
Abstract
Objectives:
Mammography is a screening tool for early detection of breast cancer. Uptake in screening use in states can be influenced by Medicaid coverage and eligibility policies, public health outreach efforts, and the Centers for Disease Control and Prevention–funded National Breast and Cervical Cancer Early Detection Program. We described state-specific mammography use in 2020 and changes as compared with 2012.
Methods:
We estimated the proportion of women aged ≥40 years who reported receiving a mammogram in the past 2 years, by age group, state, and demographic and socioeconomic characteristics, using 2020 Behavioral Risk Factor Surveillance System data. We also compared 2020 state estimates with 2012 estimates.
Results:
The proportion of women aged 50-74 years who received a mammogram in the past 2 years was 78.1% (95% CI, 77.4%-78.8%) in 2020. Across measures of socioeconomic status, mammography use was generally lower among women who did not have health insurance (52.0%; 95% CI, 48.3%-55.6%) than among those who did (79.9%; 95% CI, 79.3%-80.6%) and among those who had a usual source of care (49.4%; 95% CI, 46.1%-52.7%) than among those who did not (81.0%; 95% CI, 80.4%-81.7%). Among women aged 50-74 years, mammography use varied across states, from a low of 65.2% (95% CI, 61.4%-69.0%) in Wyoming to a high of 86.1% (95% CI, 83.8%-88.3%) in Massachusetts. Four states had significant increases in mammography use from 2012 to 2020, and 8 states had significant declines.
Conclusion:
Mammography use varied widely among states. Use of evidence-based interventions tailored to the needs of local populations and communities may help close gaps in the use of mammography.
Keywords
In 2019, a total of 42 281 women died of breast cancer in the United States, making breast cancer the second-most deadly cancer for women. 1 Death rates per 100 000 women in 2020 were 19.1 overall, 19.4 for White women, and 26.4 for Black women. Early detection and treatment can lead to a reduction in the number of deaths from breast cancer. The US Preventive Services Task Force (USPSTF) recommends that women aged 50-74 years undergo biennial mammography to detect breast cancer. 2 Mammography can detect early-stage breast cancer, when it is more amenable to treatment. 2 In 2019, about 3 of 4 US women aged 50-74 years had received a mammogram in the past 2 years, according to self-reported data from the National Health Interview Survey (NHIS). 3 Some physicians may decide not to recommend screening because the potential harms may outweigh the benefits. 4 For example, the gains from early detection and treatment are lower among women with limited life expectancy than among those with longer life expectancy. 5 However, many women do not receive mammograms because they lack health insurance coverage or they do not have a regular source of primary care.6-8
Uptake in screening use in states can be influenced by Medicaid coverage and eligibility policies, public health outreach efforts, and publicly funded screening programs.8-10 Comparisons of mammography use by state may help identify opportunities to increase screening and guide programmatic initiatives to reduce barriers to screening. 11
We described mammography use in 2020 by demographic and socioeconomic groups and by state. We also described differences in state-specific mammography use from 2012 to 2020. These results can be used by decision makers to identify opportunities to increase guideline-concordant mammography use.
Methods
We used data from the 2020 Behavioral Risk Factor Surveillance System (BRFSS) to calculate state-specific mammography use, and we compared prevalence estimates among various groups of women by demographic characteristics and socioeconomic status. The BRFSS is a state-based telephone survey that captures information on the health, health-related behaviors, and health insurance coverage (covered vs not covered) of the US civilian, noninstitutionalized adult population. State-specific response rates to the 2020 BRFSS ranged from 38.8% to 67.2%, with a median of 49.9%. 12 State-specific response rates to the 2012 BRFSS ranged from 27.7% to 60.4%, with a median of 45.2%. 13 In the 2020 survey, all states included questions about whether women aged ≥18 years had ever had a mammogram and the time since most recent mammography. The survey does not differentiate mammograms performed for screening versus diagnosis. We also used the 2012 BRFSS data, which included the same mammography questions in the core survey, to assess changes in mammography use over time. The 2012 and 2020 data are comparable, although rules governing the inclusion of cell-phone respondents changed in the intervening period. 14
We excluded data on women with missing values for age group (n = 4589 in 2020; n = 4580 in 2012), women with missing values for the variable indicating whether they had ever had a mammogram (n = 10 094 in 2020; n = 5819 in 2012), and women who refused to answer the question about how long it had been since they last had a mammogram or women who did not know (n = 2084 in 2020; n = 1979 in 2012). We categorized a respondent as having received a recent mammogram if she reported doing so in the past 2 years in response to the question “How long has it been since you had your last mammogram?” Those whose most recent mammogram was >2 years prior or who had never had a mammogram were considered not to have received a recent mammogram.
