
Abstract
Objectives:
Among graduate public health students, Black, Indigenous, and other people of color (BIPOC; including Latinx, Asian, Middle Eastern and North African, Native Hawaiian and Pacific Islander, and multiracial) experience educational and personal challenges that require institutional support and reform. The objective of this study was to evaluate the effects of an antiracist mentorship program on the sense of belonging and overall experience among BIPOC and first-generation students at Columbia University Mailman School of Public Health in New York City.
Methods:
We used 2 data sources to retrospectively evaluate experiences of BIPOC and first-generation graduate students: the 2021 Mentoring of Students and Igniting Community (MOSAIC) Student Survey (n = 39), which collected data on experiences of students who participated in the MOSAIC program, and the 2016-2020 Graduate Exit Surveys (n = 1222), which collected data on graduating students’ experiences, satisfaction, and perspectives on diversity, equity, and inclusion. A difference-in-difference analysis compared overall experience, public health career preparedness, quality of life, and department satisfaction among all students before (2016-2018) and after (2019-2020) implementation of the MOSAIC program.
Results:
Satisfaction among graduate students attributable to the MOSAIC program introduced in 2019 increased by about 25%. Compared with students who had not been exposed to MOSAIC, students exposed to MOSAIC had a 25% positive difference (P = .003) in overall graduate school experience, a 28% difference (P < .001) in quality of life, and a 10% difference (P = .001) in satisfaction with their departments.
Conclusion:
Mentorship for BIPOC and first-generation public health graduate students offers an effective strategy to improve student experiences and satisfaction with graduate departments and, ultimately, may help students meet educational and professional goals.
The graduate school experience differs substantially between students who are White and those who are historically oppressed and marginalized, including Black, Indigenous, and other people of color (BIPOC; including Latinx, Asian, Middle Eastern and North African, Native Hawaiian and Pacific Islander, and multiracial).1-4 Negative experiences of BIPOC graduate students have included lack of institutional support, difficulty fostering relationships with faculty, limited career preparedness, and trouble finding community among peers.1,3,5 For BIPOC graduate students, structural racism, oppressive institutional systems (eg, graduate schools), and national occurrences of racial violence perpetuate vicious cycles of abuse and impede their sense of belonging.6-9 First-generation students experience their own distinct challenges, such as limited academic preparedness, strained support from families, and culture shock, all of which can exacerbate depression, decrease retention, and obstruct a sense of belonging. 10 It is imperative that schools and programs of public health meet the evolving needs of first-generation and racially and ethnically marginalized student populations to protect their health and well-being and to deconstruct existing inequities.11,12 Remedying negative experiences among BIPOC graduate students not only is important for academic success, degree completion, and career progress1,13 but also is relevant as an indication of student wellness and quality of life.
Institutional support, mentorship, and community can affect the overall well-being of graduate students. Graduate student well-being has been shown to be closely tied to financial stability, career prospects, advisor relationships, overall health, and social support. 5 Learning environments that are safe and inclusive and that acknowledge BIPOC student identities are also essential for retaining BIPOC students in graduate programs, including schools and programs of public health. 13 Being able to find belonging in a graduate school is positively correlated with successful degree completion and can bolster academic and personal experiences.14,15 Addressing challenges faced by BIPOC graduate students directly benefits antioppressive and antiracist goals of graduate schools and ensures the success of graduate students in academic programs and professional lives. 12 Thus, fostering a sense of belonging is especially critical for BIPOC and first-generation students attending predominantly White institutions, particularly large research-focused universities.
One strategy to create community and belonging is mentorship. Mentorship is recognized as essential in equipping graduate students with the necessary tools to thrive academically, advance in their careers, and enrich their institutional environments.16-19 Peer-to-peer mentorship programs are commonplace for BIPOC students. 20 However, comprehensive faculty-to-student mentorship programs at the graduate level for historically oppressed groups, including BIPOC and first-generation students, are uncommon.12,19,21 Mentorship of any kind can positively affect graduate student mental health and well-being.22-24
Although the benefits of mentorship for minoritized racial and ethnic graduate students have been reported,21,24 no previous studies, to our knowledge, have considered the effects of a graduate-level mentorship program on the well-being of first-generation and BIPOC students at a school or program of public health. One opportunity to examine the effects of faculty-to-student mentorship on the well-being of underrepresented graduate students is the Mentoring of Students and Igniting Community (MOSAIC) program, which was established in 2019 at Columbia University Mailman School of Public Health. 12 MOSAIC offers comprehensive faculty-to-student peer mentorship across 5 domains: professional development, faculty mentorship, navigating institutions, incident management, and guest speakers, including connections to faculty, alumni, and community leaders. 12 The MOSAIC program includes graduate students who self-identify as BIPOC and/or as first-generation graduate students. In this study, we used schoolwide data on academic satisfaction and a targeted survey of MOSAIC students to evaluate the effects of MOSAIC on BIPOC students’ sense of belonging and overall experience in a graduate school of public health.
Methods
Data and Sample
We used 2 data sources to retrospectively evaluate the effects of MOSAIC on BIPOC and first-generation graduate students at the Columbia University Mailman School of Public Health: the 2021 MOSAIC Student Survey and Graduate Exit Surveys from 2016-2020. One author (M.W.) distributed the 2021 MOSAIC Student Survey to participating MOSAIC students at the end of the 2021 academic year. The MOSAIC Student Survey, using Qualtrics Survey software (Qualtrics XM), collects self-reported demographic data, reasons for joining MOSAIC, and whether outcomes were improved across several domains, including faculty mentorship, professional development, and a sense of community. The same author (M.W.) sent MOSAIC students an email to the listserv containing a link to the Qualtrics surveys in June 2021 and sent weekly reminders for 1 month. Participants received $25 upon completion of the survey. The analytic sample for the 2021 MOSAIC Student Survey includes all current MOSAIC students who responded to the survey (response rate of 41%) in June 2021 (n = 39).
