
Abstract
Objective:
Organizational health equity capacity assessments (OCAs) provide a valuable starting point to understand and strengthen an organization’s readiness and capacity for health equity. We conducted a scoping review to identify and characterize existing OCAs.
Methods:
We searched the PubMed, Embase, and Cochrane databases and practitioner websites to identify peer-reviewed and gray literature articles and tools that measure or assess health equity–related capacity in public health organizations. Seventeen OCAs met the inclusion criteria. We organized primary OCA characteristics and implementation evidence and described them thematically according to key categories.
Results:
All identified OCAs assessed organizational readiness or capacity for health equity, and many aimed to guide health equity capacity development. The OCAs differed in regard to thematic focus, structure, and intended audience. Implementation evidence was limited.
Conclusions:
By providing a synthesis of OCAs, these findings can assist public health organizations in selecting and implementing OCAs to assess, strengthen, and monitor their internal organizational capacity for health equity. This synthesis also fills a knowledge gap for those who may be considering developing similar tools in the future.
Keywords
States, counties, cities, and towns across the United States are increasingly identifying racism as a public health crisis, often declaring their corresponding intent to promote equity-oriented approaches in their public health policies and programs. 1 Health inequities are systematic health disparities between groups with different levels of social power 2 ; differences in health outcomes are inequitable when they are unnecessary, avoidable, unfair, and unjust. 3 The COVID-19 pandemic has highlighted the “longstanding inequities that have systematically undermined the physical, social, economic, and emotional health of racial and ethnic minority populations and other population groups that are bearing a disproportionate burden of COVID-19.” 4 In addition to race and ethnicity, demographic characteristics such as gender, sexual identity and orientation, geographic location, disability, and other factors influence health inequities in the United States. 5 Public health organizations play a key role in achieving health equity.6,7 Public health equity work must be explicitly incorporated, prioritized, and resourced. Building the health equity capacity of public health departments can improve their ability to develop, implement, and sustain equity-centered work. 8
The Public Health National Center for Innovations defines health equity organizational competence as the “ability to strategically coordinate health equity programming through a high level, strategic vision and/or subject matter expertise which can lead and act as a resource to support such work across the department.” 9 Internal-facing capacity strategies, on topics such as organizational culture, readiness for change, policy development and program-planning processes, organizational infrastructure, staff training, and others,10,11 are central to transforming health equity–oriented public health practice. 12 Previous articles have identified the need to focus on organizational factors in public health and health care organizations to reduce disparities, 13 yet most inequity reduction frameworks lack guidelines on internal organizational assessments and do not “provide guidance on translation of equity across multiple organizational departments and levels.” 14 Organizational health equity capacity assessments (OCAs) are increasingly used by public health organizations to assess and improve their capacities to improve equity.15,16 These assessments can serve as the foundation for organizational capacity for health equity action. Currently, however, OCAs can be challenging to locate, have varied structure and content, and have limited implementation evidence. These issues can hinder OCA uptake.
OCAs can be particularly useful for state health departments, county health departments, and local health departments (LHDs). A scan of government public health capacity recommended that health departments develop internal infrastructure to advance equity, 17 and equity is now 1 of the 8 foundational capabilities described in the Foundational Public Health Services framework. 18 LHDs, for example, are well positioned to address health equity disparities locally 19 but must have “an understanding of health equity, have the means to realize facilitators of health equity work, and recognize the complex context in which health equity work exists.” 20 The OCA implementation process provides a foundation for understanding current equity capacity and where there is room for growth. In a 2019 survey 21 evaluating the Health Equity Guide 22 —a platform that provides strategic practices and case studies to help health departments advance health equity—86% (54 of 63) of respondents from state health departments and 73% (161 of 220) of respondents from LHDs reported that they were working to build organizational capacity to advance health equity and that guidance on which practices to consider or which organizational assessment to use would be useful. In the Public Health Accreditation Board’s Standards and Measures Version 2022, health equity is emphasized across every domain. 23 OCAs have the potential to help organizations progress and monitor change along the 4 stages of transformation described by the Public Health Accreditation Board toward committed equity-centered work—moving from the status quo to committed, active, equity-centered work. 24
This scoping review responds to the research question “How can we characterize existing organizational health equity capacity assessment tools for public health organizations?” We were unable to identify any systematic reviews that answer this question by collating and synthesizing information about extant OCAs. Practitioners must conduct individual searches to identify and compare available OCAs. This scoping review synthesizes and characterizes the OCAs in the gray and peer-reviewed literature, providing a baseline for researchers and practitioners searching for and selecting among the tools that have been developed to assess or review organizational health equity capacity. This scoping review can serve as a precursor to a future systematic review on this topic.
