
Abstract
Objective:
To understand SARS-CoV-2 transmission in early care and education (ECE) settings, we implemented a Test to Stay (TTS) strategy, which allowed children and staff who were close contacts to COVID-19 to remain in person if they agreed to test twice after exposure. We describe SARS-CoV-2 transmission, testing preferences, and the number of in-person days saved among participating ECE facilities.
Methods:
From March 21 through May 27, 2022, 32 ECE facilities in Illinois implemented TTS. Unvaccinated children and staff who were not up to date with COVID-19 vaccination could participate if exposed to COVID-19. Participants received 2 tests within 7 days after exposure and were given the option to test at home or at the ECE facility.
Results:
During the study period, 331 TTS participants were exposed to index cases (defined as people attending the ECE facility with a positive SARS-CoV-2 test result during the infectious period); 14 participants tested positive, resulting in a secondary attack rate of 4.2%. No tertiary cases (defined as a person with a positive SARS-CoV-2 test result within 10 days after exposure to a secondary case) occurred in the ECE facilities. Most participants (366 of 383; 95.6%) chose to test at home. Remaining in-person after an exposure to COVID-19 saved approximately 1915 in-person days among children and staff and approximately 1870 parent workdays.
Conclusion:
SARS-CoV-2 transmission rates were low in ECE facilities during the study period. Serial testing after COVID-19 exposure among children and staff at ECE facilities is a valuable strategy to allow children to remain in person and parents to avoid missing workdays.
Early care and education (ECE) programs (eg, Head Start, center-based childcare, other preschool learning centers) play a vital role in the lives of young children and their families by providing early learning and development opportunities and by allowing parents to work.1,2 The COVID-19 pandemic has caused increased absences and staffing shortages in ECE facilities throughout the United States due to isolation and home quarantine requirements, which have led to negative effects, including loss of wages for parents who are unable to attend work and diminished educational and social opportunities for children.
ECE facilities face complex challenges when preventing and controlling the spread of SARS-CoV-2, the virus that causes COVID-19, among staff and young children. Most attendees are aged <5 years, making them ineligible for COVID-19 vaccinations during the first 2 years of the pandemic, when most people were required to quarantine at home for at least 5 days after an exposure to COVID-19. 3 Centers for Disease Control and Prevention (CDC) guidance for COVID-19 prevention in ECE settings emphasized using multiple prevention measures, including staff vaccination and nonpharmaceutical interventions, such as wearing face masks and social distancing, which can be difficult for young children to adhere to consistently.4,5
Test to Stay (TTS) is a modified quarantine strategy adopted by kindergarten through grade 12 (K-12) schools during the COVID-19 pandemic that allowed asymptomatic staff and students who were not up to date with COVID-19 vaccination at the time of exposure to continue to attend in person if they adhered to serial testing. TTS implementation among K-12 schools allowed SARS-CoV-2 transmission to remain low and benefited students by preserving in-person learning days.6-9
To our knowledge, no studies have evaluated TTS and the implementation of serial testing after an exposure to COVID-19 in ECE settings; therefore, we conducted an evaluation of the implementation of TTS in 32 ECE facilities in Illinois. We described secondary and tertiary transmission rates of SARS-CoV-2, identified testing preferences among TTS participants, and estimated the number of in-person attendance days and parent workdays saved due to children and staff remaining in person after exposure to COVID-19.
Methods
Facility Enrollment
The Illinois Department of Public Health (IDPH) identified 2 local health departments (LHDs), the Chicago Department of Public Health and the Lake County Health Department, to implement TTS in ECE facilities from March 21 through May 27, 2022. The 2 LHDs identified 32 ECE facilities (23 and 9, respectively), which included private ECE centers, faith-based ECE programs, and Head Start programs located across geographic locations representing 19 zip codes. The 2 LHDs identified participating ECE facilities based on the ability of facilities to implement TTS and to report contact tracing and case investigation data to the LHD during the study period. Each ECE facility completed an enrollment form, which recorded age, sex, race, ethnicity, and vaccination status of staff and children, plus the COVID-19 prevention strategies implemented at the facility.
