
Abstract
Objectives:
Quarantine after exposure to COVID-19 has resulted in substantial loss of in-person learning in schools from prekindergarten through grade 12. Test to Stay (TTS), a strategy that limits the spread of SARS-CoV-2 while prioritizing in-person learning, requires substantial investment in resources. The objective of this study was to assess the perceived benefits, barriers, and facilitators of implementing TTS in an urban school district in the Midwest serving primarily Black or African American people with low income.
Methods:
In December 2021, we used a concurrent mixed-methods approach to understand perceived benefits, barriers, and facilitators of implementing TTS by combining quantitative analysis of telephone surveys conducted with parents (n = 124) and a qualitative inquiry involving key informants from the school district and local health department (n = 22). We analyzed quantitative data using descriptive statistics. We used thematic analysis to analyze qualitative data.
Results:
Quantitative findings showed that parents supported TTS because it was convenient (n = 83, 97%) and effective (n = 82, 95%) in keeping students learning in person (n = 82, 95%) and preventing the spread of COVID-19 (n = 80, 93%). Qualitative interviews with informants found that having a clear protocol and assigning staff to specified tasks allowed for successful TTS implementation. However, insufficient staffing and testing resources, parent mistrust of testing, and lack of communication from schools were perceived barriers.
Conclusion:
The school community strongly supported TTS despite the many implementation challenges faced. This study emphasized the importance of ensuring resources for equitable implementation of COVID-19 prevention strategies and the critical role of communication.
The COVID-19 pandemic has resulted in substantial loss of in-person learning in schools from prekindergarten (pre-K) through grade 12 because of quarantine requirements and school closures. It has highlighted educational disparities that have led to fewer in-person learning days among students in racial and ethnic minority groups. 1 Loss of in-person learning also impacts access to school-based services, including meals and physical and mental health services. 2 Additionally, Black or African American people (hereinafter, Black) and other racial and ethnic minority groups are disproportionately affected by unintended disparities (eg, lack of access to testing) caused by COVID-19 prevention strategies.1,3,4
Test to Stay (TTS) is a prevention strategy that regularly tests asymptomatic people exposed to SARS-CoV-2 and allows them to remain in school if test results are negative. When layered with other prevention strategies, such as wearing face masks, TTS limits the spread of SARS-CoV-2 while maintaining safe in-person learning. 5 While effective, TTS is resource intensive, requiring schools to initiate and complete several activities (eg, contact tracing, frequent testing), which can substantially increase demands placed on school staff.6-8 TTS implementation also requires parental support to have children tested on campus and remain in school after exposure to COVID-19. To further explore the perceived benefits, barriers, and facilitators of implementing TTS, we conducted a concurrent mixed-methods study to assess the perceptions of parents and guardians (hereinafter, parents) and local health department (LHD) and school staff who participated in TTS in a school district serving primarily Black people with low income.
Methods
School District Setting
This assessment was conducted in a school district in the Midwest composed of 1 pre-K school, 5 elementary schools, 2 middle schools, 1 alternative K-8 school, and 1 high school in an urban community in which 99.6% of students met ≥1 of the following indications of low income: receive free or reduced-price meals, live in substitute care (eg, foster care), or have families who receive public aid. 7 The district includes 4462 students, of whom 97% are non-Hispanic Black, 2% are Hispanic, and 1% are non-Hispanic White. 9 This activity was reviewed by the Centers for Disease Control and Prevention (CDC) and was conducted consistent with applicable federal law and CDC policy (eg, 45 CFR part 46, 21 CFR part 56; 42 USC §241(d); 5 USC §552a; 44 USC §3501 et seq). Verbal consent was obtained from participants prior to participation.
In fall 2021, the school district implemented weekly reverse transcriptase polymerase chain reaction screening. Prior to implementing TTS, the school district lacked the additional staff and testing resources needed to implement contact tracing; as such, when individuals received positive test results for COVID-19, everyone in their classroom was considered a close contact, and unvaccinated people were required to undergo traditional quarantine at home for up to 14 days. On October 29, 2021, the school district implemented TTS, allowing asymptomatic close contacts 10 to participate, provided that they were wearing face masks during exposure to a masked person with COVID-19 and were not fully vaccinated. School staff conducted contact tracing, notified parents of close contacts, discussed the option of TTS and traditional quarantine, and obtained consent to enroll in TTS, if eligible. TTS participants were tested by LHD staff using rapid antigen tests on campus on days 1, 3, 5, and 7 after the date of the most recent exposure.
