
Abstract
Objectives:
The 12-month vaccination campaign ¡Ándale! ¿Qué Esperas? was launched to increase COVID-19 vaccination rates in Latinx populations in California by expanding community outreach. The objectives of this evaluation were to (1) determine predictors of vaccination rates and (2) identify barriers to vaccination and potential solutions.
Methods:
Five community partners in California serving Latinx populations with high social vulnerability participated in the ¡Ándale! ¿Qué Esperas? campaign. Community health workers were hired to deliver outreach (virtual, one-on-one, group based, and information dissemination), vaccinations, and supportive services. We collected data on outreach strategy used (method and location), number of vaccinations provided and reasons for delay, and number of times that supportive services were provided. We used regression models to assess significant predictors of vaccinations and supportive services.
Results:
Community health workers (N = 146) hired from June 1, 2021, through May 31, 2022, performed outreach engagements (n = 6297) and supportive services (n = 313 796), resulting in 130 413 vaccinations and 28 660 vaccine appointments. The number of vaccinations administered was significantly higher at events in which supportive services were provided versus not provided (coefficient = 34.02; 95% CI, 3.34-64.68; P = .03). The odds ratio of supportive services was 3.67 (95% CI, 1.76-7.55) during virtual outreach and 2.95 (95% CI, 2.37-3.69) during one-on-one outreach (P < .001 for both) as compared with information dissemination encounters. Vaccination concerns were reported among 55.0% of vaccinated survey respondents (67.7%, vaccine confidence; 51.7%, access).
Conclusions:
Supportive services facilitate vaccinations, ease transportation and time barriers, and instill confidence among working-class racial and ethnic minority populations.
Latinx communities have been disproportionately affected by the COVID-19 pandemic, facing higher exposure risks, hospitalization rates, mortality rates, and economic repercussions than other racial and ethnic groups.1-3 Social vulnerabilities among Latinx populations—namely, employment in the essential workforce, living in multigenerational homes, and access constraints to COVID-19 testing and vaccinations—are salient determinants of disparate outcomes.1,4,5 California statewide trends closely parallel national trends, with a vaccination rate that is 10% lower among Latinx/Hispanic California residents as compared with non-Latinx/Hispanic White California residents, 6 reflecting potential differences in vaccine confidence and access. 7 Although use of the term Latinx has been debated, it was used throughout the campaign and used herein as a gender-inclusive ethnic label to describe individuals of Latin American origin or descent.8,9
Research has emerged during the COVID-19 pandemic on barriers and facilitators to COVID-19 vaccine access and confidence.7,10-14 Interventions have largely focused on the importance of pop-up vaccination clinics or events10-12; recent research describes the success of vaccination clinics hosted in Latinx neighborhoods in San Francisco, California, that addressed structural barriers to vaccine access. 11 Beyond pop-up clinics, existing literature has converged on the need for community investment, 13 distilled information in English and Spanish,7,10,14 trusted messengers,7,10 community-led messaging,11,14 community health worker (CHW) outreach,12,14 and virtual outreach.12,14 While consensus has developed on community needs, evidence from implementation is limited. The ¡Ándale! ¿Qué Esperas? (AQE) campaign—translating to “Come on! What are you waiting for?”—was established to address this gap, aiming to increase COVID-19 vaccination rates in Latinx communities in California by investing in CHWs to provide culturally and linguistically responsive messaging, education, and outreach.
CHWs have been recognized as vital assets in narrowing gaps in language accessibility, trust or confidence, and health care access because they often reside in the same communities, giving them shared lived experiences and local community insights. 15 Because of their understanding of the community’s needs and assets, CHWs are instrumental in facilitating outreach encounters and providing supportive services (eg, transportation assistance, translation assistance, childcare, education, decision support) when necessary to overcome barriers to care.
Purpose
In this evaluation of the AQE campaign, we sought to (1) determine predictors of vaccination rates and (2) identify barriers and potential solutions to vaccination among populations classified as “hard to reach,” a potentially deceptive label that may overlook the distinction between hard to reach and hard to vaccinate. This label encompasses communities that face barriers such as transportation, legal restrictions, discrimination, financial hardship, time poverty (limited time for engagement beyond employment and caretaking responsibilities), and distrust.16-18 Achievements in vaccination progress and lessons learned from AQE can inform future community and public health interventions during the COVID-19 pandemic and beyond, addressing disparities caused by racism and working toward health equity.
