
Abstract
This case study highlights the partnership development between a large, urban, public, community-based behavioral health system and an academic program. Using principles of partnership building and facilitators that enhance partnership building, we describe the process of initiating, building, and sustaining the partnership. The Health Resources and Services Administration (HRSA) workforce development initiative was the primary catalyst for the partnership development. The public, community-based behavioral health system is located in an urban, medically underserved area and health care professional shortage area. The academic partner is a master in social work (MSW) program in Michigan. We assessed partnership development by using process and outcome measures that captured changes in the partnerships and in implementation of the HRSA workforce development grant. The goals of this partnership were to develop the infrastructure to support the training of MSW students, expand workforce skills in integrated behavioral health, and increase the number of MSW graduates who work with medically underserved populations. During 2018-2020, the partnership trained 70 field instructors, engaged 114 MSW students in HRSA field placements, and developed 35 community-based field sites (including 4 federally qualified health centers). The partnership provided training for field supervisors and for HRSA MSW students and developed new courses/trainings focusing on integrated behavioral health assessment/intervention practices, trauma-informed care, cultural awareness, and telebehavioral health practices. Of 57 HRSA MSW graduates who responded to a postgraduation survey, 38 (66.7%) were employed in medically underserved, high-need/high-demand urban areas. Partnership sustainability was helped by formal agreements, regular communication, and a collaborative decision-making approach.
Developing partnerships between universities and communities is challenging.1,2 Drahota et al defined a community–academic partnership as being characterized by equitable control, a cause that is primarily relevant to the partners, having specific aims that address shared goals, and involving representatives or agencies that have knowledge of the cause as well as academic researchers. 1 Recent initiatives that focused on prioritizing partnership building between communities and universities highlight the importance of shared capacity-building experiences and taking a long-term perspective on collaboration for research development.3 -5 In previous studies, several themes emerged for successful community–academic partnerships, including a commitment to action, a change focus, adequate resources, organizational capacity building, an understanding of power dynamics, and engagement in reflective practice.4 -6 Swick et al added to the definition an understanding of how decisions are made, communication, transparency, accountability, formalized agreements, a well-balanced team, and opportunities to present information and publish together. 5 While previous studies focused on establishing partnerships to build research collaborations, little has been done in partnership building to address workforce development.
The Health Resources and Services Administration (HRSA) workforce development initiative focused on community–academic partnership building to expand workforce development and build the infrastructure to sustain these efforts. The community–academic partnership involved an urban, public, community-based behavioral health (PCBBH) system in a medically underserved/health care professional shortage area and a university graduate program (University of Michigan School of Social Work, Ann Arbor, Michigan).
Principles for University–Community Partnerships
PCBBH administrators and faculty leads used the principles of Hudson and Hardy to guide this partnership building. 7 They identify 6 principles for university–community partnerships: (1) acknowledgment of the need for partnership; (2) clarity of purpose; (3) commitment and ownership; (4) development and maintenance of trust; (5) establishment of clear and robust partnership arrangements; and (6) monitoring, review, and organizational learning. 7 The partners reviewed factors that can enhance partnership building: trust among partners; respect among partners; shared vision, goals, and/or mission; good relationships among partners; effective and frequent communication; differentiated roles and functions of partners; and mutual benefits. 1
Principle 1: Acknowledgment of the Need for Partnership
The HRSA workforce development grant provided a catalyst for the academic program and the PCBBH system to enter into a partnership. The faculty began a dialogue with leadership of the PCBBH system to explore workforce development and ways to build infrastructure to recruit, train, and retain master of social work (MSW) students to work in the PCBBH system.
The PCBBH system, the largest public mental/behavioral health provider in Michigan, provides behavioral health services and supports in a large urban community in collaboration with >80 contract agencies and 4 comprehensive health care provider networks. The community is designated as a medically underserved/health care professional shortage area. Medically underserved is a designation by HRSA that indicates that the community has a shortage of health care providers and is a location with a high poverty rate.
The University of Michigan School of Social Work enrolls approximately 600 MSW students each term and has >60 full-time faculty. During 2015-2020, the program awarded 1784 MSW degrees (unpublished report, University of Michigan School of Social Work Admissions and Student Services Office, September 2020). Most graduates have focused on interpersonal practice (on average, 66% each year) (unpublished report, University of Michigan School of Social Work Career Center, September 2020). The University of Michigan School of Social Work is located about 40 miles from the PCBBH system.