The Office of Education at the Mailman School of Public Health conducts the Graduate Exit Survey and compiled sequential cross-sectional survey data from 2016-2020. The Office of Education distributes the Graduate Exit Survey to all graduating master of public health (MPH) students via email and collects data on student demographic characteristics, experiences, satisfaction, and diversity goals, including the graduate student’s overall experiences in the MPH program, connections to other students, and preparedness to demonstrate competencies postgraduation. For the 2016-2020 Graduate Exit Survey analytic sample, we included all students who responded to the survey when it was released to their cohort at the time of graduation (eg, students graduating in May would receive the survey in May; n = 1222). The Office of Education reported the following Graduate Exit Survey response rates: 74% in 2016, 70% in 2017, 63% in 2018, 68% in 2019, and 45% in 2020.
From 2016 through 2018, MOSAIC did not exist; however, for the 2019 and 2020 Graduate Exit Surveys, MOSAIC was part of the educational program. Thus, for the MOSAIC sample for the Graduate Exit Survey, we included all self-identified BIPOC students in 2019 and 2020 when participation in MOSAIC was plausible (n = 116). Non-Hispanic White first-generation graduate students are welcome in MOSAIC; however, the Graduate Exit Survey has no measure of first-generation status. The Graduate Exit Survey covers various cohorts of graduating students who complete their degree by the year in which the Graduate Exit Survey is administered (eg, in 2020, all students completing their degree that year were included).
The Office of Education fields both the Graduate Exit Survey and MOSAIC Student Survey and merged and deidentified the 2016-2020 Graduate Exit Survey data prior to our analyses to protect participant confidentiality. Students consent when they opt into the Graduate Exit Survey and MOSAIC Student Survey. We used a difference-in-difference analysis for the Graduate Student Survey. The Columbia University Irving Medical Center Institutional Review Board (IRB-AAAT5993) approved the study.
MOSAIC Student Survey
We included the following demographic characteristics from the MOSAIC Student Survey: race and ethnicity (Hispanic, Asian, Black, non-Hispanic White, Middle Eastern, ≥2 races, race unknown, non–US resident), gender (female, male, gender nonconforming), identification (ie, as first-generation student, BIPOC, or both), academic department (Population & Family Health, Sociomedical Sciences, Epidemiology, Environmental Health Sciences, General Public Health, Health Policy & Management, Biostatistics), and graduate program start year (2014-2015, 2016-2018, 2019-2020). The MOSAIC Student Survey included as outcome measures 6 measures across the 5 domains that MOSAIC aims to serve: community, access to faculty, professional development, skill development, and informal interactions.
We based the categorical measure of “MOSAIC meets all needs” on the question, “Do you feel MOSAIC meets your needs as a student?” with 0 = no, 1 = some, 2 = yes, and all indicating whether some or all needs of the student were met. For community, access to faculty, professional development, skill development, and informal interactions, survey responses were coded as 0 = no and 1 = yes for questions assessing needs across specific domains. Accordingly, these outcomes were based on the following 5 survey items: (1) “Was your need for community met through MOSAIC?” (2) “Did MOSAIC increase your access to faculty?” (3) “Did MOSAIC provide professional development opportunities?” (4) “Did MOSAIC provide space for informal discussion?” and (5) “Have you gained a skill because of MOSAIC?”
The MOSAIC Student Survey also included open-ended questions about what aspects of academic life MOSAIC fulfilled for them, why they attended MOSAIC meetings, whether and how MOSAIC increased their access to faculty, what professional development opportunities were helpful, and what additional opportunities could have been helpful.
Graduate Exit Survey
The Graduate Exit Survey also included questions on race and ethnicity, gender, academic department, and start year. The Graduate Exit Survey outcomes were 4 measures of graduate student satisfaction with their overall experience, public health career preparedness, quality of life, and department satisfaction.
Overall experience was based on students’ satisfaction with their overall experience (negative = 0, positive = 1). Public health career preparedness was based on a response of dissatisfied (coded as 0) or satisfied (coded as 1) to the question, “How satisfied are you with how well your program prepared you for a career in public health?” Quality of life and department satisfaction were coded in the same way (dissatisfied = 0, satisfied = 1) based on responses to the question, “How satisfied are you with overall quality of student life?” and “How satisfied are you with your academic department?” These dichotomous outcomes were the primary outcomes of interest for the difference-in-difference analysis.
Exposure to the MOSAIC Program
We defined the exposure based on the implementation of the MOSAIC program. MOSAIC was implemented in 2019 and designed to serve students who identify as BIPOC or first-generation students. We categorized students as having been exposed to MOSAIC if MOSAIC existed during the full academic year (start year of 2019) and if students self-identified as any racial and ethnic category except non-Hispanic White. Although all BIPOC students in 2019 and 2020 did not participate in MOSAIC, the option to participate was available, and we assumed a diffusion of the effect for the institution and all BIPOC students.
