
Abstract
Objective:
The COVID-19 pandemic has disrupted traditional health care, including pediatric health care. We described the impact of the pandemic on disparities in pediatric health care engagement.
Methods:
Using a population-based cross-sectional time-series design, we compared monthly ambulatory care visit volume and completion rates (completed vs no-show and cancelled visits) among pediatric patients aged 0-21 years in 4 states in the mid-Atlantic United States during the first year of the COVID-19 pandemic (March 2020–February 2021) with the same period before the pandemic (March 2019–February 2020). We used unadjusted odds ratios, stratified by visit type (telehealth or in-person) and sociodemographic characteristics (child race and ethnicity, caregiver primary language, geocoded Child Opportunity Index, and rurality).
Results:
We examined 1 556 548 scheduled ambulatory care visits for a diverse pediatric patient population. Visit volume and completion rates (mean, 70.1%) decreased during the first months of the pandemic but returned to prepandemic levels by June 2020. Disparities in in-person visit completion rates among non-Hispanic Black versus non-Hispanic White patients (64.9% vs 74.3%), patients from socioeconomically disadvantaged versus advantaged communities as measured by Child Opportunity Index (65.8% vs 76.4%), and patients in rural versus urban neighborhoods (66.0% vs 70.8%) were the same during the remainder of the first year of the pandemic as compared with the previous year. Concurrent with large increases in telehealth (0.5% prepandemic, 19.0% during the pandemic), telehealth completion rates increased.
Conclusions:
Disparities in pediatric visit completion rates that existed before the pandemic persisted during the pandemic. These findings underscore the need for culturally tailored practices to reduce disparities in pediatric health care engagement.
The COVID-19 pandemic has disrupted traditional health care, introducing widespread changes in patterns of health care use. While studies have detailed how the pandemic has affected adult health care delivery,1-6 less is known about the impact on pediatric health care. Health care engagement of pediatric populations is critical to ensuring that children, adolescents, and young adults receive preventive care and treatment for acute and chronic conditions in a timely manner. Decreases in emergency department visits, hospitalizations,7-9 and routine vaccinations have occurred among pediatric populations.10,11 Studies have also described reduced volume of pediatric primary care and sick visits in the early months of the pandemic.12,13 It remains unclear how pediatric health care engagement, including visit attendance, has changed during the pandemic.
Studies of adults have shown that the same disparities in health care utilization that existed prior to the pandemic have persisted,14,15 with non-Hispanic Black and Hispanic adults and adults with Medicaid experiencing decreased use of in-person and telehealth services.1-6 Black and Hispanic populations and socioeconomically disadvantaged populations have always faced decreased access to quality health care because of complex systemic factors, such as structural racism in health care and barriers to health care access, including reduced economic and educational opportunities and linguistic and transportation barriers.14,15 However, to our knowledge, no studies have evaluated the role of neighborhood-level variables on health care engagement during the pandemic or the impact of telehealth on pediatric health care access.16,17
We aimed to describe changes in pediatric health care engagement during the first year of the pandemic (March 2020–February 2021) as compared with the previous year (March 2019–February 2020) among 1 556 548 scheduled pediatric visits. For this study, we defined health care engagement in terms of visit volume and completion rates (completed scheduled visits vs no-show and cancelled visits) for primary and specialty ambulatory visits and for in-person and telehealth visits. A secondary objective was to describe disparities in the completion of scheduled ambulatory care visits during the first year of the pandemic, including disparities by demographic characteristics and geocoded neighborhood-level factors. We hypothesized that visit completion rates would be lower during the first year of the pandemic than in the same months of the year before the pandemic, especially in socioeconomically disadvantaged populations.
