
Abstract
Objective:
Substantial data on COVID-19–related morbidity and mortality among medically underserved populations are available, yet data on the social impact of the COVID-19 pandemic among immigrants in the United States are limited. We identified COVID-19–related health and social disparities among US immigrants.
Methods:
We analyzed predictors of COVID-19–related health and social outcomes (including ever had or thought had COVID-19, vaccine uptake, risk-reduction behaviors, job loss, childcare difficulties, and difficulty paying rent) during the pandemic by citizenship status, using data from the 2021 California Health Interview Survey. The overall sample size included 24 453 US-born citizens, naturalized citizens, and noncitizens aged ≥18 years. We examined relationships between sociodemographic variables, including immigration-related factors, and COVID-19–related health and social outcomes using descriptive, bivariate, and multivariate logistic regression analysis.
Results:
When accounting for sociodemographic characteristics, noncitizens had higher odds than naturalized and US-born citizens of experiencing challenges during the COVID-19 pandemic, including difficulty paying rent (adjusted odds ratio [aOR] = 1.54; 95% CI, 1.47-2.42) and job loss (aOR = 1.43; 95%, CI, 1.14-1.79). At the bivariate level, noncitizens had the highest rate of ever had or thought had COVID-19 (24.7%) compared with US-born citizens (20.8%) and naturalized citizens (16.8%; all P < .001). Noncitizens also had a significantly higher likelihood of risk-reduction behaviors (eg, always wearing a face covering, getting vaccinated if available) than US-born citizens (P < .001).
Conclusion:
These findings reveal the disproportionate impact of the COVID-19 pandemic among noncitizens and reflect limited socioeconomic resources, limited access to health care, and precarious employment among noncitizens in California during the pandemic. Citizenship status should be considered a critical immigration-related factor when examining disparities among immigrant populations.
In the United States, the COVID-19 pandemic substantially affected medically underserved groups, including immigrants. 1 Long-standing systemic health and social inequities have put racial and ethnic minority groups at heightened risk for COVID-19–related morbidity and mortality. 2 A recent report underscored the importance of addressing social determinants of health among marginalized and ethnic minority groups, including individuals with low income. 3 Immigrants in particular encounter challenges in accessing health care and other barriers affecting their health. 4 Although much research has centered on the health outcomes of COVID-19, few studies have investigated the impact of COVID-19 among US immigrants, highlighting the need to examine structural determinants of health affecting this group.5-10
COVID-19–Related Morbidity and Mortality Among US Immigrants
Multiple factors, including access to health care, socioeconomic status, and underlying health conditions, contribute to disparities in COVID-19–related morbidity and mortality. 11 Limited studies have shown increased COVID-19 risks among immigrant groups, especially among Hispanic/Latinx populations. 5 For example, studies in California, New York, and Minnesota found that immigrant populations were at heightened risk for COVID-19–related mortality.9,12,13 Racial and ethnic minority populations including Hispanic/Latinx people, representing the majority of US immigrants, are considerably more likely to die of COVID-19 than their non-Hispanic White counterparts. 14 A recent study found a significant positive association between the percentage of noncitizen residents and COVID-19 mortality rates in New York and Los Angeles. 9 Frontline essential jobs during the pandemic are also likely to put workers at risk of workplace exposure to COVID-19. For example, nearly half (48%) of immigrant workers in California are employed in frontline essential jobs and, therefore, may be at greater risk of workplace exposure to COVID-19 than the 41% of US-born workers who are employed in these jobs. 15
Disparities in COVID-19–related mortality are likely due to an increased prevalence of comorbid conditions as a result of unequal socioeconomic factors and inadequate access to timely health care.8,16 Many immigrants with incomes below the federal poverty level (FPL) may also have limited access to health services, live in multigenerational households, and have limited ability to isolate or receive treatment. 17 In addition, disparities in health care coverage exist among immigrant workers. According to a study using a nationally representative database, immigrant workers have a lower prevalence of health insurance coverage than US-born workers, and workers with US citizenship have higher odds of having health insurance coverage than noncitizens. 18 However, a need exists to examine immigration-related factors to identify disparities, particularly in citizenship, and the social impact of the COVID-19 pandemic beyond morbidity and mortality. 10
Early measures to control the spread of COVID-19 included shelter-in-place policies and face mask mandates, which, while crucial, led to economic disruptions affecting the mental and physical well-being of various populations.19-21 The economic disruption of shelter-in-place policies may have had substantial negative consequences on the physical and mental health of some populations, particularly children, pregnant women, and those with precarious employment.21-23 A nationwide cohort study of 6030 US children and adolescents aged 10-13 years found that experiencing financial disruptions, despite supportive policies, was associated with a 205.2% increase in perceived stress and a 112.1% increase in sadness. 23 Physical activity levels, especially among medically underserved populations, also declined after the onset of the pandemic. 24
