
Abstract
Family members play a crucial role in the health of Asian American communities, and their involvement in health interventions can be pivotal in optimizing impact and implementation. To explore how family members can be effectively involved in Asian American health interventions and develop a conceptual framework of methods of involvement at the stages of intervention development, process, and evaluation, this scoping review documented the role of Asian American family members in interventions (across any health objective). Of the 7175 studies identified through database and manual searches, we included 48 studies in the final analysis. Many studies focused on Chinese (54%) or Vietnamese (21%) populations, were conducted in California (44%), and involved spouses (35%) or parents/children (39%). We observed involvement across 3 stages: (1) intervention development (formative research, review process, material development), (2) intervention process (recruitment, receiving the intervention together, receiving a parallel intervention, enlisting support to achieve goals, voluntary intervention support, agent of family-wide change, and participation gatekeepers), and (3) intervention evaluation (received evaluation together, indirect impact evaluation, and feedback during intervention). Impact of family member involvement was both positive (as sources of encouragement, insight, accountability, comfort, and passion) and negative (sources of hindrance, backlash, stigma, obligation, and negative influence). Suggestions for future research interventions include (1) exploring family involvement in South Asian or young adult interventions, (2) diversifying types of family members involved (eg, extended family), and (3) diversifying methods of involvement (eg, family members as implementation agents).
Asian Americans, a diverse community of people tracing their ancestry from East, South, and Southeast Asia, are the fastest growing ethnic minority group in the United States. 1 Asian Americans face a complex and growing range of disease disparities linked with a socioecological context distinct from other communities in the United States.2-5 As such, a diverse range of multilevel interventions have been explored to address Asian American health disparities,6-10 which have included educational efforts aimed at health-related knowledge or attitudes, 9 integration of technology to enhance the accessibility of health care or adherence to health behaviors,10,11 integration of cultural or religious principles as part of community- and faith-based approaches for health promotion,8,12 and expansion of the accessibility of health-related resources or services. 13 However, systematic exploration of the ways that interpersonal relationships, including those with family members, can also be integrated into Asian American health interventions to enhance the ability to meet interventional goals has been limited.7,14
Family dynamics form the foundation of the socialization, acculturation, and ultimately health experiences of Asian American communities. Across the United States, 73% of Asian Americans report living with family members (compared with the US average of 65%), although this proportion is as high as 88% and 87%, respectively, among Bangladeshi and Burmese Americans. 15 For Asian Americans, family members act as vital social resources in navigating the complex social, cultural, economic, and policy landscape of the United States. Of additional relevance to intervention health efforts is the value system of familism prevalent across Asian American communities16,17 or the system of values about the mutual interdependence, collaboration, and shared decision making within families, including the emphasis on family-level over individual-level interests.18,19
Therefore, in the context of familism and the substantial social capital of family members, individual-level or family-based interventions that actively engage family members in the different stages of the implementation process may represent a pathway to ensure the acceptability, effectiveness, and sustainability of health improvements in Asian American communities. For example, aside from involvement in the development and tailoring of intervention efforts, family members may also be powerful implementation agents to carry out intervention activities or an important source of insight during intervention evaluations. 7 This review aimed to explore how Asian American health interventions involved or collaborated with family members as part of various components of an intervention and the impact of this involvement or collaboration on intervention aims and outcomes.
Methods
We selected the scoping review method because we aimed to explore mapping concepts and themes in the extant literature and identify important research gaps, as opposed to answering a specific research question.20,21 We developed and registered a protocol for the review on PROSPERO. 22 We conducted this scoping review by following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol for scoping reviews. 23 We used search terms (eTable 1 in the Supplement) to search the literature published on or after September 1, 2021, in the following databases: PubMed, Embase, Web of Science, and Cochrane (Figure 1). An analysis informed the development of this search strategy of (1) past systematic reviews on family-based interventions and Asian Americans, (2) input from coauthor content experts on family-based interventions and Asian Americans, (3) keywords used in potential studies to be included in the analysis, (4) relevant Medical Subject Headings (MeSH) terms, and (5) pilot testing of different keyword combinations in databases. We also conducted a manual search of additional peer-reviewed and gray literature on clinical trial registries (eg, Clinicaltrials.gov) and Google Scholar by using the study search terms and snowball searching through reference lists in potentially relevant articles. 24 We applied a set of inclusion and exclusion criteria (eTable 2 in the Supplement) to determine eligibility. Intervention studies, including protocols or registered clinical trials, or observational studies describing the impact or characteristics of an intervention (eg, process evaluations) focused on any health-related issue in a US-based population primarily composed of those with ancestry from East, South, Southeast, or Central Asia were eligible for inclusion.