Methods
Study Design, Population, and Setting
We conducted a population-based cross-sectional time-series study using retrospective data from the electronic health record (EHR) of a large pediatric health care system providing care in 4 states in the mid-Atlantic United States. We extracted data on all scheduled primary care and specialty care ambulatory visits for patients aged 0-21 years in the year before the COVID-19 pandemic (March 2019–February 2020) and in the first year of the pandemic (March 2020–February 2021). Concurrent with the states of emergency and closure of schools and nonessential businesses across the region, our pediatric health care system cancelled all nonurgent care on March 18, 2020. This state of emergency ended April 2, 2020, and precautions were instituted, including policies on wearing face masks, limiting the number of family members who could accompany a pediatric patient to a visit, and screening visitors for infectious diseases, to facilitate the reopening of facilities for nonurgent care. Telehealth-to-home visits through a mobile platform were encouraged. Soon after, phased reopening began but was halted by a surge in COVID-19 cases from November 2020 through January 2021.
Outcome Variables: Health Care Engagement
We extracted data from the EHR about each scheduled visit: date, type (in-person or telehealth), department, and completion status (completed, no-show, left without being seen, or canceled by patient or for technology issues). Visits that were scheduled with the outpatient laboratory and occurred on the same day that they were scheduled were also excluded because they represented urgent visits (eg, sick visits) that were more likely to be completed than routine preventive visits. Our primary outcome measures were number and rate of completed visits each month (ie, total number of completed visits divided by total number of scheduled visits). Because visit completion rates were the same between primary care and specialty care visits (71% and 70%, respectively), we evaluated these visits together. The Nemours Institutional Review Board approved this study.
Predictor Variables: Sociodemographic Characteristics
We extracted data from the EHR on the patient’s race and ethnicity, sex, and age; the primary language of the patient’s caregiver; the patient’s household zip code; and the patient’s health insurance status (private, public, or other). We grouped and categorized pediatric patients’ race and ethnicity as non-Hispanic Black (Black), Hispanic, non-Hispanic White (White), non-Hispanic multiracial (multiracial), or other; we also categorized caregiver primary language as English or non-English (ie, Spanish or other). We used zip code to identify pediatric patients from rural neighborhoods (rural–urban commuting area code ≥4) 18 and to categorize neighborhood inequity based on the Child Opportunity Index (COI; state normed). 19 The COI combines indicators of education (eg, early childhood education enrollment, high school graduation rate), health and environment (eg, access to healthy food, health insurance coverage), and socioeconomic opportunity (eg, employment rate, median annual household income) for all US neighborhoods. These indicators are used to categorize COI as very low, low, moderate, high, and very high.
Analysis
We used Stata version 17.0 (StataCorp) for all analyses. We calculated visit completion rates by month for the prepandemic and pandemic periods and then stratified by visit type (telehealth or in-person) and sociodemographic variables (patient’s race and ethnicity, caregiver primary language, COI, and rurality). We used a suite of commands (“epitab”) that were designed for epidemiologic tables to compare monthly visit completion rates by sociodemographic variables by calculating unadjusted odds ratio (OR) point estimates (with an OR <1 indicating a lower likelihood of visit completion of a subgroup vs the referent group) and 95% CIs. We based the calculation of ORs on the Cornfield method of approximation to the sampling distribution. To describe ORs for sociodemographic variables where there were multiple categories (race and ethnicity, COI), we compared the 2 categories with the highest and lowest visit completion rates (White vs Black for race and ethnicity and COI of 1 vs 5), controlling for false-positive errors while conducting comparisons that would be most informative. 20 We produced corresponding graphs of the unadjusted ORs by month using the “meta” suite in Stata. Given the potential relationship between sociodemographic variables, we used the Mantel–Haenszel method to calculate adjusted ORs to confirm that the unadjusted ORs were not different in direction or significance as compared with adjusted ORs (data not shown).