Objective
We conducted a scoping review to identify and characterize existing OCAs. Scoping reviews provide an overview of the evidence related to a particular concept—in this case, an overview of existing OCA tools to explore commonalities or key characteristics among these assessments. 25 We conducted a search among the peer-reviewed and gray literature to identify as many OCAs as possible, with the objective of understanding similarities, differences, and key characteristics of each.
Methods
Our methods were based on the 6-stage standard scoping study framework proposed by Arksey and O’Malley, which included identifying the research question and relevant studies, selecting studies, charting the data, collating and summarizing the results, and validating the findings with practitioners. 26
Eligibility Criteria
Inclusion criteria were OCAs published in peer-reviewed or gray literature and in the English language, with no restrictions on geographic origin or publication year. Articles, reports, and tools had to measure or assess the development of the health equity–related capacity of any public health organization. Organizational health equity capacity could be described by using terms such as health inequities, inequalities, and/or disparities. We did not restrict the structure of the OCAs.
We excluded sources if they did not address organizational-level capacity related to health equity or did not include any measurement or assessment of such capacity. We excluded 147 articles for not meeting multiple inclusion criteria; for example, we excluded some articles for not focusing on capacity building and for not including relevant assessment tools or approaches. It was not sufficient to describe other aspects of health equity work (eg, the measurement of inequities or the implementation of equity-oriented policies and programs) without an approach to assessing health equity capacity building at the organizational level.
Information Sources
We conducted the search in the PubMed, Embase, and Cochrane databases. Using a strategy of snowball and purposive sampling, 26 we identified practitioner literature via the following practitioner websites and resources: the Health Equity Guide, the National Association of County and City Health Officials (NACCHO) Toolbox, the Racial Equity Tools website, Government Alliance on Race and Equity Toolkit, the Minnesota Department of Health’s Health Equity Resources list, and the Bay Area Equity Atlas. We hand searched reference lists.
Search Strategy
We developed and used a 3-step search strategy to be as comprehensive as possible within the constraints of time and resources. 27 A search in PubMed and Embase used preliminary limited keywords to elicit potentially relevant articles. We reviewed the titles, abstracts, and keywords of these initial articles to develop a comprehensive list of keywords. We also compiled search terms with the help of partners at NACCHO and Human Impact Partners. We engaged with NACCHO and Human Impact Partners on search terms because of our knowledge of their ongoing work and expertise in the development of organizational health equity capacity. We then conducted a second search using all identified keywords and corresponding MeSH (Medical Subject Headings) and Emtree terms using the following databases: PubMed (on December 30, 2021), Embase (on January 15, 2022), and Cochrane (on January 15, 2022) (Box). As a quality control measure, we confirmed that preidentified relevant preliminary citations were identified through the full searches. After selecting sources for inclusion, we examined these reference lists to identify additional potential sources.
Final PubMed search string for articles related to organizational health equity capacity assessments, December 30, 2021
To identify relevant OCAs in the gray literature, we searched the previously described websites and common databases. We applied the same inclusion and exclusion criteria. We recognized that we had reached saturation when citation searching and reviews of practitioner resources consistently referenced the same OCAs. We deduplicated results across the peer and gray literature databases. Once we made final inclusion decisions, we searched again for each tool by name to capture examples of implementation. We also contacted the owner of every tool by email to request additional information on where and how OCAs had been implemented. Most owners did not respond; those who replied did not track information beyond what was available publicly. One organization indicated anecdotal awareness of some uses but did not share further information.
Selection of Sources of Evidence
For the published literature, we based the first round of source selection on title and abstract examination and the second round on full-text review. We performed source selection based on the inclusion and exclusion criteria. One author (R.M.) reviewed all articles at both stages. A second author (N.M.N.) reviewed a subset of articles at the full-text stage to reach consensus on articles that were included for data extraction. Both authors reviewed all articles that were included in the final review. For the gray literature, 1 author (R.M.) conducted the initial search and screening, and both authors (R.M., N.M.N.) reviewed the findings to reach consensus on which sources to include. For gray and published literature, a third author (K.M.P.P.) provided oversight of the process and reviewed a subset of full-text articles and tools to ensure consensus among all authors. Final articles from the peer-reviewed literature were deduplicated in EndNote and uploaded into Covidence for extraction. We extracted data from the gray literature into a Microsoft Excel spreadsheet with the same categories as the Covidence template.
