
Abstract

Keywords
The COVID-19 pandemic highlighted the tragic consequences of underlying health disparities in racial and ethnic minority populations and other underresourced and medically underserved populations experiencing social discrimination in the United States. 1 A high prevalence of chronic conditions in these communities is largely attributable to differences in multigenerational discrimination, living conditions, and societally mediated stressors, which are often collectively called the social determinants of health (SDOH). 2 The co-occurrence of climate change–related extreme weather events during the COVID-19 pandemic starkly illustrated a grim parallel: the same chronic conditions that contribute to the poor health outcomes from COVID-19—namely, diabetes, obesity, hypertension, and cardiovascular and respiratory diseases—are also risk factors for the poor health outcomes resulting from heat waves, wildfires, and other natural disasters.3-8
The COVID-19 pandemic is one of a spectrum of public health crises whose outcomes are anchored in SDOH.9,10 Effective solutions targeting underlying disparities in SDOH need to be locally designed and managed; indeed, first on the 2021 Presidential COVID-19 Health Equity Task Force’s list of recommendations is to invest in community-led solutions to address health equity with flexible funding options to address the needs of the community. 1 What is less well appreciated is that local actions that improve SDOH can simultaneously build climate resilience by reducing disparities in chronic conditions and vulnerability to poor health outcomes from climate-related hazards. Local actions that address SDOH (eg, housing and food security, home environments, safe spaces to gather, social capital, health care access) can provide health benefits that reduce COVID-19–related risks and climate-related risks.
Challenges and Opportunities
The challenge for building climate health resilience is aligning health and public health efforts holistically with policies and project implementation targeting underlying disparities in SDOH in a way that is led by and fully leverages community resources, community expertise, and community capacity. Place-based climate health inequities are largely the result of decades of discriminatory policies such as redlining: the intentional concentration of resources and opportunities in predominantly White neighborhoods at the expense of those who identify as Black, Indigenous, and other racial and ethnic minority groups.11,12 Place-based solutions that deliver community benefits year-round can begin to ameliorate historical deprivation and build social capital and climate resilience.13,14 Successful initiatives are characterized by a bottom-up approach, whereby outside donors, community development investors, federal/state/local government, and other partners support the communities themselves to identify local problems and priorities and design, manage, and implement solutions.15,16
New opportunities to coordinate resources from various sources toward place-based climate resilience solutions (ie, “braiding” and “blending”) may be realized by the Biden-Harris administration’s prioritization of enhancing the climate resilience of communities, with funds distributed through the Federal Emergency Management Agency’s Building Resilient Infrastructure and Communities program, the US Department of Transportation’s PROTECT program (Promoting Resilient Operations for Transformative, Efficient, and Cost-Saving Transportation), the Administration for Children and Families’ Low Income Home Energy Assistance Program, and the National Oceanic and Atmospheric Administration’s Climate Ready Coasts, among others. 17 Additionally, the Infrastructure Investment and Jobs Act and the Inflation Reduction Act include provisions for decarbonization and green energy, energy-efficient housing, transportation infrastructure and transit-oriented construction, and environmental justice block grants.18,19
Resilience Hubs as Focal Points for Investment
One promising model for this kind of community-led, bottom-up resilience planning is to use place-based resilience hubs originated by one of the authors (K.B.) and further developed with the Urban Sustainability Directors Network. 14 Resilience hubs are trusted physical sites in neighborhoods that can serve as gathering spaces, information centers, and response centers every day and during periods of disruption and recovery. They provide benefits to the community year-round in 5 foundational areas: (1) services and programming, (2) communications, (3) building and landscape, (4) power systems, and (5) operations and maintenance. 20 The resilience hub model favors a combination of strategies that retrofit or otherwise improve a building envelope and surrounding landscape; develop energy efficiency and energy independence; and reduce greenhouse gas emissions while providing programs and services tailored to the needs of the community, such as meal services, mental health, employment assistance, housing assistance, and children’s programming. Examples of successful implementation of resilience hub foundational areas include the following:
• In Los Angeles, California, enhanced communications via a radio station led by local young people that provides language-appropriate radio programming and outreach
• In Washington, DC, a community center that has been enhanced to provide local jobs, programming for young people, and proactive relationship building among community members in Ward 7
• In Cambridge, Massachusetts, a food distribution space that has been enhanced to provide mental health services and prekindergarten care while improving the weatherization and energy efficiency of the site13,14
The most effective resilience hub might benefit from braided and blended resources and funding to establish and support each of the hub’s 5 foundational areas in the short and long term.
