
Abstract
The COVID-19 pandemic has placed an unprecedented burden on patients, health care providers, and communities and has been particularly challenging for medically underserved populations impacted by the social determinants of health, as well as people with co-occurring mental health and substance use risks. This case study examines outcomes and lessons learned from a multisite low-threshold medication-assisted treatment (MAT) program at a federally qualified health center in partnership with a large suburban public university in New York to integrate and train Health Resources & Services Administration Behavioral Health Workforce Education and Training–funded graduate student trainees in social work and nursing in screening, brief intervention, and referral to treatment and patient care coordination, including social determinants of health and medical and behavioral comorbidities. The MAT program for the treatment of opioid use disorder has a low threshold for entry that is accessible and affordable, reduces barriers to care, and uses a harm reduction approach. Outcome data showed an average 70% retention rate in the MAT program and reductions in substance use. And, while more than 73% of patients reported being somewhat or definitely impacted by the pandemic, most patients endorsed the effectiveness of telemedicine and telebehavioral health, such that 86% indicated the pandemic did not affect the quality of their health care. The main implementation lessons learned were the importance of increasing the capacity of primary care and health care centers to deliver integrated care, using cross-disciplinary practicum experiences to enhance trainee competencies, and addressing the social determinants of health among populations with social vulnerabilities and chronic medical conditions.
Keywords
The COVID-19 pandemic has placed an unprecedented burden on patients, medical and behavioral health care providers, and communities. Because of quarantine restrictions, treatment of substance use disorders (SUDs) that required in-person visits was interrupted, potentially leading to a recurrence of substance use.1 -3 The pandemic presented a particular challenge to medically underserved populations and people with co-occurring mental health and substance use risks and opioid use disorder (OUD) because of vulnerabilities including psychosocial stressors (eg, poverty, diminished respiratory health, comorbid chronic diseases).2 -5 OUD can lead to impairment or distress, recurrent social or interpersonal problems, and the potential for chronic opioid abuse and early death.4 -7
Coinciding with the implementation of widespread mitigation measures for the pandemic and the need to address comorbidity, a pressing need also exists to address SUDs, including opiate overdose reversal interventions, medication-assisted treatment (MAT), and effective alternatives to pain management.8,9 Addressing this need involves increasing the capacity of primary care and health care centers to deliver integrated care and includes the need for overdose prevention and harm reduction strategies in the context of telehealth services. Systemwide changes involving the use of team-based brief interventions and collaborative care management models to increase practice integration are needed.10 -14 The US Department of Health and Human Services has recommended a 5-point strategy to combat the opioid epidemic, including (1) prevention, (2) treatment and recovery, (3) effective data collection, (4) pain management, and (5) utilization of pharmacotherapy. 15 These recommendations can be implemented through harm reduction strategies that include collaborative treatment, opioid maintenance therapy, and fully integrated MAT programs at federally qualified health centers (FQHCs) using a team-based approach in which waivered medical providers and social workers address all identified medical and psychosocial needs.
Consistent with the literature on team-based care, a systemwide pipeline for delivering integrated workforce-ready treatment providers (ie, graduate students in behavioral health and social work, as well as psychiatric mental health nurse practitioners [PMHNPs]) has been shown to be an important component of integrated care for OUD. In fact, the Health Resources and Services Administration (HRSA) allocated additional resources to fund training initiatives to establish this infrastructure for graduate health care training programs to improve public health outcomes that also targeted efforts to reduce health care provider burnout, which became critical during the pandemic when the acute need for additional help became evident. The barriers to building capacity for MAT include workforce development issues associated with locating skilled MAT providers, delivering telehealth/telemedicine, and training non-MAT professionals (eg, social workers, other medical providers) to screen for SUD, provide behavioral health interventions, and refer patients appropriately for services. The Agency for Healthcare Research and Quality has described models of care for integrating OUD MAT into primary care settings and derived common components for care that include (1) pharmacotherapy with buprenorphine or naltrexone, (2) health care provider and community education, (3) coordination and integration of OUD with other medical and psychological needs, and (4) psychosocial services and interventions. 11
Purpose
The purpose of this case study is to describe the primary lessons learned from this HRSA integrated/interprofessional Behavioral Health Workforce Education and Training (BHWET) project: (1) developing curricula to support integrated care coordination for graduate student trainees and community health care providers, (2) building effective care coordination in primary care centers with a focus on the delivery of low-threshold MAT for OUD, and (3) delivering MAT and care coordination through telemedicine.