Description of Program Being Evaluated
AQE Campaign
AQE was a 12-month grassroots outreach campaign (June 1, 2021–May 31, 2022) to enhance communications and COVID-19 vaccine access in communities rendered vulnerable to COVID-19 exposure by structural racism and disinvestment that, as a result, encounter barriers to health services. This campaign was implemented in counties in California with substantial (1) social vulnerability, as measured by the Centers for Disease Control and Prevention’s Social Vulnerability Index, 18 and (2) Latinx populations. The AQE campaign was led by AltaMed Health Services as a collaboration among 5 centers: 1 community-based organization (Latino Health Access, serving Orange County) and 4 federally qualified health centers (AltaMed, serving Los Angeles County; Golden Valley Health Center, serving Merced and Stanislaus counties; La Clínica de la Raza, serving Alameda, Contra Costa, and Solano counties; and San Ysidro Health, serving San Diego County). Each center was responsible for hiring CHWs to facilitate community outreach. Evaluation measures included the number and type of outreach encounters executed, number of COVID-19 vaccinations administered, number of vaccine appointments scheduled, self-reported demographic characteristics of those vaccinated, and self-reported reasons for delays in vaccination.
Methods
Outreach and COVID-19 Vaccination
AltaMed and the Latino Coalition for a Healthy California (Sacramento, California) served as the lead agencies to build capacity among centers to conduct outreach, education, and engagements. Each center hired CHWs to deliver a multipronged outreach strategy to increase COVID-19 vaccine access and confidence. The outreach method was categorized as virtual (emails, training sessions, virtual town halls, webinars), one-on-one (door-to-door, text, telephone call), group based (community fairs or events; focus groups; partnerships with local school districts, community centers, and libraries), or information dissemination (social media, flyers, postal mail, advertisements, and websites). Each time that a CHW had an outreach engagement, the CHW collected data on the following items: center affiliation of CHW, the number of individuals reached, location (clinic or community site), outreach method (virtual, one-on-one, group based, information dissemination), supportive services provided (eg, assistance with transportation, translation, technology, childcare, appointment registration following initial encounter), and number of vaccine appointments and vaccinations.
Additionally, those vaccinated were asked to complete a postvaccine survey that captured data on demographic characteristics and reasons for delaying vaccination, which were categorized as being related to the following:
Access: no time off work, transportation barriers, no childcare, not knowing where to get the vaccine, not knowing that the vaccine was free, not being able to make an appointment, incarceration, concerns about immigration status, concerns about legal identification requirement, and recently living outside the United States
Confidence/perception: misinformation, concerns about side effects, not thinking that they were at high risk, not concerned about getting COVID-19, not trusting the health care system, or not trusting vaccines
One center did not implement the postvaccine survey and instead used electronic medical record (EMR) data to report the demographic characteristics of those vaccinated as part of AQE.
We used REDCap (Research Electronic Data Capture) hosted at The Ohio State University for data collection and management. 19 The Claremont Graduate University Institutional Review Board (no. 4084) approved all study procedures.
Evaluation
The Center for Health Outcomes and Policy Evaluation Studies at The Ohio State University managed REDCap and led all campaign evaluation activities. We computed descriptive statistics to analyze aggregate demographic characteristics and outcomes of those vaccinated, with significance of comparisons assessed by the Pearson χ2 test of independence. Denominators varied by indicator because we did not require survey questions to be answered. Additionally, for analysis, we restricted data to those answering the question, including “prefer not to answer” responses; we excluded blank or unanswered responses in denominator counts.
We then developed a logistic regression model to determine which outreach strategies led to greater provision of supportive services during outreach, controlling for period (June–December 2021 and January–May 2022 to account for an updated data collection tool) and center (AltaMed, Golden Valley Health Center, La Clínica, Latino Health Access, and San Ysidro Health) as covariates. We assessed the significance of model parameters using the Wald test. We then developed a linear regression model to assess how outreach characteristics (location, methods, and whether supportive services were provided) contributed to vaccination volume (measured as number of individuals vaccinated) at outreach events, again controlling for period and center as covariates. We assessed the significance of model parameters using the Student t test. We performed all analyses using R version 3.6.2 (R Foundation for Statistical Computing).
Results
Aggregate Data
Participating centers hired 146 CHWs from June 2021 through May 2022 to facilitate outreach. Of 6297 executed outreach engagements, 14.1% (n = 887) were virtual, 30.0% (n = 1892) were one-on-one, 12.5% (n = 787) were group based, 36.0% (n = 2268) were information dissemination, and 7.4% (n = 463) were unspecified. Outreach engagements led to the provision of 313 796 supportive services and facilitated 130 413 COVID-19 vaccinations and 28 660 vaccine appointments. Trends in the number of vaccinations associated with the AQE campaign paralleled California statewide trends. The linear trend was steady from June through October 2021, increased in November 2021, and plateaued in March 2022 (Figure 1). The types of supportive services provided varied by outreach method and overall: transportation assistance (offered at 59.8% of all encounters), vaccine appointment registration (36.9%), education (27.9%), moral support (10.1%), and referrals and linkages to other services or care (9.7%) (Table).
