
Abstract
Objectives:
The COVID-19 pandemic has disproportionately affected racial and ethnic minority populations in the United States. The National Center for Health Statistics adapted the Research and Development Survey (RANDS), a commercial panel survey, to track selected health outcomes during the pandemic using the series RANDS during COVID-19 (RC-19). We examined access to preventive care among adults by chronic condition status, race, and Hispanic origin.
Methods:
NORC at the University of Chicago conducted RC-19 among US adults in 3 rounds (June–July 2020 [round 1, N = 6800], August 2020 [round 2, N = 5981], and May–June 2021 [round 3, N = 5458]) via online survey and telephone. We evaluated reduced access to ≥1 type of preventive care due to the pandemic in the past 2 months for each round by using logistic regression analysis stratified by chronic condition status and race and Hispanic origin, adjusting for sociodemographic and health variables.
Results:
Overall, 35.8% of US adults reported missing ≥1 type of preventive care in the previous 2 months in round 1, 26.0% in round 2, and 11.2% in round 3. Reduced access to preventive care was significantly higher among adults with ≥1 chronic condition (vs no chronic conditions) in rounds 1 and 2 (adjusted odds ratios [aOR)] = 1.5 and 1.4, respectively). Compared with non-Hispanic White adults, non-Hispanic Black adults reported significantly lower reduced access to preventive care in round 1 (aOR = 0.7), and non-Hispanic Other adults reported significantly higher reduced access to preventive care in round 2 (aOR = 1.5).
Conclusions:
Our findings may inform policies and programs for people at risk of reduced access to preventive care.
Keywords
Preventive care includes routine health care such as regular checkups and screenings. However, during the COVID-19 pandemic, access to preventive care was impacted by several factors, including medical office closures, limited appointment availability, and concerns about COVID-19. Previous research based on administrative and electronic health record data suggests that the first several months of the pandemic were associated with sharp reductions in the use of services for a range of health conditions. A retrospective cohort study of 89 university-affiliated medical practices in Toronto found that 34.5% fewer patients visited their physician at the beginning of the pandemic (March–June 2020) compared with prepandemic (March–June 2019). 1 Comparing health care utilization in March–April 2020 with March–April 2019, an analysis of employer-sponsored health insurance claims (6.4 million individuals in 2019, 6.8 million in 2020) from all 50 states found reductions in the number of surgical and diagnostic procedures. 2
In addition to administrative and health record data routinely captured before and after the emergence of the COVID-19 pandemic in the United States in March 2020, population-based surveys on the health impacts of COVID-19, including reasons for missed or delayed care, were implemented later in 2020. An online survey of a representative sample of US adults conducted during July 2020 found that 41% of adults avoided medical care between March and July 2020. 3 Among those needing health care during this time, the impact was more pronounced. Fifty-two percent of these adults avoided medical care, with approximately 25% indicating delays due to concern about COVID-19 exposure. 3 In another study, a sample of adult participants in 12 southeastern states from a prior cohort study were recontacted for a COVID-19 impact survey in the fourth quarter of 2020. Among the 4463 respondents, 40% reported missing or delaying a health appointment during the pandemic, with the most common reason being provider-initiated cancellation or delay. 4
While many studies have indicated worse access to care during the pandemic compared with previous years, the impact of the pandemic on access to care has varied among demographic groups.5,6 In an online survey of a representative sample of US adults conducted in June 2020, approximately 40% of adults avoided medical care during the pandemic because of concerns about COVID-19, including 12.0% who avoided urgent or emergency care and 31.5% who avoided routine care. 5 Avoidance of urgent or emergency care was significantly higher among people with ≥2 selected underlying medical conditions (vs no conditions), people with health insurance (vs no health insurance), and non-Hispanic Black and Hispanic adults (vs non-Hispanic White adults). 5 Another online survey representative of US adults aged 18-64 years conducted during September 2020 found that 39.7% of non-Hispanic Black adults, 34.3% of non-Hispanic White adults, and 35.5% of Hispanic adults avoided health care because of concerns about COVID-19 exposure or limited health care availability. 6 Furthermore, a higher percentage of adults with chronic health conditions than adults without chronic health conditions had delays in ≥1 type of health care (40.7% and 26.4%, respectively). Approximately one-third of adults who had delayed or forgone health care because of concerns about the pandemic reported negative effects on their health, ability to work, or ability to perform other daily activities. 6
These studies demonstrate a decline in access to care and varying levels of access to care by sociodemographic factors, particularly early in the pandemic. However, the impact of the pandemic has changed over time. While most states implemented lockdowns or stay-at-home orders early in the pandemic, many medical offices and health care facilities reopened following these lockdowns. In addition, the COVID-19 vaccine became available to health care personnel and people at increased risk of infection from COVID-19 in the United States in December 2020. 7 Although nearly 13 million adults received ≥1 dose of the vaccine in the first month of the US COVID-19 vaccination program, uptake was slower among certain sociodemographic groups, including racial and ethnic minority groups. 7
To further understand the differential impact of the pandemic on access to preventive care in the United States over time, we evaluated data from the Research and Development Survey (RANDS) during COVID-19 (RC-19). We examined the impact of the pandemic on access to preventive care among adults by race, Hispanic origin, and chronic condition status simultaneously and used cross-sectional analyses during 3 periods to assess how access to preventive care changed during the pandemic.