Naturalized Citizens and Noncitizens
Citizenship status plays a crucial role in health outcomes and resource access during crises. Naturalized citizens, who undergo a process to gain US citizenship, are critical to consider in health disparities research. While they compose a substantial portion of the immigrant population, their experiences and challenges can differ based on their region of origin, language proficiency, and education level. In 2021, naturalized US citizens composed 53% of the total immigrant population of 45.3 million. 25 Language proficiency and education are critical factors in naturalization. 26 One study found that immigrants who have high levels of education and speak English well are more likely to naturalize than those with lower levels of education and poor English-speaking skills. 27
Noncitizens include unauthorized migrants, lawful permanent residents, refugees, asylum seekers, temporary lawful permanent residents, and other visa holders and generally refer to any individual who is not a member of a state in which they currently reside. 27 Noncitizens may face heightened health challenges and access issues because of their status, low socioeconomic conditions, environment, and living conditions. 17 In 2017, approximately 25 million immigrants were noncitizens.28,29 Studies suggest that noncitizens are more likely to be low income, be younger, and live in multigenerational households when compared with US-born and naturalized citizens.30,31 These conditions may increase noncitizens’ heightened risk of health challenges and contracting COVID-19. Even before the COVID-19 pandemic, noncitizens faced challenges with accessing health care.31,32 Access to health care may be further influenced by language barriers, lack of health insurance due to legal status, and fear of accessing medical services due to immigration enforcement.31,33,34
The objective of the current study was to identify COVID-19–related disparities among US immigrants. We hypothesized that differences in COVID-19–related outcomes among noncitizens, naturalized citizens, and US-born citizens would be significant. We explored this hypothesis by describing the distribution of health-related outcomes (including ever had COVID-19, testing, vaccine uptake, and wearing face coverings) and social outcomes (including difficulty paying rent, job loss, and childcare issues) and their relationship to citizenship status, as reported by a large population-based sample of California adults.
Methods
We analyzed secondary data from the 2021 California Health Interview Survey (CHIS), with an overall sample size of 24 453 immigrant and non-immigrant adults aged ≥18 years. 35 CHIS, the largest population-based state health survey in the United States, collects information on health status, health conditions, health-related behaviors, access to health care, and other health-related issues in California. CHIS is a collaborative project of the University of California, Los Angeles Center for Health Policy Research. The Charles R. Drew University of Medicine and Science Institutional Review Board determined this study was exempt because of the lack of interaction with or collection of identifiable information about human subjects and because it was a secondary analysis of publicly available, deidentified data.
Data Collection and Sample
The CHIS sample is representative of California’s noninstitutionalized household population, including adults and children. According to the 2021 CHIS, data collection methods used a mixed-mode web and telephone survey using an address-based sampling frame. 35 For CHIS data collected in 2021, household data were collected by using a computer-assisted telephone or online interviewing system between March and October 2021. For all sampled households, 1 randomly selected adult in each household either completed an online survey or was interviewed via telephone by an interviewer. The CHIS design regularly includes additional samples for specialized analyses of certain geographic areas. Survey interviews were available in 6 languages: English, Spanish, Chinese (Mandarin and Cantonese dialect), Vietnamese, Korean, and Tagalog. To produce population estimates from CHIS data, the sample data were weighted to compensate for the probability of selection and various other factors.
Data Analysis
We analyzed data using descriptive, bivariate, and multivariate analyses. We used descriptive statistics to describe the data in the study. We examined the relationship between citizenship status (US-born citizen, naturalized citizen, and noncitizen) and various health and social outcomes related to COVID-19. We examined associations between the main independent variable of interest and dependent variables by using the Pearson χ2 2-tailed test of significance, with P < .05 considered significant. We then conducted a multivariate logistic regression analysis for each COVID-19–related health and social outcome variable accounting for key sociodemographic characteristics. We weighted all analyses to account for the complex survey design of CHIS. We conducted all analyses using Stata version 17 (StataCorp LLC).