This activity was reviewed by CDC and did not require institutional review board approval. Data collection was consistent with applicable federal law and CDC policy (eg, 45 CFR part 46; 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
TTS Protocol
We defined an ECE index case as a person attending the ECE facility with a positive SARS-CoV-2 test result (by polymerase chain reaction [PCR] or rapid antigen test) during the infectious period (from 48 hours before to 10 days after symptom onset or, if asymptomatic, 10 days after a positive test result) if not first identified as a close contact at the ECE facility during their incubation period (10 days before symptom onset or, if asymptomatic, 10 days before a positive test result). We defined a community index case as a person outside the ECE facility (eg, household member, teammate) with a positive SARS-CoV-2 test result who exposed a staff member or child participating in TTS during their infectious period. We defined a secondary case as a person with a positive SARS-CoV-2 test result within 10 days after exposure to any index case. We defined a tertiary case as a person with a positive SARS-CoV-2 test result within 10 days after exposure to a secondary case. We included close contacts in the dataset more than once if they were exposed to COVID-19 and participated in TTS more than once during the study period.
We considered a person to be a close contact if they came within 6 feet of a person with COVID-19 for a cumulative total of 15 minutes or more during a 24-hour period, regardless of face mask use. 3 Close contacts aged <18 years were not required to quarantine if they had completed a primary COVID-19 vaccine series. ECE staff close contacts were not required to quarantine if they were up to date with COVID-19 vaccination, defined as having received a primary series and all boosters recommended when eligible. Close contacts with a positive COVID-19 test in the past 90 days who remained asymptomatic were not required to quarantine.
Close contacts were eligible to participate in TTS if they were unvaccinated, partially vaccinated, or not up to date with COVID-19 vaccination; aged ≥2 years at the time of exposure; remained asymptomatic while enrolled in TTS; and gave personal consent (staff) or parental consent (children). Children aged <2 years were ineligible for TTS because at-home antigen tests had not been authorized for this age group and they were unable to wear face masks. Eligible close contacts could participate in TTS if their exposure occurred either while attending the ECE or outside the ECE setting. Staff TTS participants were required to wear face masks, whereas child participants were encouraged to wear face masks to the best of their ability. TTS participants were tested twice within 7 days of last exposure to COVID-19, with the second test occurring between days 5 and 7 after exposure.
Children identified as close contacts who did not meet TTS eligibility criteria or opted out of TTS were required to quarantine at home for at least 5 days, depending on their respective ECE facility’s protocol. If the child returned to the ECE facility before day 10, wearing a face mask was required to the best of the child’s ability. Staff who were identified as close contacts but did not meet TTS eligibility criteria or opted out of TTS were required to quarantine at home for at least 5 days and then wear face masks consistently after return to the ECE through day 10 after exposure.
For this analysis, we excluded data from facilities when substantive deviations occurred from the original TTS protocol developed by IDPH, such as increasing the testing cadence to once daily, requiring staff who were up to date with COVID-19 vaccination to be tested after an exposure, or not conducting contact tracing.
COVID-19 Testing
ECE facilities implemented COVID-19 testing for TTS participants on Mondays and Thursdays of each week. Participants had 3 testing options to choose from: (1) the SHIELD Illinois saliva-based PCR test collected at home by parents and brought to the ECE facility for pickup and testing, (2) the SHIELD Illinois saliva-based PCR test collected at the ECE facility by SHIELD Illinois staff, or (3) a rapid antigen test collected at home by parents, which was provided by the ECE facility or purchased privately. Turnaround time for PCR test results ranged from 24 to 48 hours. Turnaround time for antigen test results collected at home varied; parents or staff provided either verbal confirmation of the test result or a picture of the test result to the ECE facility.
Case Investigation and Contact Tracing
ECE facilities collected data from March 21 through May 27, 2022. ECE staff conducted contact tracing and case investigation with assistance from their respective LHDs and entered data on demographic characteristics, exposure dates, type of quarantine, and test results into an electronic spreadsheet. ECE staff then submitted the electronic spreadsheets to the LHD, which conducted data verification and cleaning before entering data into REDCap, a secure web-based data collection database hosted by IDPH. Contact tracers then reviewed data in REDCap to ensure completeness and conducted 10-day follow-up telephone calls with cases and close contacts.