The resilience hub model implicitly provides community benefits targeting SDOH and therefore builds resilience to climate change and extreme weather events. This model also provides for colocated health services or a satellite office or staff member of a nearby community health center or hospital (Figure). Colocation with a trusted and community-managed space can improve the efficiency of 2 pipelines—community services to health care and health care to community services—by streamlining sign-ups for health care and social services simultaneously and more effectively integrating community health workers and promotores employed by community-based organizations or health care systems. 21 It can also improve delivery of health services to those at greatest risk of climate-sensitive health effects and better incorporate health services and management into local operations during periods of disruption and recovery. The integration of health services can also expand potential funding opportunities, including those from agencies of the US Department of Health and Human Services (eg, Centers for Medicare & Medicaid Services, Health Resources and Services Administration, Substance Abuse and Mental Health Services Administration), health care systems, and medical foundations. Indeed, this matching of needs to location is an opportunity to obtain development funds and resources from governmental, health care, civic, and philanthropic organizations.
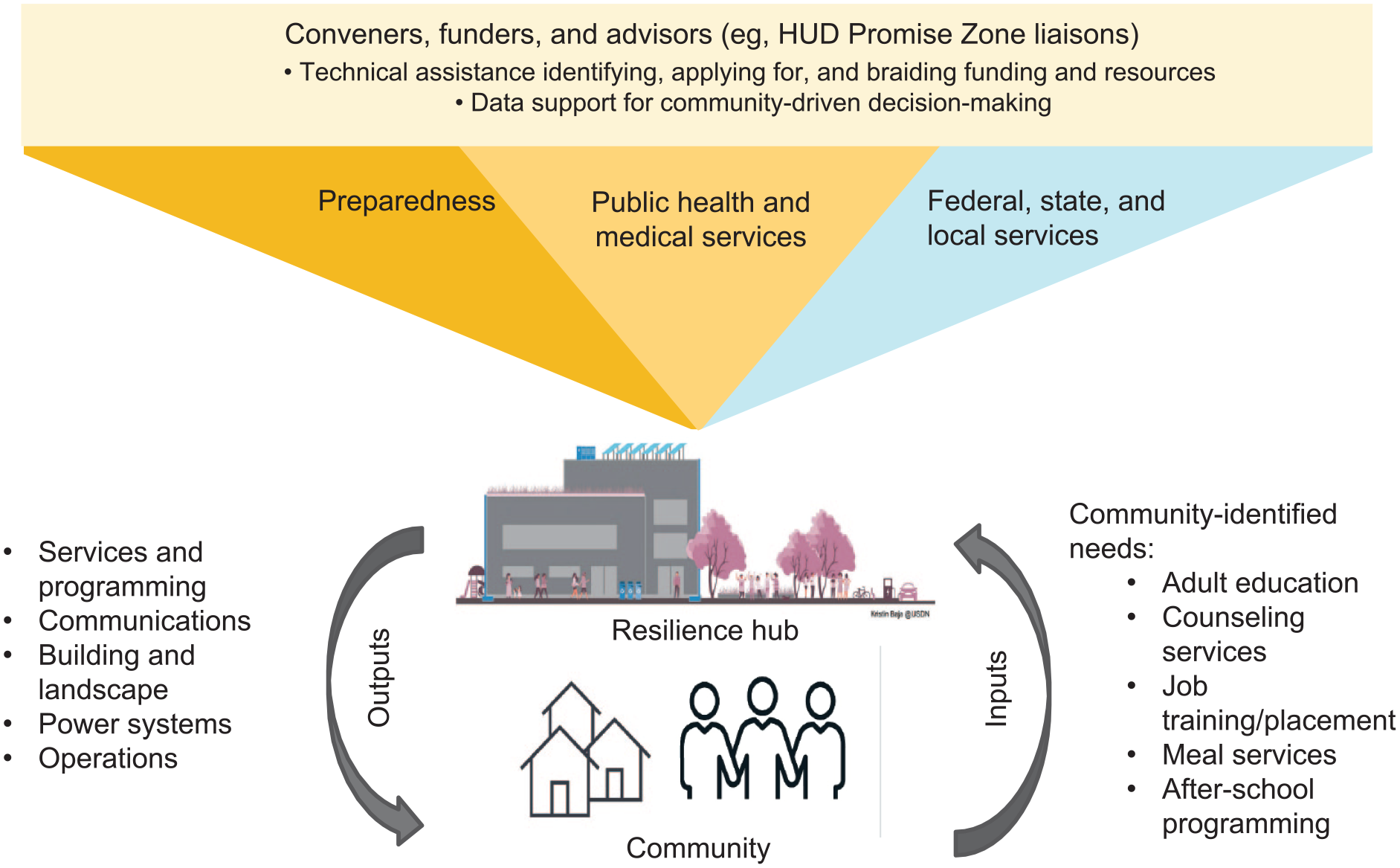
Incorporation of public health and medical services into a resilience hub model. A resilience hub is a community-determined trusted facility that supports the community by providing services and programming, coordinating communications, facilitating distribution of resources, connecting people to nature, and serving as a focal point during responses. 14 Abbreviation: HUD, US Department of Housing and Urban Development.
Community health benefits can be further enhanced by colocating community-desired public health services for vaccination, maternal child health, case management, or other local needs. Such colocalization may synergistically improve acceptance and uptake of public health services and target preventive services to those who are most medically vulnerable, therefore reducing the burden of health care use and costs. While resilience hubs are designed to provide year-round community benefits, they have a clear purpose to serve as trusted focal points for preparedness and response activities. Partnership with local emergency management agencies, including integration of the resilience hub into hazard mitigation planning, can not only better prepare the local population for disruption and mitigate its impacts but also create new opportunities for acquiring, braiding, and blending funding and resources (eg, Building Resilient Infrastructure and Communities). 22
