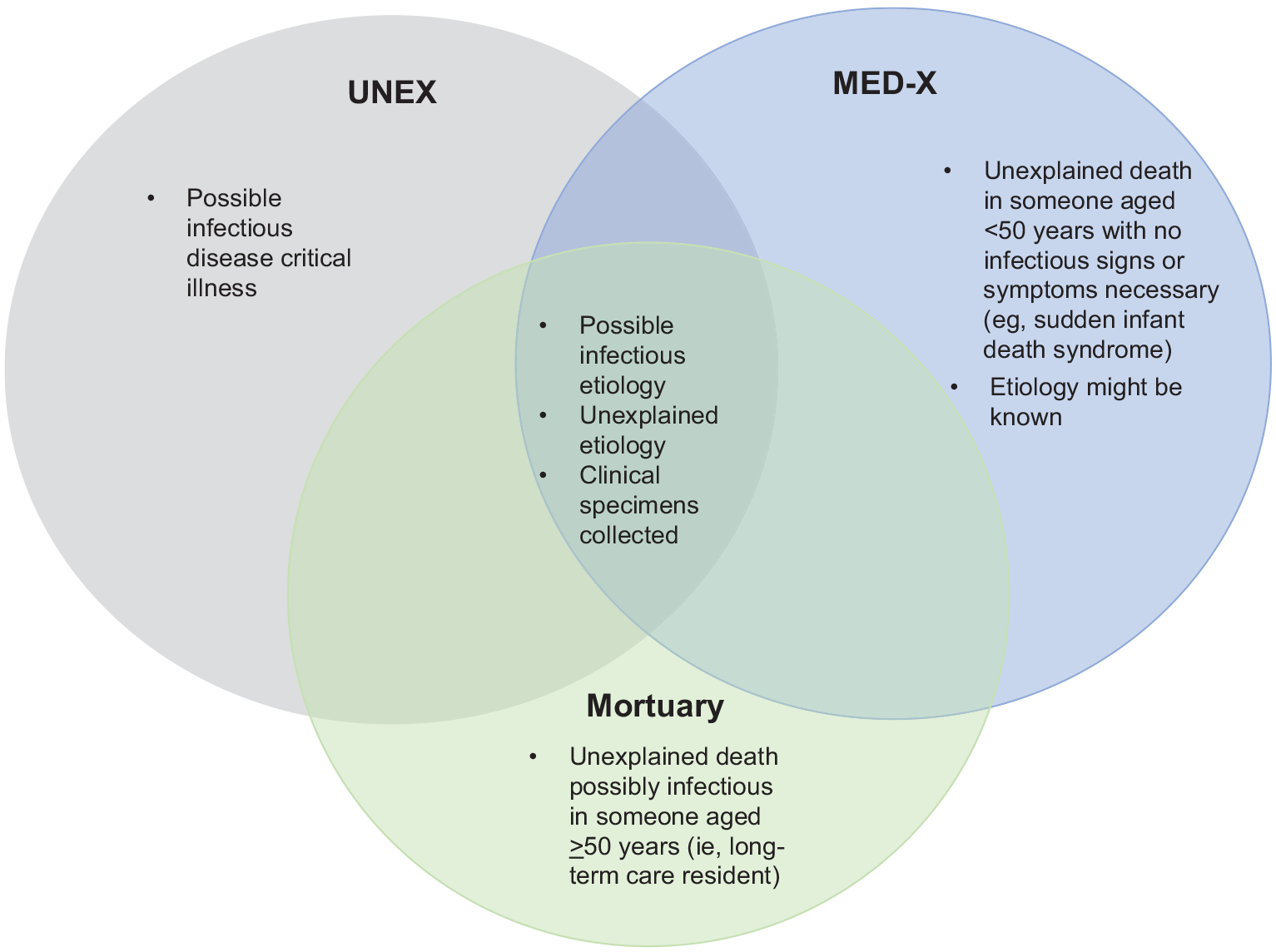
Components of the UNEX/MED-X surveillance system, Minnesota. A critical illness is defined as the condition of a person who is hospitalized in an intensive care unit or is critically ill in the judgment of a licensed health care provider. Abbreviation: UNEX/MED-X, Unexplained Deaths and Critical Illnesses of Possible Infectious Etiology and Medical Examiner Infectious Deaths.