Results
Patient and Visit Characteristics
A total of 181 523 unique pediatric patients had a scheduled visit in the year before the pandemic as compared with 175 501 unique pediatric patients in the first year of the pandemic (Table). The patient population—which was 11.4% Hispanic, 23.5% Black, and 5.4% rural and represented multiple age ranges and levels of COI—was nearly identical in the first year of the pandemic as compared with the previous year. A total of 786 120 scheduled visits took place in the year before the pandemic, and 770 429 took place in the first year of the pandemic. In both years, approximately 70% of visits were completed. Telehealth visits increased substantially from 0.5% prepandemic to 19.0% during the first year of the pandemic. The overall volume of visits decreased in the first few months of the pandemic but returned to prepandemic levels by month 4 (June 2020) (eFigure 1 in Supplemental Material).
Patient and visit characteristics among pediatric patients aged 0-21 years at a large mid-Atlantic pediatric health care system before and during the COVID-19 pandemic a
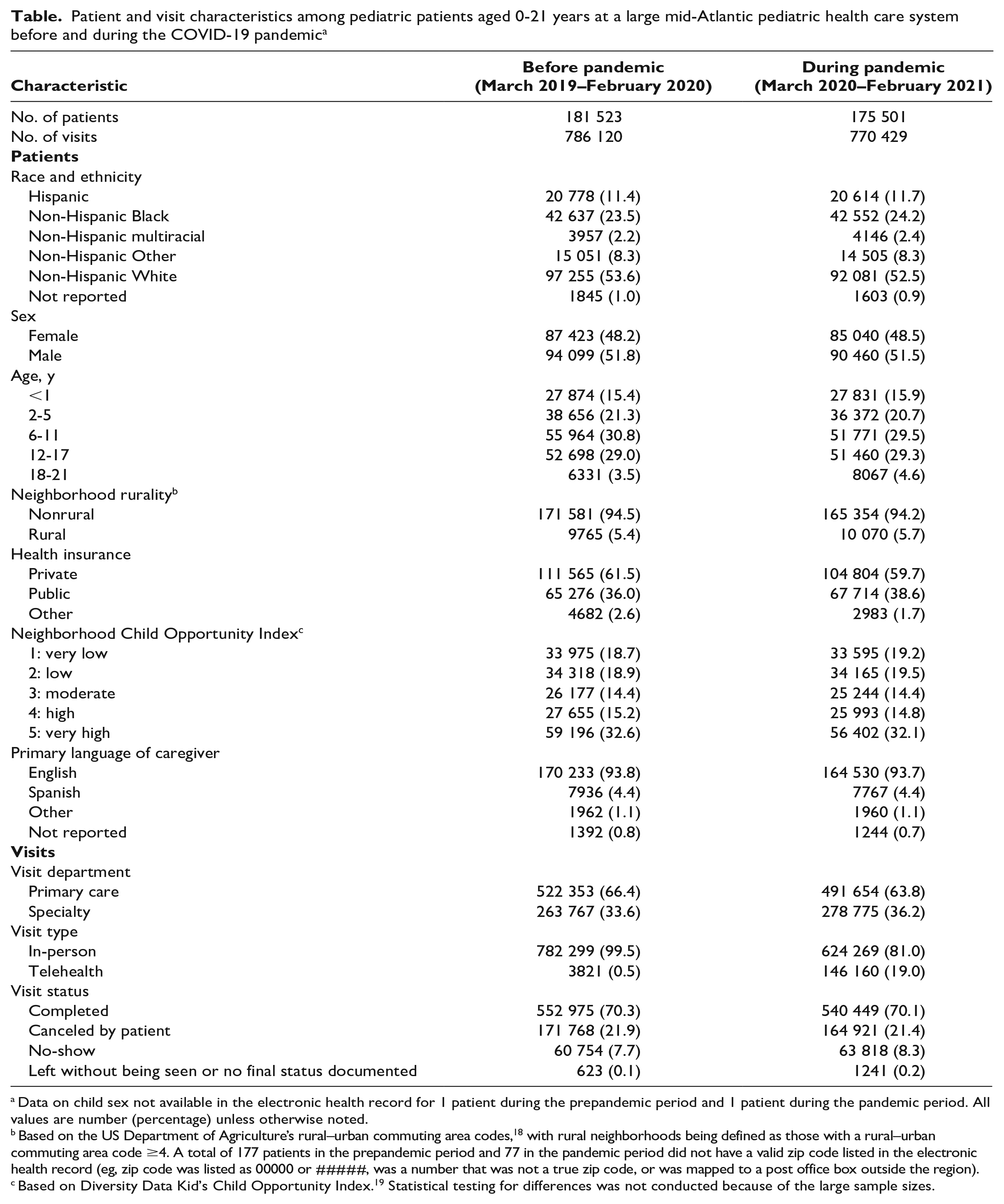
Data on child sex not available in the electronic health record for 1 patient during the prepandemic period and 1 patient during the pandemic period. All values are number (percentage) unless otherwise noted.