Analysis
We first examined sample characteristics and frequency distributions of variables in the 2021 MOSAIC Student Survey and the 2016-2020 Graduate Exit Surveys. We then stratified student characteristics for the 2016-2020 Graduate Exit Surveys by exposure to MOSAIC. For the 2021 MOSAIC Student Survey, we considered differences in the distribution of measures of MOSAIC student outcomes by race and ethnicity and first-generation identity and used the Pearson χ2 test of significance, considering P < .05 significant. We also reviewed the open-ended responses and identified common themes. For the 2016-2020 Graduate Exit Surveys, we calculated differences in distributions of outcome measures of graduate student satisfaction between students exposed to MOSAIC, as indicated by graduation years 2019 and 2020, and those who were not exposed, as indicated by graduation years 2016, 2017, and 2018. Because MOSAIC was started in 2019, we determined that students exposed to MOSAIC had start years from 2017 through 2020. In bivariable analyses, we used the Pearson χ2 test of significance, considering P < .05 significant.
Using difference-in-difference analysis, an approach that entails comparing mean changes in a treatment group outcome before and after a policy change 25 (in this case, the presence of MOSAIC at the school) with mean changes in a control group outcome with no policy change, we estimated the association between implementation of MOSAIC and overall experience, public health career preparedness, quality of life, and department satisfaction among students.25,26 The difference-in-difference approach requires that baseline temporal trends (but not in absolute levels) of the outcome were equivalent among students who were and were not exposed to the MOSAIC program; the corollary is that the trends among students would have continued to be the same in the absence of implementation of the MOSAIC program (parallel trends). We estimated a linear difference-in-difference model with a binary indicator for MOSAIC exposure, with year fixed effects and with controls for gender and academic department. We estimated the final models with wild cluster bootstrapped SEs.
Results
Student Characteristics
Thirty-nine students responded to the 2021 MOSAIC Student Survey, and 1222 students responded to the 2016-2020 Graduate Exit Surveys (Table 1). Among students who responded to the MOSAIC Student Survey, 33.3% (n = 13) identified as Black, 38.5% (n = 15) as Asian, 12.8% (n = 5) as Hispanic, 7.7% (n = 3) as Middle Eastern, and 7.7% (n = 3) as ≥2 races or ethnicities. Thirty-five (89.7%) MOSAIC students identified as female, and 19 (48.7%) respondents were first-generation students. Most respondents (76.9%) were in the Heilbrunn Department of Population & Family Health, and 20.5% of students were in the Sociomedical Sciences or Epidemiology departments.
Demographic characteristics of respondents to the 2021 MOSAIC Student Survey and the 2016-2020 Graduate Exit Surveys, Columbia University Mailman School of Public Health a
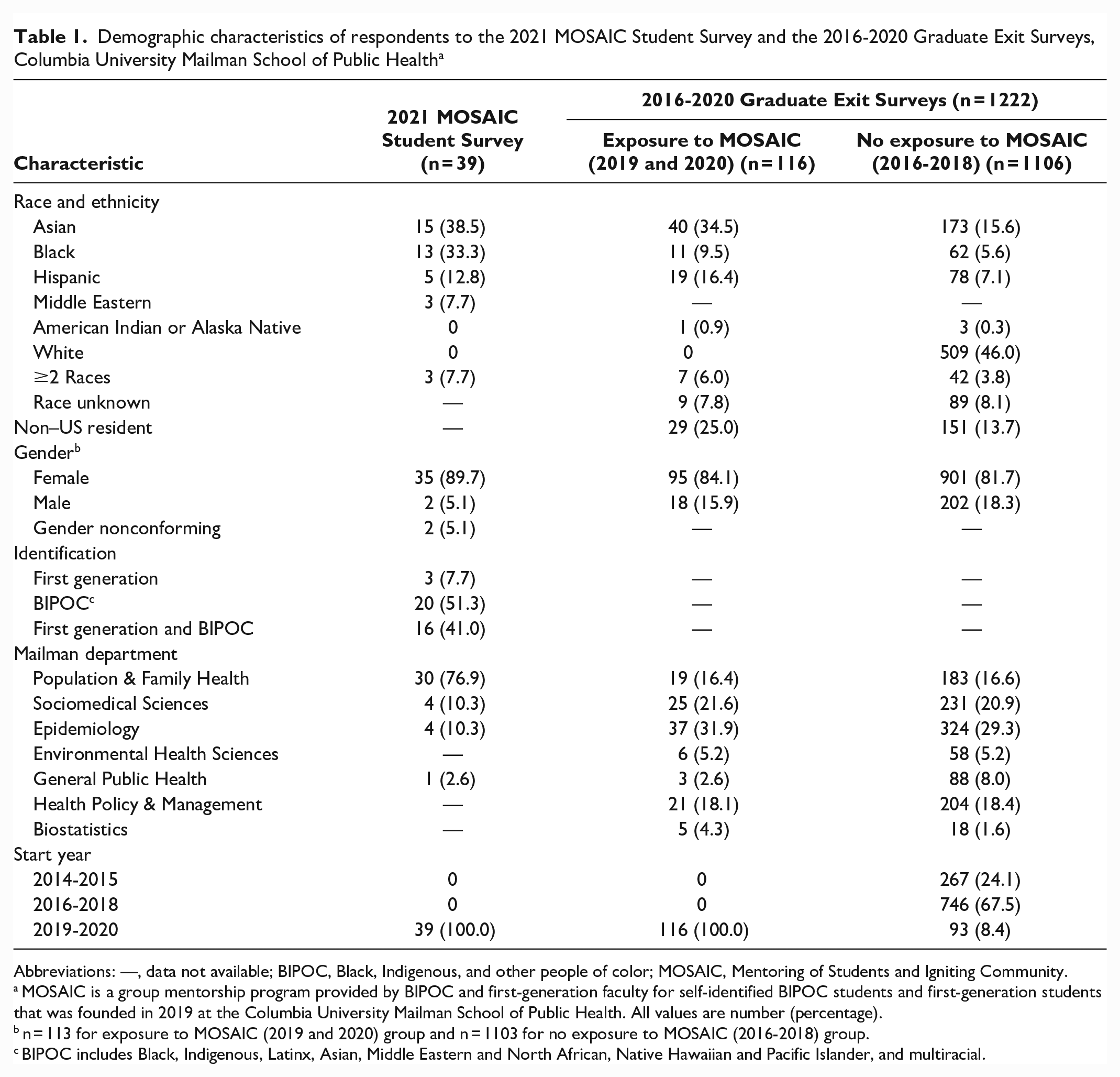
Abbreviations: —, data not available; BIPOC, Black, Indigenous, and other people of color; MOSAIC, Mentoring of Students and Igniting Community.