Prior to building this partnership, the academic program worked individually with contract agencies in the large PCBBH system to arrange social work field placements. The field placement process was time intensive for both the academic program and the contract agency. The quality of the learning varied by what resources each contract agency had to support supervision of students. The high turnover of field instructors and scarce resources limited the sustainability of placements.
PCBBH administrators were concerned with the time and resources that contract agencies spent on supporting the training of MSW students, with minimal direct benefits to the agencies. They were interested in developing a pipeline to recruit qualified staff.
Principles 2 and 3: Clarity of Purpose and Commitment/Ownership
The leaders from the academic program and the PCBBH system set ground rules for working together. These rules helped build trust between partners and a shared vision for the partnership. The group appointed a primary lead from each partner to establish regular meetings and facilitate communication. The collaboration focused on challenges in workforce development and building a sustaining partnership based on the strengths of each partner. The partnership was formalized through agreements signed between the academic program and the PCBBH system. Seed funds offered by the HRSA workforce development initiative motivated the partners to submit the workforce grant proposal. The academic partner took responsibility for writing the HRSA workforce grant proposal, and PCBBH administrators provided input on each component of the proposal. The commitment to the partnership was reinforced when the partnership secured the HRSA workforce development grant.
Methods used to assess partnership building
Different process and outcome methods assessed progress related to the partnership building. The process methods included periodically conducting informal interviews and focus groups with key partners (eg, PCBBH administrators, field instructors, faculty, students) to identify challenges and solutions related to partnership goals, quarterly meetings to review progress related to the tasks and workforce implementation, and rapid check-ins to modify goals or tasks where needed. To assess outcomes, the partnership team identified target goals for the development of centralized training opportunities for field instructors and for the development of field placement sites that focus on integrated behavioral health. Postmeasures assessed training resources, courses, and programs developed; field instructor assessment of skill building; and MSW student skill acquisition. Feedback from the process and outcome measures guided changes in the implementation of the partnership and workforce development goals.
Principles 4 and 5: Development and Maintenance of Trust and Establishment of Clear and Robust Ownership
While securing seed money from HRSA, the partners established shared goals and identified areas that each partner could contribute toward the shared goals. Preparing the workforce development grant proposal opened the door to thinking creatively about how to better prepare the current/future workforce in an integrated health environment in medically underserved communities. By sharing data and drafts of the proposal, the faculty and the PCBBH administrators began to appreciate the challenges that each partner faced when delivering quality education and effective behavioral health services with scarce resources and a shortage of professional staff.
Trained MSW interviewers conducted informal interviews with various partners (eg, faculty, field instructors, administrators, students) about the initiative’s shared goals. The team reviewed ideas generated, and the plan that emerged addressed the following: (1) current challenges related to recruitment of students committed to working in medically underserved communities and health professional shortage areas, (2) reorganizing the MSW field placement support at the PCBBH system level by providing funding to help support the development of a centralized field supervisor training, (3) using various platforms (in-person formats, online options) to provide integrated health training for students and current staff, and (4) increasing interest of MSW graduates to work within the PCBBH system. The plan required a review of current academic courses and field trainings as they relate to integrated behavioral health skills, trauma-informed care practices, diversity trainings, and interprofessional teamwork. The PCBBH leaders and academic leaders, as well as key team members who are experts in the areas covered, reviewed the current certification/trainings offered by the PCBBH system and identified areas for modifications. The academic team and the PCBBH administrators supported the plan that evolved for workforce development enhancement that required action from both partners to implement. With the HRSA grant, the partnership began to implement the goals established for collaboration and system improvements. It was important for trust building that the funds allotted for administrative tasks and training development in the HRSA grant were shared between the partners.
The HRSA workforce development grant had 4 primary objectives that were consistent with the partnership goals: (1) developing a specialized Training Program in Integrated Behavioral Health and Primary Care for MSW students (n = 30 per year), (2) developing centralized programs to enhance multidisciplinary workforce trainings, (3) establishing formal agreements between the university and the PCBBH system, and (4) promoting recruitment and retention of MSW students after graduation to continue to work in medically underserved communities.