Based on the US Department of Agriculture’s rural–urban commuting area codes, 18 with rural neighborhoods being defined as those with a rural–urban commuting area code ≥4. A total of 177 patients in the prepandemic period and 77 in the pandemic period did not have a valid zip code listed in the electronic health record (eg, zip code was listed as 00000 or #####, was a number that was not a true zip code, or was mapped to a post office box outside the region).
Based on Diversity Data Kid’s Child Opportunity Index. 19 Statistical testing for differences was not conducted because of the large sample sizes.
Child Race and Ethnicity
Ambulatory visit completion rates were highest among White pediatric patients (mean, 73%), followed by pediatric patients who were other (72%), multiracial (69%), and Hispanic (69%); the lowest completion rates were among Black patients (63%).
In-person visits
Before the pandemic, Black pediatric patients were less likely (OR = 0.63; 95% CI, 0.61-0.64) to complete in-person visits than White pediatric patients (average completion rate, 63.3% vs 73.3%) (Figure 1). During April 2020, Black patients were more likely than White patients to complete in-person visits (OR = 1.19; 95% CI, 1.07-1.32). After month 2 of the pandemic, the disparities that existed before the pandemic reemerged with Black patients, who were less likely (OR = 0.63-0.67; 95% CI, 0.58-0.70) to complete in-person visits than White patients (average completion rate, 64.9% vs 74.3%).

Ambulatory care visit completion rates among non-Hispanic White and non-Hispanic Black pediatric patients (ages 0-21 years) before (March 2019–February 2020) and during (March 2020–February 2021) the COVID-19 pandemic, by race (Black or White), type of visit (A, in-person visits; B, telehealth visits), and month. Visit completion rates are from data on >1.5 million visits. To right, unadjusted odds ratios for visit completion by month (Black vs White [reference]). Error bars indicate 95% CIs.
Telehealth visits
Before the pandemic, Black pediatric patients were less likely (OR = 0.62; 95% CI, 0.48-0.76) to complete telehealth visits than White pediatric patients (average completion rate, 62.7% vs 70.5%). This disparity persisted during the pandemic: Black patients were less likely (OR = 0.50; 95% CI, 0.49-0.52) than White patients to complete telehealth visits (average completion rate, 56.7% vs 73.9%).
Caregiver Primary Language
In-person visits
Before the pandemic, pediatric patients for whom the caregiver’s primary language was not English (vs English) were more likely (OR = 1.16; 95% CI, 1.11-1.20) to complete in-person visits (average completion rate, 73.2% vs 70.2%) (Figure 2). During the first 5 months of the pandemic, we found no meaningful differences in in-person visit completion rates between pediatric patients based on the caregiver’s primary language. After month 5 of the pandemic (July 2020), the same differences that existed before the pandemic began to emerge. Pediatric patients for whom the caregiver’s primary language was not English (vs English) were again more likely (OR = 1.08-1.18; 95% CI, 1.00-1.28) to complete in-person visits (average completion rate, 72.7% vs 70.7%).