We focused on mammography use among women aged 50-74 years, but we also reported prevalence estimates among women aged 40-74, 40-49, and ≥75 years because the USPSTF states that screening among women aged 40-49 years should be an individual decision. The USPSTF concluded that evidence is not sufficient to recommend for or against screening women aged ≥75 years. We weighted all estimates using BRFSS sample weights to produce estimates representative of the noninstitutionalized population and adjusted SEs to account for the complex survey design. We used t tests to determine the significance of differences in screening use in states from 2012 to 2020, with P < .05 considered significant. We conducted the analysis using Stata version 16.0 (StataCorp LLC). The Emory University Institutional Review Board determined that the study did not count as human subjects research because it used only aggregated census data.
Results
The sample (women aged ≥40 y) included 153 803 respondents in 2020 and 217 084 in 2012. The proportion of women aged 50-74 years who received a mammogram in the past 2 years was 78.1% (95% CI, 77.4%-78.8%) in 2020. The proportion of women aged 50-74 years who received a mammogram was highest among non-Hispanic Black women (84.5%; 95% CI, 82.6%-86.4%) and lower among women in all other racial and ethnic groups (range, 70.6%-79.6%) (Table 1). Across measures of socioeconomic status, mammography use generally was lower among women who did not have health insurance (vs did have health insurance) or a usual source of care (vs no usual source of care). The proportion of women aged 50-74 years who received a mammogram was 75.4% (95% CI, 74.2%-76.6%) among those who did not attend college and 82.0% (95% CI, 80.9%-83.0%) among those who graduated from college. Among women aged 50-74 years, 52.0% (95% CI, 48.3%-55.6%) without health insurance and 79.9% (95% CI, 79.3%-80.6%) with health insurance had received a mammogram in the past 2 years.