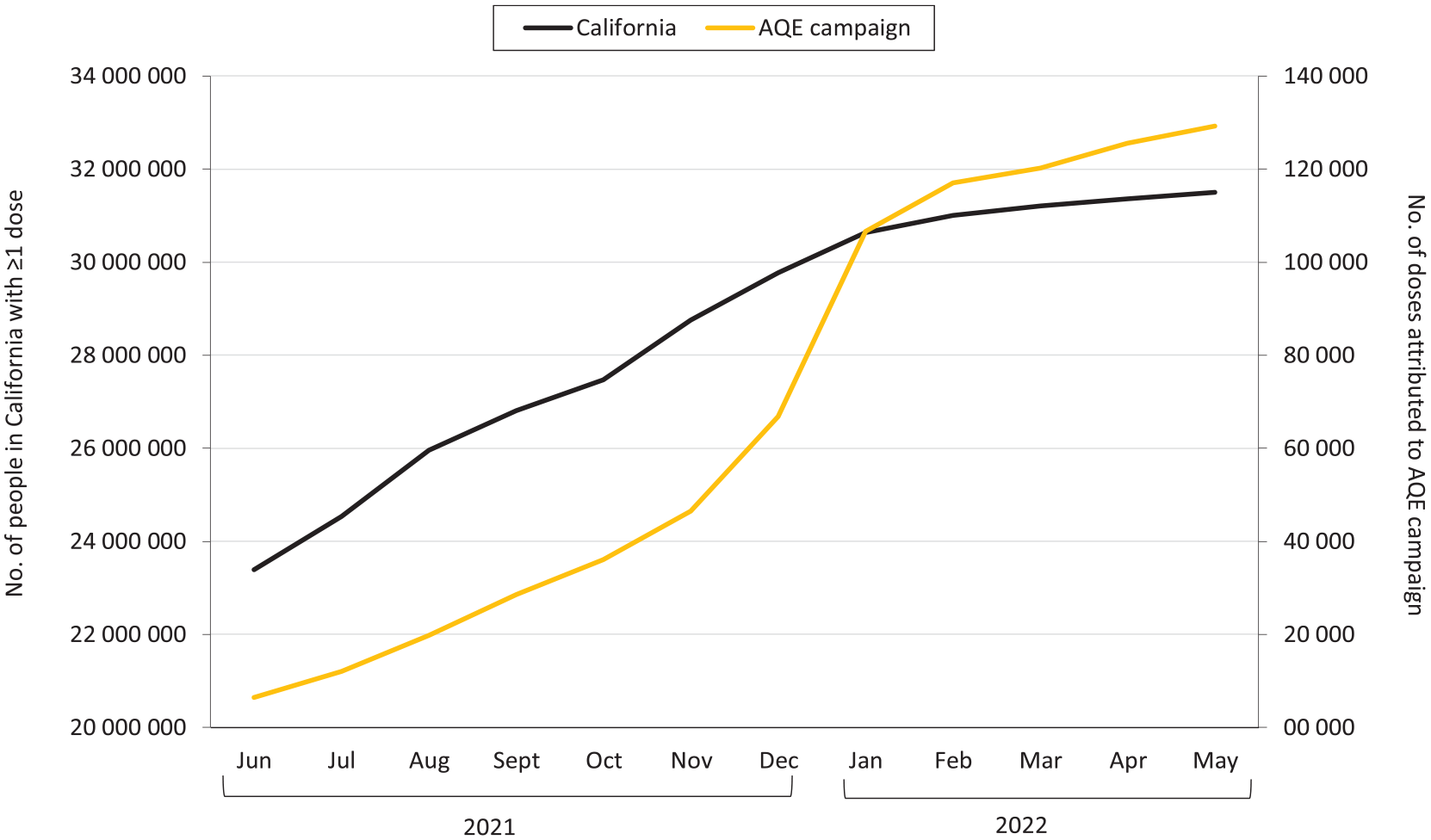
COVID-19 vaccination trends among Latinx populations during the ¡Ándale! ¿Qué Esperas? (AQE) campaign, mapped onto statewide vaccination trends, California, June 2021–May 2022. A total of 130 413 COVID-19 vaccinations were administered in California from June 2021 through May 2022 as part of the AQE campaign. The yellow line indicates a cumulative count of vaccinations attributed to the AQE campaign (n = 129 255); 1158 AQE-associated vaccinations were excluded from analysis because of missing date of administration. The blue line indicates a cumulative count of people in California who had ≥1 dose of the COVID-19 vaccine by the end of the AQE campaign, May 2022 (n = 31 498 986).
