
Abstract
Objectives:
Minimal research has examined the number of health departments conducting work related to equity and/or the kind of work, if any, they are conducting. We examined the relationship between public health accreditation and work related to health equity by analyzing accredited health departments’ responses to a prompt in the Public Health Accreditation Board’s (PHAB’s) annual report.
Methods:
We analyzed self-reported responses from accredited health departments to questions about emerging public health issues and innovations in PHAB’s annual report. We identified themes using a priori and inductive coding.
Results:
A total of 316 health departments submitted an annual report from January 2015 through December 2021. Of those health departments, 283 (89.6%) stated in their annual report that they engaged in work related to health equity, 50 (17.7%) of which provided a narrative about this work. Of those 50 health departments, the most common theme reported was community partnership, described by 23 (46.0%) health departments. The next most reported themes were COVID-19 vaccine access for racially or socioeconomically marginalized communities (n = 17, 34.0%) and programs related to health equity (n = 16, 32.0%).
Conclusions:
We found that most accredited health departments conduct work related to health equity. Further research is needed to examine characteristics that influence a health department’s likelihood of conducting equity work. Models and resources on how health departments, particularly small health departments, can begin equity work would be valuable.
The Public Health Accreditation Board (PHAB) is the national accrediting body for governmental health departments in the United States. As of April 2023, a total of 365 health departments (40 state, 316 local, 6 Tribal, and 3 Military Installation Departments of Public Health)—plus 1 statewide integrated local public health department system and 1 international health department—were accredited through the voluntary, peer-reviewed process. 1 Many national partner organizations, including the American Public Health Association, the Association of State and Territorial Health Officials, the National Association of County and City Health Officials, the National Indian Health Board, the National Network of Public Health Institutes, the Public Health Foundation, and the Centers for Disease Control and Prevention, support accreditation readiness by providing resources and technical assistance to health departments throughout the accreditation process. 2 Governmental health departments interested in pursuing initial accreditation must (1) determine their eligibility; (2) review a free introduction to PHAB web course; (3) register, pay, and complete the readiness and training process; and (4) review PHAB policies, Standards & Measures for Initial Accreditation, Version 2022 (hereinafter, Standards & Measures), 3 and additional resources that serve as a roadmap to the accreditation process. 4 The time it takes to complete initial accreditation varies depending on the health department’s readiness. Initial accreditation lasts 5 years; health departments must then apply for reaccreditation. 5 Accredited health departments report a wide range of benefits to accreditation related to quality improvement, community partnerships, accountability, and health equity. 6 In a survey of health departments 4 years after becoming accredited, 74% agreed that accreditation helped their health department use health equity as a lens for identifying and addressing health priorities. 7
The responsibility of the public health field to address health equity has received renewed attention in the wake of the racial and ethnic inequities highlighted by the COVID-19 pandemic, which has disproportionately affected racial and ethnic minority groups; the police killing of George Floyd, which brought awareness of the Black Lives Matter movement; and the rise of conversations related to disparities associated with immigration status, economic status, gender, sexual identity, and other identities that have been historically marginalized.8,9 Other factors that affect health equity are social and community context, neighborhood and physical environment, workplace conditions, education, and income and wealth gaps. 10 Some data collection addresses the broader relationship between health equity and COVID-19 in health departments, 10 and other data collection addresses actions that health departments are taking to promote health equity in their communities.11-13 However, research is lacking on a complete view of the number of health departments that are conducting work related to equity and/or the kind of work, if any, they are conducting. To begin to build this body of research, we examined the relationship between public health accreditation and work related to health equity by analyzing accredited health departments’ self-reported responses to a prompt in PHAB’s annual report about work concerning health equity. We sought to identify whether accredited health departments reported working on health equity–related activities and, if so, to explore the type of activities that occurred.
The PHAB Glossary of Terms: Inclusion, Diversity, Equity, and Antiracism (hereinafter, IDEA Glossary)
14
includes the following definition of health equity: Achieved when everyone has a just opportunity to be as healthy as possible. This requires removing obstacles to health such as poverty, discrimination, and their consequences, including powerlessness and lack of access to good jobs with fair pay, quality education and housing, safe environments, and health care. It is integral that health departments be bold and explicit that health equity is central to governmental public health practice. Health equity should shape and guide health department strategic plans, health improvement efforts, and performance measures.