Mammography use among women aged ≥40 years, by demographic and socioeconomic characteristics, United States, 2020 Behavioral Risk Factor Surveillance System a
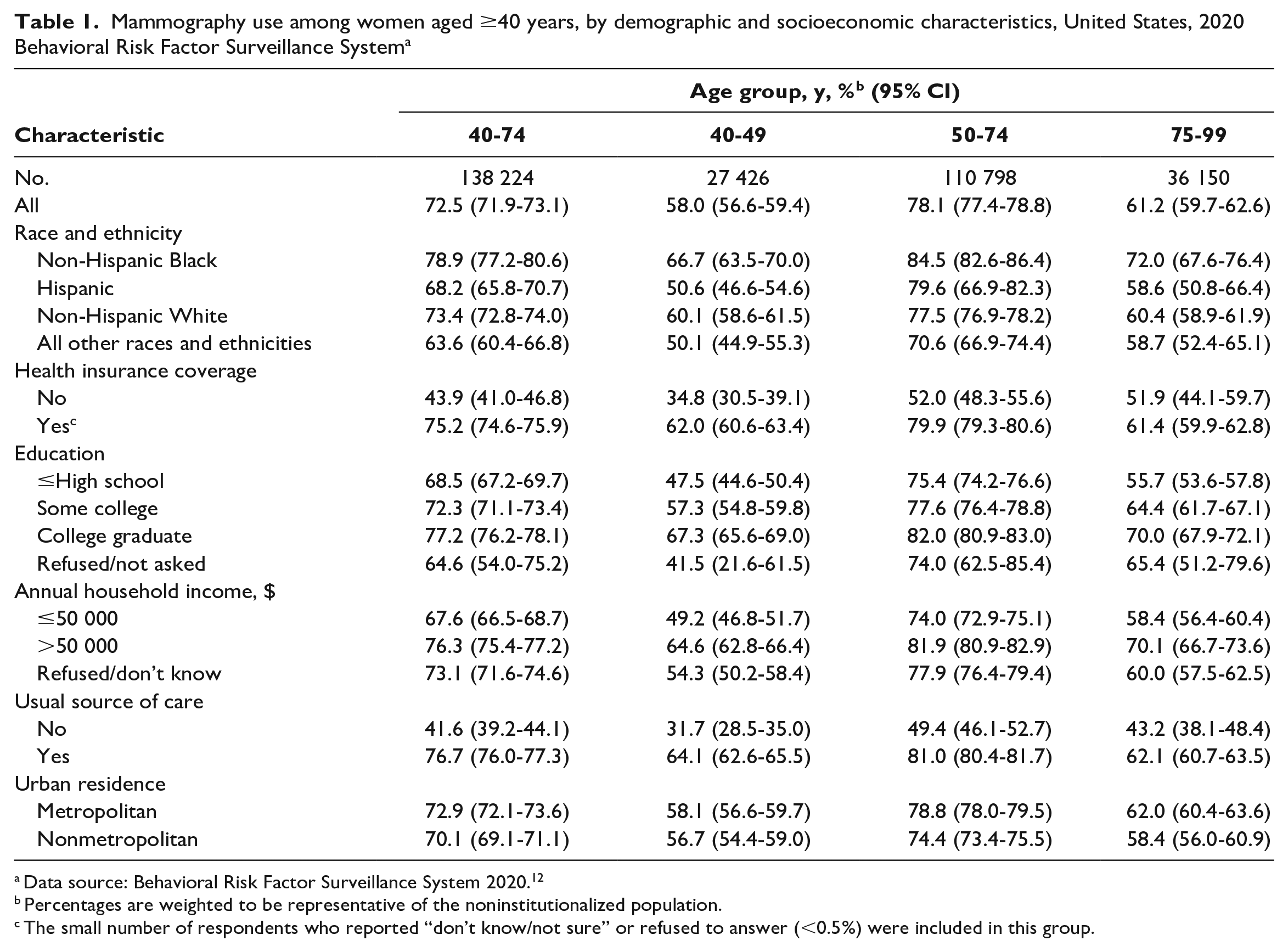
Data source: Behavioral Risk Factor Surveillance System 2020. 12
Percentages are weighted to be representative of the noninstitutionalized population.
The small number of respondents who reported “don’t know/not sure” or refused to answer (<0.5%) were included in this group.
By age, the proportion of women who received a mammogram in the past 2 years was 58.0% (95% CI, 56.6%-59.4%) among those aged 40-49 years, 72.5% (95% CI, 71.9%-73.1%) among those aged 40-74 years, and 61.2% (95% CI, 59.7%-62.6%) among those aged ≥75 years (Table 1).
Mammography use varied across states, from a low of 65.2% (95% CI, 61.4%-69.0%) in Wyoming to a high of 86.1% (95% CI, 83.8%-88.3%) in Massachusetts among women aged 50-74 years (Table 2). Mammography use among women aged 50-74 years was similar in 2012 (77.3%; 95% CI, 77.3%-77.5%) and 2020 (78.1%; 95% CI, 77.4%-78.8%). Four states had significant increases in mammography use from 2012 to 2020 (Arkansas, 7.1% [P = .01]; California, 6.1% [P = .047]; Louisiana, 5.0% [P = .03]; Texas, 5.9% [P = .045]), and 8 states had significant decreases (Delaware, −7.1% [P = .01]; District of Columbia, −6.2% [P = .034]; Georgia, −5.1% [P = .03]; Kansas, −0.8% [P < .001]; Massachusetts, −4.1% [P = .006]; Minnesota, −5.8% [P < .001]; New Hampshire, −8.1% [P < .001]; Vermont, −9.6% [P < .001]) (Figure).