Types of supportive services dispensed by community health workers as part of the ¡Ándale! ¿Qué Esperas? campaign, by outreach method, California, June 2021–May 2022 a
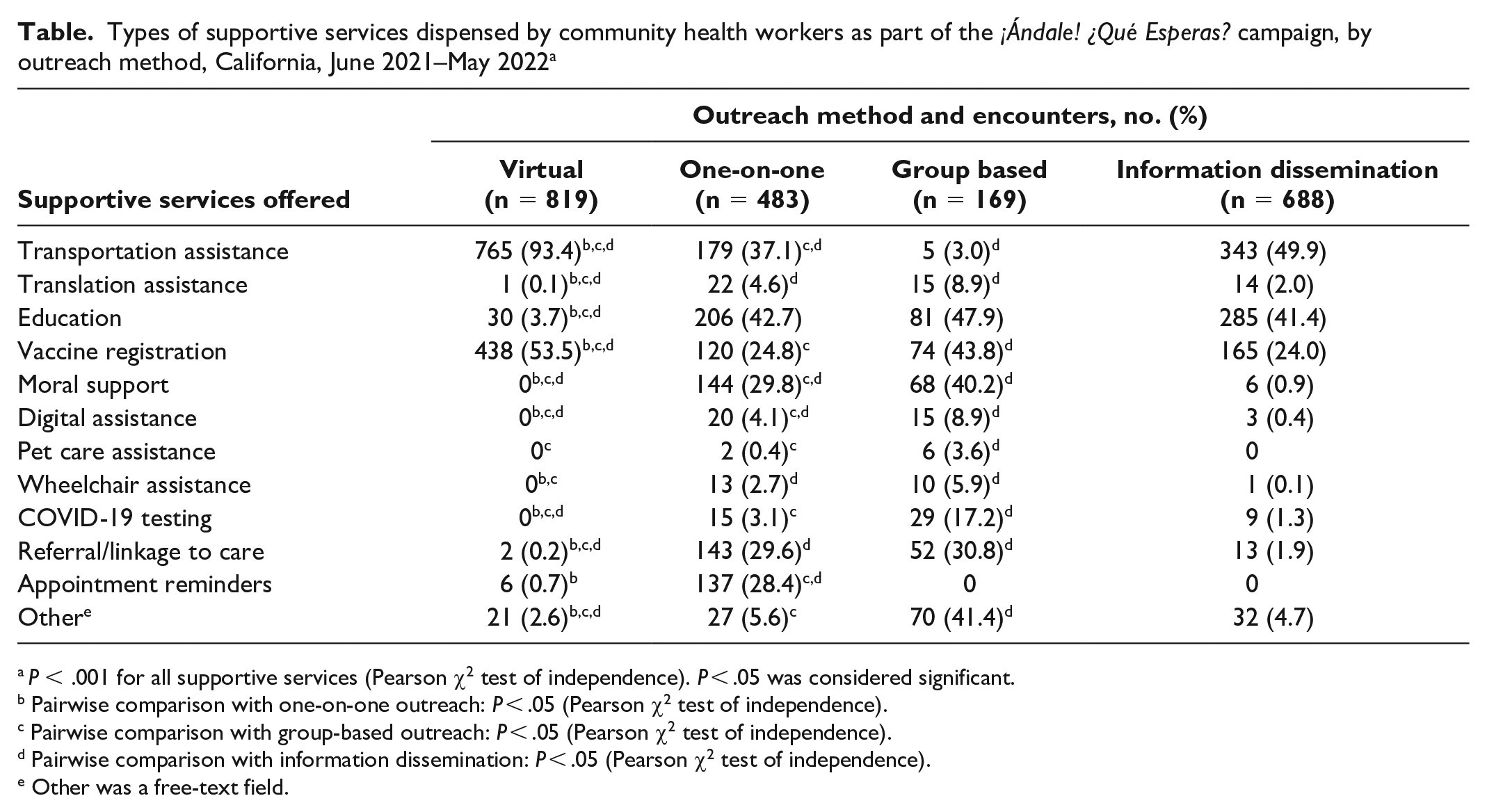
P < .001 for all supportive services (Pearson χ2 test of independence). P < .05 was considered significant.
Pairwise comparison with one-on-one outreach: P < .05 (Pearson χ2 test of independence).
Pairwise comparison with group-based outreach: P < .05 (Pearson χ2 test of independence).
Pairwise comparison with information dissemination: P < .05 (Pearson χ2 test of independence).
Other was a free-text field.
Among those vaccinated through AQE who either completed the postvaccine survey or had an EMR with a partner clinic (n = 79 828), most self-identified as Latinx/Hispanic/Chicanx (80.9%; 57 770 of 71 445), 55.4% (44 228 of 79 824) as female, 66.6% (18 438 of 27 666) as heterosexual, and the median age was 35 years (IQR, 17-55 y).
Regression Analyses
Predictors of supportive services
The odds ratio (OR) of providing supportive services during outreach was greatest for virtual outreach (OR = 3.67; 95% CI, 1.76-7.55), followed by one-on-one (OR = 2.95; 95% CI, 2.37-3.69) and group based (OR = 0.43; 95% CI, 0.33-0.55; all P < .001). Outreach encounters hosted at community sites were not significantly more likely than those hosted at clinic sites to lead to provision of supportive services (OR = 0.92; 95% CI, 0.66-1.28; P = .61).