Ambulatory care visit completion rates among pediatric patients (ages 0-21 years) before (March 2019–February 2020) and during (March 2020–February 2021) the COVID-19 pandemic, by primary language of caregiver (non-English or English), type of visit (A, in-person; B, telehealth), and month. Visit completion rates are from data on >1.5 million visits. To right, unadjusted odds ratios for visit completion by month (non-English vs English [reference]). Error bars indicate 95% CIs.
Telehealth visits
Before the pandemic, pediatric patients for whom the caregiver’s primary language was not English (vs English) were less likely (OR = 0.41; 95% CI, 0.33-0.48) to complete telehealth visits (average completion rate, 50.3% vs 68.3%). The same disparities existed during the pandemic, but the disparity decreased (OR = 0.57; 95% CI, 0.54-0.61). Pediatric patients for whom the caregiver’s primary language was not English (vs English) had an average telehealth visit completion rate of 57.5% (vs 69.6%).
Neighborhood COI
In-person visits
We found a gradient effect: visit completion rates were generally highest among pediatric patients from neighborhoods with a COI of 5 and decreased with each level of COI. We therefore compared visit completion rates of patients from neighborhoods with a COI of 1 (disadvantaged) and a COI of 5 (advantaged) (Figure 3). Before the pandemic, patients from socioeconomically disadvantaged (vs advantaged) neighborhoods were less likely (OR = 0.66; 95% CI, 0.64-0.67) to complete in-person visits (average completion rate, 65.0% vs 73.9%). After month 2 of the pandemic, the same disparities that existed before the pandemic began to emerge. Patients from disadvantaged (vs advantaged) neighborhoods were again less likely (OR = 0.57-0.65; 95% CI, 0.53-0.68) to complete in-person visits (average completion rate, 65.8% vs 76.4%).

Ambulatory care visit completion rates among pediatric patients (ages 0-21 years) before (March 2019–February 2020) and during (March 2020–February 2021) the COVID-19 pandemic, by neighborhood Child Opportunity Index (COI), type of visit (A, in-person visits; B, telehealth visits), and month. Visit completion rates are from data on >1.5 million pediatric (ages 1-21 years) visits. The 2 groups are those with the highest (COI-5) and lowest (COI-1) completion rates. 19 To right, unadjusted odds ratios for visit completion by month (COI-1 vs COI-5 [reference]). Error bars indicate 95% CIs.
Telehealth visits
Before the pandemic, pediatric patients from disadvantaged (vs advantaged) neighborhoods were less likely (OR = 0.37; 95% CI, 0.26-0.47) to complete telehealth visits (average completion rate, 56.1% vs 72.1%). The same disparities existed during the pandemic, but the disparity decreased (OR = 0.51; 95% CI, 0.47-0.56). During the pandemic, patients from disadvantaged (vs advantaged) neighborhoods had an average telehealth completion rate of 60.2% (vs 74.8%).
Neighborhood Rurality
In-person visits
Before the pandemic, pediatric patients from rural (vs urban) neighborhoods were less likely (OR = 0.90; 95% CI, 0.88-0.92) to complete in-person visits (average completion rate, 68.2% vs 70.5%) (Figure 4). The same disparities existed during the pandemic, but the disparity increased (OR = 0.80; 95% CI, 0.77-0.84). During the pandemic, patients from rural (vs urban) neighborhoods had an average in-person visit completion rate of 66.0% (vs 70.8%).

Ambulatory care visit completion rates among pediatric patients (ages 0-21 years) before (March 2019–February 2020) and during (March 2020–February 2021) the COVID-19 pandemic, by neighborhood rurality (rural or nonrural), type of visit (A, in-person; B, telehealth), and month. Visit completion rates are from data on >1.5 million visits. To right, unadjusted odds ratios for visit completion (families from rural neighborhoods vs nonrural neighborhoods [reference]). 18 Error bars indicate 95% CIs.