Data-Charting Process and Data Items
The analysis phase of the scoping review involved charting the extra data in Excel to sort through and synthesize qualitative material according to key issues and themes and to capture a set of predefined characteristics of the identified OCAs. One author (R.M.) conducted the initial data extraction, and a second author (N.M.N.) reviewed the data to reach consensus on the extraction. For each OCA, we captured and summarized the following information: aims, structure or methods, themes, intended audience (if any), and definition of health equity capacity (if included). Where possible, we documented suggestions for implementation, such as resources required, or examples of implementation (geographic location, population served, capacity findings/results, or other implementation information). Charted data for each source of evidence are also available (eTable in the Supplement). Aligned with long-standing guidance for scoping reviews,26,28 we did not consider the quality of the assessments and tools.
Synthesis of Results
We organized and described the findings thematically according to the previously described categories (ie, aim, structure or methods, themes, audience, and definitions). The analysis and presentation of findings align with the PRISMA for scoping reviews (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 29
Results
Selection of Sources of Evidence
The PRISMA flow diagram details the number of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at the full-text stage (Figure).
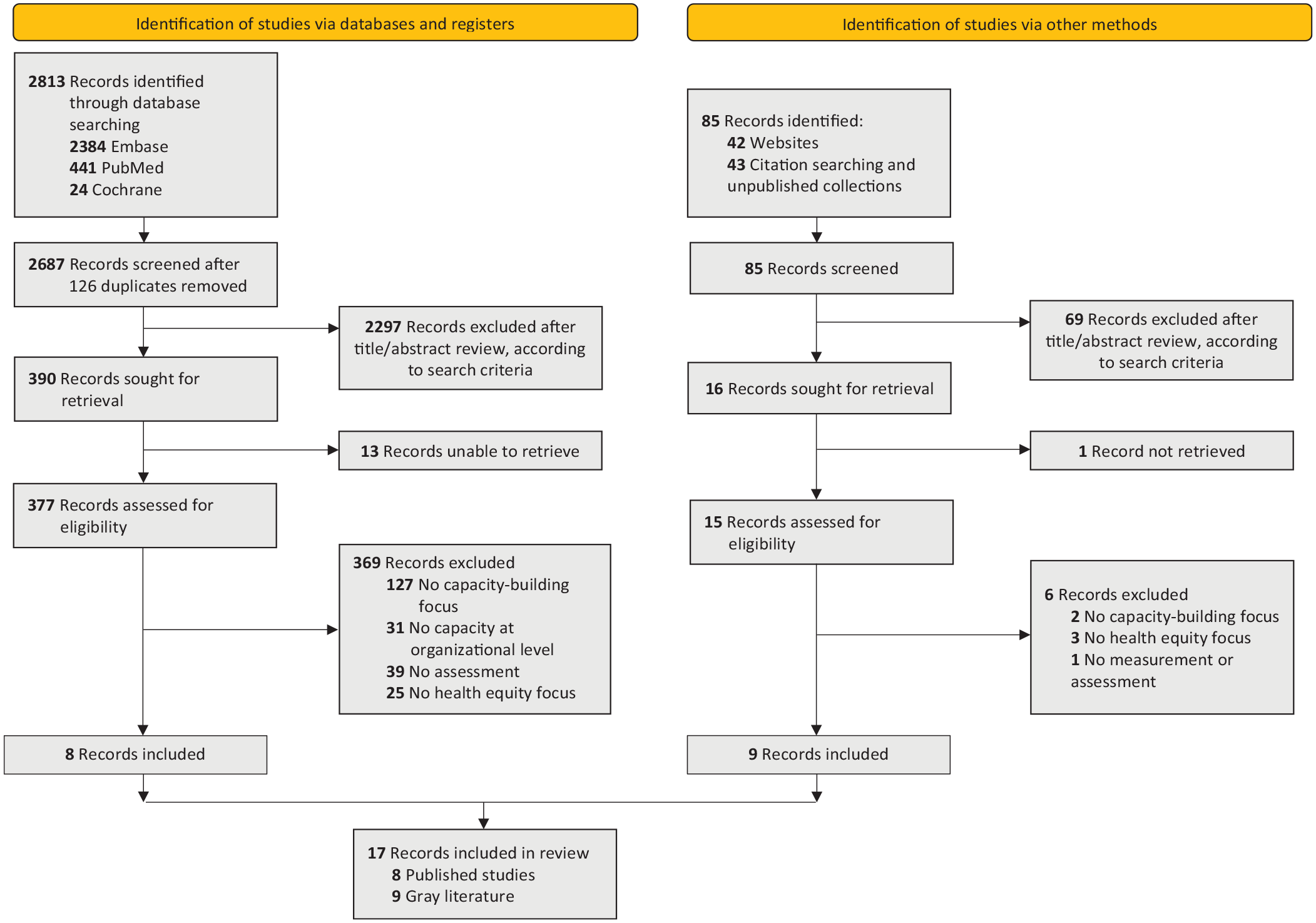
PRISMA flow diagram (Preferred Reporting Items for Systematic Reviews and Meta-analyses) illustrating the results of a search conducted in January–February 2022 for organizational health equity capacity assessments.