Principle 6: Monitoring, Review, and Organizational Learning
The HRSA seed money was used for the following: (1) support stipends for recruitment of MSW students committed to work in medically underserved communities and where health professional shortages exist, (2) provide funds for an on-site coordinator at the PCBBH system to facilitate the centralized field placement process and a lead field liaison from the academic social work program, and (3) develop centralized training resources for field instructors to complete integrated health certificates and other trainings using a range of learning platforms. The faculty and administrators established a tracking system to monitor the work of the partnership and the grant work. The team divided roles and responsibilities to ensure that each objective was accomplished.
Methods
Students completed an online pre-/postsurvey that focused on 14 integrative health core competency skills to assess growth during field placement. The online surveys took about 15 minutes to complete. The students were in field placements for 12 months. The request to complete the surveys was sent by email. Students rated their demonstration of the competency skill on a scale from 0 to 2, where 0 = no opportunity to demonstrate, 1 = beginning to demonstrate competency, and 2 = demonstrating competency in using the skill. We analyzed these surveys using SPSS version 28 (IBM Corp). We used 2-sided t tests to determine significant differences between the premeasure (taken in the first month that students entered field placements) and the postmeasure (completed 12 months later, at the end of the field placement). We set significance at P < .05. We calculated the mean (SD) for each competency item. We used Cohen d to determine the effect size. The University of Michigan Institutional Review Board–Health Sciences and Behavioral Science Research determined the research met the criteria for exemption status (HUM00141871).
The academic team also sent a postsurvey to MSW graduates from 2018-2019 and 2020 who completed the HRSA training and field placement each year. The initial postsurvey was sent at least 1 year after graduation to the 2018 and 2019 MSW graduates, and the same survey was sent 1 year after graduation to the 2020 MSW graduates. Graduates were contacted via email, and reminders were sent 7 and 14 days after the initial email. We analyzed responses using descriptive statistics. Questions in the postsurvey focused on employment in MSW positions, target populations that they serve (medically underserved populations, racially and ethnically marginalized populations), work setting type (integrated health care settings, behavioral health settings), whether they use telebehavioral health, and the types of telebehavioral health services used (eg, case management, care coordination, counseling or talk therapy, referrals, assessment, collaboration).
Outcomes
For objective 1, the academic faculty had primary responsibility to develop new courses within the MSW curriculum to meet the needs identified by the PCBBH system for successful student placements and to develop certificate programs in integrated health and addictions for field instructors (Table 1). PCBBH administrators served in an advisory capacity for these curricular changes and training programs. One new MSW course developed was an Interprofessional Clinical Decision Making course that enrolled not just social work students but also students from medicine, nursing, dentistry, and pharmacy. This course used case studies in which students worked in interprofessional teams to address complex integrated health issues. To strengthen student skills in integrated health assessment and evidence-informed practices, 2 additional MSW courses were developed: Integrated Behavioral Health Assessment and Integrated Health Practice. Several 1-credit MSW courses focusing on special populations served by the PCBBH system, as well as more intensive courses on substance use disorders and opioid treatment approaches, trauma-informed care, telebehavioral health practices, diversity training, and suicide prevention/treatment, were also developed and approved by the academic program. Students evaluate the new courses after each offering, and core faculty review the courses annually for modifications or updates. For example, when a need was identified for more training in telebehavioral health practices, telebehavioral health assessment and practices were integrated into the core courses. In addition, students who engage in a field placement at the PCBBH sites also complete the Certifications for Mental Health in the State and the HRSA Area Health Education Center training certificate in integrated health. The PCBBH system identified these additional certifications as critical for student readiness to engage in field learning.