Participants
Among 589 close contacts identified from October 29 through November 20, 2021, 465 (79%) enrolled in TTS and 124 (21%) in traditional quarantine. After we excluded parents with incomplete information, 382 unique parents were identified as eligible for the parent survey. People eligible to participate in the qualitative portion of the study included local school staff (eg, principals, teachers) from 9 schools that reported COVID-19 cases during the study period and the LHD staff who implemented TTS.
Data Collection and Analysis
This study used a concurrent mixed-methods design that comprised a telephone-based survey and key informant interviews to collect data from parents and LHD/school staff.
Parent Surveys
Trained staff used a standardized telephone-based questionnaire developed in REDCap version 12.0.8 (Vanderbilt University) to contact eligible parents and administer surveys (eFigure in Supplemental Material). Parents were called at least twice unless a person refused participation or the telephone number was disconnected or incorrect. The survey took approximately 15 minutes to complete. Respondents were asked about demographic characteristics and awareness, attitudes, and perceptions of the TTS program. Response options were either multiple choice or a 5-point Likert scale (1 = completely disagree, 5 = completely agree). We conducted a descriptive analysis for the parent survey in R version 4.1.2 (R Foundation for Statistical Computing), and results include data from complete (n = 93) and partial (n = 31) interviews to minimize the possibility of response bias.
Informant Interviews
Pairs of trained staff conducted in-person semistructured informant interviews in private rooms; all participants wore face masks. Staff used an interview guide that included questions on perceptions of implementing TTS. Interviews lasted approximately 60 minutes and were digitally recorded and documented through note taking. Interviews were transcribed verbatim and analyzed with Microsoft Word and Excel.