Methods
Data Source
To evaluate the impact of the COVID-19 pandemic on access to preventive care, we used data from the National Center for Health Statistics’ (NCHS) RC-19. 8 RC-19 is a probability-sampled commercial survey panel that was adapted from the existing RANDS program to monitor health outcomes during the pandemic. NORC at the University of Chicago conducted 3 rounds of data collection using the AmeriSpeak Panel 9 from June 9–July 6, 2020 (N = 6800), August 3-20, 2020 (N = 5981), and May 17–June 30, 2021 (N = 5458). Adults aged ≥18 years were sampled from the AmeriSpeak Panel using simple random sampling within strata defined by age, race and Hispanic origin, education, and annual household income. Rounds 1 and 2 had a longitudinal design, in which selected panelists were invited to participate in both rounds, whereas round 3 panelists were sampled independently. The 3 surveys had completion rates of 78.5%, 69.1%, and 69.5%, respectively. The Centers for Disease Control and Prevention Ethics Review Board reviewed and approved the RC-19 surveys.
NORC provided panel weights for each round, which account for the recruitment of panelists into the AmeriSpeak Panel, nonresponse follow-up, selection of panelists into the study, and adjustments to external population totals. NCHS further adjusted the panel weights to the National Health Interview Survey (NHIS) to account for potential selection bias. Specifically, weights from rounds 1 and 2 were calibrated to the 2018 NHIS on selected demographic and health variables including age, sex, race and Hispanic origin, education, annual household income, US Census region, marital status, diagnosed high cholesterol, diagnosed asthma, diagnosed hypertension, and diagnosed diabetes. Weights from round 3 were calibrated to the 2019 NHIS on the same demographic and health variables from the prior 2 rounds, as well as on metropolitan area and telephone service to adjust for the telephone oversample in the third round. The NHIS-calibrated weights, used to produce experimental estimates of health outcomes from RC-19, were used for the public release of selected outcomes 8 and are used for analyses in this article. The RC-19 data are publicly available. 10
Variables
RC-19 included measures of reduced access to 4 types of preventive care due to the pandemic in the previous 2 months: diagnostic or medical screening tests, regular checkups, dental care, and vision care. Reduced access to ≥1 type of preventive care was defined as reduced access to ≥1 of 4 preventive care types.
We considered adults to have chronic disease if they reported a diagnosis of ≥1 of the following chronic conditions: hypertension; high cholesterol; coronary heart disease; current asthma; chronic obstructive pulmonary disease, emphysema, or chronic bronchitis; cancer or a malignancy of any kind; and diabetes excluding prediabetes, borderline diabetes, and gestational diabetes. The frequency of missing values for individual chronic conditions in each round was low (0.32%-0.84%). Missing values were assumed to be a response of no (no chronic condition diagnosis). Race and Hispanic origin were complete in all 3 rounds and were evaluated using 4 categories: Hispanic (any race), non-Hispanic Black, non-Hispanic Other (including ≥2 race groups), and non-Hispanic White.
Additional sociodemographic and health variables considered included age group (18-44, 45-64, and ≥65 years), sex (male, female), education (≤high school diploma, some college, ≥bachelor’s degree), annual household income (<$50 000, $50 000-$99 999, and >$99 999), current health insurance coverage (yes, no), self-rated health (excellent/very good, good, fair/poor), US Census region (Northeast, Midwest, South, West), metropolitan area (metropolitan, nonmetropolitan), and usual place of care (≥1, none).
Statistical Analysis
Reduced access to ≥1 type of preventive care was evaluated using survey-adjusted logistic regression by chronic condition status and race and Hispanic origin. Three cross-sectional models were evaluated to assess the differential impact on adults with chronic disease and by race and Hispanic origin in each round while adjusting for variables known to be associated with health care access. The NHIS-calibrated weights and complex sample design were incorporated to produce nationally representative results. Adjusted odds ratios (aORs) were reported by chronic condition status (reference = no chronic conditions) and by race and Hispanic origin (reference = non-Hispanic White). We considered 95% CIs that did not contain 1 to be significant at α = .05. We performed analyses in SUDAAN version 11.0.3 (RTI International) to account for the complex survey design. The NCHS data presentation standards for proportions 11 were applied to all reported experimental estimates.