New MSW courses, student trainings, and key trainings for field instructors who supervise MSW students completing the HRSA Workforce Development Professional Training, University of Michigan School of Public Health, 2018-2020
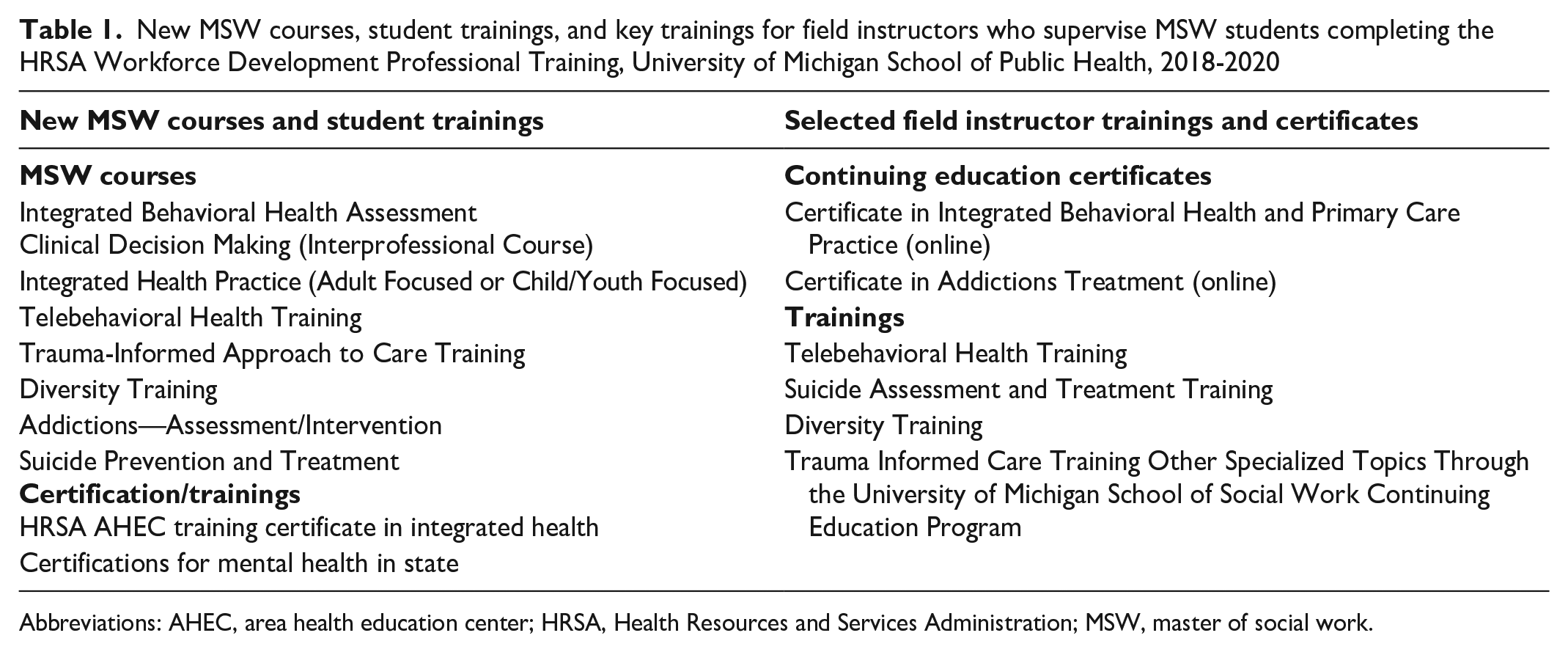
Abbreviations: AHEC, area health education center; HRSA, Health Resources and Services Administration; MSW, master of social work.
For objective 2, trainings for field instructors were developed jointly with administrators from the PCBBH system and faculty from the university (Table 1). The trainings were offered on site, in person, or online. The online field instructor trainings included single-session workshops and certificates. The online certificates were offered using asynchronous and synchronous formats. The 2 online certificate programs developed were based on the highest-priority training needs identified by PCBBH administrators. Continuing education certificates were the Certificate in Integrated Behavioral Health and Primary Care Practice and Addictions Treatment. An advisory group (including faculty and PCBBH administrators) reviewed the programs. Seventy to 80 field instructors participated in workshops or trainings each year during 2018-2020. The online Certificate in Integrated Behavioral Health and Primary Care Practice was completed by 35 field instructors.
For objective 3, formal agreements between the university and the PCBBH system and with each contract agency were signed for a 5-year cycle. The agreements identified how the partnership was being structured and what the expectations were of each partner.
For objective 4, the academic program recruited MSW students committed to working in medically underserved communities. The academic program recruited students through a formal application process. Students wrote an essay focusing on their career goals and how those goals fit with those of this workforce initiative. An advisory group of faculty and PCBBH administrators reviewed applicants. The top applicants were interviewed, and those selected signed an agreement that they would seek employment after graduation in medically underserved communities. A total of 114 students completed the HRSA training program during 3 years: 30 (26.3%) came from economically disadvantaged backgrounds (eg, poverty, low-income communities); 29 (25.4%) identified as African American, 20 (17.5%) as Hispanic, and 73 (64.0%) as White; and 98 (86.0%) reported gender identity as female.