Methods
Coroners, MEs, morticians, and other staff collected postmortem nasopharyngeal and lung swabs from decedents at ME and mortuary facilities who had an infectious prodrome or unexplained death, with no known recent infectious disease testing, and submitted swabs to UNEX/MED-X for testing. MDH provided guidance for testing decedents for COVID-19. 14 MEs occasionally collected other specimens, including blood, stool, and cerebrospinal fluid samples. The MDH PHL used nucleic acid amplification testing or viral culture and applied a standard testing algorithm to test samples for SARS-CoV-2, influenza virus, and other reportable and nonreportable pathogens. 15 The MDH PHL routinely tested nasopharyngeal and lung swabs by using either the TaqPath COVID-19 Combo Kit or the CDC Influenza SARS-CoV-2 Multiplex Assay and, if negative, performed additional testing by using the Luminex NxTAG Respiratory Pathogen Panel and viral culture. The MDH PHL also developed and used agent-specific polymerase chain reaction tests for certain pathogens, including enterovirus, rhinovirus, and parechovirus. In some cases, MDH PHL obtained and sent paraffin-embedded tissue to the CDC Infectious Disease Pathology Branch for additional testing. The MDH PHL attempted to identify the following pathogens (some are not routinely tested for): adenovirus, astrovirus, bocavirus, Bordetella species, Chlamydia pneumoniae, coronavirus 229E, coronavirus HKU1, coronavirus NL63, coronavirus OC43, cytomegalovirus, enterovirus, Epstein-Barr virus, Escherichia coli, Fusobacterium species, Haemophilus influenzae, herpes simplex virus types 1 and 2, human herpes virus 6-8, human metapneumovirus, influenza A and B, Legionella pneumophila, Mycoplasma pneumoniae, norovirus, parainfluenza 1-4, parechovirus, respiratory syncytial virus A and B, rhinovirus, rhinovirus/enterovirus (not characterized further), rotavirus, Salmonella, sapovirus, SARS-CoV-2, and Streptococcus pneumoniae.
We reviewed UNEX/MED-X data from March 2, 2020, through December 31, 2021, and characterized results according to where postmortem specimens were obtained (ie, ME or mortuary) to distinguish standard UNEX/MED-X surveillance (ME) from expanded (mortuary) surveillance. We excluded all critical illness cases, which were reported and tested antemortem, and decedents without postmortem SARS-CoV-2 testing. MDH defines critical illness as the condition of a person who was hospitalized in an intensive care unit or was critically ill in the judgment of a licensed health care provider. 7 We then identified decedents with SARS-CoV-2 detections or codetections. We reviewed death certificates for decedents with SARS-CoV-2 detections to determine whether the death met the CDC/Council of State and Territorial Epidemiologists COVID-19 death case definition 15 at the time of review.
We collected information on decedents from medical records (if available), scene investigation findings, and autopsy and pathology reports. We matched decedent data to Minnesota death certificates to determine race and ethnicity information and location of death. We did not have death certificate information if the decedent died in another state (n=73), if the decedent was a stillbirth (n=4), or if the death certificate was not filed or found (n=4). We classified race and ethnicity as a composite measure, with decedents categorized as Hispanic, non-Hispanic White, non-Hispanic Black, non-Hispanic American Indian or Alaska Native, non-Hispanic Asian or Pacific Islander, and other (ie, >1 race or ethnicity or not identifying with any other category). Hereinafter, we refer to decedents as Hispanic, White, Black, American Indian, Asian/Pacific Islander, and other. We categorized location of death as outside a health care facility (ie, decedent’s residence, other residence, street, vehicle, outdoors, or other non–health care location); in a health care facility (ie, emergency department, urgent care, or other health care clinic); hospital inpatient; or hospice, nursing home, or long-term care or assisted living facility. This activity was reviewed by CDC and conducted consistent with applicable federal law and CDC policy (45 CFR part 46 and 21 CFR part 56, 42 USC §241[d], 5 USC §552a 44, USC §3501 et seq).