Eight trained coders developed the codebook together using an inductive, grounded theory approach. The coders developed 24 codes based on prominent topics that emerged from the interviews. Pairs of coders then individually coded the same transcript using the codebook. The coders subsequently reviewed their codes together and discussed any coding differences until 100% agreement was attained. 11 This discussion method identified differences in coding and helped to achieve interrater reliability. Rigor in analysis was established by achieving 100% agreement in the application of codes. After this discussion, the coders independently coded the remaining transcripts. The coders used the codes to analyze the data to examine the obstacles, disadvantages, successes, and benefits of implementing TTS.
Results
Parent Survey
Of 382 unique parents who were eligible for the parent survey, 124 (32%) participated. Most (n = 108, 87%) were parents of a child who participated in TTS; the remainder (n = 16, 13%) were parents of children who participated in traditional quarantine. Most parents reported their race as Black (85 of 91, 93%), were employed (69 of 92, 75%), and worked outside the home (64 of 69, 93%). More than half of student close contacts were in pre-K through fifth grade (66 of 122, 54%) (Table 1). Overall, 97% (92 of 95) of responding parents supported the implementation of TTS in their child’s school.
Characteristics of parents or guardians (n = 124) who participated in a telephone survey on the benefits, barriers, and facilitators of implementing a Test to Stay strategy for COVID-19 in a school district in the Midwest serving primarily Black or African American people with low income, December 2021 a
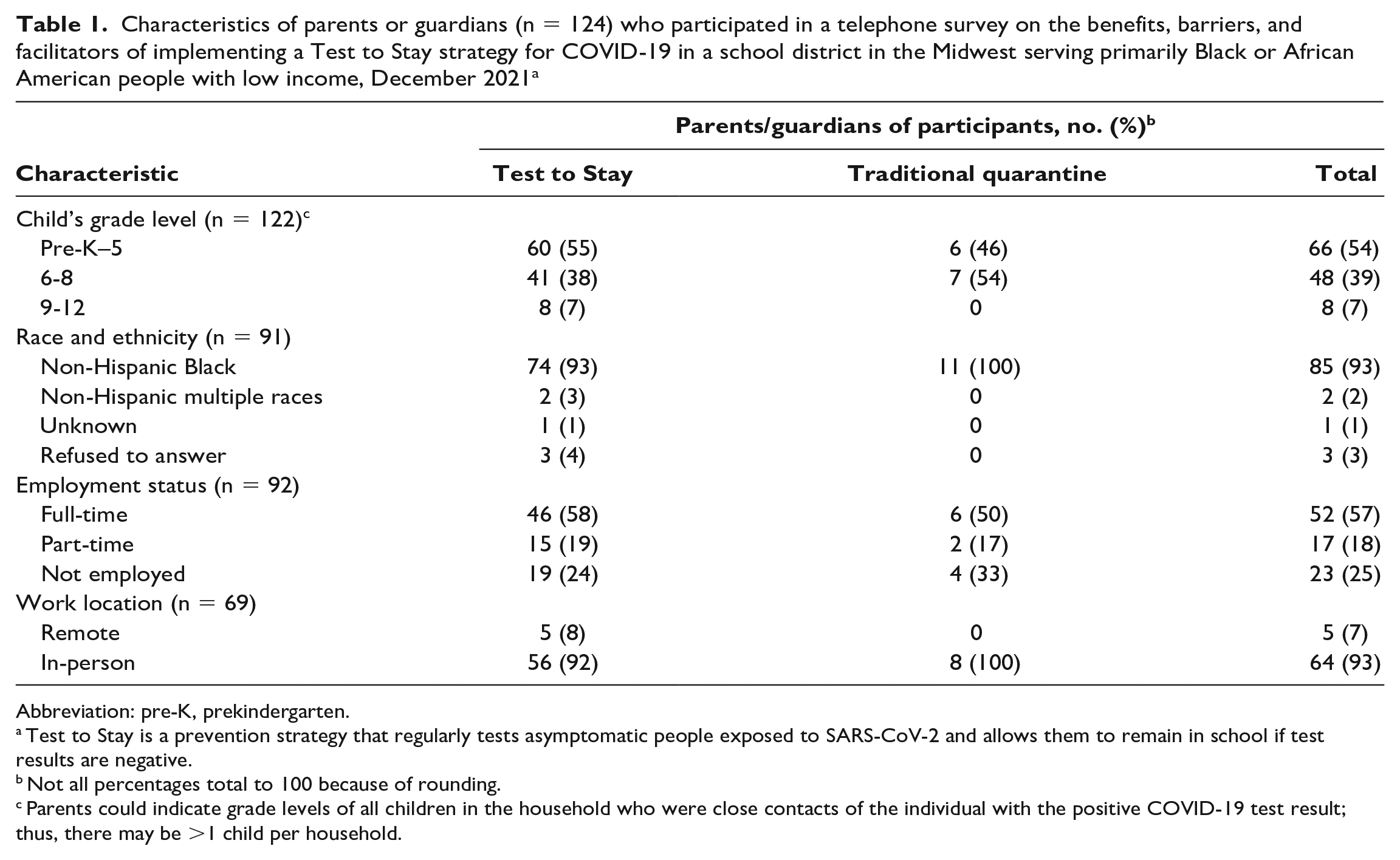
Abbreviation: pre-K, prekindergarten.
Test to Stay is a prevention strategy that regularly tests asymptomatic people exposed to SARS-CoV-2 and allows them to remain in school if test results are negative.
Not all percentages total to 100 because of rounding.
Parents could indicate grade levels of all children in the household who were close contacts of the individual with the positive COVID-19 test result; thus, there may be >1 child per household.
Benefits of TTS
Of 86 parents who completed the Likert-scale questions, most “completely agreed” or “somewhat agreed” that TTS was a convenient (n = 83, 97%) and effective (n = 82, 95%) way to keep students learning in person (n = 82, 95%) and prevent the spread of COVID-19 (n = 80, 93%) (Figure).