A strength that emerged from this partnership was that (1) the participation of key faculty and administrators from the PCBBH system remained stable during the 3 years of the partnership building and (2) the commitment to the initiative remained high. Thirty-five field placement sites were developed within the PCBBH system, including 4 federally qualified health centers. This change in the number of field placement sites is important. Of the 35 field placements developed, 30 (85.7%) settings had behavioral health and medical providers physically or virtually located at the setting, and in 27 (77.1%) settings, patient information is exchanged with other health care providers. Seventeen (48.9%) settings had medical and behavioral health providers who were equally involved in patient care.
Pre- and Postsurveys
Eighty-seven students responded to the pre-/postsurvey on integrated health core competency skills (Table 2). On the postsurvey, students reported demonstrating the highest level of competency (mean [SD] 2.0 [0.5]) on 2 core competency skills: (1) establish rapport rapidly and develop and maintain effective working relationships; (2) listen actively and effectively, as demonstrated by the ability to quickly grasp presenting problems, needs, and preferences. For other health core competency skills, the scores ranged from 1.6 to 1.9 on the postsurvey. All changes in scores from pre- to postsurvey were significant at P < .001.
Pre- and postmeasures of integrated health core competency skills of HRSA MSW students identified by the Interprofessional Education Task Group at the University of Michigan School of Social Work, 2018-2020 (N = 87)
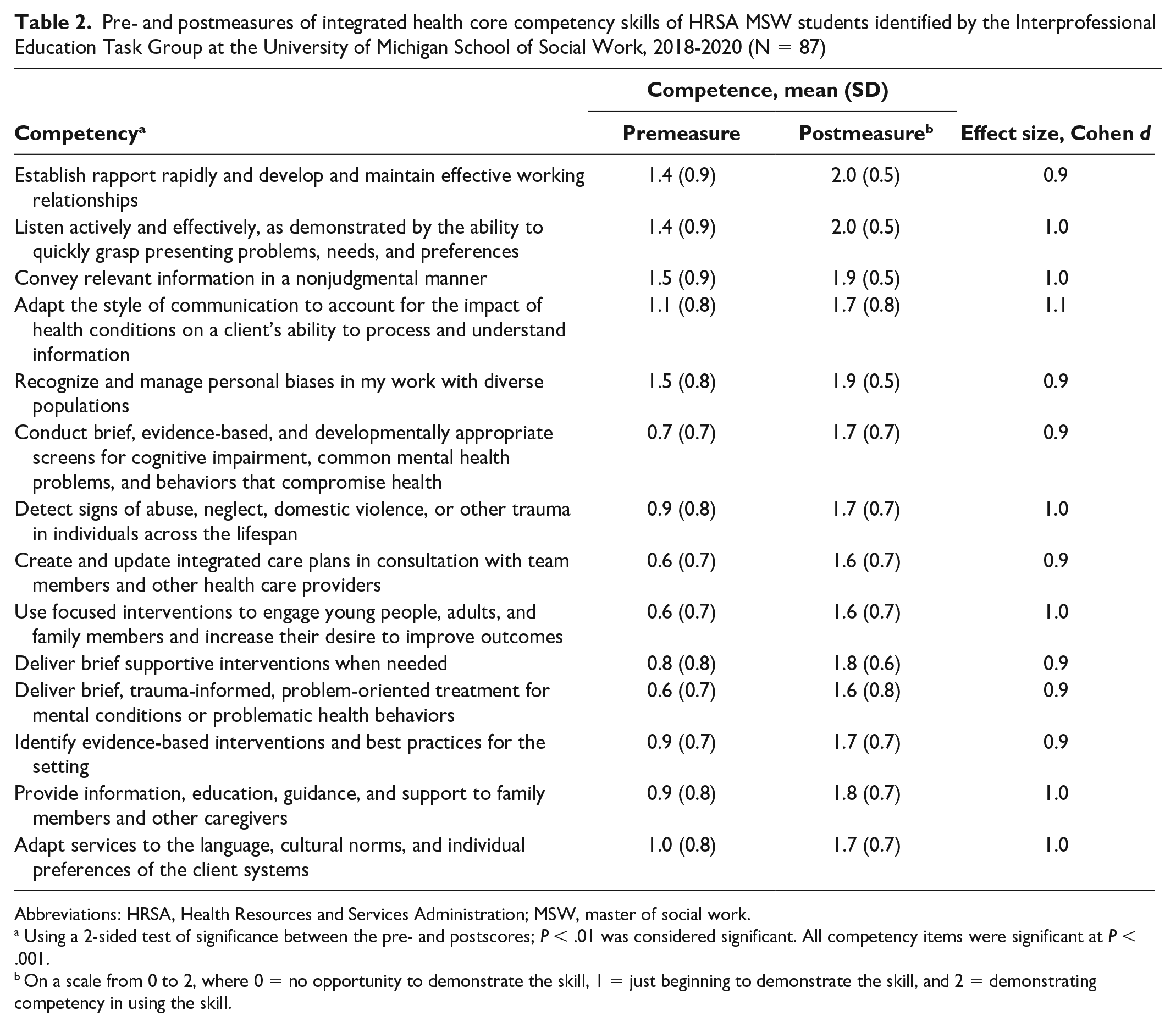
Abbreviations: HRSA, Health Resources and Services Administration; MSW, master of social work.