Contact tracers attempted to reach cases and close contacts by telephone at least twice; if a case or close contact was aged <18 years, the parents were interviewed. Contact tracers called index and secondary cases at least 10 days after their positive COVID-19 test date to inquire about symptom onset and whether additional SARS-CoV-2 transmission occurred outside the ECE setting (eg, among household members). Contact tracers called TTS-eligible contacts at least 10 days after their last date of exposure to COVID-19 to verify test results, ask about symptoms, and confirm whether they participated in TTS or quarantined at home.
In-Person Days Saved
Parent workdays saved may include days parents would have missed work to provide care for their child or would have needed to arrange for non-ECE childcare to continue to work outside the home. We calculated the number of in-person days saved by assuming an average of 5 days of quarantine averted for each TTS participant. We assumed that delays in the reporting of positive test results may have created a lag in notification of exposures, resulting in shorter quarantine periods or that, in some instances, parent preference or ECE facility protocol resulted in a longer home quarantine of 7, 10, or 14 days.
Statistical Analysis
We calculated counts and proportions of demographic characteristics of TTS participants, the type of COVID-19 test, and the reported testing location. We computed Clopper–Pearson exact 95% CIs for secondary and tertiary attack rates. We used SAS version 9.4 (SAS Institute, Inc) for all analyses.
Results
During the study period (March 21–May 27, 2022), of 414 close contacts who were eligible for TTS among index and secondary cases, 383 (92.5%) ECE children and staff elected to participate in TTS. ECE facilities reported 35 ECE index cases and 9 community index cases at 14 of 32 ECEs participating in the study. Of the 35 ECE index cases, 29 were symptomatic (15 of 17 staff, 14 of 18 children). The index cases generated 360 unique TTS-eligible close contacts, of whom 331 (91.9%) participated in TTS (ie, elected to remain in person at ECE facilities and test twice for COVID-19 after exposure) and 29 (8.1%) participated in home quarantine (Figure). The index cases also generated 90 close contacts who were exempt from quarantine due to up-to-date vaccination status (65 staff and 25 children aged ≥5 years) and 59 TTS-ineligible close contacts (32 children aged <2 years and 27 children with an unspecified reason who quarantined at home).
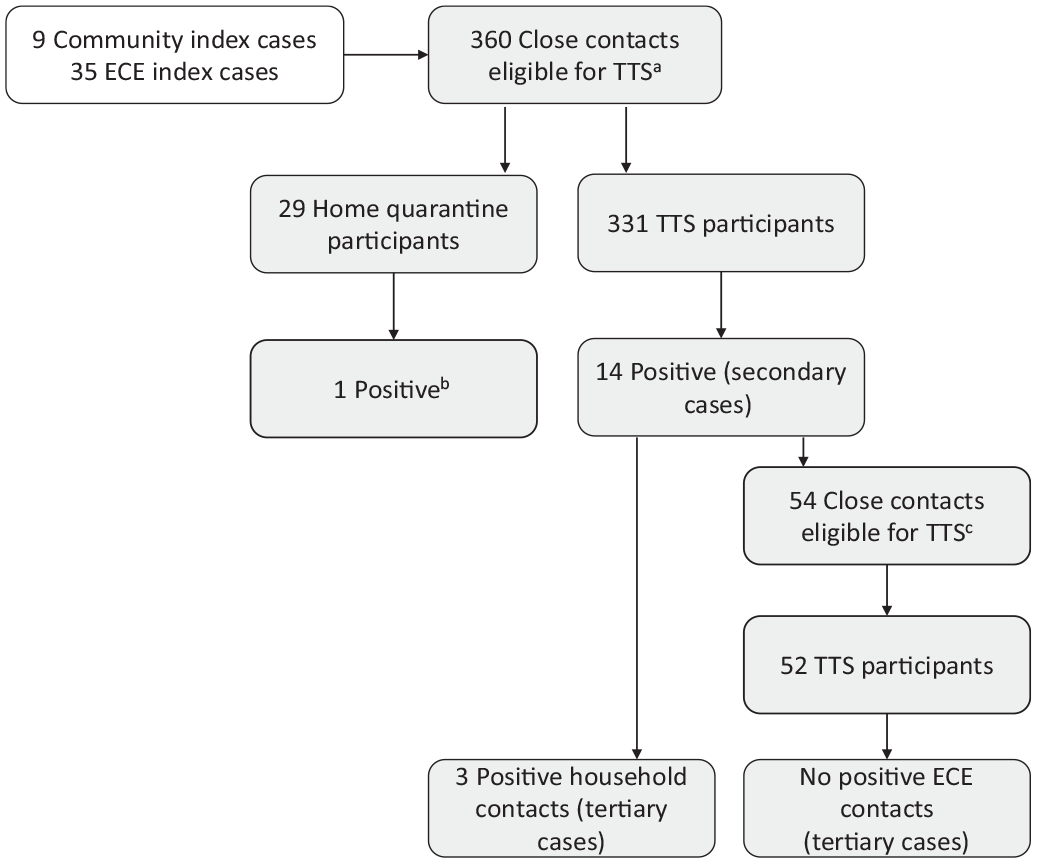
Identification of index cases (children or staff with positive COVID-19 test results who attended an early care and education [ECE] facility or people in the community with positive COVID-19 test results who exposed an ECE staff or child participating during their infectious period) and close contacts (ECE children and staff who had a COVID-19 exposure) eligible for Test to Stay (TTS) among 32 ECE facilities in Illinois, March 21 through May 27, 2022.