Mammography use among women aged ≥40 years, by state, United States, 2020 Behavioral Risk Factor Surveillance System a
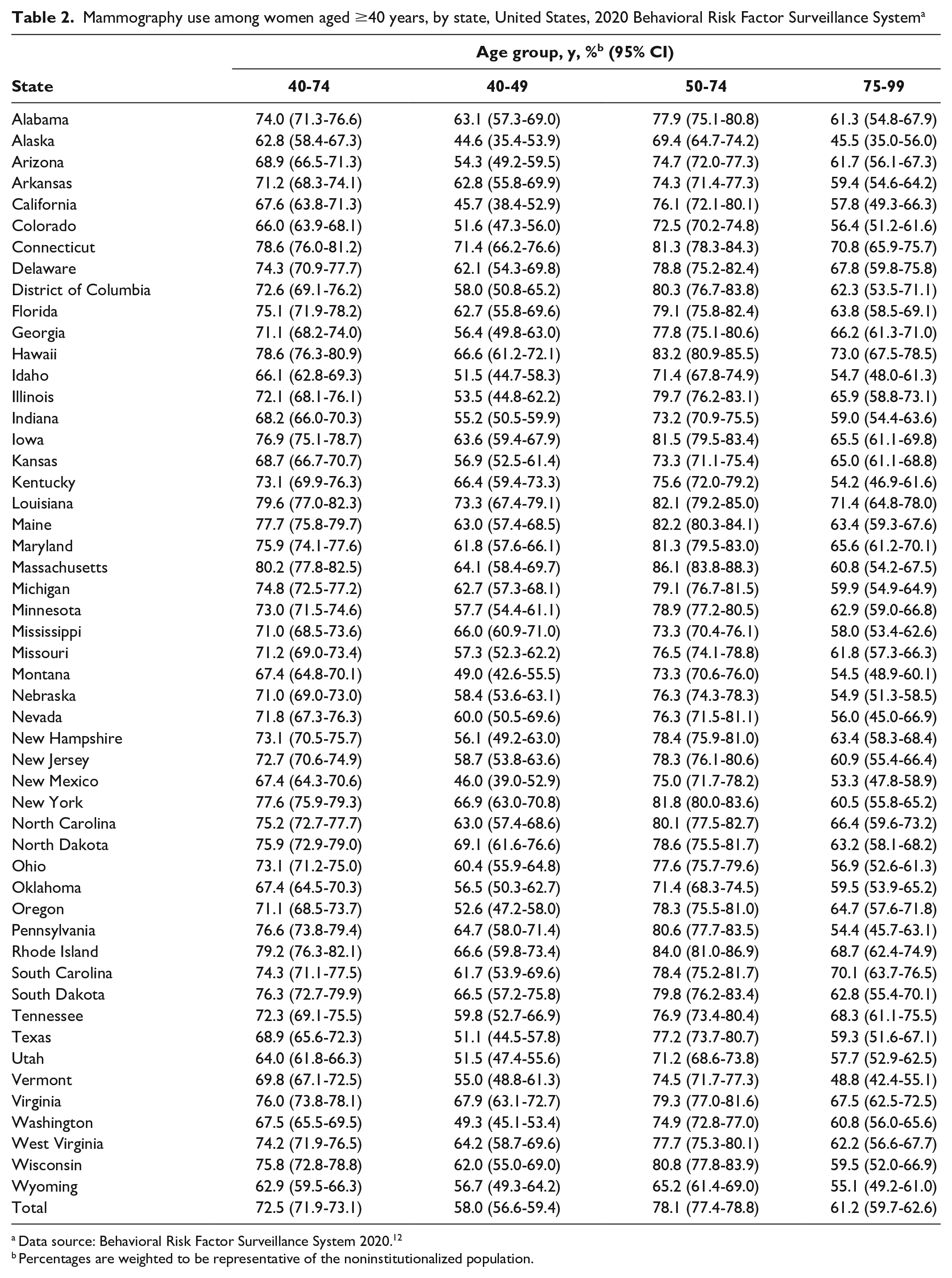
Data source: Behavioral Risk Factor Surveillance System 2020. 12
Percentages are weighted to be representative of the noninstitutionalized population.