From March 2, 2020, through December 31, 2021, MDH reported 10867 deaths in Minnesota from COVID-19. 16 Overall, 1.9% (n=203) were American Indian, 3.8% (n=418) Asian/Pacific Islander, 5.0% (n=542) Black, 2.9% (n=313) Hispanic, 0.7% (n=71) other, and 85.7% (n=9316) White; 4 decedents had missing race or ethnicity information.
Results
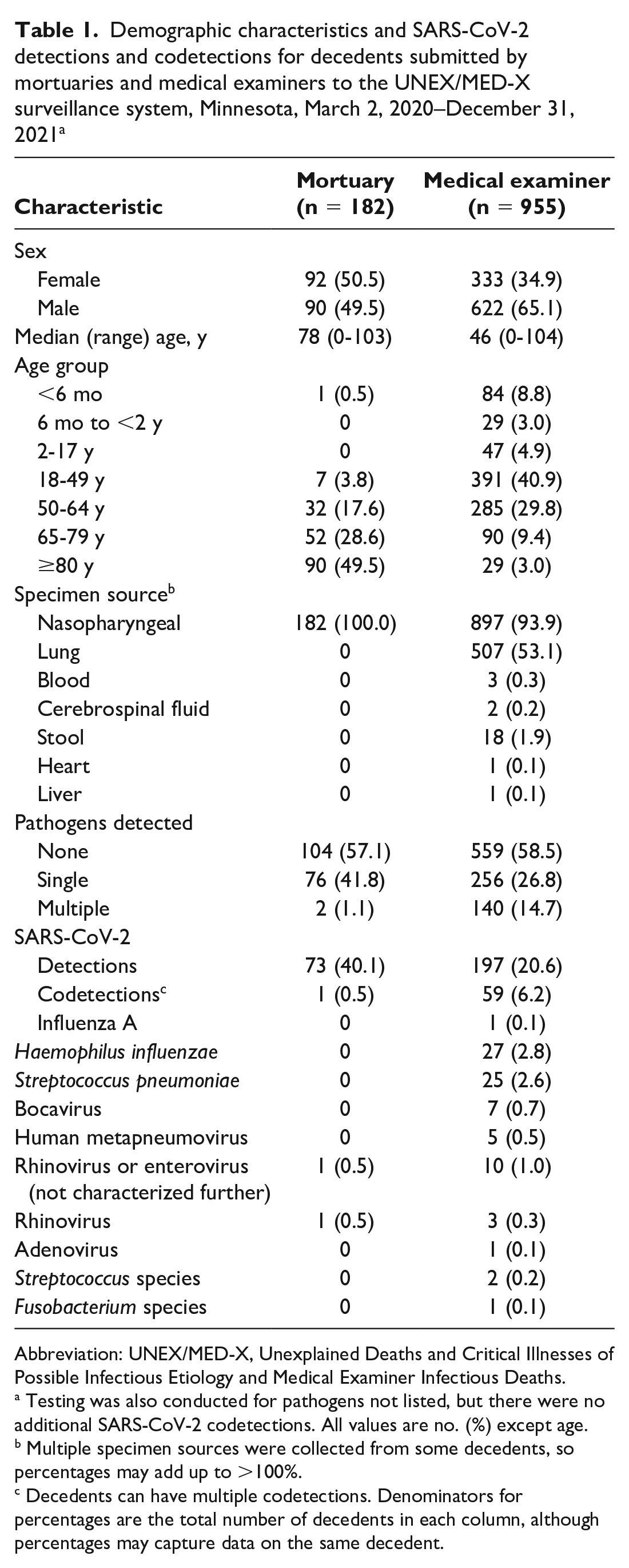
From March 2, 2020, through December 31, 2021, UNEX/MED-X identified 182 decedents from mortuaries and 955 decedents from MEs (Table 1). The percentage of male decedents was higher among ME decedents than mortuary decedents (65.1% vs 49.5%). Mortuary decedents were older than ME decedents (median age, 78 vs 46 y). Among mortuary decedents, 76 (41.8%) had a single pathogen detected and 2 (1.1%) had multiple pathogens detected. Among ME decedents, 256 (26.8%) had a single pathogen detected and 140 (14.7%) had multiple pathogens detected. Seventy-three mortuary decedents (40.1%) and 197 ME decedents (20.6%) had SARS-CoV-2 detections. One mortuary decedent had a SARS-CoV-2 codetection with rhinovirus. Fifty-nine ME decedents (6.2%) had SARS-CoV-2 codetections (some decedents had multiple codetections): 27 (2.8%) H influenzae, 25 (2.6%) S pneumoniae, 10 (1.0%) rhinovirus or enterovirus (not characterized further), 7 (0.7%) bocavirus, 5 (0.5%) human metapneumovirus, 2 (0.2%) Streptococcus species, 1 (0.1%) adenovirus, and 1 (0.1%) Fusobacterium species.