Methods
Through the HRSA workforce development project, graduate social work and nursing programs at Stony Brook University (SBU) with a specialized integrated behavioral health curriculum partnered with an FQHC to enhance team-based care. The FQHC provides comprehensive primary, preventive, behavioral, and oral health care in 11 counties in New York State to more than 176 000 predominantly low-income, racially and ethnically diverse patients annually. The counties vary from rural (eg, Hudson Valley) to urban (eg, Yonkers), and most counties have inadequate (or absent) public transportation systems and lack resources such as subsidized housing and social services. The SBU project serves Suffolk County, which covers a large geographic region on the east end of Long Island. Suffolk County has large socioeconomic disparities, with extreme wealth in some regions (the Hamptons) and abject poverty in other regions. Suffolk County also has a poor to nonexistent public transportation system. The MAT program operates as a low-threshold-for-entry program and uses a harm reduction approach to enhance engagement, increase access to care, and ensure safety. The FQHC uses a multidisciplinary team model, consisting of a MAT provider, a licensed practical nurse, a care manager, an outreach coordinator, and an SBU social worker and PMHNP. Trainees are part of the care coordination team. An integral part of this MAT program is the education of patients, staff, and community members on opioid overdose prevention with naloxone.
Clients accessing mental health services are offered an integrated continuum of care, including initial screening and assessment (psychosocial multi-contextual evaluation with a behavioral health specialist), diagnosis, development of a treatment plan, referrals to a mental health specialist for treatment and/or psychiatry or adjunctive services for more intensive mental health needs, referral to the FQHC’s expanded suboxone/buprenorphine program or partnering alcohol and substance use treatment programs, crisis intervention, care coordination, and clinical supervision. Services include individual and group counseling, patient education, and case management. MAT services start with infectious disease testing and patient and health care provider referral for a comprehensive screen that provides an assessment of active use of alcohol or nonopioid substances. The program provides an intensive field experience opportunity for trainees. Trainees receive stipends and curated social work and nursing graduate courses in integrated care (eg, motivational interviewing, cognitive behavioral therapy), supporting their competencies and clinical skills in conducting initial assessments and providing patient care throughout their engagement with the MAT program. Moreover, to maintain continued access to MAT at the onset of the pandemic, the clinicians and prescribers at the FQHC adopted telemedicine and telehealth strategies into the workflow. In addition to the BHWET grant, the FQHC also received a Center for Substance Abuse and Treatment quality improvement grant targeting the needs of patients with co-occurring disorders, which provided additional support for evaluation of the MAT program and training.
Data Collection
Our analysis included data on MAT program patients enrolled in treatment at the FQHC from January 2019 through November 2020; all data collected and extracted were de-identified. In addition, we calculated retention rates from the electronic health record (EHR) from January 2019 through October 2020. We used 3 datasets: (1) the FQHC’s EHR for aggregate patient outcomes (E-Clinical Works 11 e v11.52.305.66.20; N = 606); (2) SBU’s HRSA project assessing trainee knowledge acquisition focused on integrated care and the elements of screening, brief intervention, and referral to treatment (SBIRT), 16 as well as competencies in MAT (N = 121 trainees); and (3) intake interviews via social workers/care coordinators (N = 439) using data from a comprehensive psychosocial assessment Government Performance and Results Act (GPRA OMB-0930-280) federal report as part of the Center for Substance Abuse and Treatment HIV grant. 17 The current evaluation was a quality improvement effort focused on measuring and enhancing the standard of care; thus, the SBU Institutional Review Board considered this study exempt from institutional review board review.