Percentage of women aged 50-74 years who received a mammogram in the past 2 years, Behavioral Risk Factor Surveillance System (BRFSS) 2012 and 2020. Percentages were weighted to be representative of the US noninstitutionalized population. The mean percentage was 77.3% in 2012 and 78.1% in 2020. Data source: BRFSS 2012 and 2020. 12
Discussion
Estimates based on BRFSS data suggest that in 2020, 78.1% of women aged 50-74 years had received a mammogram in the past 2 years. The comparable estimate from the 2018 NHIS was 72.4%. 15 Estimates of the proportion of women undergoing mammography based on BRFSS data tend to be higher than estimates based on the NHIS because of differences in survey methodology. 16
BRFSS allows for state-specific estimates, which may help gauge the usefulness of state-level programs to increase screening. Mammography use is below the Healthy People 2030 target of 77.1% in 21 states (including the District of Columbia), 17 suggesting possible opportunities for focused efforts to increase uptake of screening. We found that mammography use among Black women aged 50-74 years was higher than among White women of the same age group; an analysis of NHIS data found that prevalence was similar. 8 However, large gaps in mammography use between women with and without health insurance still exist, consistent with prior work. 7 The National Breast and Cervical Cancer Early Detection Program funds states, territories, and tribal organizations to provide breast and cervical cancer screening and diagnostic services to low-income, uninsured, and underinsured women. 18 In 2017, 2.8 million women met national and state-specific program eligibility thresholds for breast cancer services. 19 Fifteen percent of eligible women were screened for breast cancer through this program. In the absence of screening, women may be more likely to be diagnosed with late-stage disease and have breast cancer–related morbidity and mortality. 2
Mammography use was similar in 2012 and 2020. Thirty-four states expanded Medicaid under the Affordable Care Act (ACA) prior to 2020, 20 and many people became eligible for subsidized Marketplace insurance during this period. 21 Not only was the higher number of individuals with health insurance expected to increase screening uptake, but so were the provisions of the ACA that eliminated cost sharing for many clinical preventive services—including mammography—in Medicare and many private health insurance plans when received in network. 22 Estimates of the impact of the ACA on breast cancer screening vary, but most estimates suggest no effect or only a small effect on uptake of screening among low-income women.23-29 The association between health insurance coverage and mammography use has not changed over time. Using BRFSS data, Miller et al 22 reported a 28.2 percentage-point gap in age-adjusted mammography use between uninsured and insured women aged ≥40 years in 2010. We found a 27.8 percentage-point gap between insured and uninsured women aged 40-64 years in 2020 (estimates were not age adjusted, and BRFSS survey and weighting methods changed in 2011). 30 The lack of change in mammography use during a period that coincided with a large increase in coverage emphasizes the importance of barriers to mammography uptake other than health insurance coverage. 31
Other factors—such as constraints on the supply of primary care physicians, lack of easily accessible mammography facilities, and competing health priorities—may have blunted the impact of coverage expansions on mammography use. 19 The availability of patient navigation and supportive services, such as transportation assistance, translation services, and extended clinic hours for screening, may help increase the number of women who get mammograms.32-34
Limitations
Our study had several limitations. First, our estimates may be biased by differences between respondents and nonrespondents to the BRFSS, although BRFSS weights are adjusted for nonresponse. Respondents may have been more likely than nonrespondents to receive regular mammograms. Second, estimates do not represent actual screening use because the BRFSS survey does not differentiate between screening and diagnostic mammograms. Third, receipt of mammograms is self-reported. Self-reports display high sensitivity (a high proportion of women who were screened report it) but low to moderate specificity (women who were not screened state that they were), 35 and so self-reported measures will tend to overstate mammography use. Fourth, comparison of changes over time may be affected by differences in the age structure or other characteristics of women in the eligible population.
Fifth, the American Cancer Society (ACS) changed its recommendations for screening in 2015. ACS recommended that women be screened beginning at age 45 years instead of age 40 years and that screening be conducted biennially instead of annually starting at age 55 years. The change in recommendations probably affected our results but only modestly. Only one-quarter of physicians list the ACS guidelines as their most trusted source, 36 and prior recommendations that increased the recommended age at which women are first screened for breast cancer had only a small effect. 37
Lastly, the COVID-19 pandemic caused a steep decline in screening mammography volumes in and around April 2020.38-41 However, the declines were short-lived, and volumes had rebounded to near 90% of prepandemic levels by July 2020. 23 We examined mammography use during a 2-year recall period that included 2020. Thus, our prevalence estimates are likely lower than they would have been in the absence of the COVID-19 pandemic.
Conclusions
Our results indicate that in 2020, almost one-quarter of women in the USPSTF–recommended age range did not receive a mammogram in the past 2 years. Most women aged 40-49 and ≥75 years did receive recent mammograms, despite a lack of evidence indicating more than a small net benefit for women in their 40s or that mammograms improve outcomes for women in the older age group. 2 Mammography use varied widely among states. These results highlight the continued opportunities to better align breast cancer screening with recommendations.
Footnotes
Acknowledgements
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support for David H. Howard was provided by the Centers for Disease Control and Prevention (Intergovernmental Personal Act, assignment agreement 16IPA1604432).