MOSAIC is a group mentorship program provided by BIPOC and first-generation faculty for self-identified BIPOC students and first-generation students that was founded in 2019 at the Columbia University Mailman School of Public Health. All values are number (percentage).
n = 113 for exposure to MOSAIC (2019 and 2020) group and n = 1103 for no exposure to MOSAIC (2016-2018) group.
BIPOC includes Black, Indigenous, Latinx, Asian, Middle Eastern and North African, Native Hawaiian and Pacific Islander, and multiracial.
At the school-wide level, the 2016-2020 Graduate Exit Surveys showed that, of students exposed to MOSAIC (n = 116), 9.5% (n = 11) were Black, 34.5% (n = 40) were Asian, 16.4% (n = 19) were Hispanic, and 6.0% (n = 7) were ≥2 races; 25.0% (n = 29) were non–US residents. Among respondents not exposed to MOSAIC (n = 1106), 5.6% (n = 62) were Black, 15.6% (n = 173) were Asian, 7.1% (n = 78) were Hispanic, 46.0% (n = 509) were White, 3.8% (n = 42) were ≥2 races, and 13.7% (n = 151) were non–US residents. Similar to findings in the 2021 MOSAIC Student Survey, in the Graduate Exit Surveys, 84.1% of students exposed to MOSAIC identified as female and 81.7% of students not exposed to MOSAIC identified as female. For students exposed to MOSAIC, department distribution included 16.4% in Population & Family Health and 53.5% in Sociomedical Sciences or Epidemiology.
2016-2020 Graduate Exit Surveys
We found minimal differences in graduate student satisfaction between those exposed and not exposed to MOSAIC (Table 2). For quality of life, students with potential exposure to MOSAIC reported 74.1% satisfaction, and students not exposed to MOSAIC reported 58.9% satisfaction.