Primary Independent and Dependent Variables
The primary independent variable was citizenship status, categorized as US-born citizens, naturalized citizens, and noncitizens. Dependent variables included health and social outcomes. Health-related variables were measured as ever had or thought had COVID-19 (yes or no) and ever tested for COVID-19 (yes or no). Risk-reduction behaviors included how often wore a face covering when left home in the past week (always, usually, sometimes, never) and would get vaccine if available (yes/already received ≥1 dose or no). Social-related variables were measured as job loss due to COVID-19 (yes or no), childcare difficulties (yes or no), and difficulty paying rent (yes or no) during the pandemic.
Confounding Variables
Confounding variables included the following sociodemographic characteristics: race and ethnicity (Hispanic/Latinx, non-Hispanic Black/African American, non-Hispanic Asian, non-Hispanic White, and non-Hispanic Other [non-Hispanic American Indian/Alaska Native, non-Hispanic ≥2 races]), sex (male, female), age (18-39, 40-59, ≥60 y), education level (<high school, high school diploma/some college, ≥college degree), FPL (<200% FPL or ≥200% FPL), and employment status (full-time, part-time, unemployed). We also recategorized the 13 main occupations of respondents into 5 categories: professional/technical, education/legal and community/art, sales and related services, support/infrastructure/production, and military.
Results
Of 24 453 adults in the sample, 18 122 (74.1%) were US-born citizens, 4493 (18.4%) were naturalized citizens, and 1838 (7.5%) were noncitizens (Table 1). Noncitizens were primarily from Mexico (48.4%), Asia and the Pacific Islands (28.6%), Central America (11.7%), other Latin America (3.1%), Europe (5.2%), and other countries (3.0%). In the total sample, 51.0% were female, 15.0% were female, 14.7% had <high school education, 92.3% had health insurance, 38.3% were unemployed, and 29.8% were living at <200% FPL. About 1 in 5 (20.6%) adults in the analytic sample reported they had ever had or thought they had COVID-19 (Table 2).