Predictors of vaccination
Vaccination volume (coefficient = 34.02; 95% CI, 3.24-64.68) was significantly higher at encounters in which supportive services were provided versus not provided (P = .03), when controlled for center and period as covariates. The location of encounters was not significant (P = .43): vaccination volume at community sites was similar to vaccination volume at clinic sites (coefficient = 18.40; 95% CI, –27.64 to 64.44). Similarly, method of outreach was not a significant predictor of vaccination: vaccination volume was not significantly different for encounters by virtual outreach (coefficient = −9.31; 95% CI, –78.59 to 59.97; P = .79), group level (coefficient = 21.63; 95% CI, –11.39 to 54.65; P = .20), or one-on-one (coefficient = 8.23; 95% CI, –20.85 to 37.31; P = .58) as compared with information dissemination.
Barriers to Vaccination
Of the 26 355 vaccinated participants who completed the postvaccine survey, 11 861 (45.0%) reported no concerns or deliberations about getting vaccinated. Those reporting concerns or deliberations cited reasons of perception or confidence in the vaccine (63.4%) and access constraints (51.7%) (Figure 2A). Distrust of vaccines was the primary reason for delay related to perception of or confidence in the vaccine (Figure 2B). Time poverty, transportation, knowledge, cost, and childcare needs contributed to access issues (Figure 2C). Other reasons included concerns about immigration status, legal identification requirement, pregnancy, need for parental consent, waiting for a vaccination mandate from schools or employers, and preexisting medical conditions (Figure 2D). Significant variability existed among sites in the number of supportive services provided per individual vaccinated: 0.07 supportive services were provided for every vaccination administered by AltaMed, 5.57 at Golden Valley Health Center, 2.46 at La Clínica, 1.55 at Latino Health Access, and 1.02 at San Ysidro Health (Figure 3).
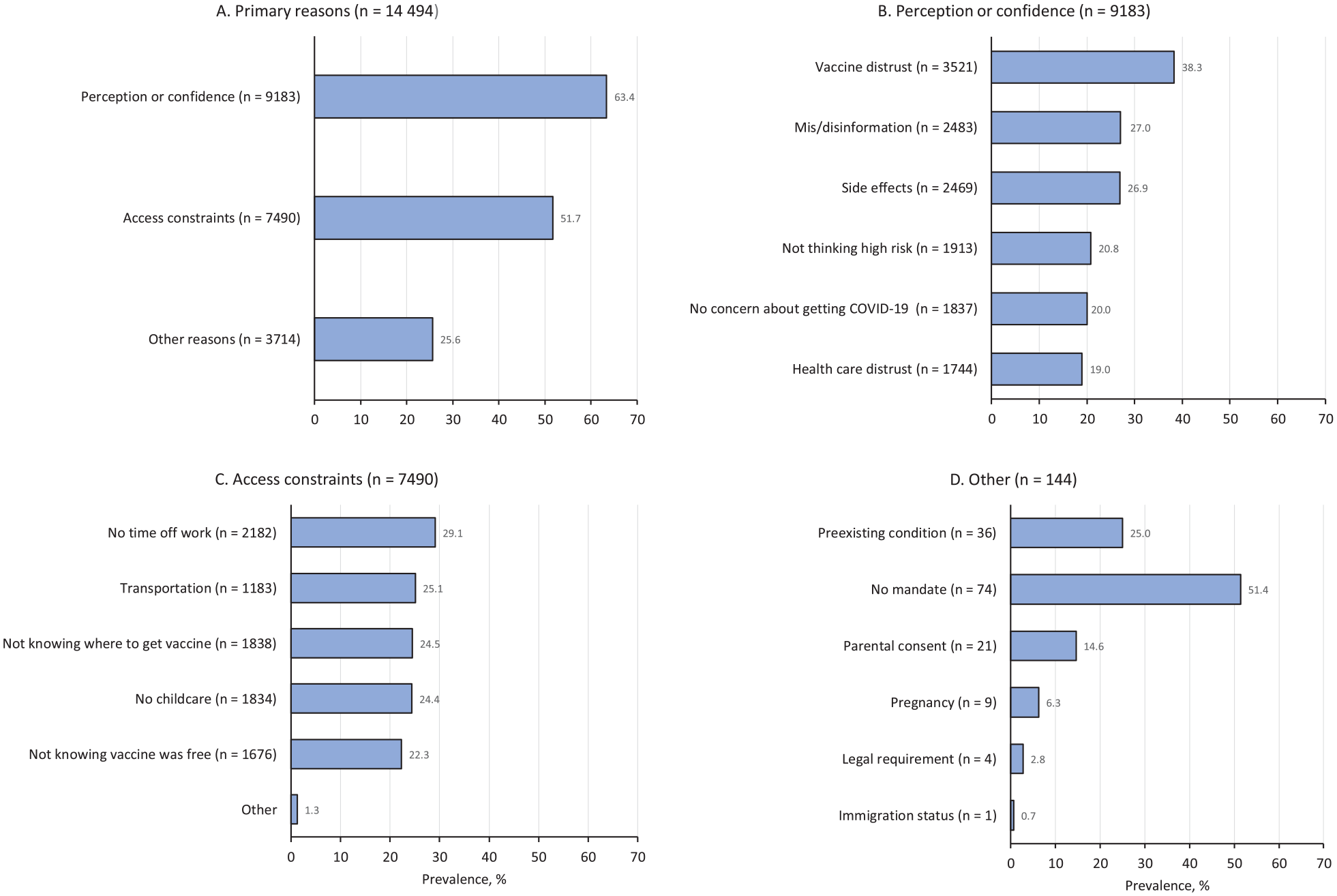
Reasons for delay in COVID-19 vaccinations among Latinx residents in California during the ¡Ándale! ¿Qué Esperas? campaign, June 2021–May 2022: (A) primary reasons, (B) perception or confidence, (C) access constraints, and (D) other reasons. Participants may have reported >1 reason; therefore, data are not exclusive and percentages do not total to 100. Of 3714 respondents who reported other concerns, only 144 specified them. As such, percentages were calculated by using the total number of respondents who specified concerns (n = 144) as the denominator.