Results
Reduced access to ≥1 type of preventive care in the previous 2 months varied by round. In rounds 1 (June–July 2020), 2 (August 2020), and 3 (May–June 2021), 35.8%, 26.0%, and 11.2% of adults, respectively, reported missing ≥1 type of preventive care due to the pandemic.
Most respondents were non-Hispanic White and reported having ≥1 chronic condition (Table 1). The most common conditions reported were diagnosed hypertension and diagnosed high cholesterol. In all 3 survey rounds, <2.8% of respondents were missing data on ≥1 of the chronic conditions studied (164 in round 1, 165 in round 2, and 118 in round 3).
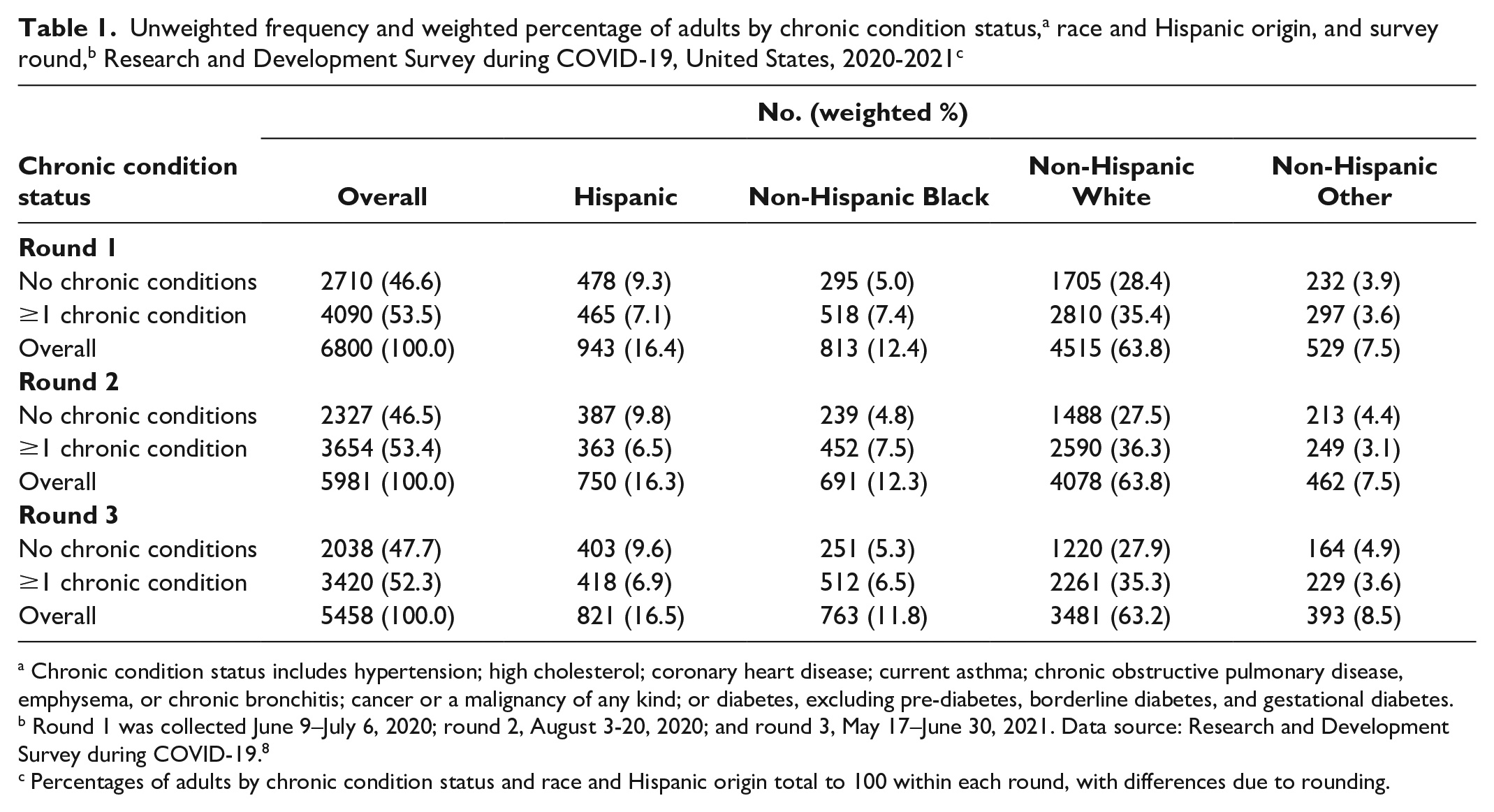
Chronic condition status includes hypertension; high cholesterol; coronary heart disease; current asthma; chronic obstructive pulmonary disease, emphysema, or chronic bronchitis; cancer or a malignancy of any kind; or diabetes, excluding prediabetes, borderline diabetes, and gestational diabetes.