Characteristics of the sample population of adults aged ≥18 years (N = 24 453) in the 2021 California Health Interview Survey (CHIS), by immigration status a
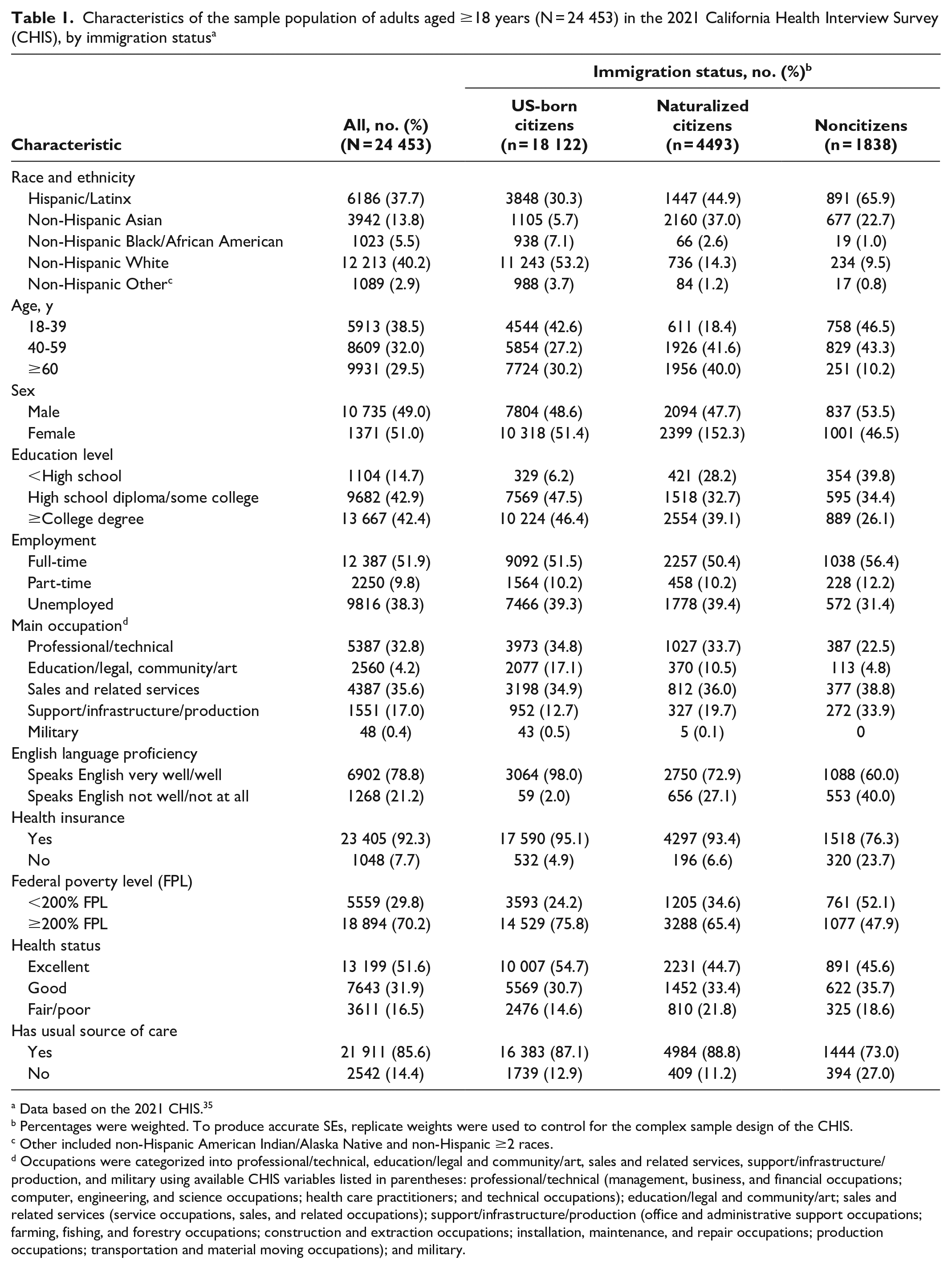
Data based on the 2021 CHIS. 35
Percentages were weighted. To produce accurate SEs, replicate weights were used to control for the complex sample design of the CHIS.
Other included non-Hispanic American Indian/Alaska Native and non-Hispanic ≥2 races.
Occupations were categorized into professional/technical, education/legal and community/art, sales and related services, support/infrastructure/production, and military using available CHIS variables listed in parentheses: professional/technical (management, business, and financial occupations; computer, engineering, and science occupations; health care practitioners; and technical occupations); education/legal and community/art; sales and related services (service occupations, sales, and related occupations); support/infrastructure/production (office and administrative support occupations; farming, fishing, and forestry occupations; construction and extraction occupations; installation, maintenance, and repair occupations; production occupations; transportation and material moving occupations); and military.
Bivariate analysis of the health and social impact of the COVID-19 pandemic on California adults aged ≥18 years in the 2021 California Health Interview Survey, by immigration status a
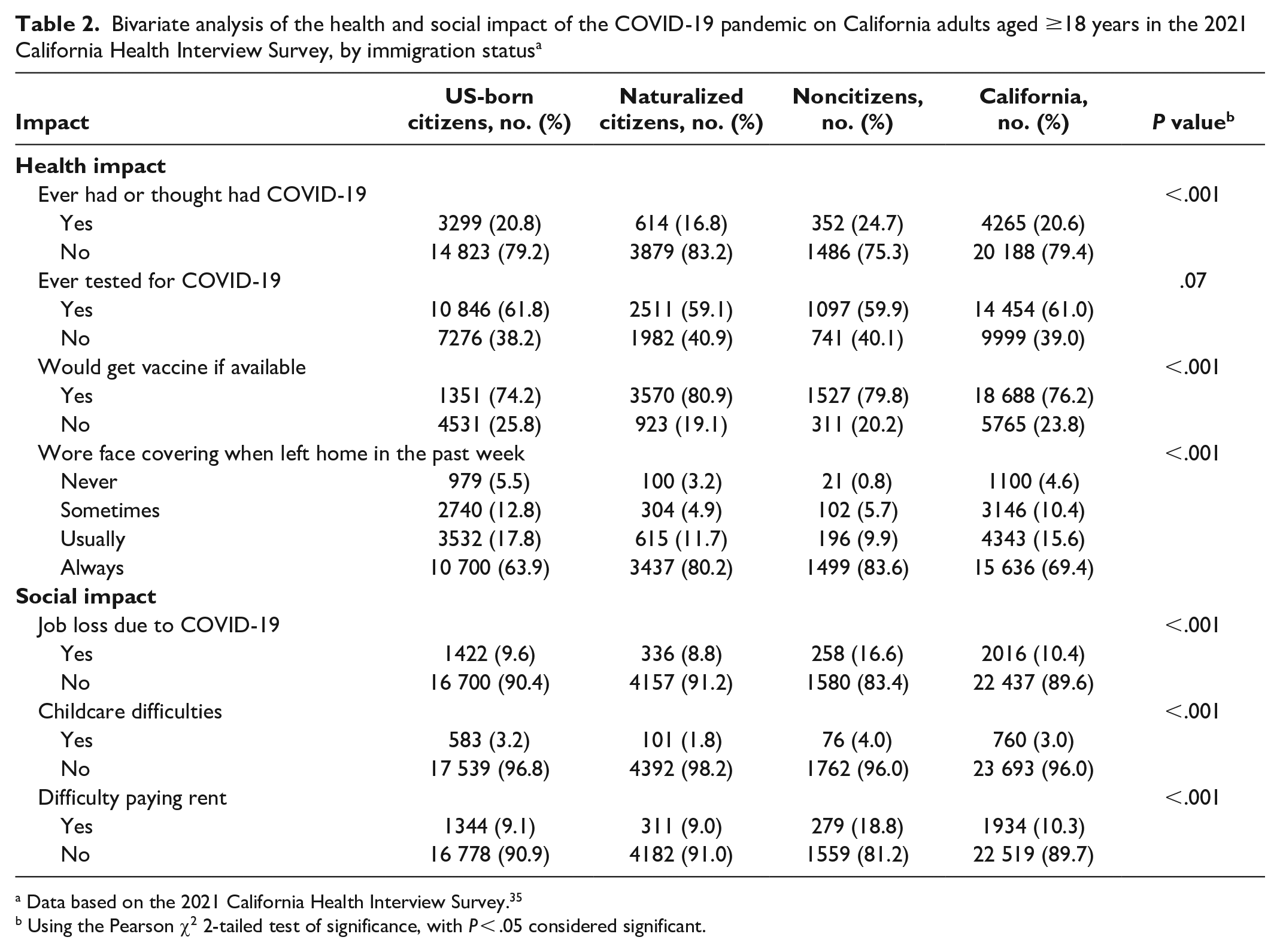
Data based on the 2021 California Health Interview Survey. 35
Using the Pearson χ2 2-tailed test of significance, with P < .05 considered significant.
In the bivariate analysis, noncitizens had the highest rates of having ever had or thought had COVID-19 (24.7%) and had significantly higher rates of always wearing a face covering (83.6%) than US-born citizens (63.9%) (P < .001) (Table 2). Both noncitizens and naturalized citizens had higher rates of reporting would get vaccine if available than US-born