
Abstract
Objective:
Clostridium perfringens and Bacillus cereus are common causes of reported foodborne illness. On August 6, 2021, the Alaska Division of Public Health identified a multipathogen gastrointestinal outbreak among hospital staff in Homer, Alaska. The objectives of this study were to identify the outbreak source and prevent future illness.
Methods:
We conducted a retrospective cohort study of hospital staff who participated in luncheon events during August 5-7, 2021, and used an online survey to identify hospital staff with gastrointestinal illness. We defined case patients as people who reported new-onset gastrointestinal illness (diarrhea or abdominal cramping) after food consumption during the luncheon events. We calculated adjusted odds ratios of gastrointestinal illness associated with reported food exposures. We tested available food samples for C perfringens and B cereus and tested case patient stool specimens for C perfringens. We conducted an environmental investigation at the implicated vendor site.
Results:
Of 202 survey responses, 66 (32.7%) people reported acute gastrointestinal illness: 64 (97.0%) reported diarrhea, 62 (94.9%) reported abdominal cramps, and none were hospitalized. Of 79 people who consumed ham and pulled pork sandwiches, 64 (81.0%) met the case definition; this food item was significantly associated with increased odds of gastrointestinal illness (adjusted odds ratio = 296.4; 95% CI, 76.7-2019.1). C perfringens and B cereus were isolated at confirmatory levels from sandwich samples. C perfringens enterotoxin was detected in all 5 stool specimens tested. Environmental investigators observed other food items at the sandwich vendor that were refrigerated outside the required temperature range (>41 °F); no clear handling deficiencies for the implicated food were identified.
Conclusion:
Quick notification and effective collaboration can help detect an outbreak, identify the responsible food vehicle, and mitigate further risk.
Clostridium perfringens is an anaerobic, gram-positive, spore-forming bacillus that germinates in foods under anaerobic conditions. If ingested, it can cause in vivo toxin production resulting in acute gastrointestinal illness. Bacillus cereus is a facultatively anaerobic, toxin-producing, gram-positive bacterium capable of forming heat-resistant spores in foods. If ingested, it can result in vomiting shortly after eating contaminated food or diarrhea after a longer incubation period. Both organisms are common etiologic agents of foodborne outbreaks in the United States. 1 However, outbreaks attributable to both organisms simultaneously are rare. Multiple-etiology foodborne disease outbreaks involving ≥2 organisms of any kind are seldom reported in the United States. Of 2986 foodborne disease outbreaks reported to the Centers for Disease Control and Prevention (CDC) from 2009 through 2015, only 33 (1.1%) were attributable to multiple etiologies. 2 We describe a foodborne outbreak of acute gastrointestinal illness caused by 2 bacterial pathogens among hospital workers in Alaska.
Methods
On August 6, 2021, the Alaska Division of Public Health, Section of Epidemiology was informed of an outbreak of gastrointestinal illness among staff at a hospital in Homer, Alaska. In the 2 days preceding reported illness onset, lunches were provided to hospital staff through takeout from local food vendors; the hospital cafeteria had been closed because of staffing concerns associated with the COVID-19 pandemic. By 10
This project was reviewed by CDC, and its conduct was consistent with applicable federal law and CDC policy (eg, 45 CFR part 46; 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq).
Case Finding
We conducted a retrospective cohort study of all hospital staff who reported consuming foods at luncheon events on August 4 or 5, 2021. We developed and emailed an online anonymous survey to all hospital staff (N = 515) by 5
Laboratory Investigation
We obtained stool specimens from hospital staff members who experienced gastrointestinal symptoms. We sent stool specimens to the Enteric Diseases Laboratory Branch at CDC; the CDC laboratory performed C perfringens testing using the Oxoid C perfringens enterotoxin reverse passive latex agglutination test. We did not have enough samples to test for B cereus in stool specimens. We sent leftover food items from the August 5, 2021, luncheon to the Washington State Public Health Laboratories. On the basis of the calculated incubation period and the symptoms observed among case patients, we directed the laboratory to test for C perfringens and B cereus. Given the estimated infective dose for C perfringens and B cereus (≥106 organisms 3 ), the laboratory used isolation of ≥106 organisms/g to confirm epidemiologic causation of that food 4 or C perfringens detection. After anaerobic colony growth, the laboratory identified isolates by Gram staining, motility tests, nitrate reduction, lecithinase tests, and color change in lactose gelatin media. For B cereus detection, the laboratory grew selected colonies on nutrient agar and identified isolates by Gram staining, motility tests, nitrate reduction, gelatin hydrolysis, glucose fermentation, the Voges–Proskauer test, and hemolysis on blood agar plates.