Round 1 was collected June 9–July 6, 2020; round 2, August 3-20, 2020; and round 3, May 17–June 30, 2021. Data source: Research and Development Survey during COVID-19. 8
Percentages of adults by chronic condition status and race and Hispanic origin total to 100 within each round, with differences due to rounding.
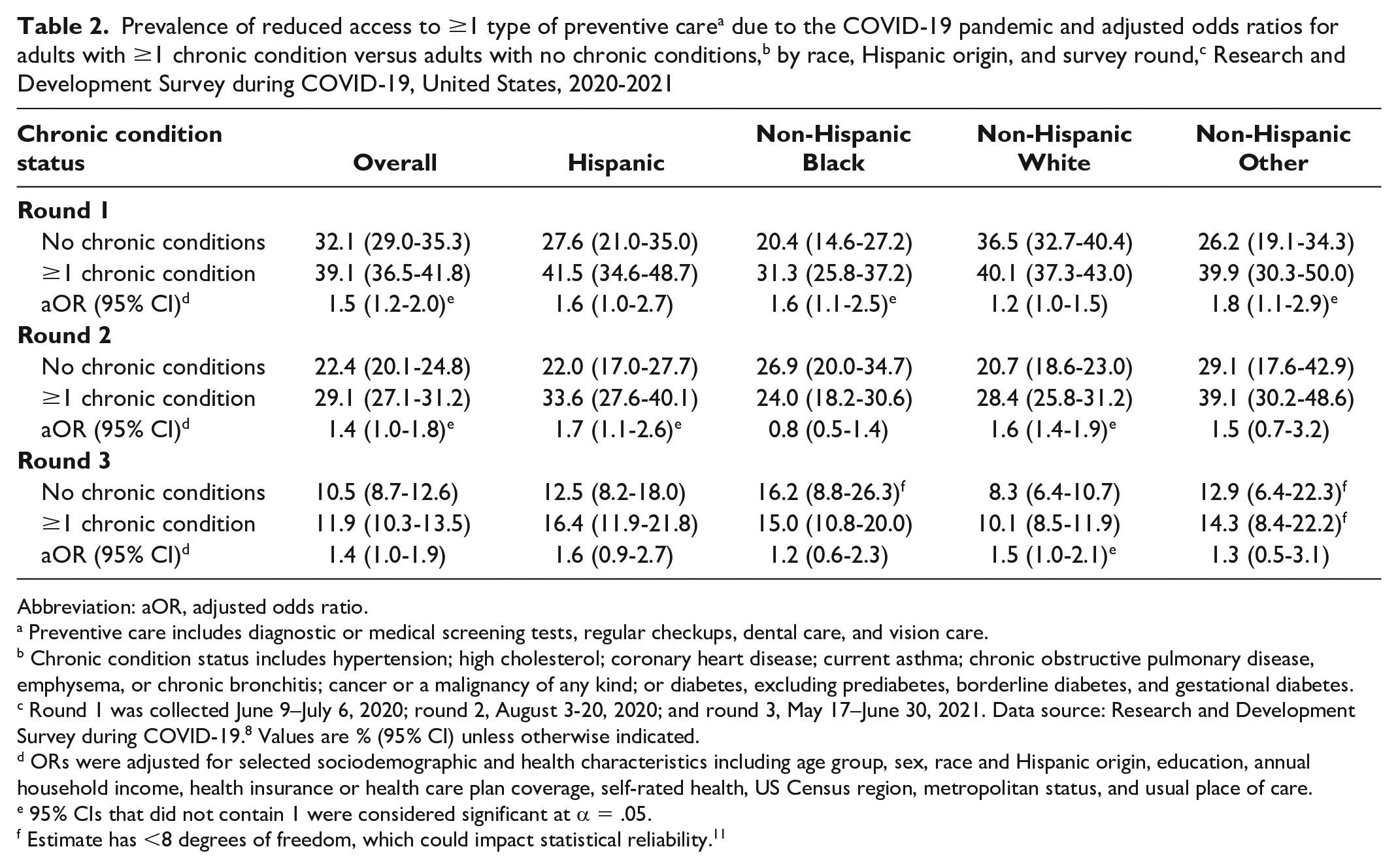
Overall, estimates of reduced access to preventive care were significantly higher among adults with ≥1 chronic condition than among adults with no chronic conditions in rounds 1 and 2 (Table 2). Differences by race and Hispanic origin varied by round. In round 1, non-Hispanic Black (aOR = 1.6; 95% CI, 1.1-2.5) and non-Hispanic other (aOR = 1.8; 95% CI, 1.1-2.9) adults with ≥1 chronic condition had higher adjusted odds of reduced access to preventive care than adults without chronic conditions. Hispanic adults with ≥1 chronic condition also had higher adjusted odds of reduced access to preventive care than Hispanic adults without a chronic condition (aOR = 1.6; 95% CI, 1.0-2.7), but this result was not significant. In round 2, non-Hispanic White (aOR = 1.6; 95% CI, 1.4-1.9) and Hispanic (aOR = 1.7; 95% CI, 1.1-2.6) adults with ≥1 chronic condition had significantly higher adjusted odds of reduced access to preventive care than adults without chronic conditions, but we found no differences in access to preventive care among non-Hispanic Black and non-Hispanic Other adults. In round 3, we found significant differences between adults with ≥1 chronic condition and without chronic conditions among non-Hispanic White adults (aOR = 1.5; 95% CI, 1.0-2.1). Differences among Hispanic adults were not significant, although the adjusted odds (aOR = 1.6; 95% CI, 0.9-2.7) were similar to those of non-Hispanic White adults.