citizens. Rates of intention to vaccinate against COVID-19 were highest among naturalized citizens (80.9%), followed by noncitizens (79.8%) and US-born citizens (74.2%). Rates of job loss during the pandemic were highest among noncitizens (16.6%) compared with naturalized citizens (8.8%) and US-born citizens (9.6%). Noncitizens also had significantly higher rates of childcare difficulties (4.0%) compared with US-born citizens (3.2%) (P < .001). Noncitizens had significantly higher rates of difficulty paying rent (18.8%) than US-born citizens (9.1%) (P < .001).
Multivariate analysis revealed significant predictors of health-related outcomes (including ever had or thought had COVID-19, testing for COVID-19, and intention to vaccinate), accounting for sociodemographic characteristics (mainly sex, race and ethnicity, age, education level, poverty level, and employment status) (Table 3). Adults aged 18-39 and 40-59 years had significantly higher odds of ever having had or thought had COVID-19 than adults aged ≥60 years (P < .001). Hispanic/Latinx adults (adjusted odds ratio [aOR] = 1.61; 95% CI, 1.42-1.83) had higher odds of ever having had or thought had COVID-19 than non-Hispanic White adults. Participants with <high school education (aOR = 1.32; 95% CI, 1.11-1.58) or a high school diploma/some college (aOR = 1.24; 95% CI, 1.12-1.36) had significantly higher odds of ever having had or thought had COVID-19 than those with ≥college degree. Noncitizens (vs US-born citizens), those with lower education levels (vs ≥college degree), and adults who were working part-time or unemployed (vs full-time) had lower odds of ever testing for COVID-19. Naturalized citizens (aOR = 1.26; 95% CI, 1.09-1.46) and noncitizens (aOR = 1.27; 95% CI, 1.04-1.54) were significantly more likely to have received or intend to receive the COVID-19 vaccine than US-born citizens. Hispanic/Latinx (aOR = 1.14; 95% CI, 1.00-1.28) and non-Hispanic Asian (aOR = 1.34; 95% CI, 1.15-1.57) adults were significantly more likely than non-Hispanic White adults to get vaccinated.