Telehealth visits
Before the pandemic, pediatric patients from rural (vs urban) neighborhoods were less likely (OR = 0.54; 95% CI, 0.48-0.67) to complete telehealth visits (average completion rate, 56.5% vs 68.3%). The same disparities existed during the pandemic, but the disparity decreased (OR = 0.84; 95% CI, 0.78-0.89). Patients from rural (vs urban) neighborhoods were still less likely to complete their telehealth visits (average completion rate, 65.5% vs 69.3%), but the difference in completion rates between the groups was smaller. During April 2020, November 2020, and January 2021, when surges in COVID-19 cases occurred, the use of telehealth among pediatric patients from rural neighborhoods was comparable to that of families from urban neighborhoods.
Discussion
In our study of >1.5 million unique visits scheduled during 2 years among a diverse population of pediatric patients, ambulatory care visit volume and completion rates decreased in the early months of the pandemic before quickly returning to prepandemic levels. We also found that preexisting racial, ethnic, and neighborhood-level disparities in ambulatory care visit completion rates generally persisted during the pandemic. The exponential increase in telehealth during the pandemic reduced the disparity in visit completion rates for many populations but did not eliminate disparities completely. These findings underscore the need to address barriers to health care access for certain populations beyond the COVID-19 pandemic.
Black pediatric patients were less likely than patients in other racial and ethnic groups to complete in-person and telehealth visits, and pediatric patients of caregivers whose primary language was not English were less likely than patients of caregivers whose primary language was English to complete telehealth visits before and during the pandemic. These disparities were similar to disparities seen in other pediatric and adult studies.1-4,21-26 Black and Hispanic populations in the United States have faced a long history of systemic racism, originating from foundations in slavery. Structural racism has also permeated the health care system, ranging from mistreatment of Black populations in medical research to racial segregation of hospitals. Furthermore, discrimination and segregation have contributed to increased negative social determinants of health among Black and Hispanic populations and a lack of culturally and/or linguistically competent health care, which persist today and can amplify mistrust and reluctance to engage in health care services.27-29 In addition, telehealth platforms have not adapted quickly to the need for services such as interpreters for populations not proficient in English. Finally, pediatric patients of caregivers whose primary language is not English may prefer in-person visits, as evidenced by the higher in-person visit completion rates among this population as compared with patients whose caregivers’ primary language was English, before and during the pandemic. Understanding cultural reasons for increased attendance to in-person visits (eg, preference for in-person interpreters or dialogue with health care providers) among this group may be important when considering how best to deliver care to this population.
To our knowledge, this is the first study to examine the impact of neighborhood-level sociodemographic factors such as COI and rurality on health care disparities among pediatric patients during the pandemic. In our patient population, pediatric patients from more socioeconomically disadvantaged neighborhoods were less likely than patients from socioeconomically advantaged neighborhoods to complete in-person and telehealth visits before and after the pandemic began. Beyond aspects of the physical environment that shape health outcomes (eg, housing, violence), neighborhoods can determine access to key resources, such as health care, education, and transportation.30,31 Moreover, one’s social environment (eg, norms, relationships, stressors) can influence health care utilization. 32 For example, those living in socioeconomically disadvantaged neighborhoods may have increased psychosocial strain, which can negatively affect an individual’s self-efficacy for engaging in health promotion behaviors.32-34 These barriers disproportionately affect Black and Hispanic populations, who are more likely than other racial and ethnic populations to live in socioeconomically disadvantaged neighborhoods because of redlining and lack of investment in their communities from decades of systemic racism. 35
Finally, pediatric patients from rural versus urban neighborhoods were less likely before and even more so during the pandemic to attend in-person visits, but access to care improved with the surge in telehealth. This finding again highlights the importance of understanding neighborhood-level barriers to health care delivery. Reasons for disparities in health care utilization in rural communities are many, from barriers to health care access (eg, low health literacy, travel time) to lack of local health care infrastructure.36-38 However, studies confirm the potential for telehealth to reduce many of these barriers, including costs to families living in rural areas in terms of travel and time away from school and work to attend visits.39-41