Demographic characteristics and SARS-CoV-2 detections and codetections for decedents submitted by mortuaries and medical examiners to the UNEX/MED-X surveillance system, Minnesota, March 2, 2020–December 31, 2021 a
Abbreviation: UNEX/MED-X, Unexplained Deaths and Critical Illnesses of Possible Infectious Etiology and Medical Examiner Infectious Deaths.
Testing was also conducted for pathogens not listed, but there were no additional SARS-CoV-2 codetections. All values are no. (%) except age.
Multiple specimen sources were collected from some decedents, so percentages may add up to >100%.
Decedents can have multiple codetections. Denominators for percentages are the total number of decedents in each column, although percentages may capture data on the same decedent.
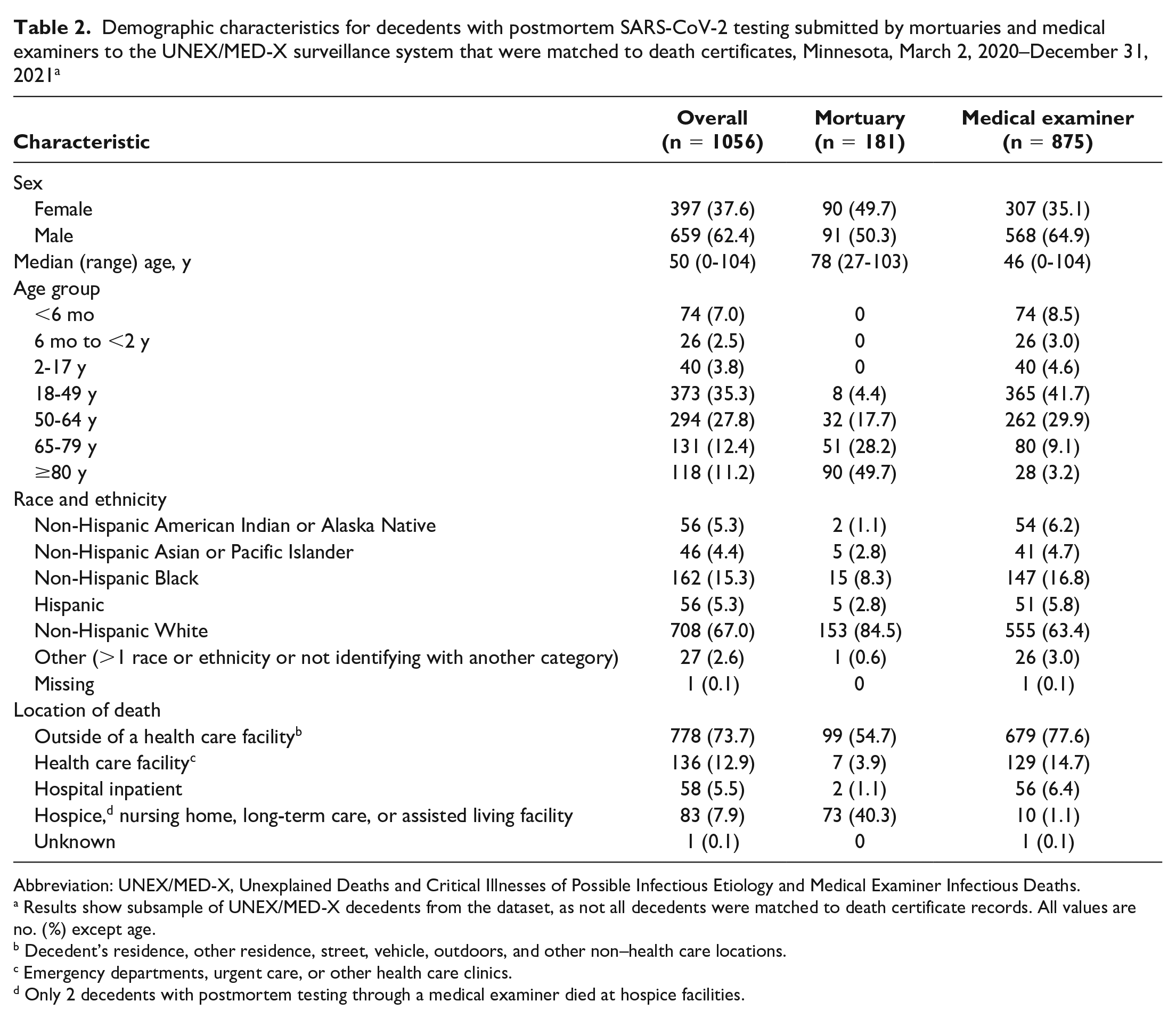
Among 1137 decedents, death certificates were matched for 1056 (181 mortuary decedents, 875 ME decedents) (Table 2). Among the 1056 decedents with matched death certificates, 5.3% were American Indian, 4.4% Asian/Pacific Islander, 15.3% Black, 5.3% Hispanic, 67.0% White, and 2.6% other. A higher percentage of mortuary decedents than ME decedents were White (84.5% vs 63.4%). Conversely, a higher percentage of ME decedents than mortuary decedents were American Indian, Asian/Pacific Islander, Black, Hispanic, and other. Among 1056 decedents