PHAB staff and the PHAB Board of Directors wrote this definition through a collaborative process for PHAB’s IDEA Glossary, which was developed and published to ensure shared understanding and reflection of PHAB’s values. Health departments can adopt definitions unique to their community, but health equity must position communities to have a just opportunity to be healthy and thrive.
PHAB’s annual report process fosters a health department’s commitment to quality improvement and performance management; health departments are required to provide updates and examples of their efforts annually by responding to a series of questions. Annual reports also offer an opportunity for health departments to demonstrate continual engagement of key processes related to community health assessments, community health improvement plans, strategic plans, and more, while keeping a health department engaged in the process needed for reaccreditation. 15 Previous analyses of data from the annual report have focused on quality improvement, which provided results that complement studies conducted using data sources external to PHAB.16,17
Methods
We obtained data for this study through PHAB’s annual report process. Health departments submit annual reports for each of the 4 years after they are initially accredited or reaccredited. Results reflect self-reported responses from accredited health departments for questions related to the topic “emerging public health issues and innovations” in annual reports. Health departments were asked the following closed-response question: “Has the health department conducted work in any of the following areas? Select all that apply” (Box). Health departments then answered the annual report prompt: “If the health department is engaged in work in an emerging area, such as COVID-19, please tell the story of the health department’s work in one area.” Health departments can choose to write a narrative about any of the emerging topics they select.
Available responses for accredited health departments responding to the following question as part of the Public Health Accreditation Board’s annual report process: “Has the health department conducted work in any of the following areas?” Respondents were asked to select all responses that applied.
Authors compiled all data related to the previously stated question from annual reports submitted from January 2015 through December 2021. Any duplicate or incomplete data were removed prior to analysis. Using Microsoft Excel, authors identified themes by using a priori and inductive coding; an initial sample of responses was examined to determine a list of present themes. Two authors (B.L., N.R., both with formal training and experience with qualitative methods) reviewed all responses that described work related to health equity and then coded those responses to 1 or more themes as identified by the sample analysis 18 (Table). Further themes were identified through this coding process, and the list of themes was updated accordingly. The 2 authors compared findings, resolved differences collaboratively, and then determined how many health departments were coded to each theme.