Characteristics of Sources of Evidence
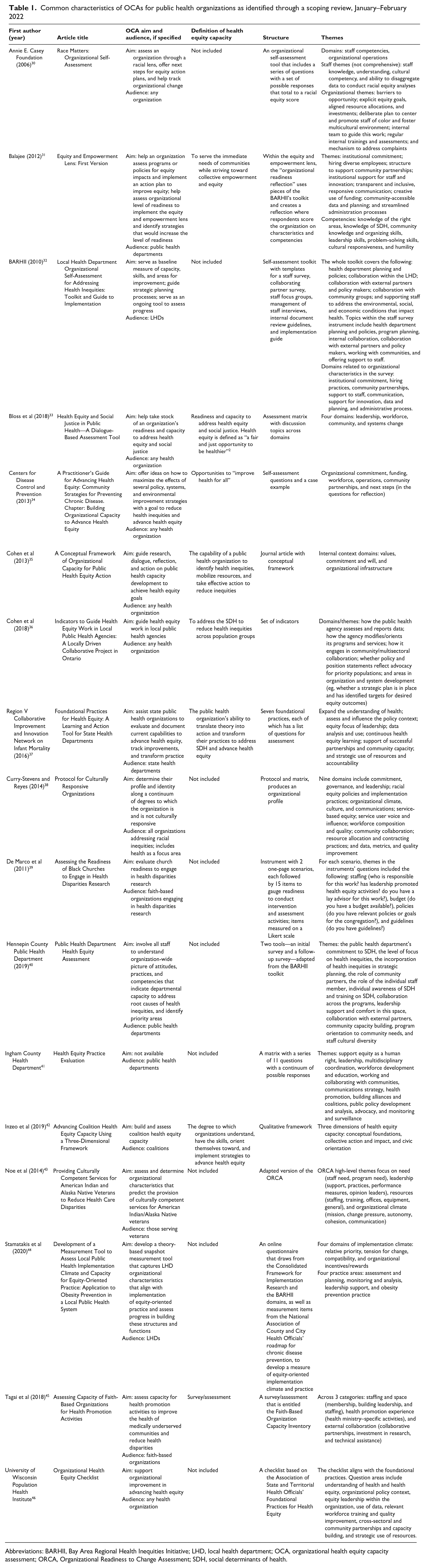
We found consistency across major themes. All OCAs assessed equity-oriented internal capacities, such as institutional leadership and governance, policies and guidelines, budget alignment and resource allocation, commitment and shared visions, internal structures, use of data, staff training and support, and/or staff diversity. However, each OCA differed in which themes were included and how they were described (Table 1). The level of detail ranges from 3 to 9 overarching domains per tool. Most but not all include measures or indicators aligned with each domain or subdomain. Some OCAs distinguished between individual staff competencies and organizational competencies, while other OCAs assessed staff competencies holistically as part of the organization’s workforce measurement. Some OCAs included measures related to external-facing capacity, such as the strength of collaboration with community partners, noting that external and internal capacity can be intertwined and that evaluating the internal capacity component requires awareness of the external enabling environment. 35 An organization exploring OCA implementation must review OCA content to ensure that the focal areas and approach will align with organizational needs.