The Promise Zone Initiative, enacted during the Obama-Biden administration, is a “collaborative effort—between private business and federal, state, and local officials; faith-based and non-profit organizations; and striving kids and parents—to ensure that hard work leads to a decent living for every American in every community (urban, rural, and tribal).”23,24 The US Department of Agriculture supports the 8 rural and tribal Promise Zones, and the US Department of Housing and Urban Development supports the 14 urban Promise Zones. For the urban Promise Zones, the department provides dedicated community liaisons who assist local leaders in garnering federal, state, and local funding and resources to address local priorities, including increasing economic activity, improving educational opportunities, leveraging private investment, reducing violent crime, and enhancing public health. By combining the power of convening, technical assistance, quantitative and qualitative data generation and analysis, and support for obtaining funding, Promise Zones can augment and support community-driven development and implementation of resilience hubs. Community needs and community-driven decisions and priorities can be supplemented by an implementation science framework coordinated by Promise Zones and local partners. Strategic partnerships with community-serving housing and economic development programs such as Promise Zones can help guarantee long-term success. Through this multisectoral approach, resilience hubs can help communities reap the benefits of year-round and disruption services.
Conclusion
The growing recognition that health disparities are rooted in historical place-based deprivations of social and environmental determinants of health means that health equity must similarly be rooted in place-based solutions and interventions that improve those determinants. The Federal Plan for Equitable Long-term Recovery and Resilience for social, behavioral, and community health recognizes that “recovery to the pre-pandemic conditions in our nation is unacceptable, as doing so would eliminate the likelihood of improved resilience for the nation. Instead, we must better position public systems to evolve in transformational ways to address community and individual well-being as the primary outcome of collective federal government resources.” 15 The growing severity of climate change and related shocks and disruptions to communities and health care delivery requires careful, evidence-based interventions that achieve multiple resilience goals: for pandemic threats such as COVID-19, for extreme weather events, and for other social stressors and shocks. By piloting and testing resilience hubs that are anchored in community leadership, design, and ownership, an opportunity exists to combine protections from climate-related shocks and the delivery of health care and social services year-round as well as during disruptions. Communities, in partnership with local governments and federal agencies, can help redress historical sources of health disparities, improve quality of life, and meet the challenges of future stresses.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or of their employing agencies.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.