Multivariate analysis of COVID-19–related outcomes among California adults (N = 24 453) accounting for sociodemographic characteristics a
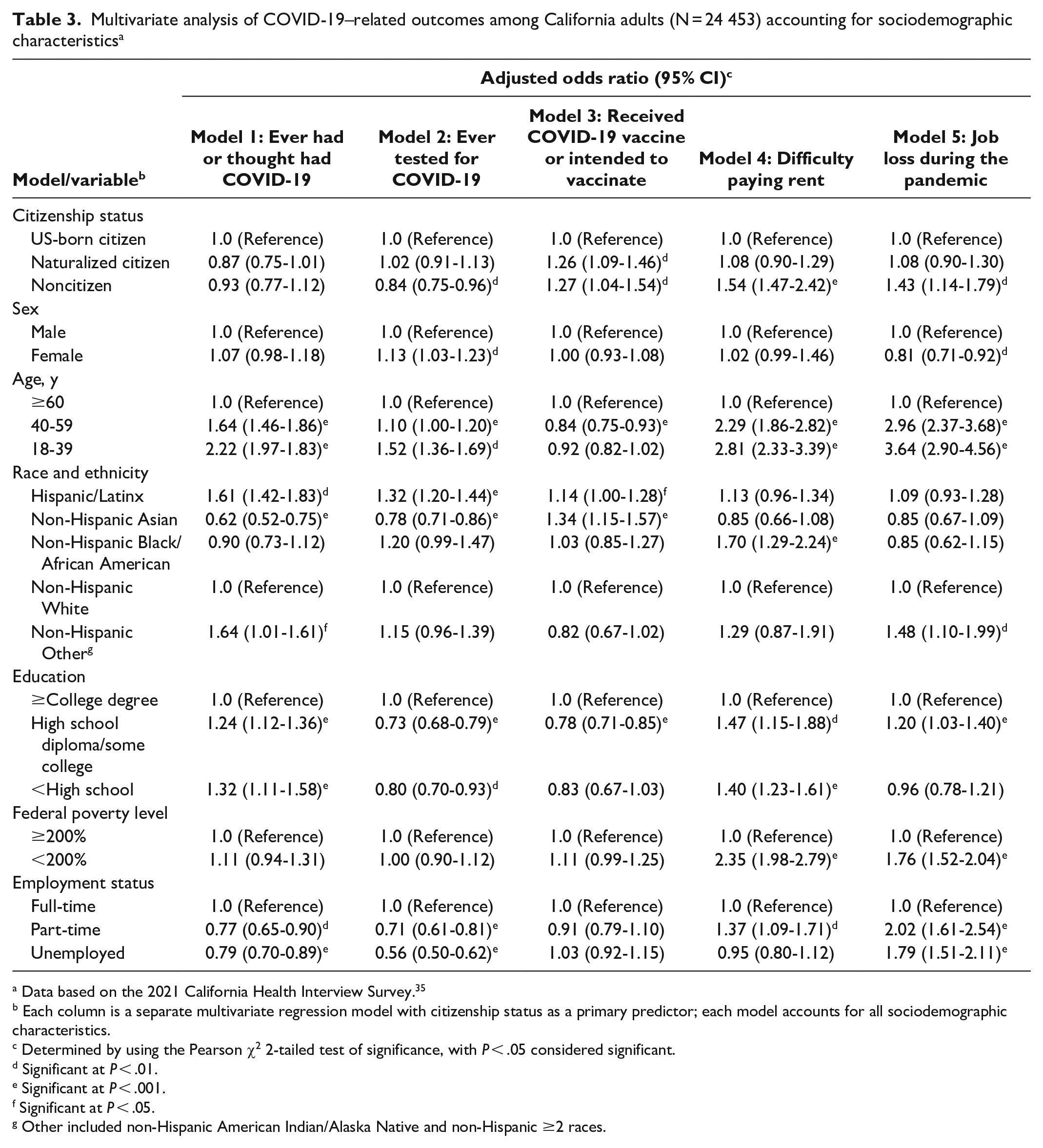
Data based on the 2021 California Health Interview Survey. 35
Each column is a separate multivariate regression model with citizenship status as a primary predictor; each model accounts for all sociodemographic characteristics.