Common characteristics of OCAs for public health organizations as identified through a scoping review, January–February 2022
Abbreviations: BARHII, Bay Area Regional Health Inequities Initiative; LHD, local health department; OCA, organizational health equity capacity assessment; ORCA, Organizational Readiness to Change Assessment; SDH, social determinants of health.
The OCAs ranged widely in publication dates (from 2006 to 2020), place of origin, and intended audience. We identified implementation case examples or published studies (Table 2) in the following geographic locations: Maricopa County, Arizona; Prince George’s County and Baltimore City, Maryland; Ingham County, Michigan; Hennepin County (Minneapolis) and Rice County, Minnesota; Missouri; North Carolina; Multnomah County, Oregon; Harris County, Texas; Kenosha County, Wisconsin; the Veterans Integrated Service Networks in the US Western Region; Ontario, Canada; local and regional health units in 7 Canadian provinces; and Australia. Six OCAs were intended for any public health organization.30,33,35,38,46 Three OCAs were intended for LHDs32,36,44; 3 for any type of public health department but with implementation information only at the county level31,40,41; 1 for state health departments 37 ; 2 for faith-based organizations, specifically churches39,45; 1 for the US Department of Veterans Affairs service networks 43 ; and 1 for public health coalitions. 42
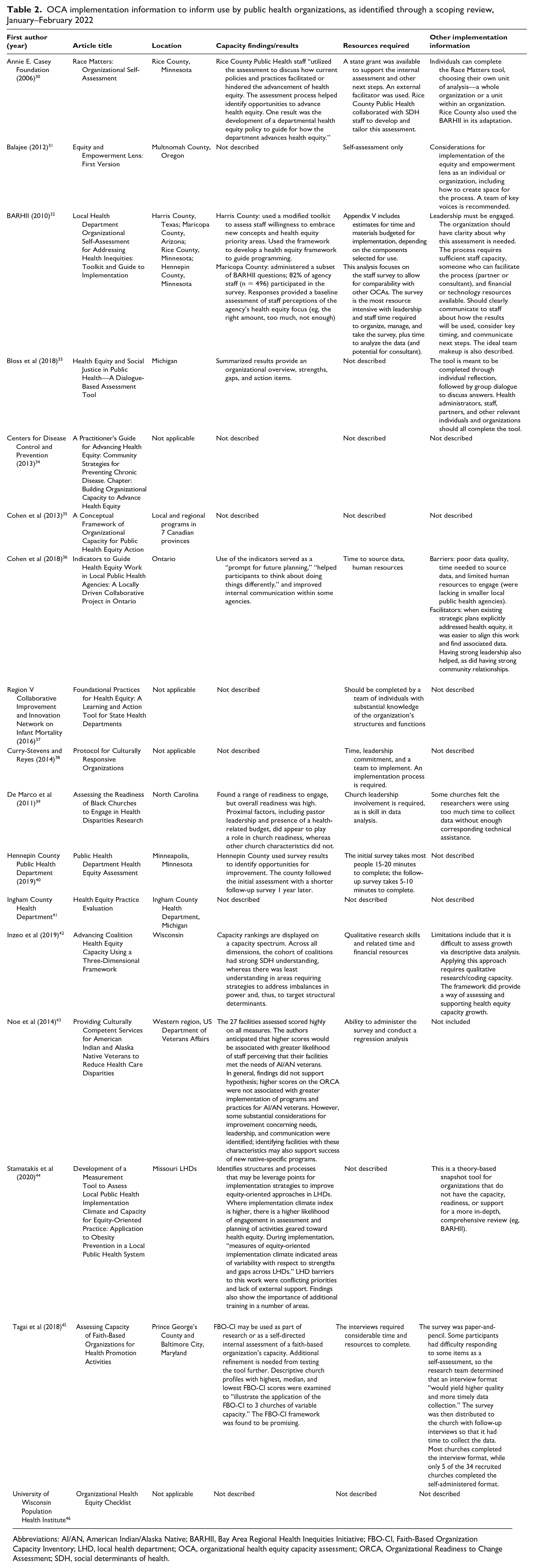
OCA implementation information to inform use by public health organizations, as identified through a scoping review, January–February 2022
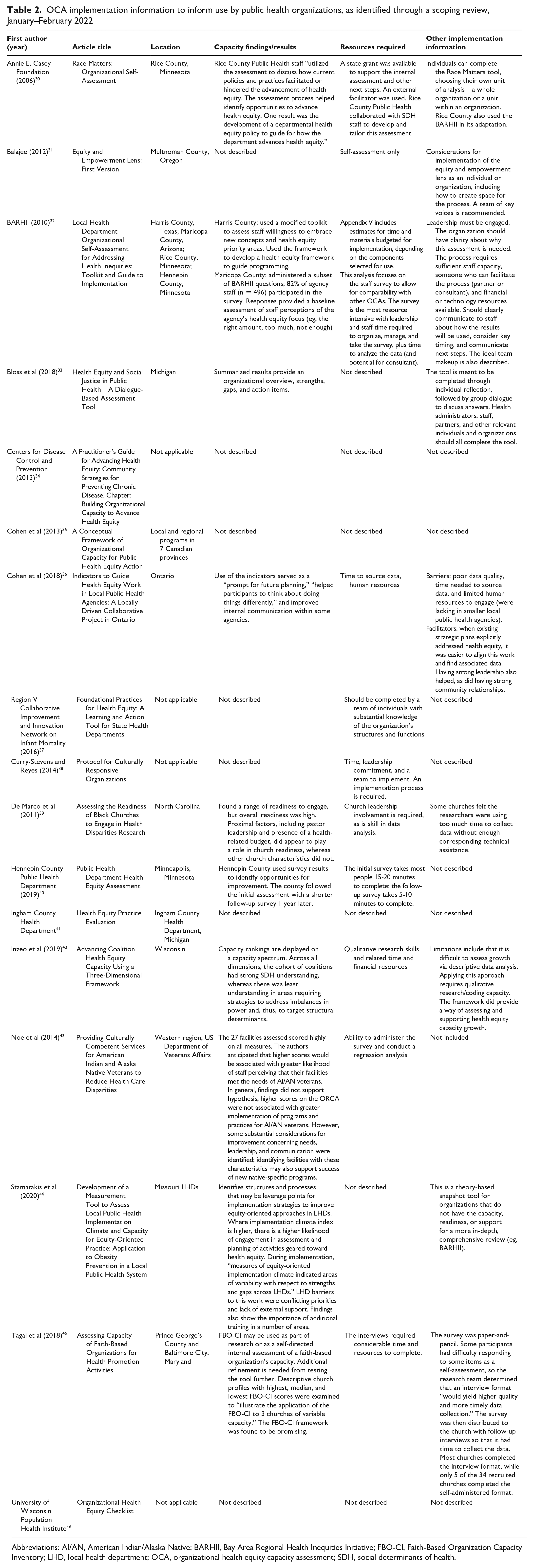
Abbreviations: AI/AN, American Indian/Alaska Native; BARHII, Bay Area Regional Health Inequities Initiative; FBO-CI, Faith-Based Organization Capacity Inventory; LHD, local health department; OCA, organizational health equity capacity assessment; ORCA, Organizational Readiness to Change Assessment; SDH, social determinants of health.
Discussion
We found little consistency in how organizational health equity capacity is defined or assessed. As public health organizations seek to strengthen efforts to reduce health inequities, we sought to fill a key gap in the literature by identifying and characterizing the tools that have been developed to assess or review capacity for organizational health equity. The 17 OCAs that we included can help public health organizations improve their capacity to develop, implement, and sustain equity-focused work. The OCAs all described a similar purpose, with common aims of assessing readiness or capacity for organizational health equity. Most aimed to provide considerations or strategies to increase organizational health equity capacity or readiness and can be used repeatedly to monitor progress.
Many OCAs lack specific definitions of organizational health equity capacity. Where specified, organizational health equity capacity is variably defined to include equity-oriented organizational characteristics, practices, programs, and policies; key competencies; and foundational practices. Some tools do not include definitions, making it challenging for potential OCA implementers to quickly assess whether the approach to organizational health equity capacity in a given tool is appropriate for their organization.