Graduate student satisfaction, stratified by participation in MOSAIC, according to Graduate Exit Surveys, 2016-2020, Columbia University Mailman School of Public Health a
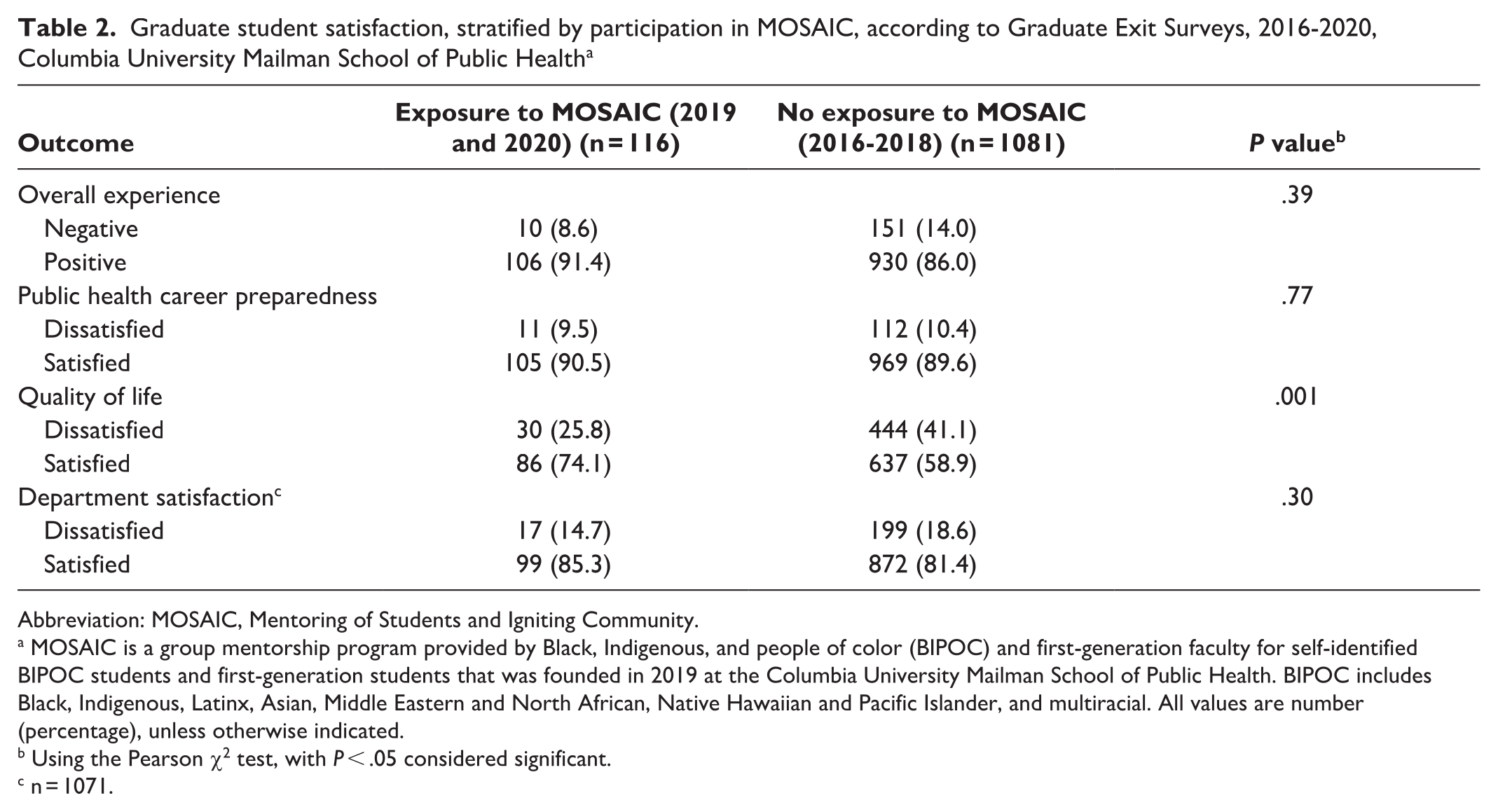
Abbreviation: MOSAIC, Mentoring of Students and Igniting Community.
MOSAIC is a group mentorship program provided by Black, Indigenous, and people of color (BIPOC) and first-generation faculty for self-identified BIPOC students and first-generation students that was founded in 2019 at the Columbia University Mailman School of Public Health. BIPOC includes Black, Indigenous, Latinx, Asian, Middle Eastern and North African, Native Hawaiian and Pacific Islander, and multiracial. All values are number (percentage), unless otherwise indicated.
Using the Pearson χ2 test, with P < .05 considered significant.
n = 1071.
Across the entire student body, we estimated positive associations with overall experience (Table 3). Compared with students who were not exposed to MOSAIC, students exposed to MOSAIC had a 25% increase in overall experience (P = .003), a 28% increase in quality of life (P < .001), and a 10% increase in satisfaction with their departments (P < .001).
Difference-in-difference estimates of changes in graduate student satisfaction after implementation of MOSAIC in 2019, according to Graduate Exit Surveys, 2016-2020, Columbia University Mailman School of Public Health a
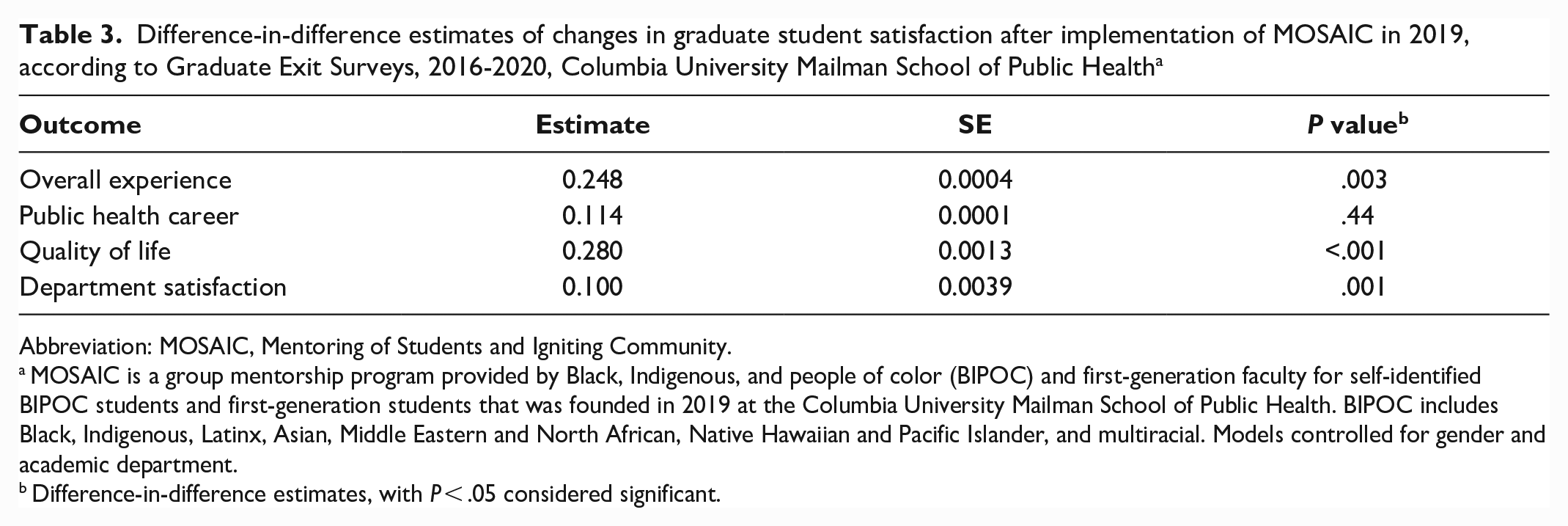
Abbreviation: MOSAIC, Mentoring of Students and Igniting Community.