with matched death certificates, 73.7% died outside a health care facility. The percentage of decedents who died in hospice, a nursing home, or long-term care or assisted living facility was higher among mortuary decedents than among ME decedents (40.3% vs 1.1%).
Demographic characteristics for decedents with postmortem SARS-CoV-2 testing submitted by mortuaries and medical examiners to the UNEX/MED-X surveillance system that were matched to death certificates, Minnesota, March 2, 2020–December 31, 2021 a
Abbreviation: UNEX/MED-X, Unexplained Deaths and Critical Illnesses of Possible Infectious Etiology and Medical Examiner Infectious Deaths.
Results show subsample of UNEX/MED-X decedents from the dataset, as not all decedents were matched to death certificate records. All values are no. (%) except age.
Decedent’s residence, other residence, street, vehicle, outdoors, and other non–health care locations.
Emergency departments, urgent care, or other health care clinics.
Only 2 decedents with postmortem testing through a medical examiner died at hospice facilities.
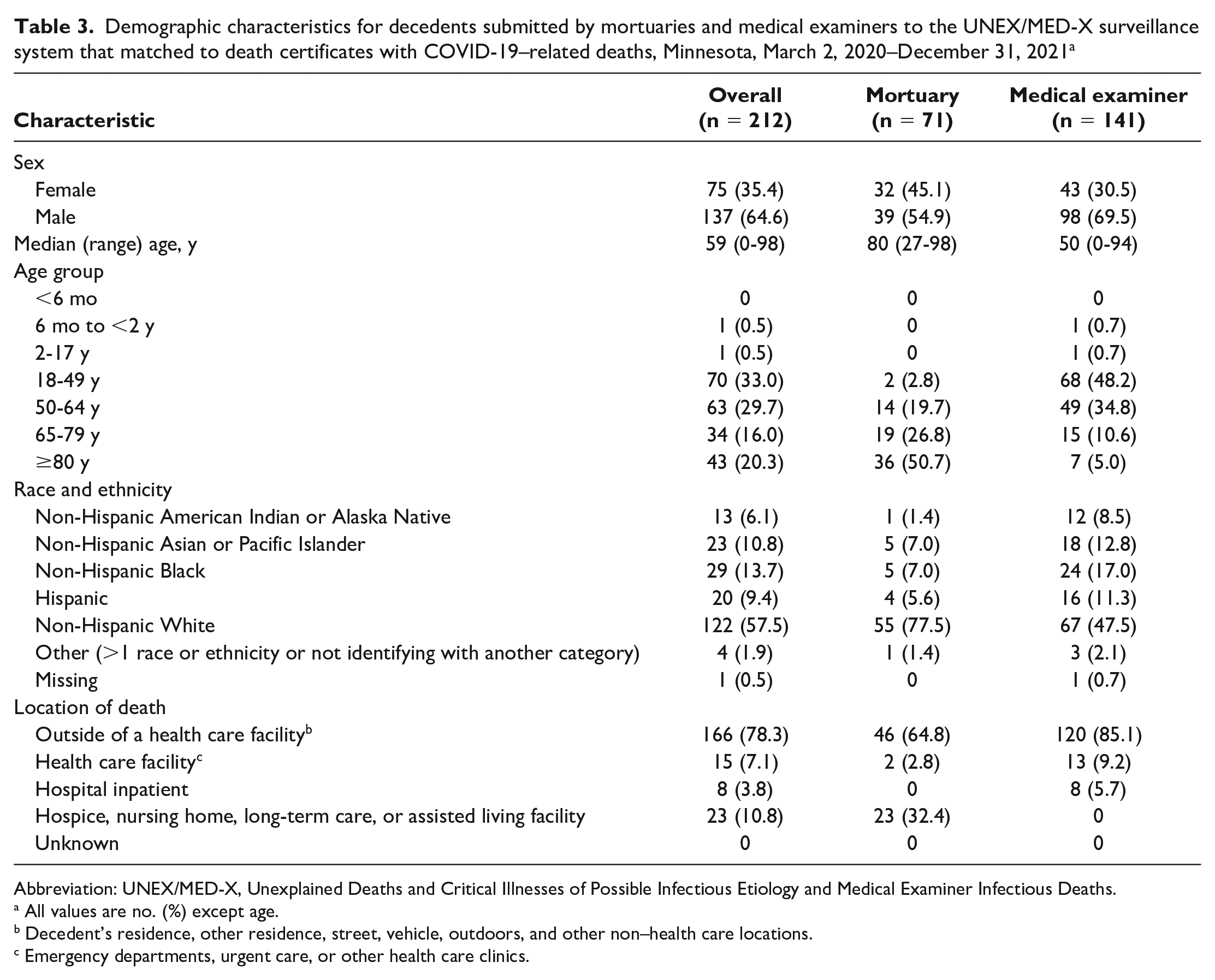
Of 270 UNEX/MED-X decedents with a SARS-CoV-2 detection, 212 deaths (78.5%) were considered COVID-19–related, including 71 mortuary decedents (33.5%) and 141 ME decedents (66.5%) (Table 3). UNEX/MED-X decedents accounted for 2.0% of