Of the 331 ECE children and staff who participated in TTS, 14 were identified as secondary cases, of whom 7 were symptomatic. The 14 secondary cases in turn generated 54 TTS-eligible close contacts, of whom 52 (96.3%) participated in TTS and 2 (3.7%) quarantined at home; 8 additional close contacts (5 staff members and 3 children aged ≥5 years) were exempt from quarantine due to up-to-date vaccination status. The 52 close contacts who participated in TTS did not generate any tertiary cases in the ECE facility; however, 3 tertiary cases were identified among household members of the 14 secondary cases. Two household tertiary cases were up to date with COVID-19 vaccination, and 1 was unvaccinated.
Demographic Characteristics
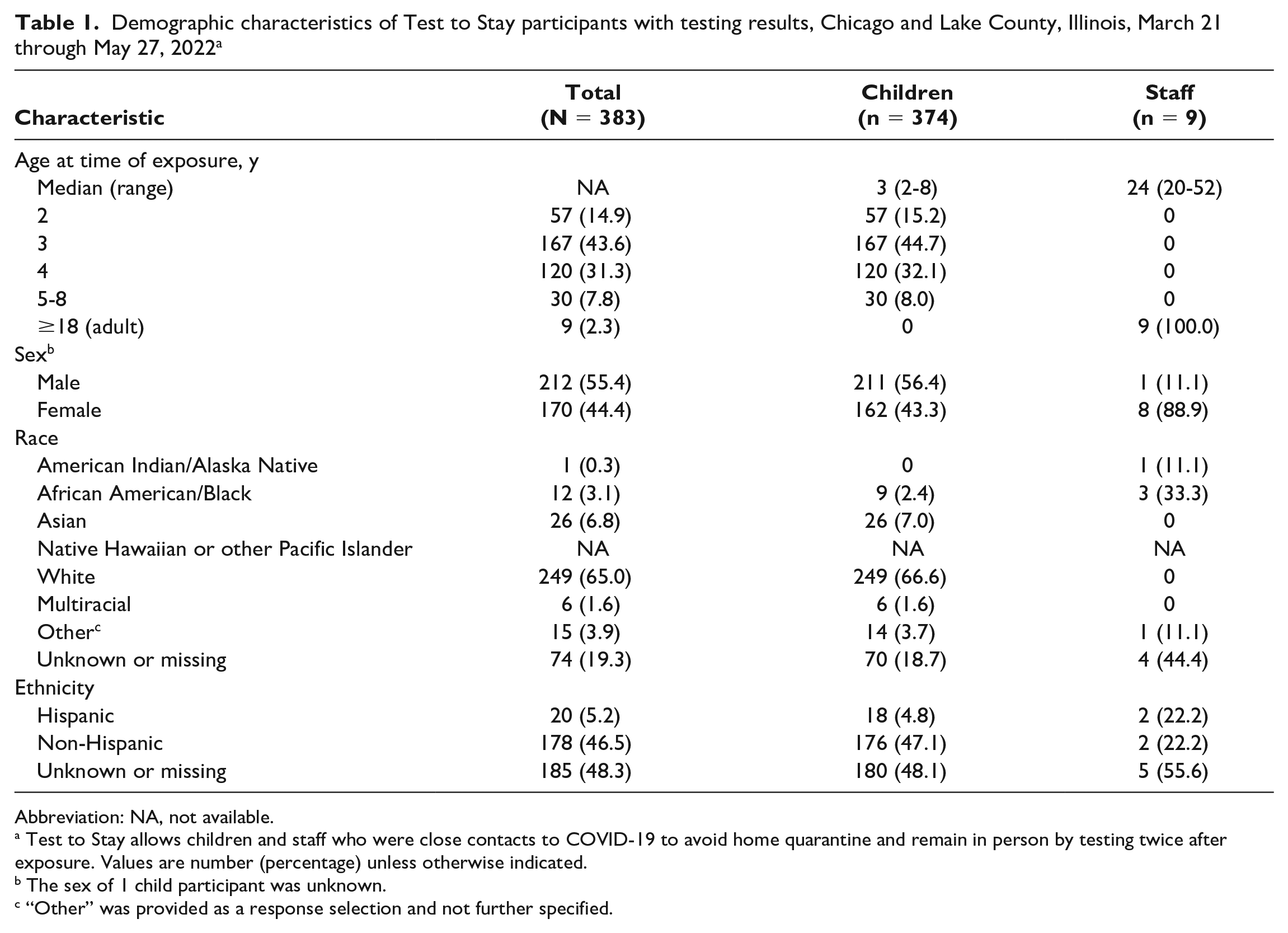
Of the 383 TTS-eligible close contacts who elected to participate in TTS and had SARS-CoV-2 test results, 374 were children and 9 were staff (Table 1). The 