Prevalence of reduced access to ≥1 type of preventive care a due to the COVID-19 pandemic and adjusted odds ratios for adults with ≥1 chronic condition versus adults with no chronic conditions, b by race, Hispanic origin, and survey round, c Research and Development Survey during COVID-19, United States, 2020-2021
Abbreviation: aOR, adjusted odds ratio.
Preventive care includes diagnostic or medical screening tests, regular checkups, dental care, and vision care.
Chronic condition status includes hypertension; high cholesterol; coronary heart disease; current asthma; chronic obstructive pulmonary disease, emphysema, or chronic bronchitis; cancer or a malignancy of any kind; or diabetes, excluding prediabetes, borderline diabetes, and gestational diabetes.
Round 1 was collected June 9–July 6, 2020; round 2, August 3-20, 2020; and round 3, May 17–June 30, 2021. Data source: Research and Development Survey during COVID-19. 8 Values are % (95% CI) unless otherwise indicated.
ORs were adjusted for selected sociodemographic and health characteristics including age group, sex, race and Hispanic origin, education, annual household income, health insurance or health care plan coverage, self-rated health, US Census region, metropolitan status, and usual place of care.
95% CIs that did not contain 1 were considered significant at α = .05.
Estimate has <8 degrees of freedom, which could impact statistical reliability. 11
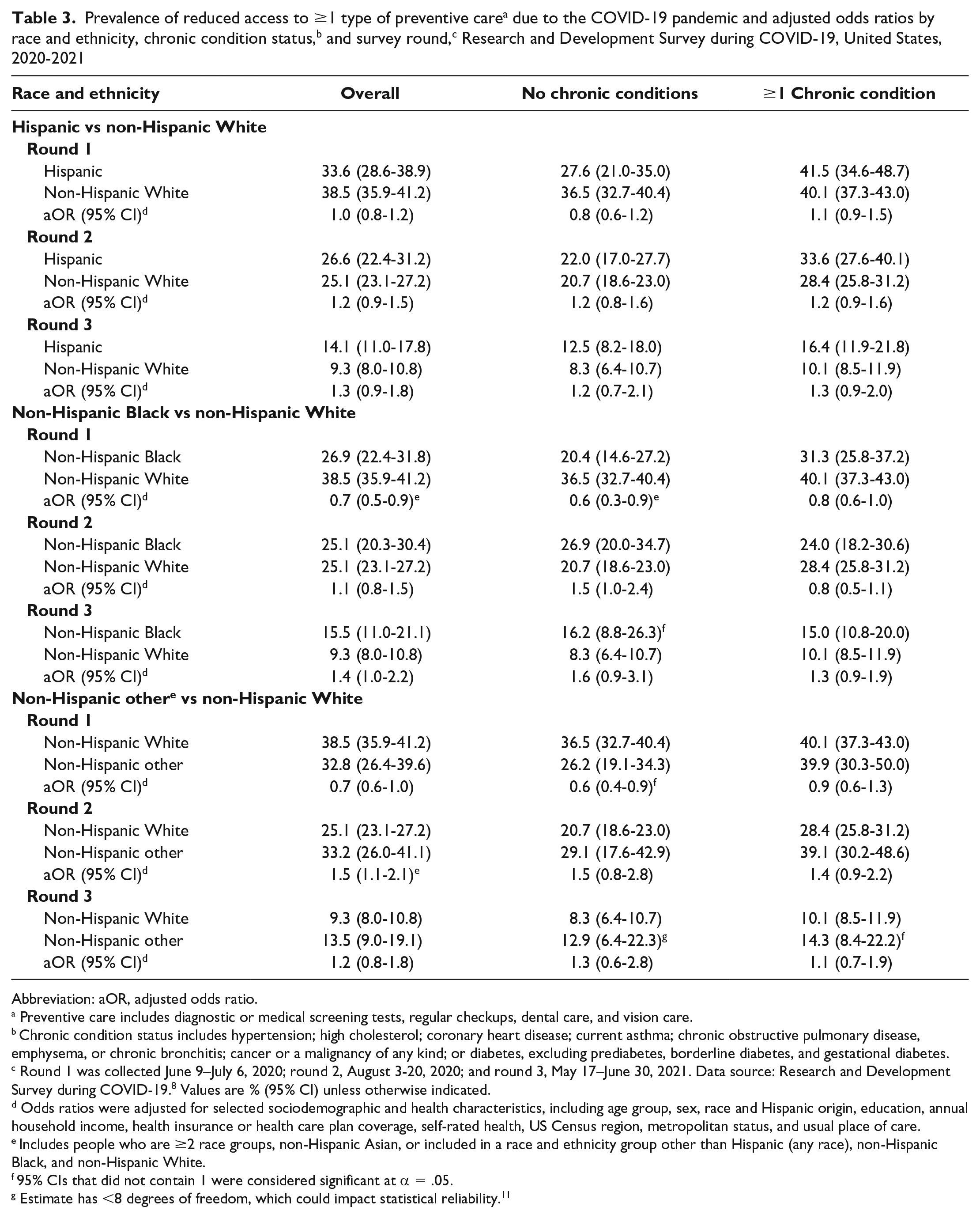