The GPRA tool is used to measure functioning during the past 30 days across a range of areas including substance use, mental health, criminal justice involvement, employment and education, social support, housing, and other wellness items. Examples of items on the GPRA tool included energy levels, physical health, wellness, and quality of life. This interview assessment tool was originally developed by using the Addiction Severity Index 18 ; on average, it took about 25-35 minutes to complete. Patients were readministered the GPRA 6 months post-intake to measure changes across these life domains.
Of 439 patients who received the GPRA interviews, 254 (58%) were male and 185 (42%) were female; 68 (15%) were Hispanic or Latino, 25 (6%) were African American, and 19 (4%) were Native American; and 272 (62%) were aged 25-44 years. Patients were diagnosed with multiple physical and mental health conditions and comorbid diabetes, HIV, hepatitis, chronic obstructive pulmonary disorder, hypertension, and traumatic stress/posttraumatic stress disorder.
Model/Approach
The SBU project enhances the health care workforce to address current needs resulting from health disparities and inequities in access to care compounded by the opioid epidemic and COVID-19 pandemic. As the nation enters the next phase of the pandemic, it is important to identify and disseminate successful efforts and lessons learned, such that professionals can apply them for enhancing more effective care. This case study illustrates the successes of the SBU project, in partnership with a large multisite FQHC in New York and with patients with lived experience, to develop effective integration models and recovery pathways in addiction treatment. 12 The SBU project is a 4-year behavioral health workforce training project funded by HRSA to embed students in the SBU School of Social Welfare and PMHNP students in high-need, high-demand community care settings. In this case study, we explore outcomes from a multisite FQHC effort to integrate and train graduate students in SBIRT 15 and care coordination using the Collaborative Care Model19 -21 adopted by the university and the FQHC. An additional focus was on addressing the needs of racial and ethnic minority people with SUD or co-occurring substance use/mental health disorders who are HIV positive or at high risk for HIV and hepatitis C virus infection.
The Collaborative Care Model incorporates a population management evidence-based approach for integrating physical and behavioral health services that can be implemented within a primary care–based Medicaid health home model, among other settings. 13 The model establishes collaboration among patients, care managers, social workers, nurses, PMHNPs, medical providers, and psychiatrists. Communication among mental health providers is often disconnected, and 50% to 90% of referrals made to other clinics or health care providers do not result in an appointment. 14 To address these barriers, some primary care practices use a co-location model in which a behavioral health provider, such as a psychologist, PMHNP, or licensed clinical social worker, is available at the same location. 22 Although co-location eliminates some barriers to access, our case study illustrates the move toward fully integrated behavioral health care, in which the behavioral health provider is treated as a member of the practice, takes part in team meetings, and shares workspace, infrastructure, records, and support systems.19 -21
Since 2017, social worker and PMHNP student trainees have been embedded to provide SBIRT within the framework of the Collaborative Care Model. This approach accounts for shifts in the demands in behavioral health care and the impact of the COVID-19 pandemic in community primary care and behavioral health organizations.22 -24 Preparation for onboarding at the site included a didactic component, role-playing, cross-disciplinary training, interactive exercises, and the use of standardized patients to evaluate SBIRT and motivational interviewing knowledge and skills acquisition. At the onset of the COVID-19 pandemic, the project team successfully pivoted to online training that included video conferencing and the use of standardized patients. Curricula changes enhanced typical specialized advanced graduate courses by adding methods in integrated health, clinical practice, telehealth, trauma-informed care, SBIRT and SUD/OUD, and specialty supervision from social work field placements and nursing clinical rotation faculty. The SBIRT trainings include the use of and response to risks identified from an automated suite of screening tools: Patient Health Questionnaire, Alcohol Use Disorders Identification Test, Drug Abuse Screening Test, Cannabis Intervention Screener, and the Generalized Anxiety Disorder assessment.23,24 Booster sessions were held throughout the field placements to provide real-time training enhancements, address supervision issues, and reinforce learning as students identified workflow or clinical challenges.