Areas of work related to health equity highlighted by accredited health departments as determined by self-reported responses to the Public Health Accreditation Board’s annual report process a
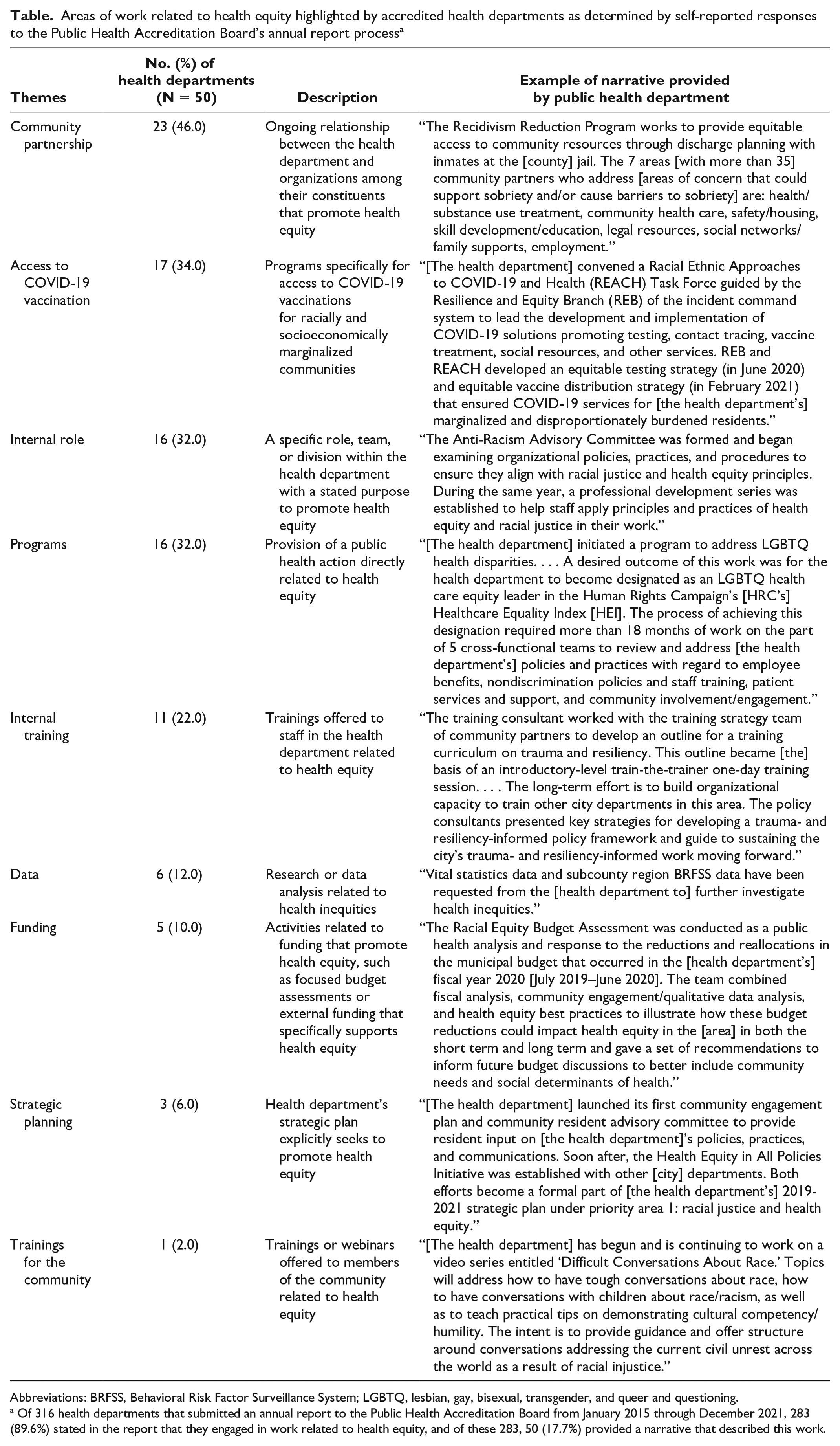
Abbreviations: BRFSS, Behavioral Risk Factor Surveillance System; LGBTQ, lesbian, gay, bisexual, transgender, and queer and questioning.
Of 316 health departments that submitted an annual report to the Public Health Accreditation Board from January 2015 through December 2021, 283 (89.6%) stated in the report that they engaged in work related to health equity, and of these 283, 50 (17.7%) provided a narrative that described this work.
For this study, the unit of analysis was the health department. If the same health department provided a response related to health equity for more than 1 year, the responses were combined to create a holistic description of the health department’s work. This study was deemed exempt from human subject research protocols by PHAB under 45 CFR §46.101 because no human subjects were used. 19
Results
A total of 316 health departments completed an annual report from January 2015 through December 2021. Of those health departments, 283 (89.6%) stated in at least 1 of their annual reports that they engaged in work related to health equity, 50 (17.7%) of which provided a narrative of their work related to health equity. Among those 50 health departments, the most common theme reported in their narratives was community partnership, reported by 23 (46.0%) health departments. The next most reported theme, COVID-19 vaccine access for racially or socioeconomically marginalized communities, was reported by 17 (34.0%) health departments. Other common themes, reported by more than 20% of health departments, included programs (n = 16, 32.0%), having an internal department or role devoted to health equity (n = 16, 32.0%), and internal training (n = 11, 22.0%).
Narratives related to health equity were more common among larger health departments, defined as serving a population of ≥500 000 (n = 27, 54.0%), than among smaller health departments, defined as serving a population of <50 000 (n = 5, 10.0%).
Discussion
As of March 2023, accredited health departments served more than 90% of the population in the United States. 20 Although most (89.6%) accredited health departments reported health equity–related work from 2015 to 2021, the degree to which equity efforts were embedded in health departments’ work varied. Examining accredited health departments’ work related to health equity is a valuable way of understanding their approaches to achieving health equity and may provide insights on how accreditation can shape their work in this area.
Community partnerships, access to COVID-19 vaccines, and internal roles were the most frequently reported ways health departments worked on health equity activities. However, the number of themes and actions related to those themes suggest that health equity can be integrated into various health department activities.