the 10867 COVID-19–related deaths in Minnesota during the study period. Mortuary decedents with COVID-19–related deaths were older than ME decedents with COVID-19–related deaths (median age, 80 vs 50 y). Among decedents with COVID-19–related deaths, 30.5% of ME decedents and 45.1% of mortuary decedents were female. Of 212 COVID-19–related deaths, 6.1% were American Indian, 10.8% Asian/Pacific Islander, 13.7% Black, 9.4% Hispanic, 57.5% White, and 1.9% other. A higher percentage of mortuary decedents (77.5%) than ME decedents (47.5%) with COVID-19–related deaths were White. The percentage of decedents with COVID-19–related deaths who were American Indian, Asian/Pacific Islander, Black, Hispanic, and other was higher among ME decedents than among mortuary decedents.
Demographic characteristics for decedents submitted by mortuaries and medical examiners to the UNEX/MED-X surveillance system that matched to death certificates with COVID-19–related deaths, Minnesota, March 2, 2020–December 31, 2021 a
Abbreviation: UNEX/MED-X, Unexplained Deaths and Critical Illnesses of Possible Infectious Etiology and Medical Examiner Infectious Deaths.
All values are no. (%) except age.
Decedent’s residence, other residence, street, vehicle, outdoors, and other non–health care locations.
Emergency departments, urgent care, or other health care clinics.