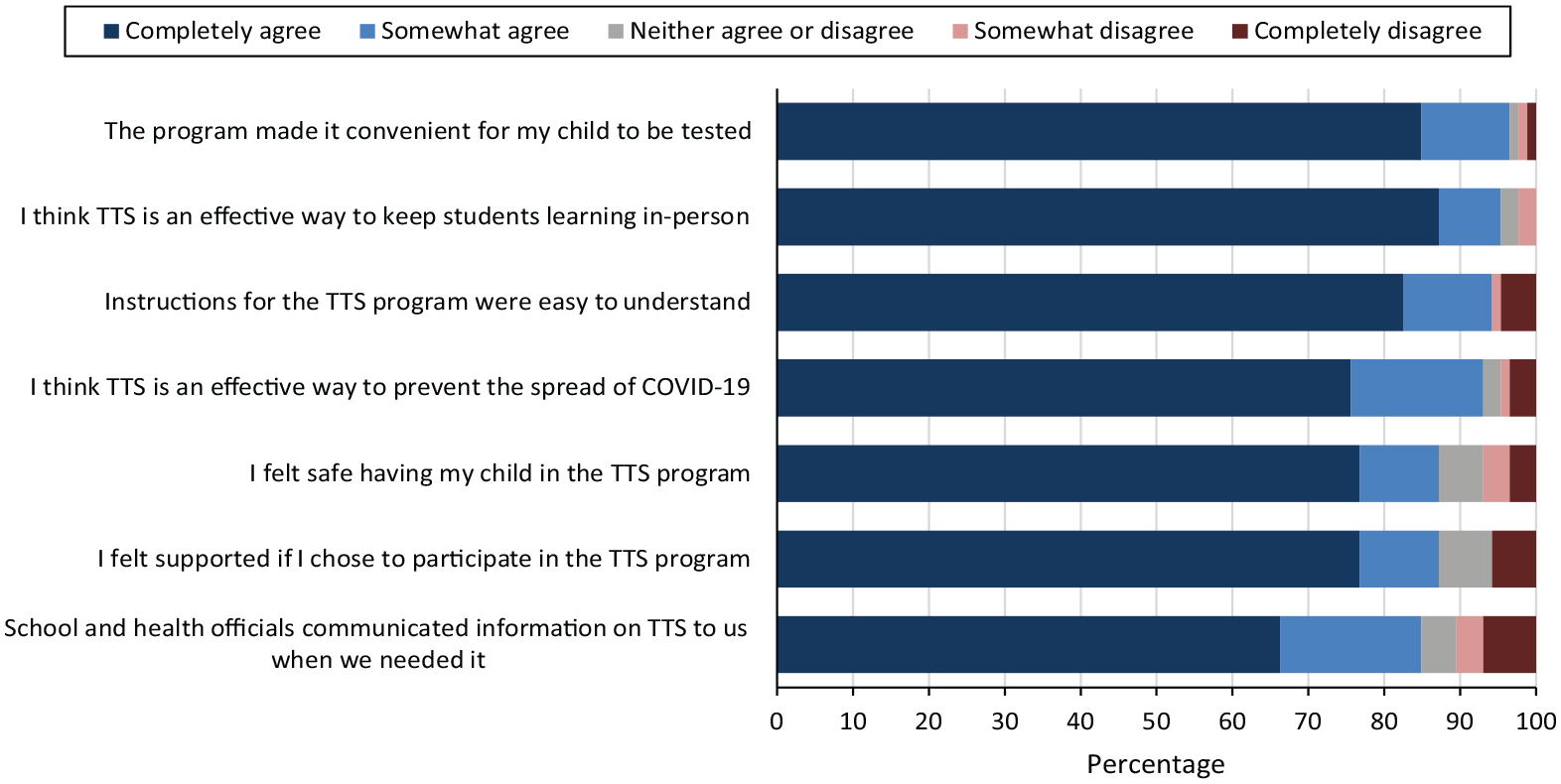
Parent/guardian attitudes toward and perceptions of a Test to Stay (TTS) program for COVID-19 in a school district in the Midwest serving primarily Black or African American people with low income, December 2021. Eighty-six parents/guardians responded to the telephone survey. Test to Stay is a prevention strategy that regularly tests asymptomatic people exposed to SARS-CoV-2 and allows them to remain in school if test results are negative.
Barriers to TTS
The 2 most common reasons for not participating in TTS (n = 15) were that parents did not want their child to get tested (n = 5) and were unaware of the TTS option or reported that their child was ineligible (n = 3). Moreover, 17% (16 of 96) of parents whose children participated in TTS were unaware of their participation.
Facilitators of TTS
Among parents whose children participated in TTS (n = 87), the most common reasons for participation were keeping children and families safe (n = 31, 36%), keeping children in school (n = 26, 30%), and providing the opportunity for children to be tested (n = 13, 15%).
Informant Interviews
Twenty-two informants were interviewed to assess the benefits, barriers, and facilitators of TTS. Informants consisted of 7 pre-K or elementary school principals, 3 middle school or senior high school principals or assistant principals, 3 elementary school teachers and 1 elementary school nurse, 2 middle school teachers and 1 middle school nurse, and 3 administrators/nurses and 2 contact tracers from the LHD.