Statistical Analysis
We conducted descriptive analyses to examine patient engagement, retention, and health care provider type from the FQHC’s EHR. To measure the significance of change between GPRA intake and the 6-month follow-up, we conducted 1-tailed and 2-tailed paired t tests using SPSS version 26.0 (IBM Corp). Variables examined included substance use, mental health, and physical health indicators. We considered P < .05 to be significant.
Results
A total of 606 patients were in the MAT program during the 18-month study period. In January 2019, after 1 month of treatment, 563 patients had been prescribed MAT, and 460 adhered to their MAT regimen. By October 2020, 339 patients were in the MAT program, 210 of whom adhered to their MAT regimen.
Eighty-eight graduate social work students and 33 PMHNP students were trained in SBIRT. Of 121 graduate students who responded to questions about demographic characteristics, 16 reported male sex, 18 reported female sex, and 54 did not respond to the question; 53 were White, 27 were Black, 8 were Asian, 13 were Hispanic, 5 were multiracial, and 15 students did not respond. Eighteen students were placed in the FQHC sites that included the integrated FQHC MAT program. In the MAT program, among patients whose first visit was with a MAT provider, the next follow-up visit occurred with licensed clinical social workers, other licensed mental health providers, nurse practitioners, and family physicians.
FQHC EHR data showed the following outcomes: (1) 294 of 428 (68.7%) MAT patients remained in care at 6 months; (2) 277 of 439 (63.1%) patients who responded to the GPRA follow-up survey had mental health symptoms (eg, depression, anxiety) in the past 30 days, and 248 of 606 (40.9%) had a mental health diagnosis; (3) 170 of 606 (28.1%) patients had an HIV and/or hepatitis C virus infection; (4) 279 of 606 (46.0%) patients endorsed risky behaviors (injecting drugs, having unprotected sex, having sex with multiple partners, drunk and disorderly, fighting, and criminal activity); (5) during the 18-month study period, 9 of 69 (13.0%) patients had a fatal overdose; and (6) patients aged 30-39 years were 5 times more likely to overdose than patients aged 20-29, 40-49, and 50-59 years. Although more than 73% of patients reported being somewhat to definitely impacted by the pandemic, 72% reduced or did not change the level of substance use from pre–COVID-19 to COVID-19, and the effectiveness of the telemedicine/telehealth approach was endorsed by 86% of the patient population who indicated that the pandemic did not affect the quality of health care they received at the FQHC.
GPRA data represented 439 FQHC patients who endorsed the top 4 drugs of choice as heroin (26%), marijuana (2%), cocaine/crack (18%), and Oxycontin (4%). We found a significant increase in the rates of abstinence among patients who were non-Hispanic White (from 41.0% at intake to 63.2% at 6-month follow-up; P < .001) and non-White and/or Hispanic (from 43.8% at intake to 67.2% at follow-up; P = .001) (Table 1).