From March 2 through June 28, 2020, before Minnesota reached its testing capacity target, 57.6% (30 of 52) of COVID-19–related deaths in UNEX/MED-X were residents of long-term care facilities, as compared with 4.3% (2 of 46) from June 29 through December 31, 2020. Among 212 COVID-19–related deaths in UNEX/MED-X, 3.8% died at a hospital (inpatient) and 7.1% died at another health care facility (Table 3). Among decedents with COVID-19–related deaths, 64.8% of mortuary decedents and 85.1% of ME decedents died outside a health care facility. None of the ME decedents with COVID-19–related deaths died in hospice, a nursing home, or a long-term care or assisted living facility, as compared with 32.4% of mortuary decedents with COVID-19–related deaths.
Discussion
UNEX/MED-X is a flexible surveillance system that leveraged existing relationships to expand postmortem infectious disease surveillance during the COVID-19 pandemic. Expanded (mortuary) and standard (ME) UNEX/MED-X surveillance identified COVID-19–related deaths in Minnesota—specifically, 2.0% of the total identified COVID-19–related deaths in Minnesota during March 2, 2020–December 31, 2021, thereby reducing the underreporting of COVID-19-related deaths. We noted some differences in decedent characteristics between standard and expanded UNEX/MED-X surveillance. For example, mortuary decedents were generally older than ME decedents. This finding was not unexpected because standard UNEX/MED-X surveillance prioritizes decedents aged <50 years. 5 A greater percentage of mortuary decedents than ME decedents had SARS-CoV-2 detected postmortem, indicating that increasing testing capacity through partnerships with mortuaries was a useful strategy for enhancing surveillance for unexplained deaths during the COVID-19 pandemic. During the first wave of the pandemic, COVID-19 disproportionately affected adults residing in long-term care facilities, 11 and COVID-19 testing was prioritized for hospitalized patients, health care workers, and people living in congregate settings. 10 The UNEX/MED-X surveillance system captured data on decedents who might not have been in the priority category for testing before death or who might have been unable to obtain testing for other reasons, such as reduced staff capacity to collect specimens. We found that more than half of UNEX/MED-X COVID-19–related deaths during the initial months of the COVID-19 pandemic were among long-term care residents and only 2.8% of mortuary decedents with a COVID-19–related death died in a health care facility; this demonstrates that expanded surveillance achieved the goal of identifying COVID-19–related deaths that otherwise would have been missed because of limited testing capacity or reduced health care–seeking behaviors early in the pandemic.
Notably, we found that a lower percentage of ME decedents than mortuary decedents were White. Similarly, among those with COVID-19–related deaths, the percentage of White ME decedents was lower than the percentage of White mortuary decedents. The Minnesota population is 5.8% Hispanic, 78.1% White, 7.4% Black, 1.4% American Indian or Alaska Native, 5.5% Asian/Pacific Islander, and 1.8% other. 17 In our study, 32.9% of overall deaths and 42.0% of COVID-19–related deaths were among racial and ethnic minority and American Indian populations, demonstrating our system’s unique ability to capture deaths in racial and ethnic minority and American Indian populations. UNEX/MED-X identified 89 COVID-19–related deaths among decedents from racial and ethnic minority and American Indian populations, which represented 5.8% of the total COVID-19–related deaths among this population in Minnesota or 6.1% more total COVID-19–related deaths among this population than what would have been recognized without UNEX/MED-X. Thus, standard and expanded UNEX/MED-X surveillance reduced underreporting of COVID-19–related deaths in Minnesota and reduced underreporting of infectious diseases and COVID-19–related deaths among racial and ethnic minority and American Indian populations. This finding is similar to a study that found that H1N1 2009–associated deaths identified by an UNEX/MED-X surveillance system were more likely to be among racial and ethnic minority or American Indian populations than among decedents identified by hospital surveillance (48% vs 22%). 8
UNEX/MED-X has demonstrable value for enhancing public health surveillance to detect emerging severe infectious disease threats. UNEX/MED-X has previously detected numerous pathogens among decedents, including enterovirus, Fusobacterium species, parainfluenza, Neisseria meningitidis, Legionella species, parechovirus, and rotavirus. 2 This system has also detected Powassan virus, N meningitidis, and Epstein-Barr virus among critical illness cases. 2 COVID-19–related deaths are typically identified through review of vital statistics and death certificate matching to recent SARS-CoV-2 reports to the Minnesota Electronic Disease Surveillance System. Because MEs have jurisdiction over deaths not attended by a physician, deaths occurring outside licensed health care or residential hospice facilities, and deaths of people not seen by their physicians within the past 120 days, 6 UNEX/MED-X enables infectious disease testing that otherwise would not have been conducted and identification of causes of death that might otherwise go unrecognized, including among populations that might have limited access to health care or among young and previously healthy people. During the 2008 H1N1 pandemic, UNEX/MED-X identified 21% more total H1N1 influenza–associated deaths than by hospital-based surveillance alone. 8 In our study, 194 of 1056 decedents (18.4%) died at a hospital or other health care facility. Among 1056 decedents, 83 (7.9%) died in hospice, a nursing home, or long-term care or assisted living facility, with most (88.0%, n=73) reported by mortuaries; thus, they did not receive autopsies and would not have had postmortem infectious disease testing without the expanded UNEX/MED-X surveillance. Among 212 decedents with COVID-19–related deaths, 166 (78.3%) died outside the health care system and 23 (10.8%) died in a nursing home, long-term care, or assisted living facility. Overall, our findings demonstrate the value of the UNEX/MED-X system in discovering COVID-19–related deaths occurring outside the health care system and in racial and ethnic minority and American Indian populations that otherwise would have gone unrecognized.