Overall, regardless of chronic condition status, compared with non-Hispanic White adults, non-Hispanic Black adults reported significantly lower reduced access to preventive care in round 1, and non-Hispanic Other adults reported significantly higher reduced access to preventive care in round 2 (Table 3). Among adults with no chronic conditions, non-Hispanic Black (aOR = 0.6; 95% CI, 0.3-0.9) and Hispanic (aOR = 0.6; 95% CI, 0.4-0.9) adults had significantly lower reduced access to preventive care than non-Hispanic White adults did in round 1. However, we found no significant differences in rounds 2 and 3.
Abbreviation: aOR, adjusted odds ratio.
Preventive care includes diagnostic or medical screening tests, regular checkups, dental care, and vision care.
Chronic condition status includes hypertension; high cholesterol; coronary heart disease; current asthma; chronic obstructive pulmonary disease, emphysema, or chronic bronchitis; cancer or a malignancy of any kind; or diabetes, excluding prediabetes, borderline diabetes, and gestational diabetes.
Round 1 was collected June 9–July 6, 2020; round 2, August 3-20, 2020; and round 3, May 17–June 30, 2021. Data source: Research and Development Survey during COVID-19. 8 Values are % (95% CI) unless otherwise indicated.
Odds ratios were adjusted for selected sociodemographic and health characteristics, including age group, sex, race and Hispanic origin, education, annual household income, health insurance or health care plan coverage, self-rated health, US Census region, metropolitan status, and usual place of care.
Includes people who are ≥2 race groups, non-Hispanic Asian, or included in a race and ethnicity group other than Hispanic (any race), non-Hispanic Black, and non-Hispanic White.
95% CIs that did not contain 1 were considered significant at α = .05.