Change in abstinence at 6-month follow-up among patients receiving medication-assisted treatment for opioid use disorder at a federally qualified health center in New York (N = 439), January 2019–November 2020
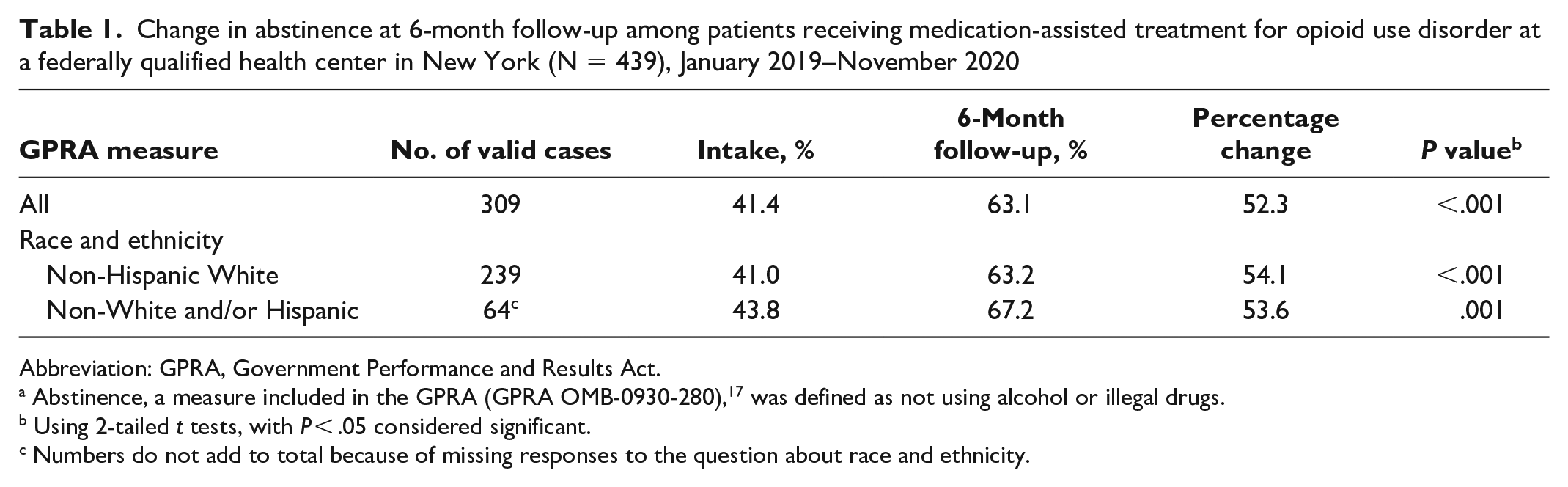
Abbreviation: GPRA, Government Performance and Results Act.
Abstinence, a measure included in the GPRA (GPRA OMB-0930-280), 17 was defined as not using alcohol or illegal drugs.
Using 2-tailed t tests, with P < .05 considered significant.
Numbers do not add to total because of missing responses to the question about race and ethnicity.
We found a significant decrease in the mean number of days of heroin use, from 3.62 days at intake to 1.34 days at 6-month follow-up (P < .001) (Table 2). Moreover, the use of other substances significantly decreased, with the exception of Percocet. Through November 2022, of 453 patients, 313 completed follow-up; 306 patients responded to a question about whether they had injected illegal drugs. The numbers of patients (n = 295) reporting they had not injected any substance from intake to the 6-month follow-up interview were as follows: 42 (14.2%) at intake and 22 (7.5%) at follow-up (P < .001). There was a 7 percentage-point increase in the number of patients reporting not injecting any substance (n = 288) from intake (15%) to 6-month follow-up (8%; P < .001).
Change in the mean number of days of use, by drug type, from intake to 6-month follow-up among patients receiving medication-assisted treatment for opioid use disorder at a federally qualified health center in New York, January 2019–October 2020
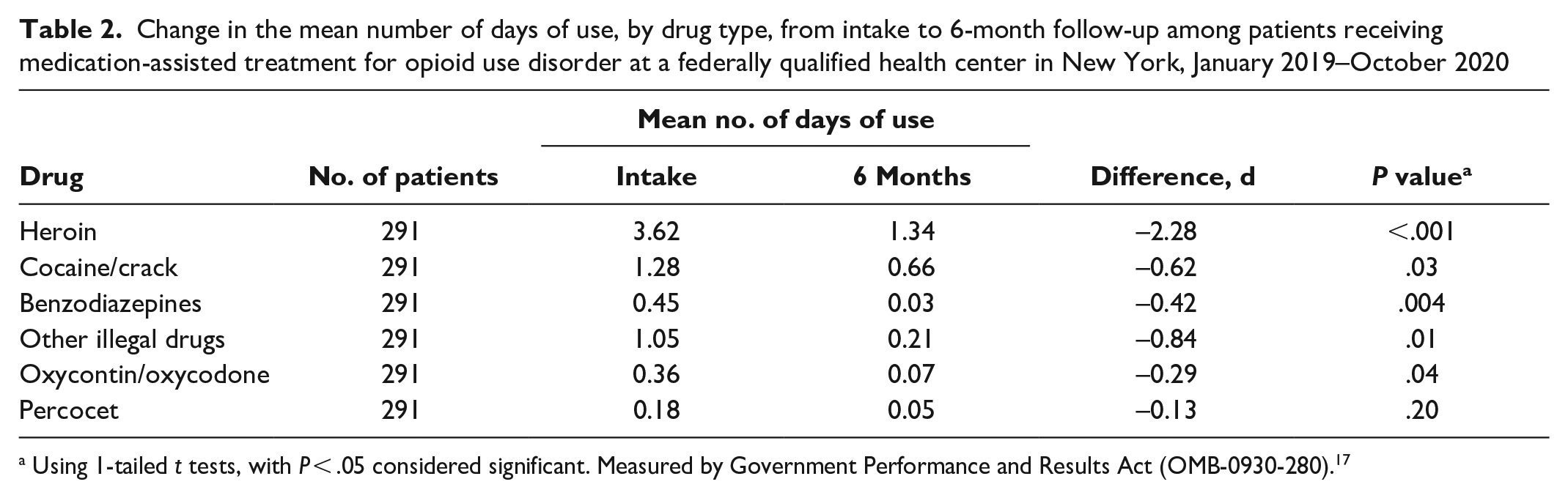
Using 1-tailed t tests, with P < .05 considered significant. Measured by Government Performance and Results Act (OMB-0930-280). 17
Patient physical health also improved from intake to follow-up: the percentage of patients who indicated “feeling good” increased from 36% at intake to 43% at follow-up, and the percentage of respondents who indicated “feeling poorly” decreased from 9% at intake to 4% at follow-up. In addition, the percentage of patients (n = 287) who reported their quality of life improved from “very poor” or “poor” to “good” increased from 52% at intake to 60% at follow-up (P = .02). Energy levels also increased significantly (P = .009), and substance-related negative health, behavioral, or social consequences decreased significantly by 11.5% from intake to 6-month follow-up (n = 27; P < .001).
Lessons Learned