Environmental Investigation
The Alaska Department of Environmental Conservation’s Food Safety and Sanitation Program initiated an investigation that included an environmental assessment at the location of the food vendor that prepared the ham and pulled pork sandwiches. The assessment included a review of food production, processing, and holding, which was compared with Alaska food establishment requirements 5 to identify environmental antecedents. The team from the Alaska Department of Environmental Conservation Food Safety and Sanitation Program also assessed the distribution of the suspected food item.
Data Analysis
Because our survey did not collect exact times of food consumption, we used a proxy time of noon on August 5, 2021 (the reported time when lunch containing the suspected food item was served to staff) to calculate the median incubation period. We calculated food-specific attack rates for all food exposures (ie, the proportion of people exposed to food who reported acute gastrointestinal illness); food exposures included the available takeout lunch dishes offered to staff on the 2 days (August 4 and 5) preceding the reported illness onset. On August 4, 2021, food items consisted of 5 types of pizza (cheese, pepperoni, meat, vegetable, and sausage with pepperoni) and 2 types of house salad (1 with garlic vinaigrette and 1 with balsamic vinaigrette dressing). On August 5, food items consisted of ham and pulled pork sandwiches, garlic chicken wings, Asian sauce chicken wings, 4 types of wraps (Thai turkey, vegan, chicken Caesar, and club), a broccoli salad, assorted chips, and a homemade salad brought in by a staff member. To determine exposures significantly associated with illness, we used Pearson χ2 tests or Fisher