Using a 2-sided test of significance between the pre- and postscores; P < .01 was considered significant. All competency items were significant at P < .001.
On a scale from 0 to 2, where 0 = no opportunity to demonstrate the skill, 1 = just beginning to demonstrate the skill, and 2 = demonstrating competency in using the skill.
In 2 separate surveys of employment, work, and telehealth skills conducted among MSW students who graduated in 2018-2019 and 2020, 57 of 87 (65.5%) respondents worked in medically underserved communities providing integrated health or behavioral health services (Table 3). Of 28 survey respondents who graduated in 2018-2019, 22 (78.6%) were serving as new field instructors within the PCBBH system. Nearly all respondents (27 from 2018-2019 and 27 from 2020) indicated working with racially and ethnically marginalized populations.
Employment, settings, and provision of telebehavioral health services of MSW graduates of the HRSA partnership training, University of Michigan School of Social Work, 2018-2020
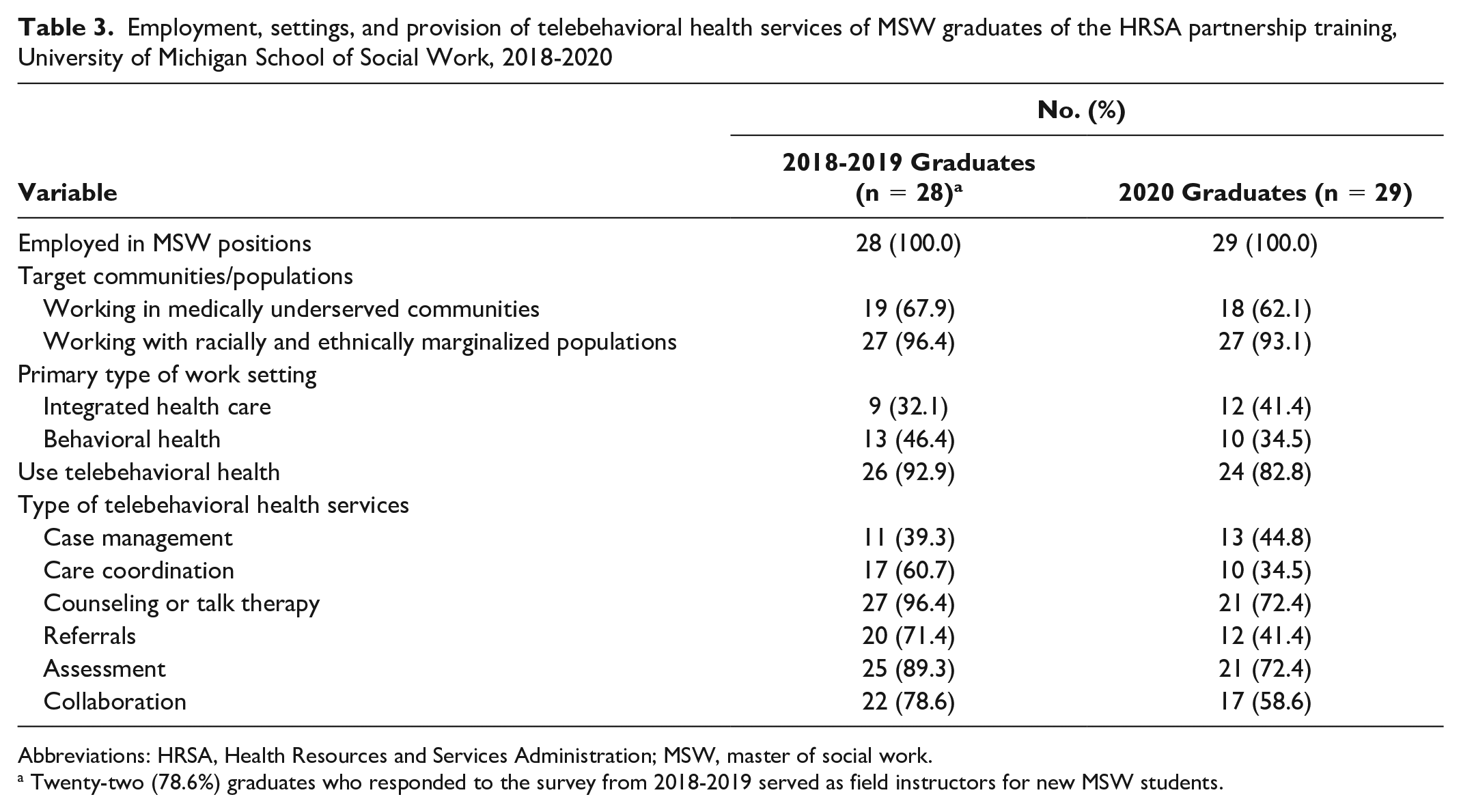
Abbreviations: HRSA, Health Resources and Services Administration; MSW, master of social work.
Twenty-two (78.6%) graduates who responded to the survey from 2018-2019 served as field instructors for new MSW students.
Lessons Learned
Using the principles of partnership building and addressing facilitators that promote partnership building helped to keep this partnership on track, especially when unexpected changes occurred during the implementation phase (eg, mission changes, the COVID-19 pandemic).1,7 First, the PCBBH system changed its mission and charter during the partnership development period and increased its focus on integrated behavioral health and primary care. This change required the team to reexamine how students were trained while in field placement, what training supervisors needed to have to improve delivery of behavioral health services, and how interprofessional education would be supported in this new mission. Second, the MSW program was going through a major curriculum reform at the same time that the PCBBH was changing its mission. The MSW program was involved in a strategic planning process to revise and update the curriculum in all areas, including the interpersonal practice curriculum. These 2 challenges strengthened the partnership. The leaders from the PCBBH team and the academic program sought input from each other while the changes were being discussed, and modifications were initiated per feedback from partners. The team members also noted when the decision-making process was outside the control of the team.