Benefits of TTS
Most informants indicated that TTS was beneficial by allowing students to remain safely in school and preventing teachers from worrying about working in an unsafe environment (Table 2). Informants stated that students benefited by staying in school, which allowed them to socialize, participate in extracurricular activities, and receive free or reduced-price school lunch programs. One contact tracer from the LHD said the following:
Themes from key informant interviews on perceptions of benefits, barriers, and facilitators of TTS program implementation during COVID-19 in a school district in the Midwest serving primarily Black or African American people with low income, December 2021 a
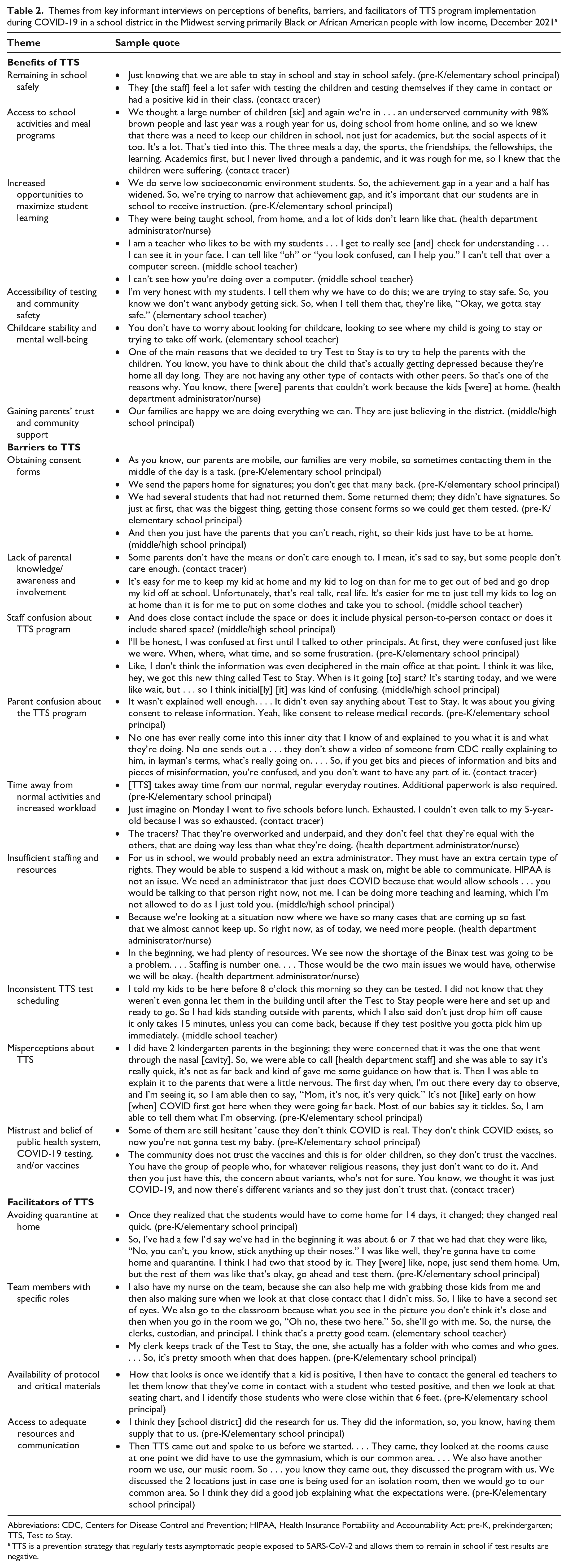
Abbreviations: CDC, Centers for Disease Control and Prevention; HIPAA, Health Insurance Portability and Accountability Act; pre-K, prekindergarten; TTS, Test to Stay.
TTS is a prevention strategy that regularly tests asymptomatic people exposed to SARS-CoV-2 and allows them to remain in school if test results are negative.
We’re an underserved community with 98% brown people and last year was a rough year for us, doing school from home online, and so we knew that there was a need to keep our children in school, not just for academics, but the social aspects of it too . . . the three meals a day, the sports, the friendships, the fellowships, the learning.
TTS helped students maximize instructional hours at school. In-class learning allowed teachers to identify students who were struggling and assist them in real time. TTS also provided an opportunity for increased testing to help identify asymptomatic and presymptomatic students with COVID-19. Principals, nurses, teachers, and LHD contact tracers agreed that safety was one of the main benefits of TTS and that routinely testing children helped protect older adults and others in households (Table 2).