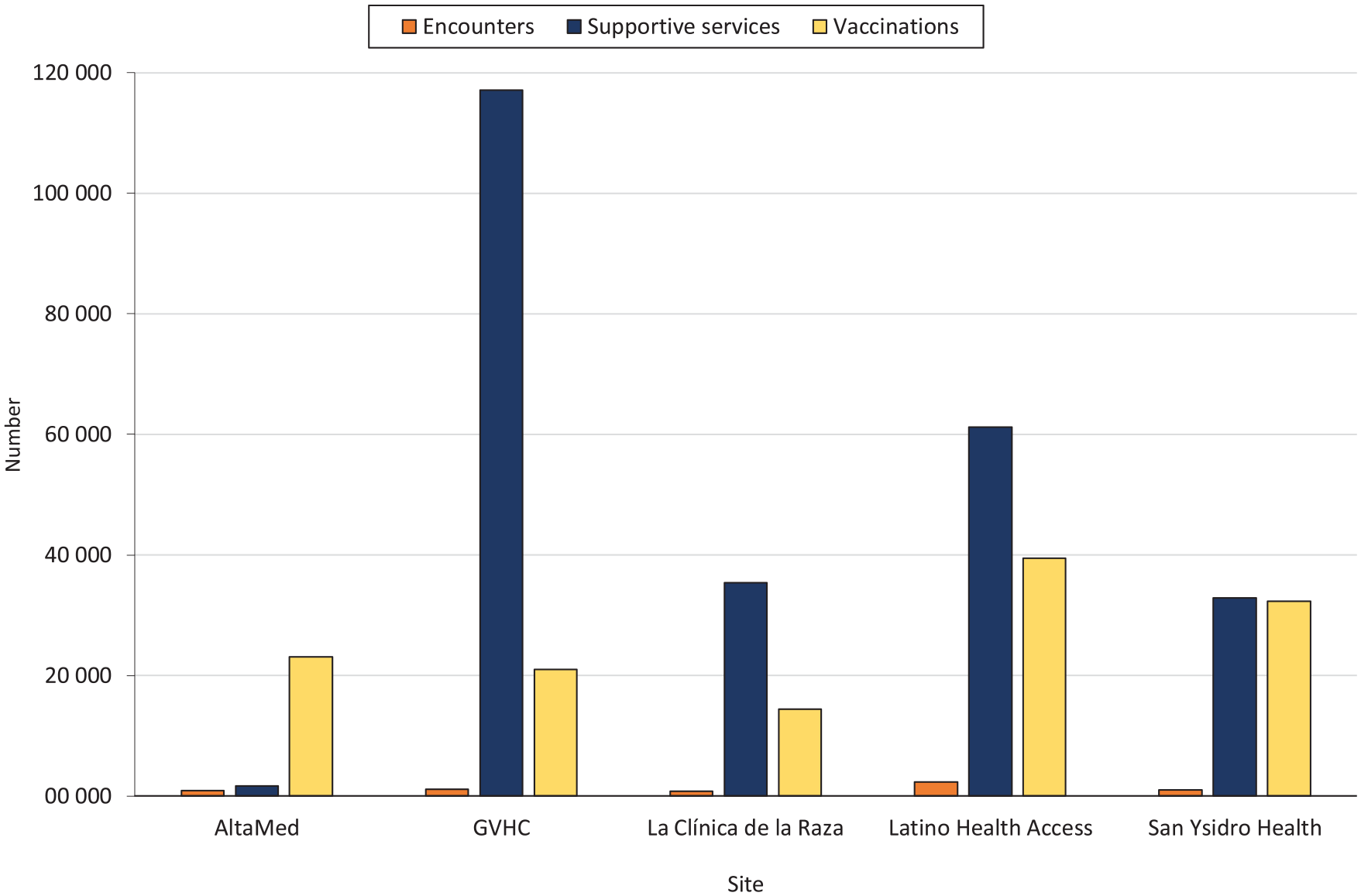
Number of outreach encounters, supportive services, and vaccinations among Latinx populations led by community health workers at each site during the ¡Ándale! ¿Qué Esperas? (AQE) campaign, California, June 2021–May 2022. AltaMed facilitated 953 outreach encounters, 1644 supportive services, and 23 115 vaccinations (0.07 supportive services per vaccination); GVHC, 1132 outreach encounters, 117 109 supportive services, and 21 014 vaccinations (5.57 per vaccination); La Clínica de la Raza, 788 outreach encounters, 35 363 supportive services, and 14 366 vaccinations (2.46 per vaccination); Latino Health Access, 2294 outreach encounters, 61 189 supportive services, and 39 505 vaccinations (1.55 per vaccination); and San Ysidro Health, 982 outreach encounters, 32 891 supportive services, and 32 315 vaccinations (1.02 per vaccination). Site affiliation was missing from 148 outreach encounters (from a total of 6297), 65 600 supportive services (from a total of 313 796), and 98 vaccinations (from a total of 130 413). These encounters are not shown.