374 children had a median age of 3 years (range, 2-8 years), and 211 (56.4%) were boys. The 9 staff had a median age of 24 years (range, 20-50 years), and 8 (88.9%) were women. Among 383 participants, most (n = 249, 65.0%) were White; race was unknown or missing for 74 (19.3%) participants. Reported ethnicity among participants showed most as non-Hispanic (n = 178, 46.5%) or unknown or missing ethnicity (n = 185, 48.3%).
Demographic characteristics of Test to Stay participants with testing results, Chicago and Lake County, Illinois, March 21 through May 27, 2022 a
Abbreviation: NA, not available.
Test to Stay allows children and staff who were close contacts to COVID-19 to avoid home quarantine and remain in person by testing twice after exposure. Values are number (percentage) unless otherwise indicated.
The sex of 1 child participant was unknown.
“Other” was provided as a response selection and not further specified.
COVID-19 Test Characteristics
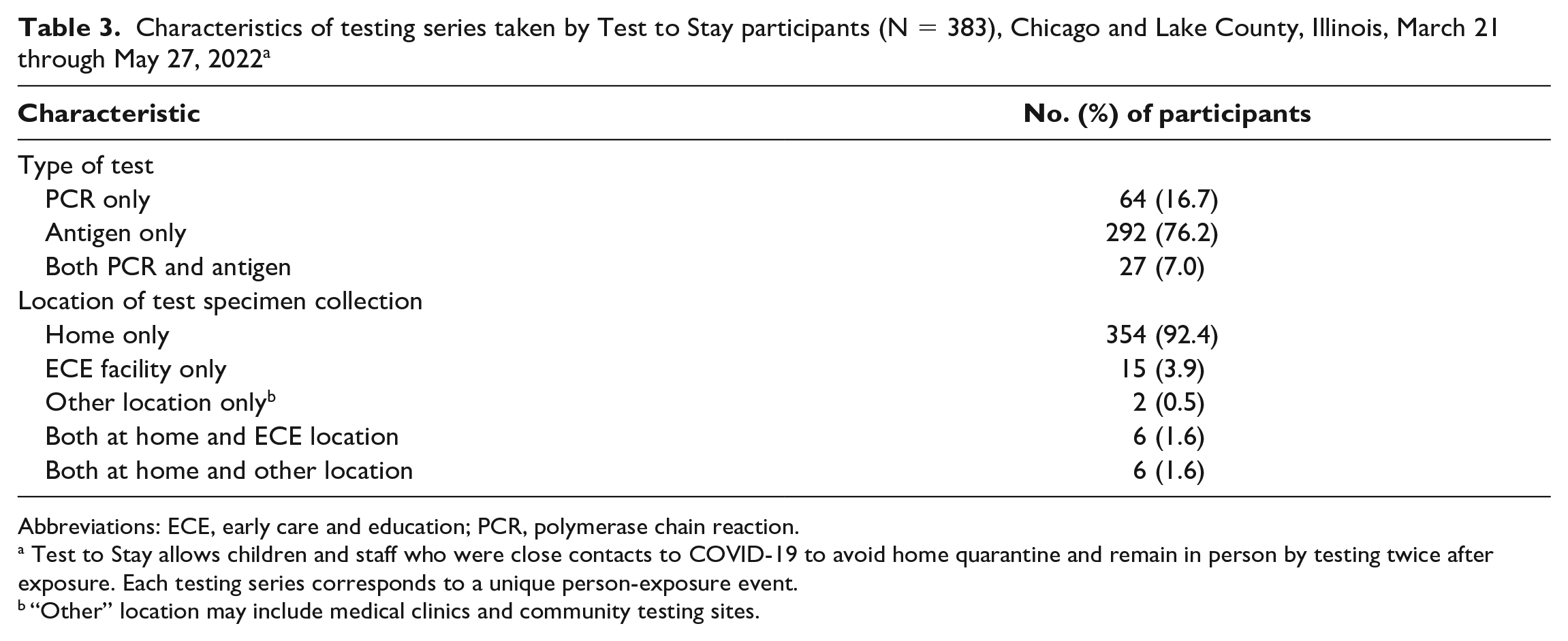
Of the 793 COVID-19 test types reported among 383 TTS participants, 631 (79.6%) were rapid antigen tests and 162 (20.4%) were PCR tests. Most test samples were collected by parents at participants’ homes (n = 748, 94.3%) (Table 2). Of 383 TTS participants, 292 (76.2%) used only rapid antigen tests, 64 (16.7%) used only PCR tests, and 27 (7.0%) used both. Most participants conducted at least 1 home test (366 of 383, 95.6%), with most conducting only home tests (354 of 383, 92.4%) (Table 3).
Characteristics of the 793 unique COVID-19 tests taken by 383 Test to Stay participants, Chicago and Lake County, Illinois, March 21 through May 27, 2022 a
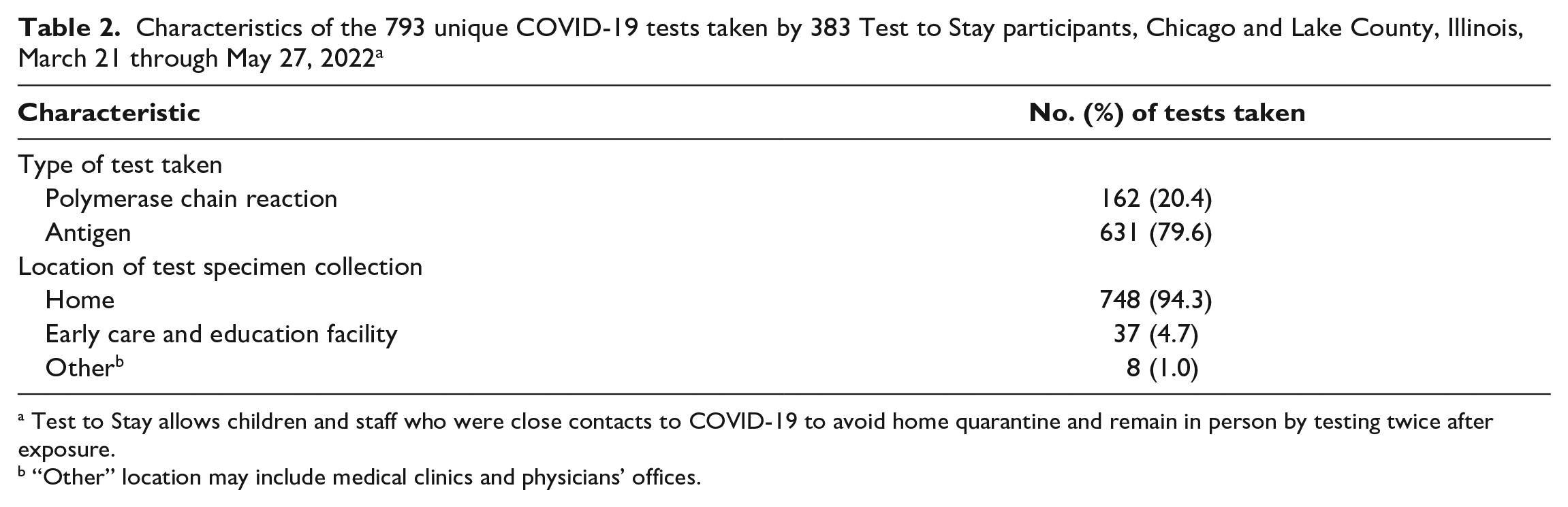
Test to Stay allows children and staff who were close contacts to COVID-19 to avoid home quarantine and remain in person by testing twice after exposure.