exact tests to calculate P values and odds ratios (ORs). We included identified food exposures in bivariable analyses with P < .10 and an OR >1 in the multivariable logistic regression model to calculate ORs for illness, with P < .05 considered significant; we also included age and sex as potential confounding variables. For our multivariable analysis, we excluded food items not considered plausible sources of infection based on results of the bivariable analysis. We also excluded 1 food item (club wrap) from analysis because no case patient reported consuming it.
We performed statistical analyses using R version 4.1.1 (R Foundation for Statistical Computing).
Results
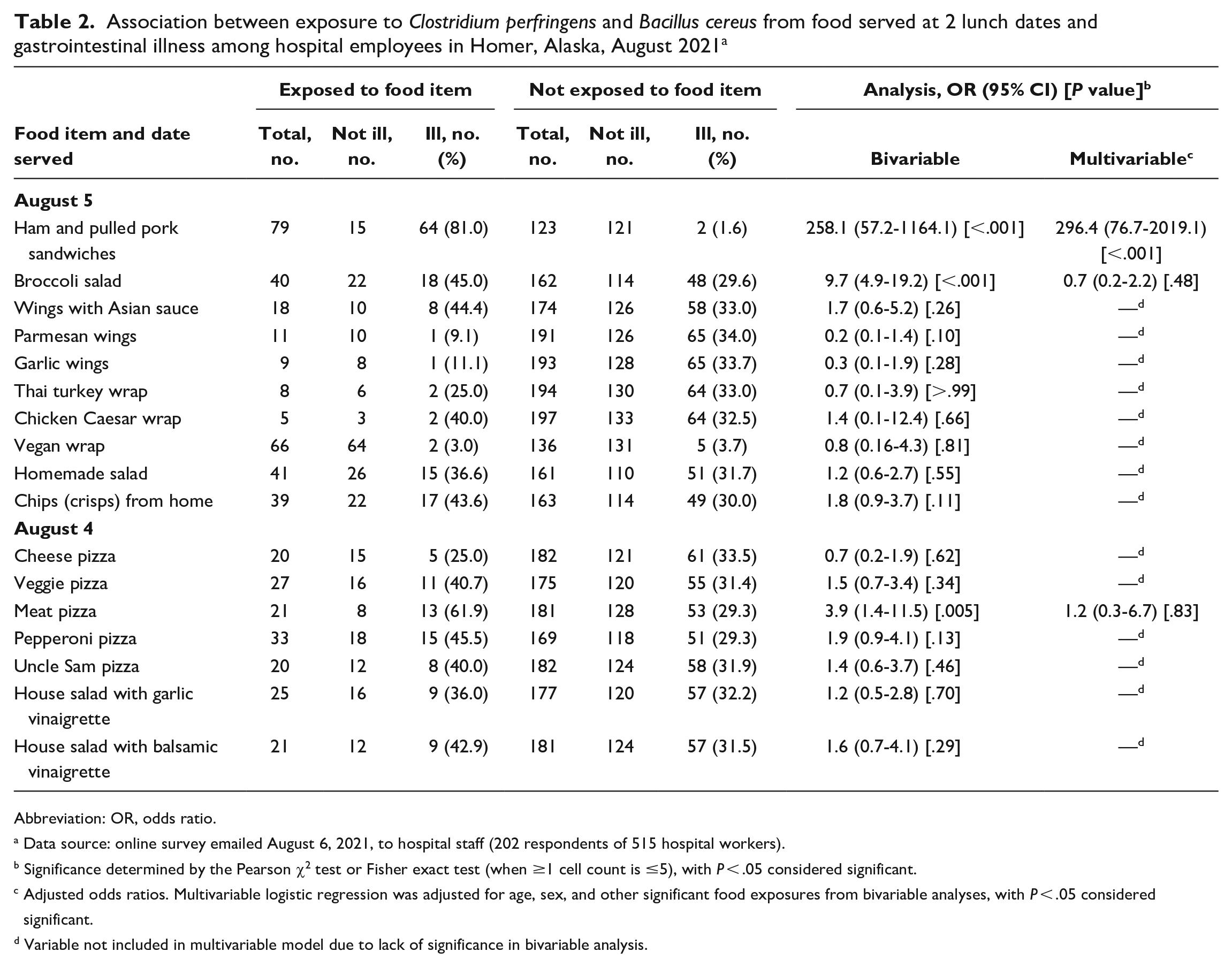
Of 515 surveys emailed to hospital staff members, 202 (39.2%) were returned by those who reported consuming foods at luncheon events. Of 202 respondents, 66 (32.7%) met the outbreak case definition for gastrointestinal illness and were considered case patients (Figure). The median incubation period was 8.5 hours (range, 3.5-45.0 hours). The median duration of illness was 23 hours (range, 2-48 hours), with 17 (25.9%) case patients still reporting symptoms at the time of survey completion. Among 66 case patients, 47 (71.2%) were aged 20-49 years, 19 (28.8%) were aged 50-74 years, and 53 (80.3%) self-identified as female. Of 66 case patients, 64 (95.5%) reported diarrhea; 62 (93.9%), abdominal pain or cramping; and 37 (56.1%), nausea (Table 1). No reports of hospitalization were received; however, 1 case patient sought care from a health care provider. Attack rates were highest among survey respondents who reported consuming the ham and pulled pork sandwiches (64 of 79; 81.0%) and the meat pizza (13 of 21; 61.9%) (Table 2).