Determined by using the Pearson χ2 2-tailed test of significance, with P < .05 considered significant.
Significant at P < .01.
Significant at P < .001.
Significant at P < .05.
Other included non-Hispanic American Indian/Alaska Native and non-Hispanic ≥2 races.
Noncitizens (aOR = 1.54; 95% CI, 1.47-2.42) had significantly higher odds of difficulty paying rent than US-born citizens (Table 3). Identifying as non-Hispanic Black/African American (aOR = 1.70; 95% CI, 1.29-2.24), having <high school education (aOR = 1.47; 95% CI, 1.15-1.88), living at <200% FPL (aOR = 2.35; 95% CI, 1.98-2.79), and working part-time (aOR = 1.37; 95% CI, 1.09-1.71) were associated with significantly higher odds of difficulty paying rest during the pandemic as compared with those who identified as non-Hispanic White, had ≥college degree, were living at ≥200% FPL, and worked full-time, respectively. Being a noncitizen (aOR = 1.43; 95% CI, 1.14-1.79), being aged 18-39 years (aOR = 3.64; 95% CI, 2.90-4.56) or 40-59 years (aOR = 2.96; 95% CI, 2.37-3.68), being of non-Hispanic Other race and ethnicity (aOR = 1.48; 95% CI, 1.10-1.99), living at <200% FPL (aOR = 1.76; 95% CI, 1.52-2.04), having a high school diploma/some college (aOR = 1.20; 95% CI, 1.03-1.40), and working part-time (aOR = 2.02; 95% CI, 1.61-2.54) or being unemployed (aOR = 1.79; 95% CI, 1.51-2.11) were associated with significantly higher odds of reporting job loss during the pandemic when compared with people who were US-born citizens, aged ≥60 years, non-Hispanic White, living at ≥200% FPL, or working full-time, respectively.
Discussion
In our examination of the impact of the COVID-19 pandemic on California adults by citizenship status, we found disparities across health (eg, COVID-19 infection and risk-reduction behaviors such as testing and wearing face masks) and social (eg, difficulty paying rent and job loss) consequences among California adults. Differences across these outcomes may be influenced by social and economic determinants that affect susceptibility to COVID-19, the precarious workforce in which noncitizens are employed, and the limited resources available (eg, access to testing sites or kits) during the COVID-19 pandemic. Our study highlights the need for more disaggregated data on COVID-19–related outcomes beyond race and ethnicity and the importance of immigration-related variables, such as citizenship status, as critical factors when considering the disproportionate impact of the COVID-19 pandemic on medically underserved populations.14,17,36
Housing Instability
Noncitizen immigrants in California had higher odds of difficulty paying rent than US-born citizens, which may stem from factors contributing to their economic vulnerability and reduced access to social safety nets. Working in low-paying jobs with limited benefits, often within the informal economy, noncitizens may struggle to consistently pay rent. Despite rent-relief policies in California, noncitizens encounter barriers to accessing public assistance programs, such as unemployment insurance, housing subsidies, and food assistance, and these barriers may be due to their immigration status. The “chilling effect” exacerbates this situation, as many noncitizens, out of fear of deportation or harming their future immigration status, might hesitate to seek or entirely avoid seeking public benefits to which they are legally entitled. 37 Furthermore, some federal and state relief programs in California excluded or had limited access for noncitizens, leaving them without adequate financial support in times of crisis. Consequently, noncitizens in California continue to face precarious employment, limited access to social services and benefits, and vulnerability during economic downturns, resulting in difficulties in paying rent and unstable housing.