MOSAIC is a group mentorship program provided by Black, Indigenous, and people of color (BIPOC) and first-generation faculty for self-identified BIPOC students and first-generation students that was founded in 2019 at the Columbia University Mailman School of Public Health. BIPOC includes Black, Indigenous, Latinx, Asian, Middle Eastern and North African, Native Hawaiian and Pacific Islander, and multiracial. Models controlled for gender and academic department.
Difference-in-difference estimates, with P < .05 considered significant.
2021 MOSAIC Student Survey
Of 39 students who evaluated the MOSAIC program, 87.2% (n = 34) reported that all their needs were met; 89.7% (n = 35) felt they had access to community, professional development, and informal discussion; 76.9% (n = 30) reported increased access to faculty; and 71.8% (n = 28) reported greater ability to develop skills (Table 4). In skill development, we found significant differences by first-generation identity (P = .04); 60.0% of BIPOC students versus 86.7% of BIPOC and first-generation students said their skill development needs were met. In informal discussions, we found some significant differences by race and ethnicity (P = .03); 80.0% of Latinx students, 50.0% of students who identified as ≥2 races, and 100% of students of all other races reported improvements in opportunities for informal discussions. We found no other significant differences by race and ethnicity and first-generation identity across outcomes.
Graduate student satisfaction with MOSAIC meeting academic and professional needs, by race and ethnicity and identity, according to the 2021 MOSAIC Student Survey (n = 39), Columbia University Mailman School of Public Health a
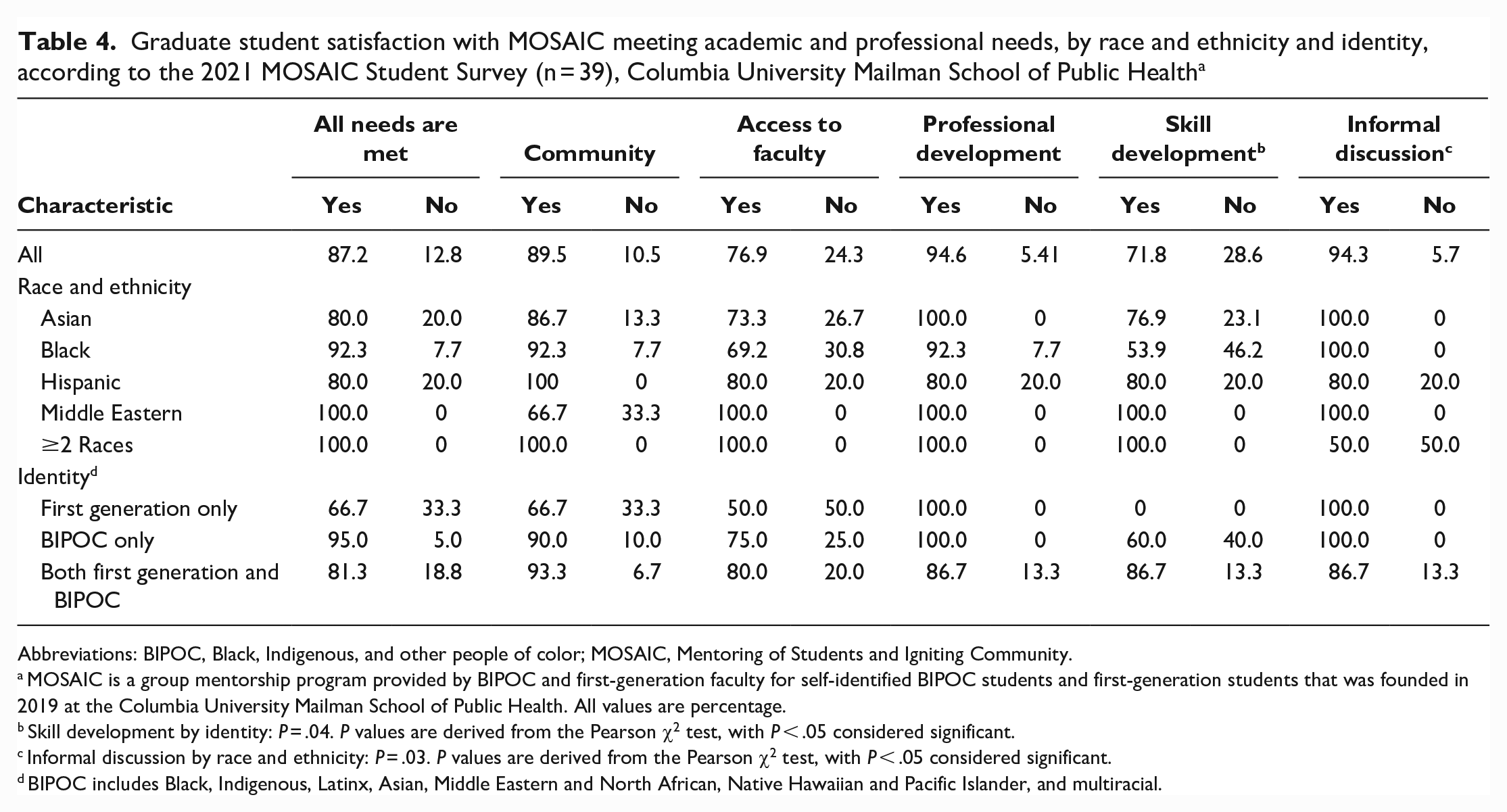
Abbreviations: BIPOC, Black, Indigenous, and other people of color; MOSAIC, Mentoring of Students and Igniting Community.