Another benefit of TTS was that parents did not have to worry about finding alternate means of childcare or having to take time off from work (Table 2). One elementary school teacher said, “You don’t have to worry about looking for childcare . . . looking to see where my child is going to stay or trying to take off work.” Furthermore, attendance at school can help prevent depression caused by lack of contact with peers. One administrator/nurse noted, “You have to think about the child that’s actually getting depressed because they’re home all day long. They are not having any other type of contacts with other peers.”
TTS also helped to garner support from the community and support for the school system (Table 2). A high school principal/assistant principal said, “I think people who didn’t have the trust in us before the pandemic have seen how the district handled COVID-19 versus the rest of the world and really fell in love with us.”
Barriers to TTS
Informants noted several barriers to TTS. One barrier to implementing TTS in schools was the difficulty that staff encountered in obtaining parental consent. Communication barriers, such as disconnected telephone numbers or unavailability, frequently made it difficult to reach parents. Another barrier was the lack of parental knowledge, awareness, and involvement. A middle school teacher stated, “The kids who have not participated or did not participate in TTS, I believe it’s because the parents are not knowledgeable, not made aware, or saying they’re not made aware.” In some cases, parental confusion may have resulted from schools’ lack of clear communication about TTS (Table 2). One pre-K/elementary school principal said, “It wasn’t explained well enough. . . . It didn’t even say anything about Test to Stay. It was about you giving consent to release information. Yeah, like consent to release medical records.”
Staff members noted several barriers to TTS. One barrier was staff confusion about TTS programs. Some school and LHD staff did not initially understand how to implement TTS. Specifically, they reported confusion about the protocol and the definition of “close contact.” Additionally, all principals agreed that TTS increased administrative tasks. The testing schedules and associated paperwork, in addition to regular teaching responsibilities, resulted in teachers reporting increased stress and exhaustion. TTS also required a heavy workload for LHD staff, who struggled to keep up with TTS testing demands. Staff indicated that another barrier was a lack of sufficient staff and resources available to efficiently implement TTS. LHD staff expressed concern about the shortage of testing kits, lack of financial compensation for the additional hours of work that TTS required, and cost of using personal vehicles to travel to schools daily.
An inconsistent TTS testing schedule was a barrier for TTS participants and staff. TTS participants had to wait in a testing area to obtain negative test results prior to attending class. The testing schedule changed frequently because of LHD staff capacity and availability; thus, school staff had to accommodate changing schedules in an effort to return students to their classrooms as quickly as possible.
Parent misperceptions about TTS led to a reluctance to have their children tested. For example, some parents thought that children would be hurt by the swab going too far up the nasal cavity and causing damage, and principals worried about the trauma to students who were constantly tested. One high school principal/assistant principal said, “You putting things into his nose . . . I can’t do that to my kids. I’m a parent. That hurt me.” Some parents feared that the nasal swab would give their children COVID-19. A pre-K/elementary school principal said, “A lot of the people . . . in the community, especially when the testing first came, felt like that you could possibly get COVID from them swabbing your nose with this thing, so they were anti–COVID testing.” Some parents thought that the school was collecting children’s DNA and did not want to consent. A pre-K/elementary school principal stated, “They [parents] don’t know if we’re collecting DNA or what we are doing.”
Some informants mentioned that parents were hesitant to have their children participate in TTS because of disbelief in COVID-19 and mistrust of testing and vaccines. A pre-K/elementary school principal said, “They don’t think COVID exists, so now you’re not gonna test my baby” (Table 2). Another pre-K/elementary school principal said, “We do have some that don’t believe in the shots.”
Facilitators of TTS
Many parents who initially did not allow their children to be tested at school eventually agreed to TTS participation once they learned that it would prevent their children from having to quarantine at home. Informants indicated how helpful or essential it was to have TTS staff assigned to designated roles, which appeared to ease the burden of 1 person occupying many roles. School administrators also recommended that each school assign TTS duties to a designated administrator to oversee classroom contact tracing, logistics, and communication.