Distribution of gastrointestinal symptoms among 66 case patients with acute gastrointestinal illness associated with Clostridium perfringens and Bacillus cereus exposure, Homer, Alaska, August 2021 a
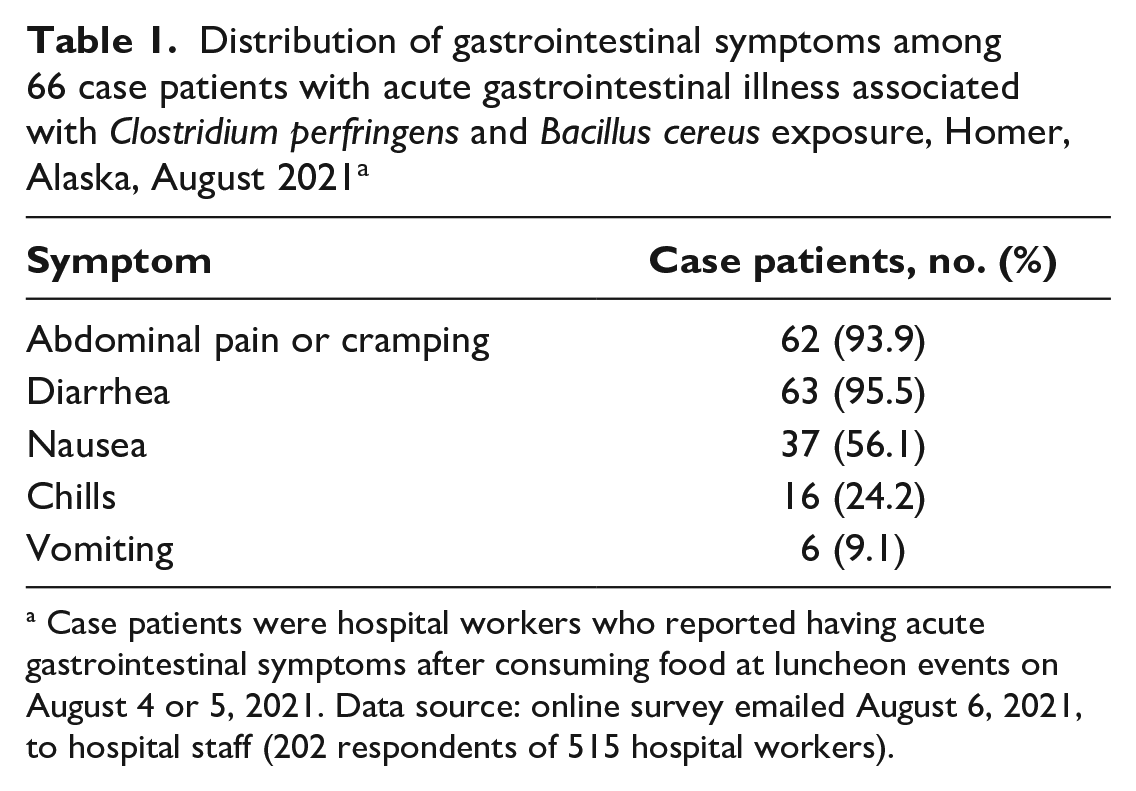
Case patients were hospital workers who reported having acute gastrointestinal symptoms after consuming food at luncheon events on August 4 or 5, 2021. Data source: online survey emailed August 6, 2021, to hospital staff (202 respondents of 515 hospital workers).
Association between exposure to Clostridium perfringens and Bacillus cereus from food served at 2 lunch dates and gastrointestinal illness among hospital employees in Homer, Alaska, August 2021 a
Abbreviation: OR, odds ratio.
Data source: online survey emailed August 6, 2021, to hospital staff (202 respondents of 515 hospital workers).
Significance determined by the Pearson χ2 test or Fisher exact test (when ≥1 cell count is ≤5), with P
Adjusted odds ratios. Multivariable logistic regression was adjusted for age, sex, and other significant food exposures from bivariable analyses, with P
Variable not included in multivariable model due to lack of significance in bivariable analysis.