“Other” location may include medical clinics and physicians’ offices.
Characteristics of testing series taken by Test to Stay participants (N = 383), Chicago and Lake County, Illinois, March 21 through May 27, 2022 a
Abbreviations: ECE, early care and education; PCR, polymerase chain reaction.
Test to Stay allows children and staff who were close contacts to COVID-19 to avoid home quarantine and remain in person by testing twice after exposure. Each testing series corresponds to a unique person-exposure event.
“Other” location may include medical clinics and community testing sites.
COVID-19 Test Results
Of the 331 TTS participants exposed to an index case, 14 tested positive for COVID-19, resulting in a secondary attack rate of 4.2% (95% CI, 2.3%-7.0%), and of the 317 participants with a negative COVID-19 test result, 291 (91.8%) had ≥2 negative tests. Of the 52 TTS participants exposed to a secondary case, none tested positive (0% tertiary attack rate; 95% CI, 0%-6.8%), and of these 52 participants, 45 (86.5%) had ≥2 negative test results.
Thirteen of the 29 TTS-eligible close contacts who elected to quarantine at home reported COVID-19 test results; 1 had a positive test result. Of the 70 staff who were up to date with COVID-19 vaccination and, thus, not required to quarantine, 30 reported COVID-19 test results; 1 had a positive test result. Twenty of 28 children aged ≥5 years who were fully vaccinated (and, thus, not required to quarantine) reported COVID-19 test results; none had a positive test result.
Case Investigation and Contact Tracing
Contact tracers completed 10-day follow-up telephone calls for 11 of 35 (31.4%) index cases, 5 of 14 (35.7%) secondary cases, and 151 of 400 (37.8%) TTS participants with negative test results or who were eligible for TTS but participated in home quarantine.
In-Person Days Saved
Assuming an average quarantine of 5 days averted among 383 staff and children who participated in TTS, we estimated that 1915 in-person ECE days were saved. Of the 9 TTS staff participants, we estimated that 45 staff workdays were saved; among the families of the 374 children who participated in TTS, we estimated that 1870 parent workdays were saved.
Discussion
This study evaluated transmission of SARS-CoV-2 in 32 ECE facilities in Illinois that implemented serial testing of close contacts to COVID-19 from March 21 through May 27, 2022. Although the participating ECE facilities had varied testing and reporting strategies, our results indicate that the secondary transmission rate was low among participants who tested after an exposure to COVID-19, and no tertiary transmission occurred in the ECE facilities. These findings are consistent with low SARS-CoV-2 transmission rates reported among K-12 schools implementing TTS.6,7,9 In addition to implementing TTS, the ECE facilities that participated in our study followed IDPH recommendations to limit SARS-CoV-2 transmission, including optimizing ventilation and requiring symptomatic children to stay home, which likely also kept transmission low. During the study period, both Chicago and Lake County experienced a substantial increase in community COVID-19 incidence (7-day rolling average number of cases per 100 000 people); incidence rates increased 368% (from 62.9 to 294.3) in Chicago and 462% (from 60.6 to 340.3) in Lake County. 10 The reported increase in community incidence was not reflected among participating ECE facilities, thus supporting previous findings that SARS-CoV-2 transmission in ECE settings remains low during periods of high community incidence. 11
Our findings showed that most eligible close contacts chose to remain in-person after an exposure to COVID-19. As a result, a substantial number of ECE in-person attendance days and workdays were saved among participants and their parents. Staff participants and parents of TTS participants in our study chose the type of test and the location of specimen collection, with most choosing to test at home. When COVID-19 exposures occur in ECE settings, offering home testing to monitor transmission may be beneficial for ECE staff, because it will decrease the time it takes to collect specimens and track results. ECE facilities included in our study designated Mondays and Thursdays for testing, which eliminated the time it would have taken for staff and parents to track the unique testing schedule of each participant based on the date of their last exposure, while also ensuring that participants received 2 tests during the 7-day period after exposure, with the second test occurring 5-7 days after exposure.