Estimate has <8 degrees of freedom, which could impact statistical reliability. 11
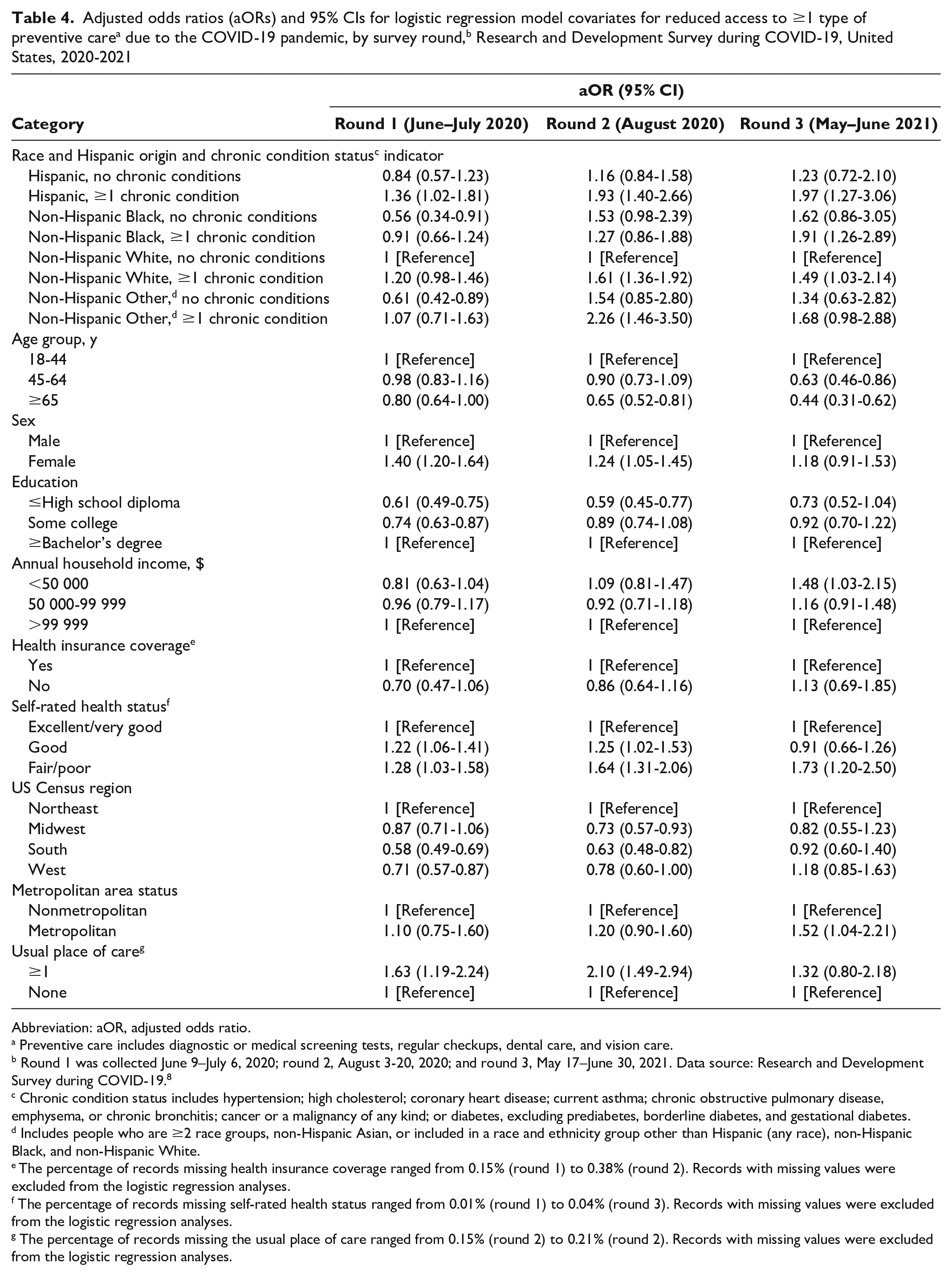
The logistic regression analyses (Table 4) revealed that self-rated health was an important predictor of reduced access to preventive care in all 3 rounds after adjusting for chronic condition status, race, and Hispanic origin. Adults with good self-rated health (rounds 1 and 2) or fair/poor self-rated health (rounds 1-3) reported significantly higher reduced access to preventive care than did adults with excellent/very good self-rated health. Age group and sex also explained differences in access to preventive care, with adults aged ≥65 years reporting better access to preventive care than adults aged 18-44 years in rounds 2 and 3, and women reporting less access to preventive care than men in rounds 1 and 2.
Abbreviation: aOR, adjusted odds ratio.
Preventive care includes diagnostic or medical screening tests, regular checkups, dental care, and vision care.
Round 1 was collected June 9–July 6, 2020; round 2, August 3-20, 2020; and round 3, May 17–June 30, 2021. Data source: Research and Development Survey during COVID-19. 8
Chronic condition status includes hypertension; high cholesterol; coronary heart disease; current asthma; chronic obstructive pulmonary disease, emphysema, or chronic bronchitis; cancer or a malignancy of any kind; or diabetes, excluding prediabetes, borderline diabetes, and gestational diabetes.
Includes people who are ≥2 race groups, non-Hispanic Asian, or included in a race and ethnicity group other than Hispanic (any race), non-Hispanic Black, and non-Hispanic White.