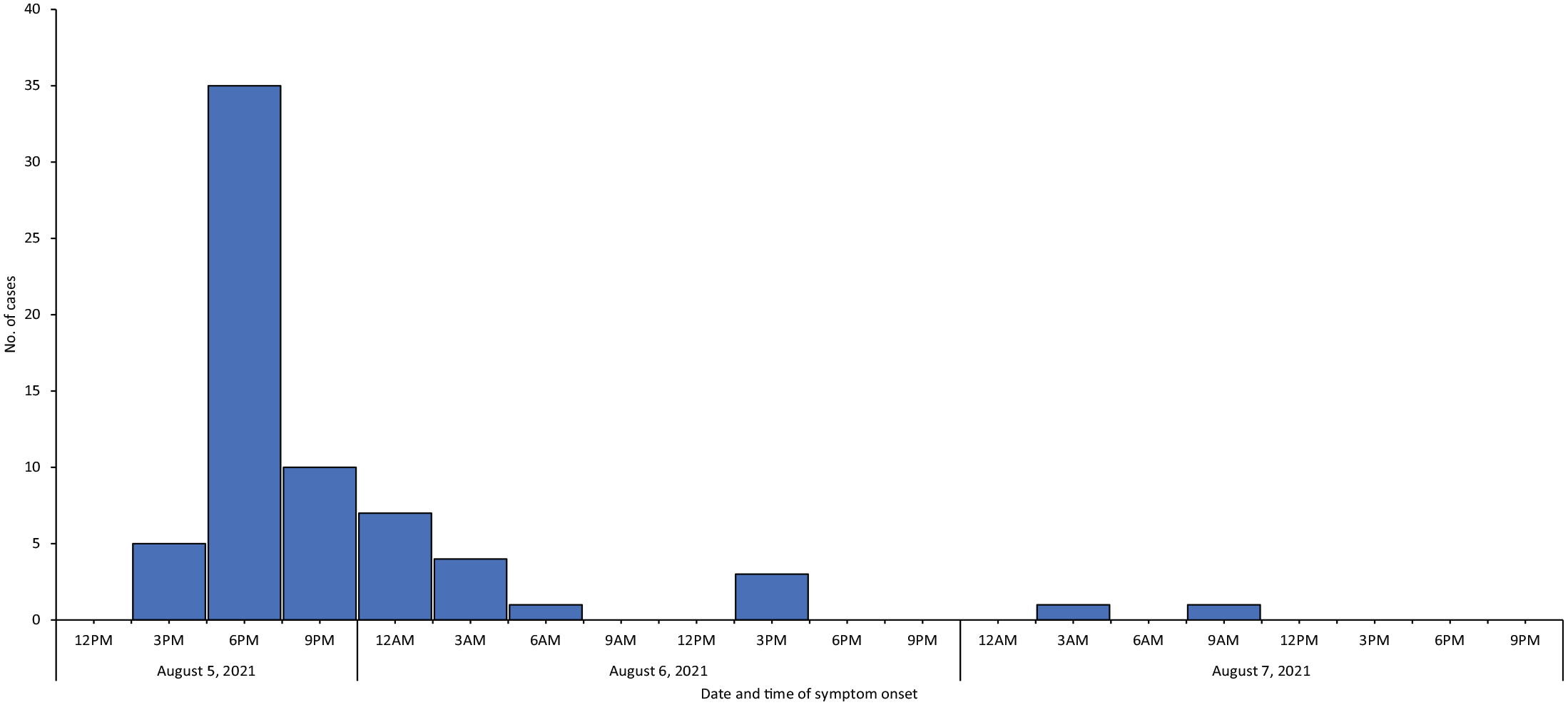
Confirmed hospital workers who met the outbreak case definition of having acute gastrointestinal symptoms associated with Clostridium perfringens and Bacillus cereus exposure, by onset date and time, Homer, Alaska, August 2021. Data source: online survey emailed on August 6, 2021, to hospital staff (202 respondents of 515 hospital workers).
Logistic Regression Analysis
In bivariable analysis, food types that were highly associated with gastrointestinal illness were the ham and pulled pork sandwiches (OR = 258.1; 95% CI, 57.2-1164.1), broccoli salad (OR = 9.7; 95% CI, 4.9-19.2), and meat pizza (OR = 3.9; 95% CI, 1.4-11.5). In the final multivariable analysis among foods evaluated, only consumption of the ham and pulled pork sandwiches remained associated with significant increased odds of gastrointestinal illness (adjusted OR = 296.4; 95% CI, 76.7-2019.1; P < .001).
Laboratory Investigation
C perfringens enterotoxin detection by reverse passive latex agglutination identified C perfringens in all 5 samples. C perfringens and B cereus were isolated from 2 leftover sandwich samples at sufficient levels to cause human illness. B cereus was also isolated from the broccoli salad dish prepared at the same establishment as the ham and pulled pork sandwiches; however, detected levels did not meet the infective dose consistent with levels that pose a human health hazard. No pathogens were isolated from the single piece of sliced ham available for testing.