Our study was conducted when quarantine was recommended for people not up to date with COVID-19 vaccinations after an exposure and when children aged <5 years were ineligible for COVID-19 vaccination and were required to quarantine at home after an exposure. Despite COVID-19 vaccine being approved for children aged 6 months to 4 years in June 2022, vaccine uptake has remained low among children; in July 2022, fewer than one-third (29.8%) of children aged 5-11 years were fully vaccinated. 10 In August 2022, CDC updated guidelines to no longer recommend quarantine after an exposure to COVID-19, instead recommending the use of well-fitted face masks through day 10 after exposure and a COVID-19 test on day 6 or later if symptoms have not developed, regardless of vaccination status. 12 While a TTS model such as the one we describe here may not be required to allow children to remain in person after an exposure to COVID-19, testing will remain crucial in reducing transmission of SARS-CoV-2 and is especially important in settings such as ECE facilities, where close contacts may not be able to use face masks consistently.
Limitations
Our study had some limitations. First, the 10-day follow-up call response rate was only 35.8%, which may have resulted in missing information, such as household tertiary cases. Second, we did not identify tertiary transmission in the ECE facilities during the study period; however, COVID-19 incubation and infectious periods vary and overlap, making it difficult to explicitly identify tertiary SARS-CoV-2 transmission when several exposures occur among a group of classmates. Third, when recruiting ECE facilities for the study, some facilities declined participation because testing support or available funding was not guaranteed after the study ended. This factor may have resulted in a selection bias toward ECE facilities with more resources compared with facilities that chose not to participate. Finally, our findings demonstrate the implementation of TTS in a real-world setting. True transmission rates of SARS-CoV-2 among ECE facilities may differ depending on local guidance, ability to conduct contact tracing, quality of home specimen collection, validation of self-reporting results, and sensitivity of home tests.
Conclusions
To our knowledge, our study is the first to examine the use of serial testing of students and staff after an exposure to COVID-19 in the ECE setting. The SARS-CoV-2 transmission rate was low among ECE facilities during the study period. Both children and parents benefit from children attending ECE programs, and low transmission rates allow children to remain in person for childcare and education and enable parents to work outside the home without having to arrange alternative childcare. In addition to implementing proven infection prevention strategies to support safe in-person learning, ECE facilities might consider implementing testing programs that offer home testing for close contacts of COVID-19–positive people to monitor transmission of SARS-CoV-2 and allow staff and young children to remain safely in person.
Footnotes
Acknowledgements
The authors thank the following people for their contributions to the implementation and data collection for this study: Tiffany Campos, MSN; Albertina Donaldson, DNP; Zeruya Gaddam, MSN; Aliyha Hill, MPH; and Sithembinkosi Ndebele, MPHc (Chicago Department of Public Health); Funmilayo Akindileni, MD; Pat Brady; Sean Kennedy, DO; Amyanne Keswani Cope, MS; Leia Mueller; and Dina Taryal, MD (Lake County Health Department and Community Health Center); Rhiannon Clifton, MBA; Maria Messmacher, BA; Tiffany Rossi, BA; SHIELD Illinois Field Operations Team, SHIELD Illinois Relationship Managers (SHIELD Illinois); Susan Bleasdale, MD; Kim Kull; Alfredo Mena Lora, MD; Natalia Lopez-Yanez, MPH; Jocelyn Vaughn, MS; and Daniel Villalobos-Terrazas, MPH (University of Illinois, Chicago); and Krutarth Dave, MPH, and Cedrick Ntambwe, MD (Centers for Disease Control and Prevention [CDC]). This project was supported in part by an appointment to the Research Participation Program at CDC administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the US Department of Energy and CDC.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of CDC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.