These outcomes are consistent with or better than outcomes listed in the broad body of research on MAT to date, which typically shows 50% retention in care.9 -11 Limited research is focused on the efficacy of low-threshold MAT programs, with few studies describing their features.3,25 Our findings illustrate the effectiveness of delivering MAT for OUD using a team-based harm reduction approach for patients with complex health care needs through an interprofessional integrated care model. Low-threshold community-based treatment is critical to addressing the social determinants of health and enhancing the continuity of care among patients with multiple comorbidities. In addition, innovative low-threshold MAT is essential to reducing barriers and enhancing access to care in the delivery of in-person care and flexible telehealth protocols. 26 Qualitative data and feedback from students in social work and PMHNP student trainees and field supervisors indicated that the SBU training model contributed to effective workforce development through the use of the Collaborative Care Model. Future research should include group comparison designs to further test the Collaborative Care Model using matched samples of patients with and without low-threshold MAT.
This case study highlights the following key lessons learned from the SBU FQHC collaboration that can be generalized to other university and community workforce development programs for successful outcomes, particularly during the COVID-19 pandemic:
(1) Develop strategies for redesigning social work and nursing graduate education and workforce development in SUD/OUD knowledge and clinical skills (eg, SBIRT/motivational interviewing).
(2) Use cross-disciplinary practicum experiences and increase trainee competencies with real-life application incorporating medical program managers and field supervisors to enhance sustainability.20 -22
(3) Deliver an enhanced, patient-centered, integrated care coordination model that boosts physical and mental health outcomes and increases retention and engagement in MAT.9,11
(4) Respond to the pandemic by using a low-threshold MAT model and adopting a more flexible approach to MAT services to individuals with OUD, transitioning to a telehealth model of care in combination with in-person appointments.
Enhancements can include increasing contact through an outreach coordinator to ensure patient needs are met and increasing distribution and access to naloxone kits, both of which are consistent with a low-barrier approach to prevent opioid overdose. Finally, future program improvements include the need to screen for posttraumatic stress and develop effective, culturally responsive trauma-informed interventions for OUD.
Footnotes
Acknowledgements
The authors acknowledge the long-standing partnership between Stony Brook University and Sun River Health that made this research possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Health Resources and Services Administration Behavioral Health Workforce Education and Training grant support.