A third challenge emerged as a result of the COVID-19 pandemic: the partners needed to rapidly change the way that field placements and trainings were implemented because of social-distancing protocols and the move to telebehavioral health practice. In partnership meetings, creative solutions were explored, flexible schedules were established, and new trainings were developed. One solution was the academic program purchasing simulations that MSW students and field instructors could use to role-play evidence-based skills. Another solution was a new field placement option that centralized students in an intake/assessment team that used telebehavioral health approaches for clients in crisis, on waiting lists, or in need of case/care management services.
The success of this partnership was based on recognizing the expertise of each partner and engaging in finding solutions as a team.5,6 The partnership focused on building trust and respect by encouraging team members to be flexible, transparent, and committed to action and to have shared goals.3 -6 The sustainability of the partnership was helped by having formal agreements and regular communication. 5 Having shared funding to build on common goals was important for initiating and sustaining the work. If the HRSA funding had not been available, it would have been difficult to build the partnership. Not surprisingly, resources to support change are essential.3 -5 This partnership was successful in building the workforce in the areas of documented need. Sustaining these gains will take time, an ongoing commitment to the partnership goals, and a willingness by both partners to create flexible boundaries to support the work.
Footnotes
Acknowledgements
The authors acknowledge the time and commitment from students, staff, and faculty to implement this initiative and sustain the partnership.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A HRSA workforce development Behavioral Health Workforce Education and Training Program grant (M01HP31331) funded the work presented in this article.