Environmental Investigation
The environmental investigation found that the suspected ham and pulled pork sandwiches were made for hospital staff and not sold publicly, limiting further exposure. No clear deficiencies were identified in food storage, processing, or handling procedures at the vendor site. Cooking and holding temperatures of the sandwich contents were also found to comply with Alaska food establishment requirements. However, the investigation did observe other food items at the site being improperly cooled and stored in a refrigerator outside the required temperature range (>41 °F). These foods were discarded, and food safety officers made corrective actions on-site, including addressing cooling and cold holding practices with the vendor and implementing a requirement for weekly temperature logs.
Discussion
Our investigation suggests that the large point-source outbreak of acute gastroenteritis was likely attributable to consumption of contaminated ham and pulled pork sandwiches cooked by and obtained from a food vendor. This finding was supported by laboratory detection of C perfringens enterotoxin in all collected stool specimens and detection of C perfringens and B cereus isolates in sandwich samples at sufficient levels to cause human illness. Although the environmental investigation was inconclusive in the context of the implicated sandwiches, other food items were found to be improperly stored by the food vendor. This evidence suggests that inadequate temperature control was a possible factor involved in facilitating pathogen proliferation in the sandwiches. C perfringens and B cereus are common contaminants of raw meat products, and inadequate temperature control is an established risk factor for both pathogens.6,7
Our investigation adds to the limited evidence base on outbreaks simultaneously involving multiple distinct pathogens.8-11 Although challenges exist in the detection of toxin-producing pathogens such as B cereus and C perfringens because of their short incubation and illness periods, increased detection of multiple-etiology foodborne outbreaks in general in the United States is likely, given the ongoing development of multianalyte culture-independent diagnostic test panels. Jurisdictions should take advantage of the increased availability of tests for multiple-etiology outbreaks to better understand the full scope of causes of foodborne outbreaks.12,13 We isolated C perfringens and B cereus from foods at sufficient levels to confirm their etiology in this multipathogen outbreak. 3 However, it is important to note that the guidelines to confirm C perfringens and B cereus have been developed for use in culture and phenotypic tests and may need to be adjusted with the development and use of multiplex polymerase chain reaction methods.
The mild self-limited gastrointestinal illness experienced by case patients in the outbreak reported in our study corresponds to the typical characteristics of C perfringens and the diarrheal form of B cereus infection. 3 We were unable to determine whether 1 of these pathogens was more likely than the other to be responsible for symptoms in case patients.
Limitations
This investigation had several limitations. First, use of an online survey to collect food histories and clinical symptoms, which had a moderate response rate (39.2%), is inherently prone to recall biases, whereby case patients can be more likely than nonrespondents to complete the survey or accurately recall their food history. However, given the substantial magnitude of the association between consumption of the ham and pulled pork sandwiches and reported gastrointestinal illness, we do not expect these biases to affect overall investigation findings. Second, the survey did not collect data on precise times of food distribution and consumption, thereby limiting accuracy of incubation period calculations. Third, identifying a specific sandwich ingredient as the causative agent for this outbreak was not possible because of the limited number of leftover food specimens sent for laboratory testing. In addition, because C perfringens and B cereus are common contaminants of raw meat products, differentiating the likelihood of their presence in the ham versus the pulled pork was not possible. Although we did not isolate C perfringens or B cereus from the single isolated ham sample tested, these results alone are not definitive given the lack of supporting epidemiologic evidence and the testing of only 1 ham sample. Finally, not enough stool sample was available to test for B cereus.
Conclusions
To our knowledge, this is one of the largest multipathogen foodborne outbreaks in a health care setting described in the published literature in the United States. Although outbreaks attributable to toxin-producing foodborne pathogens are common, 14 they can be prevented by ensuring that foods are cooked, held, and stored at the correct temperature. Quick notification and effective collaboration among state partners, hospital staff, and the vendor site substantially strengthened investigation effectiveness to detect the outbreak, identify the responsible food vehicle, and mitigate any further risk.
Footnotes
Acknowledgements
The authors thank their partners and colleagues at South Peninsula Hospital; Alaska State Public Health Laboratory; Alaska Department of Environmental Conservation, Food Safety and Sanitation Program, and Environmental Health Laboratory; Alaska Department of Health, Section of Public Health Nursing; Centers for Disease Control and Prevention, Enteric Diseases Laboratory Branch; and Washington State Public Health Laboratories.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.