MOSAIC is a group mentorship program provided by BIPOC and first-generation faculty for self-identified BIPOC students and first-generation students that was founded in 2019 at the Columbia University Mailman School of Public Health. All values are percentage.
Skill development by identity: P = .04. P values are derived from the Pearson χ2 test, with P < .05 considered significant.
Informal discussion by race and ethnicity: P = .03. P values are derived from the Pearson χ2 test, with P < .05 considered significant.
BIPOC includes Black, Indigenous, Latinx, Asian, Middle Eastern and North African, Native Hawaiian and Pacific Islander, and multiracial.
Open-ended responses provided insight into why and how the presence of MOSAIC was associated with an overall positive experience for BIPOC students and an increase in satisfaction within departments for students in the MOSAIC program (Table 5). Student responses fell into 4 main themes: increased sense of belonging and community, navigating the university and increased access to resources, MOSAIC during virtual learning, and identification of additional needs. Students emphasized the critical component of bringing faculty and students together, building community, and making space for student questions and concerns. One respondent noted, “It brought me and my faculty and peers all to a table at which conversation felt more free and colloquial, at which earnest questions could be asked and honest answers could be heard.”
Graduate student descriptions of MOSAIC, according to the 2021 MOSAIC Student Survey (n = 39), Columbia University Mailman School of Public Health a
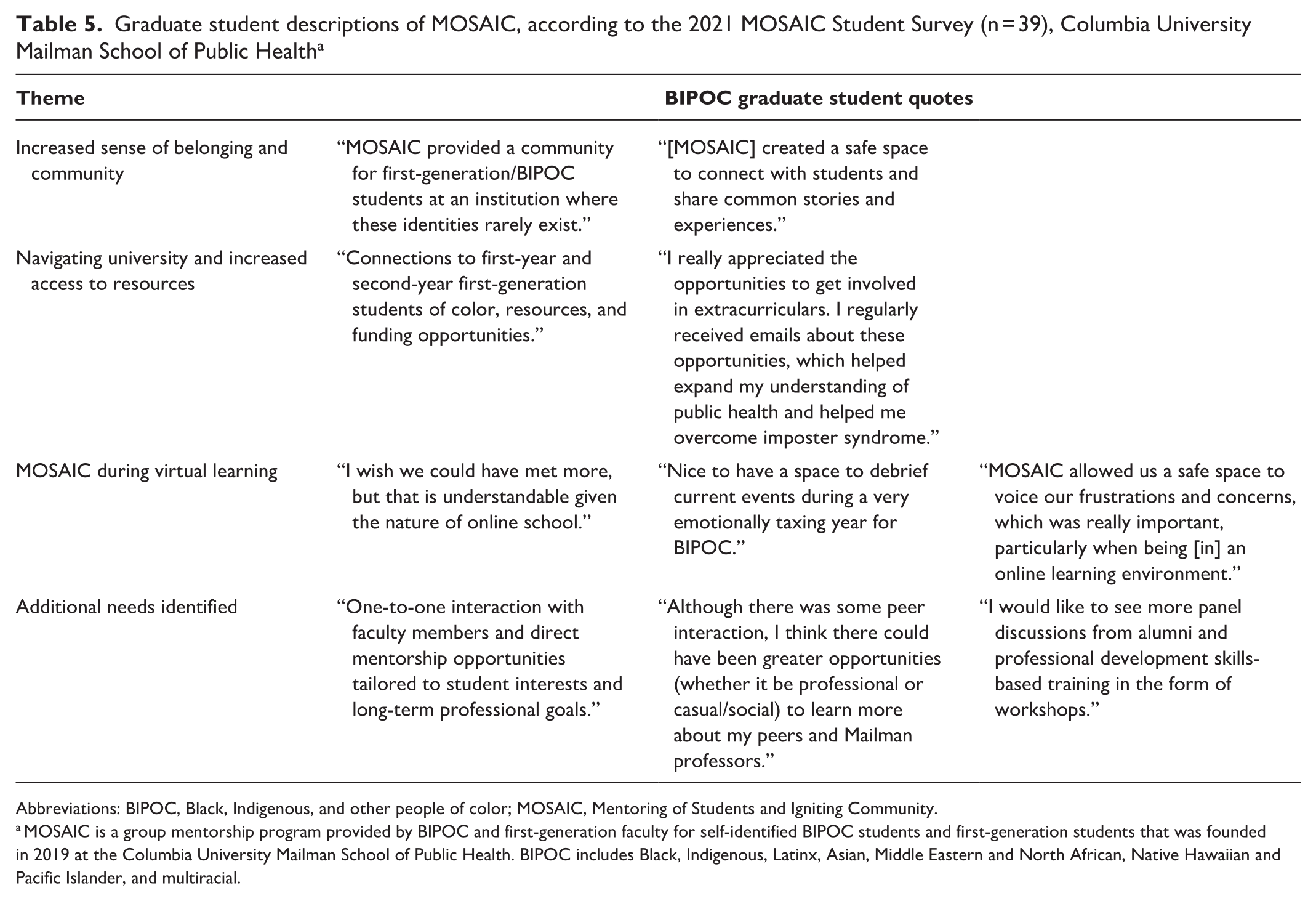
Abbreviations: BIPOC, Black, Indigenous, and other people of color; MOSAIC, Mentoring of Students and Igniting Community.