Health departments work with community partners to support health equity efforts in many ways. Community partnerships require collaboration, authentic relationships, and trust to have the desired reach and to achieve health equity goals. 21 To further explore the relationships among health equity, community partners, and accredited health departments, more research must be performed based on PHAB’s standards and measures related to community engagement and partnerships. PHAB commissioned a white paper on this topic in 2020 22 and used the results to inform the development of Standards & Measures for Initial Accreditation, Version 2022. 3 Future research should examine how changes to the accreditation requirements (eg, Measure 4.1.3: strategy implemented to provide more extensive examples of ways health departments can promote participation or eliminate barriers to participation among community members) 3 influence public health practice. Recognizing that engaging in partnership might not be sufficient to promote equity, the Standards & Measures for Reaccreditation, Version 2022, draw particular attention to decision-making processes within collaborations and the use of a community engagement model to eliminate barriers to participation. 5
As focus on health equity heightens, health departments have recognized that buy-in among leadership, through the hiring of positions focused on diversity, equity, and inclusion, is necessary. Internal roles can help a health department identify gaps and priorities, bring new perspectives to previous ways of doing things, and push a health department forward as it strives to serve all community members. 23 However, all public health roles can promote health equity through their work.
Throughout PHAB’s history, Domain 8 of the Standards & Measures has focused on the public health workforce, including efforts that incorporate equitable systems and structures; accredited health departments must demonstrate their efforts related to equity in their health department’s workforce. 3 However, much work still needs to be done to advance health equity in the workforce of accredited health departments’ hiring and retention practices and training, capacity building, and professional development. 24 This research focuses on data submitted in annual reports, leaving room to explore further connections between accreditation and equity in the public health workforce in the future.
Implementing healthy equity and antiracist practices by providing access to COVID-19 vaccinations is notable as the third most frequent theme. The pandemic increased the number of conversations on health equity and highlighted existing inequities in current systems, as demonstrated by the rise of health departments declaring racism a public health crisis. 25 The COVID-19 pandemic spurred action by accredited health departments, creating systems and best practices to implement equity in all their work.
The difference in narrative response rates between large and small health departments suggests that although health equity work is emerging at a faster rate in larger health departments than in smaller health departments, health equity work is possible in health departments of any size. Although health equity work should be tailored to the community served, the need is broad. Because this study identified few examples among small health departments, case studies to highlight work in those small jurisdictions may be particularly valuable.
To advance health equity efforts in public health, PHAB’s recently released Standards & Measures 3 emphasizes equity consistent with the 10 Essential Public Health Services 26 and the Foundational Public Health Services. 27 Both frameworks have been revised since 2020, including increasing the emphasis of the centrality of achieving health equity. Revisions to the Standards & Measures build upon what PHAB has learned from the field about equity activities already under way and strive to push the field further.
Limitations
This study had several limitations. First, the data were self-reported and, therefore, may have introduced bias or may not have fully described a health department’s efforts. Second, because the accredited health departments did not provide their own definition of health equity, they may vary in how they individually interpret or define equity and what it means to be engaged in health equity work. Third, although the PHAB IDEA Glossary is available for health departments to review, the potential variance in how health departments define equity versus how PHAB defines equity 14 presents additional limitations to this research. The authors did not collect accredited health departments’ definition of equity for analysis. This information may be beneficial to future research to increase the understanding of how health equity efforts affect a community. Fourth, the data analyzed were generated for administrative purposes, not from a data collection instrument designed for a research study. Analyzing administrative data is an effective way of minimizing contact with already overburdened health departments while still conducting research on their practices; however, we acknowledge that our approach made it difficult to determine to what degree health departments are engaging in equity work, especially for those that did not provide a narrative.
Fifth, only 50 (17.7%) accredited health departments that reported working on health equity provided a narrative for that topic; more than 80% of health departments that reported working on health equity did not provide a narrative and, therefore, were not captured in thematic analysis. This limitation means that other themes may exist and may differ from what was captured in this study. Similarly, we originally sought to examine themes related to antiracism, but at the time of writing, our data on antiracism were minimal. We plan to examine this topic in the future once we have a large enough sample for analysis. Finally, similar data on nonaccredited health departments were not available for comparison. While accredited health departments serve a large portion of the United States, many health departments have not yet been accredited.
Conclusion
Most accredited health departments reported conducting work related to health equity. Self-reported narratives demonstrated the various ways accredited health departments are implementing such practices, with some revealing how accreditation has affected this work. Further research is necessary to examine characteristics that influence a health department’s likelihood of conducting equity work and the implications it has on community health. Models and resources on how health departments can begin equity work could be valuable, particularly among small health departments where few examples have been spotlighted. As health departments begin using PHAB’s updated accreditation requirements, its focus on health equity will likely contribute to public health transformation and drive the field forward to better meet the needs of all people in all communities.
Footnotes
Disclaimer
The information contained in this article reflects the opinions of the authors and does not represent official Public Health Accreditation Board policy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.