The percentage of records missing health insurance coverage ranged from 0.15% (round 1) to 0.38% (round 2). Records with missing values were excluded from the logistic regression analyses.
The percentage of records missing self-rated health status ranged from 0.01% (round 1) to 0.04% (round 3). Records with missing values were excluded from the logistic regression analyses.
The percentage of records missing the usual place of care ranged from 0.15% (round 2) to 0.21% (round 2). Records with missing values were excluded from the logistic regression analyses.
Discussion
This study considered the differential associations of access to preventive care among adults by chronic condition status and race and Hispanic origin during various phases of the COVID-19 pandemic. Data from the NCHS RC-19 indicate that access to preventive care varied among these subgroups, although the differences were not consistent across the 3 time frames. Reduced access to preventive care due to the pandemic declined with each successive round, with the largest improvement seen between rounds 2 and 3 (August 2020 and May–June 2021).
Overall, adults with ≥1 chronic condition had significantly higher reduced access to preventive care early in the pandemic (rounds 1 and 2) than adults with no chronic conditions. This result is consistent with previous studies showing that adults with underlying medical conditions have generally accessed care less frequently during the pandemic than before the pandemic,5,6 which could be related to heightened concerns about exposure to COVID-19; early data showed a higher risk of COVID-19 complications among these individuals. 12 However, by round 3 (spring 2021), access to preventive care did not differ significantly by chronic condition status. This change could reflect the availability of vaccines and adaptations made by patients and health care providers to the new normal of the extended pandemic. Non-Hispanic Black adults reported significantly lower reduced access to preventive care than non-Hispanic White adults did early in the pandemic (round 1), while non-Hispanic Other adults reported significantly higher reduced access to preventive care than non-Hispanic White adults did in round 2. The percentages for reduced access to preventive care due to the pandemic were compared with all other adults in that subpopulation, including those who received preventive care, did not seek preventive care, or did not receive preventive care for a reason other than the pandemic. Differences in reduced access to preventive care among racial and ethnic subgroups may be in part due to differences in health-seeking behaviors for certain subgroups. Differences in help-seeking behaviors could account for the differing findings from online surveys conducted early in the pandemic, which included evaluations of urgent or emergency care and suggested that non-Hispanic Black adults were more likely than non-Hispanic White or Hispanic adults to report experiencing delays or not getting needed health care.5,6 It should be noted that differences between online surveys (eg, coverage, instruments) may have contributed to somewhat different findings. Moreover, many possible drivers of forgone health care exist among racial and ethnic subgroups that were not investigated in this study, including medical mistrust and health care–related racism, which could contribute to the reported differences.13-16
While we identified differences in access to preventive care by race, Hispanic origin, and chronic condition status during the 3 rounds, many other factors could have impacted access to preventive care earlier in the pandemic, including quarantines, medical office closures, occupancy restrictions, and reduced access to public transportation. In addition, vaccines were available in the United States during round 3, which could have impacted access to preventive care during that time. At the time of round 3, 57% of adults in the United States had received at least 1 vaccine dose, although vaccine coverage differed by sociodemographic groups. 17 Adaptations to disruptions in daily life circumstances during the pandemic could explain some insignificant findings in later rounds.
Limitations
This study had several limitations. First, this study was based on data from a commercial survey panel. While data for RC-19 were collected from a probability-based panel and are nationally representative, online panels may produce lower-quality data than traditional household surveys conducted by NCHS and other statistical agencies due to smaller sample sizes and coverage bias. Second, RC-19 had limited sample sizes for subnational estimates and, thus, less statistical power to detect significant differences. Third, because RC-19 data were self-reported, the survey responses may be subject to recall bias.
Conclusions
In the earliest months of the COVID-19 pandemic in the United States, COVID-19 reporting at the federal level often did not include data on race and ethnicity, and concerns about adherence to subsequent regulations for reporting COVID-19 cases by race and ethnicity were also noted. 18 In addition, because of the pandemic, many federal household surveys were not conducted or data collection was impacted. RC-19 was able to be developed in rapid response to the need for timely reporting of COVID-19 health measures and fielded 3 times during the pandemic to collect information on several key health outcomes. This situation highlighted the flexibility of this platform and its potential to be used as a novel survey approach for reporting on disparities, including racial and ethnic and chronic disease disparities, among the US adults in a timely manner, particularly compared with the typical turnround time of a federal household survey. 19 Our study adds to the growing literature on access to preventive care during the COVID-19 pandemic in the United States and provides evidence that the associations among race and Hispanic origin, chronic condition status, and access to preventive care varied during the first 2 years of the pandemic.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the National Center for Health Statistics or the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.