We found that OCAs published in the peer-reviewed literature were more challenging to find than OCAs published in the gray or practitioner literature, because they were not commonly linked on practice-oriented websites and were found only through a targeted search in Embase or PubMed. However, these peer-reviewed OCAs often included useful data on capacity findings or results. For example, the Health Equity and Social Justice Dialogue-Based Assessment Tool summarized results to provide an overview, strengths, gaps, and action items. 33 The LHD Implementation Climate and Capacity questionnaire, when implemented with 115 LHD practitioners in Missouri, identified barriers to health equity capacity development, including conflicting organizational priorities, a lack of external support for health equity work, and the importance of additional training in several areas. 44
Some but not all of the peer-reviewed tools included implementation information (eg, barriers to and/or facilitators of OCA implementation). Cohen et al field-tested indicators to assess and guide the health equity work of public health agencies among 4 local public health agencies in Ontario (a mix of urban and rural). 36 This pilot illuminated barriers to using the indicators, such as poor data quality, time requirements, and human resource requirements, as well as facilitators, such as strong leadership, community relationships, and existing strategic plans that address health equity. The authors of the Three-Dimensional Framework to Advance Coalition Health Equity Capacity noted that qualitative research and thematic coding capacity are needed for implementation. 42 The Faith-Based Organization Capacity Inventory framework was implemented with church congregations in Prince George’s County and Baltimore City, Maryland; although it was envisioned as a self-assessment, participants had difficulties responding, so an interview format was recommended instead. 45 In general, we found minimal descriptions of resources required.
Many LHDs—including but not limited to Harris County, Texas; Maricopa County, Arizona; Hennepin County, Minnesota; and Rice County, Minnesota—have adapted the Bay Area Regional Health Inequities Initiative’s LHD Organizational Self-assessment Toolkit for their own use. 32 (Rice County also incorporated the Race Matters Organizational Assessment. 30 ) These LHDs reported the utility of conducting these self-assessments but did not document their implementation process or results. The original Bay Area Regional Health Inequities Initiative toolkit includes a section on planning for implementation, describing leadership, communication, staff capacity, and resource requirements. 32
We could not identify capacity assessment results or implementation information for the following OCAs: the Health Department Self-Assessment Questions, 41 the Equity and Empowerment Lens, 31 the Protocol for Culturally Responsive Organizations, 38 the Learning and Action Tool for Public Health Organizations, 37 the Centers for Disease Control and Prevention’s Building Organizational Capacity to Advance Health Equity self-assessment module, 34 and the Organizational Health Equity Checklist. 46
Our research did not find sufficient evidence to explore the types of domains or measures most widely used or most applicable in different contexts. For example, 1 study identified the internal organizational health equity capacity factors that are likely important in the context of serving urban African American neighborhoods—leadership, institutional commitment, trust, credibility, and interorganizational networks. 47 Such findings could influence OCA selection. Contextual information should be included in OCA publications, if possible.
We did not restrict the type of OCA structures or formats that we included in the review, because we aimed to describe the full breadth of OCAs available. We found OCA structures ranging from a qualitative framework to individual surveys and reflections to a full toolkit with multiple components. Regardless of where an organization is in its health equity journey, an OCA is likely well suited. Yet, it was challenging to locate some OCAs, in part because the language used to describe this work varied widely. The most commonly used title was “assessment,” but OCAs were also described as a tool, protocol, conceptual framework, instrument, questionnaire, or inventory. Using consistent language would enable OCAs to be more easily found, compared, selected, and used.
Our scoping review had several limitations. First, publication bias is inherent in peer-reviewed databases, which we hope was minimized by searching the gray literature. Second, we searched as extensively as possible for gray-literature articles, reports, and case studies available online, but we may have missed some examples, including but not limited to those in languages other than English or those found only in additional databases. Finally, the field of health equity practice is changing rapidly, and our results are current only through March 2022.
Public Health Implications
Our review aims to bring the role of OCAs to the forefront of equity-oriented public health practice. OCAs provide a valuable starting point to understand an organization’s health equity readiness and capacity. Our characterizations of the identified OCAs are intended to assist public health organizations in selecting an OCA to assess, guide, and/or monitor their internal organizational health equity capacity. This review also provides a useful summary of the state of the art for anyone considering developing similar tools or frameworks. We recommend that future publications and case studies include data related to OCA implementation, including capacity findings, implementation lessons learned, and resources required, where possible. This information is necessary to inform OCA uptake and implementation.
Supplemental Material
sj-xlsx-1-phr-10.1177_00333549231151889 – Supplemental material for Characterizing Organizational Health Equity Capacity Assessments for Public Health Organizations: A Scoping Review
Supplemental material, sj-xlsx-1-phr-10.1177_00333549231151889 for Characterizing Organizational Health Equity Capacity Assessments for Public Health Organizations: A Scoping Review by Rachel Marcus, Nidhi Monga Nakra and Keshia M. Pollack Porter in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.