Lessons Learned
Outreach Encounters and Barriers to Vaccination
Our study found the following: (1) outreach encounters providing supportive services resulted in increased vaccination rates; (2) the primary barriers to vaccination were related to access constraints or perception of or confidence in the vaccine; and (3) virtual outreach encounters—a relatively new method—likely had great utility in removing barriers to access because they significantly increased the number of appointments and transportation assistance, while other outreach methods (one-on-one, group based, or information dissemination) were likely key in removing educational barriers, thereby increasing confidence. Instead of simply providing information, virtual events—as conducted on platforms that community members were comfortable using (eg, Facebook, Zoom)—offered a forum to ask questions and clarify doubts. Time poverty, which recognizes time as a form of currency that affords individuals the opportunity to engage in activities, was an important barrier addressed at virtual events. 20 Time deficits arise when required activities, such as caregiving and employment, preclude individuals from pursuing other activities, often those that require time away from work or family. 20 Time poverty describes the situation of people living in multigenerational homes and the essential workforce who lack time away from caregiving and employment, respectively, to engage in community events. For some virtual events, Zoom events were simultaneously streamed on Facebook Live to increase accessibility. CHWs provided support to individuals seeking additional assistance to connect to virtual events, working to overcome gaps in digital literacy, but extant research has identified salient disparities in access to broadband internet, which is required for participation in virtual events.21,22 Therefore, multipronged outreach strategies (ie, virtual and one of the other outreach methods) may be the most beneficial in increasing vaccination rates by maximizing reach, instilling confidence, and addressing access constraints.
Vaccine Confidence and Access
The increase in vaccinations in November 2021, as observed in campaign trends and statewide trends, was likely due to expanded vaccine eligibility because the Centers for Disease Control and Prevention recommended that children aged 5-11 years be vaccinated against COVID-19. 23 Such a convergence in trends between the AQE campaign and California State points to the value in AQE’s delivery model in increasing vaccinations among communities rendered vulnerable by structural violence, based on a CHW model that focused on building confidence via health education and addressing barriers to access, offering supportive services, and conducting in-person and virtual outreach.
Findings from this evaluation add to and challenge the narrative on vaccine hesitancy. In the earliest days of the COVID-19 vaccine rollout, vaccine hesitancy materialized as one explanation of disparate vaccination rates by race and ethnicity. 23 Emerging evidence challenges this narrative, finding no consistent racial or ethnic pattern in vaccine reluctance 24 and comparable rates of hesitancy among Black and White people in the United States. 25 Moreover, as vaccines became widely available in the United States, racial and ethnic minority groups were more likely than White people to overcome any hesitancies and participate in vaccination programs.24,25 For this reason, we used the term deliberations rather than hesitancies or hesitations when reporting results, in accordance with a recommendation by Corbie-Smith, 23 because it acknowledges that individuals must confront the tensions between evidence of vaccine efficacy and the history of racism in medical and scientific research. 23 Our study found that approximately half of those who received a vaccine during the campaign reported no concerns or deliberations, most of whom identified as Hispanic, Latinx, or Chicanx. Among those reporting concerns, they were most often due to confidence in the vaccine, potentially stemming from justified institutional mistrust and historical and contemporary experiences of racism.23,25 This mistrust and experience are especially relevant in Latinx communities, which have been marginalized by public charge rules that discourage the use of health care services, as this can negatively impact applications for permanent residency.26,27
Beyond vaccine confidence, access constraints were cited as reasons for delays in vaccination among more than half of survey respondents who reported deliberations or concerns. Supportive services were essential in increasing vaccination rates, considering that the most significant predictor of vaccination at outreach events was whether supportive services were offered. This finding aligns with existing literature demonstrating that, to increase vaccination uptake, pressing social needs must be addressed prior to or in parallel with vaccination. 28 CHWs are well positioned to address these additional needs because of their presence in the community, shared lived experience, and pulse on community needs. 28 Although we found salient differences among sites in the number of supportive services per vaccination achieved, the AQE campaign demonstrates that the provision of supportive services does not require large-scale costly events. This finding is important for community-based organizations and federally qualified health centers, which operate CHW programs. Supportive services that are responsive to individual barriers to access were just as likely to be identified and provided in the community as they were in the clinic, and virtual and one-on-one outreach methods were the most likely to dispense supportive services. Virtual outreach methods were particularly effective in offering transportation assistance, but in the COVID-19 era and beyond, virtual events could give options for translation assistance and follow-up appointment reminders via email or text to increase vaccination rates.