Limitations
Our study had a few limitations. First, pathogen detection does not guarantee that the pathogen is related to the underlying cause of death. The UNEX/MED-X system identified 270 decedents with SARS-CoV-2 detected postmortem, but only 78.5% of these deaths were determined to be COVID-19–related. The collation of information from multiple sources, such as autopsy reports, pathology reports, medical records, and scene investigation findings, can improve the understanding of pathogen detections as causes of or contributing factors to mortality. Second, despite the UNEX/MED-X surveillance system’s ability to detect infectious causes of death that otherwise would go unrecognized, some decedents might not have had postmortem testing. Some mortuary decedents were not tested because their bodies had been embalmed by the time that the deaths were reported, which eliminated the opportunity to collect swabs. Third, MEs had a reduced capacity to conduct autopsies because of the concurrent COVID-19 and opioid epidemics, which may have reduced the number of decedents receiving postmortem testing.
Practice Implications
The systematic collection and evaluation of information from deaths provide an opportunity for improved infectious disease surveillance, which is useful for increasing understanding of infectious disease–related deaths, particularly among people who may not be identified through routine infectious disease or mortality surveillance. The racial and ethnic composition of decedents with COVID-19–related deaths and the finding that 166 COVID-19–related deaths occurred outside a health care facility or hospice, nursing home, long-term care, or assisted living facility raise questions about access to health care, access to testing, and refusal to seek care. Further understanding of the underlying reasons behind these disparities is useful for allocating public health resources. Connecting laboratory findings, pathologic evidence, and clinical features allows for the detection of pathogens and causes of death that otherwise might be missed.
UNEX/MED-X is an important public health surveillance tool in Minnesota. Because UNEX/MED-X is a flexible system that relies on partnerships between MDH and MEs, coroners, and mortuary staff, this system was able to be expanded in 2020 to address the surveillance challenges presented by limited testing capacity and the need for robust surveillance. The UNEX/MED-X surveillance system identified COVID-19 and other infectious disease deaths that otherwise would have gone unrecognized. UNEX/MED-X reduced underreporting of COVID-19–related mortality, particularly among racial and ethnic minority and American Indian populations. Prioritizing postmortem infectious disease testing has demonstrated public health value and builds capacity and flexibility for identifying and responding to emerging public health threats and for more comprehensively representing causes of deaths among populations. Similar programs should be considered elsewhere as resources allow.
Footnotes
Acknowledgements
The MDH UNEX Surveillance Team included the following people: Sarah Bistodeau, BS, Jaime Christensen, BS, Allison Huske, BS, Ellen Laine, MPH, JD, Jennifer Palm, BS, Anna Panek, BS, Elizabeth Schiffman, MPH, and Kirk Smith, DVM, PhD. The authors acknowledge Kristine Bisgard, DVM, MPH (CDC), for providing technical expertise and assistance in developing this manuscript and the medical examiners, coroners, and funeral home directors who participate in UNEX/MED-X for their contributions to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.