MOSAIC is a group mentorship program provided by BIPOC and first-generation faculty for self-identified BIPOC students and first-generation students that was founded in 2019 at the Columbia University Mailman School of Public Health. BIPOC includes Black, Indigenous, Latinx, Asian, Middle Eastern and North African, Native Hawaiian and Pacific Islander, and multiracial.
Discussion
Graduate schools and programs of public health have historically lacked antiracist programs that could better address institutional shortcomings and improve outcomes of BIPOC and first-generation students.1,10,13,18,19 This study shows that implementation of MOSAIC, a faculty-led graduate student mentorship program at a predominantly White research-focused university, was associated with significantly increased satisfaction, experiences in graduate school, and overall quality of life among graduate students who participated in the program versus graduate students who did not participate in MOSAIC. Results also indicated that most of the graduate students who joined the MOSAIC program did so because of opportunities to connect to BIPOC and first-generation students, faculty mentorship, community building, and professional development, and these opportunities had a positive effect on student well-being.
Participation in MOSAIC was associated with an overall positive experience for BIPOC graduate students and on average a 25% increase in their overall experience in public health graduate school. The effects of MOSAIC may be transformative for BIPOC students, and their experiences in graduate school may have ongoing effects as MOSAIC students advance in their public health careers. Negative experiences perpetually experienced by racially and ethnically minoritized student populations are linked to increased emotional distress and a diminished sense of belonging. 1 Supportive mentoring from faculty can be an effective tool to buffer these negative experiences and can lead to increased academic engagement, well-being, and successful completion of a graduate degree.1,22 In our study, we expanded on this work, showing that mentorship of BIPOC graduate students and first-generation students is associated not only with increased experiences and satisfaction but also with an increase in overall quality of life. MOSAIC also created a meaningful opportunity for community, thus improving the quality of life for BIPOC students in graduate school.
MOSAIC sessions provided tools for BIPOC and first-generation students to combat microaggressions and build community with peers to strengthen their sense of belonging, navigate institutions, and access faculty of similar racial and ethnic backgrounds. 12 As shown in our study, the experiences of BIPOC students during graduate school improved, seemingly despite the strain of the pandemic, because they felt as though they had a space and place to make connections, to ask questions, and to connect with faculty. Through MOSAIC, students expressed that they were able to access existing resources more comfortably, both because they were made aware of them and because their sense of imposter syndrome (the feeling that an individual’s success is not deserved or has not been earned) was reduced after finding a community of students and faculty.
Public health institutions are responsible for training future generations of the public health workforce and, as a part of that mission, must tailor programming to the guidelines of evidence-based antiracist education to better meet the academic needs of future public health leaders.27,28 As the health gap continues to widen, the application of an antiracist framework is required for institutions and the public health workforce to eliminate these health disparities.8,29 As such, schools and programs of public health must reexamine how they address racism and health inequities in teaching, research, policy, and practice.28,30 Our study shows that creation of MOSAIC in response to the need of BIPOC and first-generation students to have a structured community and mentorship to help navigate and succeed in an environment that has historically excluded them is associated with overall experiences in graduate school, quality of life, and satisfaction with one’s department.
Limitations
Our study had several limitations. First, we were limited in the ability to assess the outcomes and experiences of White students; the outcomes or experiences of non-White students may be qualitatively different than the outcomes or experiences of White students. Graduate school can be a challenging environment for all students. The Mailman School of Public Health has numerous formal and informal mentoring programs for all students, including a student affairs model that uses a case-management support style and a peer-to-peer mentorship program that requires students to apply before enrollment. MOSAIC was designed to meet the unique needs of BIPOC and first-generation students and acts as a complement to the many other sources of support and mentorship available to students. Second, the pandemic undoubtedly altered the experiences of BIPOC and first-generation graduate students, intensifying their strained sense of belonging and levels of anxiety and depression. 9 MOSAIC adapted the curriculum to the virtual environment, hosting frequent informal check-ins with students to provide a safe place for them to process their altered experiences and providing various virtual professional development opportunities throughout the year, but this experience was undoubtedly different than in-person programming. 12
Conclusions
As schools and programs of public health are charged with training the next generation of public health practitioners who deconstruct existing inequities, 11 mentorship offers a promising way for career development and, ultimately, promotion of health equity. Having holistic and comprehensive inclusive programs at all graduate schools and programs of public health will help improve educational and professional outcomes for first-generation and racially and ethnically marginalized student populations. These efforts can enhance graduate students’ well-being, sense of belonging, and overall growth.1,17 As shown in our study, investing in mentorship programs has benefits from the overall experience to satisfaction with quality of life for first-generation and BIPOC graduate students at schools and programs of public health. Moreover, MOSAIC lays the foundation for other institutions to implement similar programs to support the academic and professional goals of racially and ethnically minoritized public health student populations, which is anticipated to strengthen the public health workforce and rectify health disparities.
Supplemental Material
sj-pdf-1-phr-10.1177_00333549231181346 – Supplemental material for Effects of a Mentoring Program for Black, Indigenous, and People of Color and First-Generation Public Health Students
Supplemental material, sj-pdf-1-phr-10.1177_00333549231181346 for Effects of a Mentoring Program for Black, Indigenous, and People of Color and First-Generation Public Health Students by Stephanie Grilo, Monét Bryant, Samantha Garbers, Maggie Wiggin and Goleen Samari in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by the Columbia Mailman School of Public Health Dean’s Office and the Columbia University Office of the Provost. The content is solely the responsibility of the authors and does not necessarily represent the official views of Columbia University.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.