Despite early assumptions that technological advancements would have an equalizing impact on health,42,43 our findings indicate that disparities in visit completion rates that existed before the COVID-19 pandemic persisted even after the expansion of telehealth services. Telehealth completion rates did improve among pediatric patients with caregivers whose primary language was not English and among patients from rural and socioeconomically disadvantaged communities, which decreased but did not eliminate disparities. This finding may be the result of improvements during the pandemic in the delivery of telehealth (eg, initiation of interpreter services, improved technical support) or adaptation of families to the use of internet-based services during the pandemic for everything from health care to work and school. However, the persistence of disparities likely reflects systemic barriers to telehealth use that disproportionately affect socioeconomically marginalized groups, including those with low digital literacy and unequal access to internet-enabled devices and broadband internet. Technology-based health innovations may lead to widening underlying disparities if they are designed without intentional safeguards to promote equitable access, uptake, and effectiveness.44-46 Given that telehealth will continue to play an important role in the delivery of pediatric health care during and beyond the COVID-19 pandemic, additional research is needed to identify inclusive telehealth care models. 47
Limitations
This study had several limitations. First, we could not measure potential differences between subtypes of noncompleted visits (eg, those who left without being seen vs cancellations). Second, the analysis was limited to a single pediatric health care system, which may limit the generalizability of the study to other geographic regions or other telehealth platforms besides the one implemented throughout the health care system. Third, changes in the pandemic context (eg, the availability of COVID-19 vaccinations) may have had further impacts on health care engagement, but because health care utilization and engagement returned quickly to prepandemic levels soon after the pandemic started, we believe that capturing data on the first year of the pandemic was adequate. Finally, we focused on 4 sociodemographic indicators to examine disparities in pediatric health care engagement. While the COI and rural–urban commuting areas are well studied and widely used,18,19 they are limited by their linkage to zip codes rather than census tracts, which encompass smaller and more uniform populations. We also categorized race and ethnicity into broad categories for the purpose of our analysis. Differences may exist among racial and ethnic subgroups that were not explored; the role of these differences and other factors (eg, pediatric patient age and medical complexity) on health care engagement should be explored in future studies.
Conclusion
We found that health care engagement returned to prepandemic levels soon after the onset of the COVID-19 pandemic. The pandemic exacerbated disparities in in-person visit completion rates for pediatric patients from Black and Hispanic populations, socioeconomically disadvantaged neighborhoods, and rural neighborhoods. The increase in telehealth use during the pandemic reduced some disparities, but additional research is needed to understand how to better leverage telehealth for socioeconomically marginalized communities. Our findings underscore the need for policies to invest resources into socioeconomically disadvantaged neighborhoods to overcome barriers to health care access (eg, transportation, education to improve health literacy, broadband services to medically underserved communities, paid leave for health care visits). In addition, health care systems need to continue to improve their delivery of culturally competent care, from training health care providers in cultural humility and responsiveness to combating structural racism within their institutions. This comprehensive approach to improve health care access and delivery on a systems level is needed to reduce disparities in pediatric health care use.
Supplemental Material
sj-docx-1-phr-10.1177_00333549231163527 – Supplemental material for Persistent Disparities in Pediatric Health Care Engagement During the COVID-19 Pandemic
Supplemental material, sj-docx-1-phr-10.1177_00333549231163527 for Persistent Disparities in Pediatric Health Care Engagement During the COVID-19 Pandemic by Thao-Ly T. Phan, Paul T. Enlow, Amanda M. Lewis, Kamyar Arasteh, Aimee K. Hildenbrand, Julia Price, Corinna L. Schultz, Victoria Reynolds, Anne E. Kazak and Melissa A. Alderfer in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ACCEL/Delaware Clinical and Translational Research Program (grant NIGMS U54 GM104941 to T.T.P. and P.T.E.). The National Institute of General Medical Sciences had no role in the design and conduct of the study.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.