Informants noted that another facilitator of TTS was having the protocol and supporting materials in an easily accessible location, which allowed TTS to run smoothly. Seating charts were critical for those conducting contact tracing. Several informants also expressed that having access to adequate resources and good communication among TTS team members facilitated the program and made it simpler. A pre-K/elementary school principal said, “Our board provided pretty much everything for us.”
An explanation of the TTS procedure to parents by a well-respected principal rather than a written document had the potential to positively impact participation. One elementary school nurse observed, “One out of ten would say no until they talked to the principal, and she let them understand.”
Discussion
We obtained a holistic understanding of the benefits, barriers, and facilitators associated with implementing or participating in TTS in a school district serving primarily Black people with low income. Overall, parents and informants supported TTS despite the barriers. Because of their understanding of the benefits of TTS, the school community was able to overcome many of these barriers and identify facilitators to effectively implement the program.
All informants agreed that safety was one of the main benefits of TTS, and the most common reason for parents to allow their children to participate in TTS was to keep their children and families safe through increased access to testing. This benefit may be particularly valuable among Black people, whose limited access to COVID-19 testing has been documented throughout the pandemic. 3 Parents also supported TTS because it allowed their children to remain in school, which in turn enabled parents to go to work.11-13 Informants highlighted the health and social benefits of having students attend school in person, including having access to free or reduced-price meal programs, school services, and extracurricular activities, which are especially beneficial among communities that may not have access to these services outside the school setting.11,12,14
Despite these benefits, some challenges were associated with the school district’s implementation of TTS. Although the survey found high levels of parental support, informants reported challenges obtaining consent to participate in TTS. This challenge may have been exacerbated by confusion and unclear communication about TTS, which was reported by parents and informants. Almost one-fifth of parents whose children participated in TTS were unaware of the participation even though they had given consent, which was required to participate. Parents may have confused the weekly screening testing (reverse transcriptase polymerase chain reaction) with TTS testing, and clearer communication and information are necessary moving forward. Another barrier in this community was mistrust of public health measures used to prevent COVID-19, including testing and vaccination, which may have been caused by historical and current experiences of discrimination and inequities among Black people and people in other racial and ethnic minority groups in the United States. 15 Vaccine hesitancy can lead to further inequities in access to in-person learning because fully vaccinated people did not need to quarantine after exposure. Despite the mistrust and misperceptions reported, most parents whom we interviewed chose to enroll their children in TTS.
A major facilitator of TTS reported by parents and informants was to avoid loss of in-person school days. Throughout the pandemic, racial and ethnic minority students were more likely to have received virtual learning than their non-Hispanic White counterparts, negatively impacting the learning and emotional well-being of parents and children.1,16-18 Informants also stated that adequate resources (eg, protocols, searching charts) were additional facilitators to the success of TTS. While schools faced insufficient staffing and resources to implement TTS, they were able to succeed because of their sheer determination to allow students to remain safely in school after exposure.
Limitations
This study had at least 3 limitations. First, the 32% survey response rate was low and may not fully represent the district’s parent population. Second, self-report bias and social desirability bias may have occurred among parent survey participants. Third, interviews were conducted in just 1 school district that implemented TTS; as such, results may not be generalizable to other districts with different levels of staffing and testing resources. Further studies that use larger sample sizes might help to generalize the findings in similar school districts.
Conclusion
This study revealed that parents and informants in a school district serving primarily Black people with low income supported TTS despite facing substantial challenges in implementing a school-based public health prevention program. School-based public health initiatives may use our findings to anticipate barriers and strengthen their programs accordingly and to carefully plan and assess resources that address the logistics, communication, and staffing issues involved, particularly when addressing racial and ethnic minority groups and families with low income.
Supplemental Material
sj-docx-1-phr-10.1177_00333549231155472 – Supplemental material for Perceived Benefits and Barriers of a COVID-19 Test to Stay Program in a School District Serving Black or African American People With Low Income, December 2021
Supplemental material, sj-docx-1-phr-10.1177_00333549231155472 for Perceived Benefits and Barriers of a COVID-19 Test to Stay Program in a School District Serving Black or African American People With Low Income, December 2021 by Emiko Kamitani, Emily J. Holman, David Philpott, Vidisha D. Parasram, Laird J. Ruth, Chisom Onyeuku, Brittani Carter, Eugenia Gwynn, Timothy W. Beck, Kelly Regan, LaVerne R. Hagler, Angela Clark, Gene Shelley and Ebony S. Thomas in Public Health Reports
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.