In a recent qualitative study, Latinx participants discussed the importance of social support or accompaniment, trusted messengers, representation, community partnerships, and multilingual support in instilling confidence in the vaccine and addressing structural barriers to vaccine access. 10 Each facilitator underscores the importance of CHWs: not only can their local expertise reach communities deemed hard to reach, but they can also effectively engage community members by using culturally relevant messaging, offering linguistically accessible information, and addressing access constraints. 15 AQE confirms and extends these findings, demonstrating the importance of investing in CHWs. 13 Specifically, CHWs affiliated with AQE were able to feasibly and effectively meet people where they were, using various outreach modalities (virtual outreach, community events, and one-on-one exchanges), distilling educational information, providing supportive services, and developing culturally relevant and linguistically accessible messaging that appealed to the needs, concerns, and deliberations of the community. In this way, CHWs were able to address concerns related to vaccine confidence and access, increase vaccination uptake while meeting other social needs, and promote long-term recovery among Latinx communities.
Limitations
This evaluation had several limitations. First, 1 of the 5 participating clinics reported demographic data from EMRs, which are self-reported but may be less reliable than demographic data collected by surveys. Specifically, our survey tools were designed in consultation with clinic administrators at the participating centers to ensure inclusion of the full range of ethnic identity terms (ie, Latino, Latina, Latinx, Hispanic, Mexican, Chicano, Chicana, and Chicanx).8,9 Second, we could not differentiate first series vaccinations from booster vaccinations, which hindered our ability to assess which strategies were most effective in each case. Third, strategies from this campaign were tailored to meet the needs of Latinx communities across California and may not be generalizable to other US communities. This campaign illustrates, however, that the most effective strategies rely on the expertise and lived experiences of the community in understanding the problem and creating solutions.
Conclusions
Supportive services facilitate vaccinations by removing barriers to COVID-19 vaccine access and confidence. Virtual outreach encounters offer a feasible mechanism for providing supportive services by easing access and decreasing transportation barriers, time poverty, and overall costs for working-class racial and ethnic minority communities. Given their local expertise and shared lived experience, CHWs are well positioned to deliver outreach services that overcome barriers to engagement and lead encounters that build trust and confidence in public health interventions. Lessons learned from AQE can inform interventions to address entrenched inequities that have been magnified by the pandemic, engaging in immediate recovery efforts and long-term rebuilding to advance health equity.
Footnotes
Acknowledgements
The authors thank Kathryn Hasenstab-Kenney, BS, for assistance with the manuscript-writing process. The authors also extend their sincere appreciation to all the community health workers who have championed health equity throughout the AQE campaign, as well as to implementation partners at AltaMed Health Services (Aileen Navarrete, MPH; Jasmin Navarrete, BA; An Nguyen, BA; Adelin Tiburcio, BA; Rosa Vazquez, AB), Golden Valley Health Center (Alysse Giles, MBA; Priti Golechha, MD; Kaitlyn McIntire, MPH; Myisha Reed, BA), La Clínica de la Raza (Paulina Avila-Martinez, MPH; Viola Lujan, BA; Maria Reyes, MPH; Claudia Rodriguez-Briones, BS), Latino Health Access (Ana Alvaredo, BA; Patricia Cantero, PhD; Nancy Mejia, MPH, MSW; Marcela Ortiz, BS; Alejandra Rosales, BS; Loreta Ruiz, BA), San Ysidro Health (Adriana Bearse, MPH; Ana Melgoza, MA; Fatima Muñoz, MD, MPH), and Latino Coalition for a Healthy California and Fourth Street Bridge Strategies (Esteban Garcia, MPhil; Octavio González, MPP).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ¡Ándale! ¿Qué Esperas? campaign was funded by the Health Resources and Services Administration (grant U3S42190). Data management was supported by The Ohio State University Center for Clinical and Translational Science (National Center for Advancing Translational Sciences, grant UL1TR001070).