Job Loss Due to COVID-19
Our findings suggest that the COVID-19 pandemic had a worse social and financial impact on noncitizens than on US-born citizens and on people living at ≥200% FPL than on those living at ≥200% FPL. The Pew Research Center reported that the number of non–US-born workers in the United States decreased by nearly 1 million from 2019 to 2020, with many losing their jobs due to the pandemic. 38 Disparities in job loss and financial insecurity for noncitizens may indicate employment in precarious positions. Other studies, including 1 qualitative study, highlight how immigrant families have experienced negative financial, employment, and health repercussions amid the COVID-19 pandemic.39,40 Recently arrived immigrants reported challenges due to COVID-19, including social–emotional adjustment, financial challenges, and academic difficulties. 39
COVID-19 Infection and Risk-Reduction Behaviors
Our findings suggest that noncitizens in California had high rates of COVID-19 infection or perceived infection, although these results were not significant in the multivariate analysis. Noncitizens demonstrated higher vaccine uptake and more consistent risk-reduction behaviors, such as wearing face coverings, when compared with US-born citizens. These findings may reflect heightened awareness of the risks associated with COVID-19 or immigrants’ greater sense of responsibility to protect themselves and their families and communities, when compared with US-born citizens. Notably, noncitizenship status was an important predictor for COVID-19 or vaccine uptake when accounting for other sociodemographic characteristics. Other studies have found a strong positive correlation between unauthorized immigrants and the prevalence of COVID-19 cases. 41 In our findings, noncitizens had the highest rates of vaccine uptake despite potentially higher exposure rates than US-born citizens. While vaccination trends may vary by region and over time, these findings may be attributed to several factors, including that immigrants compose a substantial share of workers in certain categories that were likely to be included in priority groups for vaccination during this early period of the pandemic or that vaccine uptake was required for employment. 5 Noncitizens’ vaccine uptake may vary because of barriers to access to care and vaccine hesitancy among US immigrants that differ by visa status holders or ethnic groups. It is also possible that strong ties to the community or trust in government or health care agencies may influence vaccine uptake. 42
On the other hand, noncitizens were less likely to have ever been tested for COVID-19 than US-born citizens. Although the availability of testing expanded after 2021—the year data collection occurred—during the height of the pandemic, access to testing may have varied widely across regions of California. This variability could have disproportionately affected noncitizens, who often face additional barriers such as limited health care access, language challenges, concerns about immigration consequences, and misinformation. As a result, these factors may have contributed to the observed lower testing rates among noncitizens than among US-born citizens during the pandemic, highlighting the need for tailored public health interventions to address these disparities and ensure equitable access to testing services for all.
Limitations
This study had several limitations. First, the study included a descriptive analysis and cannot suggest causative mechanisms by which disparities in COVID-19–related outcomes develop and persist. Second, self-reports of COVID-19 (using the question that asked respondents about ever having had or thought had COVID-19) may reflect misinterpretation and recall bias or lack of access to testing. The question relies on individuals’ perceptions of having had COVID-19, which might not align with confirmed diagnoses through testing, leading to potential underreporting. Third, the study was limited to a 1-year period and might not capture the full trajectory of the pandemic’s effects. Some long-term impacts, such as delayed economic repercussions or changes in behavior, might not be fully apparent within a year. Despite these limitations, this study provides a snapshot of this critical period in understanding the complex and evolving nature of the COVID-19 pandemic and underscores the need for ongoing efforts to capture data on the short- and long-term implications of the pandemic.
Conclusion
This study highlights the critical role of citizenship status in understanding the health and social impact of the COVID-19 pandemic on California’s immigrant populations. Notable disparities in COVID-19–related outcomes exist for noncitizens, necessitating focused public health measures to address social determinants of health and sanctuary policies to support them. This study underscores the need for comprehensive data on US immigrants, which can inform evidence-based decision-making and help eliminate health disparities. While collecting citizenship data presents challenges, a need exists to extend research to benefit US immigrants without further marginalizing noncitizen groups. Future research should examine not only individual and social determinants to COVID-19–related outcomes in this population but also the long-term impact of the pandemic on the mental health and well-being of immigrants. By acknowledging the unique challenges faced by immigrants based on their citizenship status, policy makers and public health authorities can work toward creating a more inclusive and resilient society during future public health crises. As we continue to navigate the effects of the pandemic, fostering a deeper understanding of the diverse experiences of immigrant populations will be crucial in promoting health equity and ensuring the well-being of all members of our society.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Siddiq’s and Ms Teklehaimanot’s time is supported by the Charles R Drew University Urban Health Institute through the National Institute on Minority Health and Health Disparities of the National Institutes of Health (NIH) under award no. S21MD000103. Dr Siddiq’s time is also supported through the Clinician Research Education and Career Development program (R25 MD007610). Dr Siddiq also receives funding from the Resource Center for Minority Aging Research/Center for Health Improvement of Minority Elderly (RCMAR/CHIME) under NIH/National Institute on Aging (NIA) (P30-AG021684) and the University of California, Los Angeles Clinical and Translational Science Institute (UL1TR001881). The content of this study does not necessarily represent the official views of NIA or NIH.