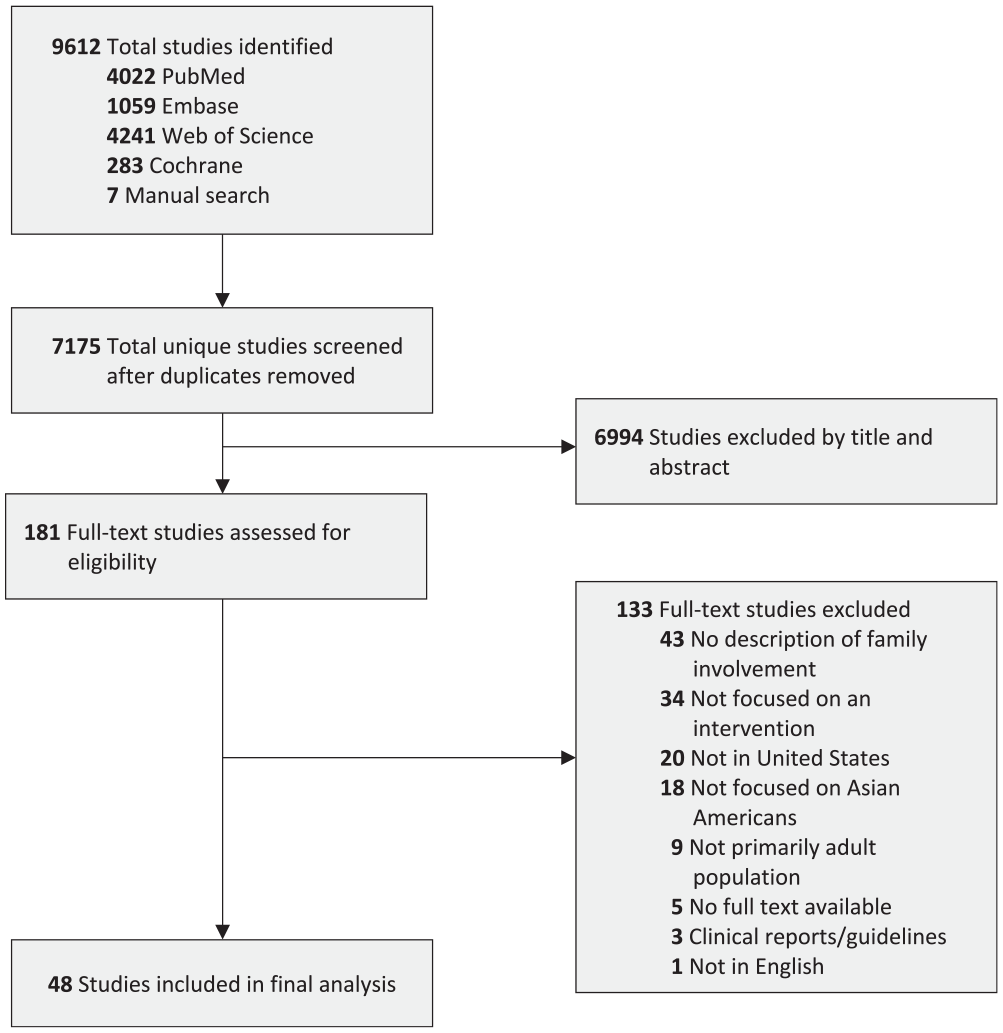
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of search strategy and final sample of studies included in a scoping review of Asian American health interventions involving family members as of 2021.
All study team members collectively reviewed iterative samples of 50-100 articles identified in the initial search; upon reaching 95% agreement on the inclusion or exclusion of articles within a sample of at least 100, each team member independently reviewed the remaining articles for inclusion. Two independent reviewers conducted full-text assessments to determine final inclusion (with a third acting as a tiebreaker). Two reviewers independently extracted data from included articles, and a third reviewer consolidated these data, including information on participant and intervention characteristics, outcomes, and a description of family involvement.
Results
Study Characteristics
Of the 7175 articles screened, 181 received full-text assessments, resulting in a final study sample of 48 (Figure 1). Studies included data from randomized controlled trials,25-38 quasi-experimental studies,39-56 protocols or trial registries,57-63 program evaluations,64-67 and developmental or usability studies.68-72
Studies spanned a 26-year time frame (1995-2021) and were conducted across at least a dozen US states; a substantial proportion (n = 21; 44%) were conducted in California (Table). Most studies involved Chinese (n = 26; 54%) populations, and intervention aims ranged from mental health and overall well-being (n = 12; 25%) to smoking cessation (n = 9; 19%). While most interventions did not specify the relationship of family members involved (n = 26; 54%), those that did reported the involvement of spouses (n = 17; 35%), parents or children (n = 14; 29%), and siblings (n = 4; 8%). Interventions with spousal involvement had proportionally less representation of participants aged ≥70 years (64% vs sample average of 75%) or those who were Southeast Asian (21% vs 31%), while interventions with parent/child involvement had proportionally less representation of participants aged 18-29 years (35% vs 46%) and those who were East Asian (59% vs 69%).
Characteristics of studies (N = 48) included in a final analysis in a scoping review of Asian American health interventions involving family members as of 2021
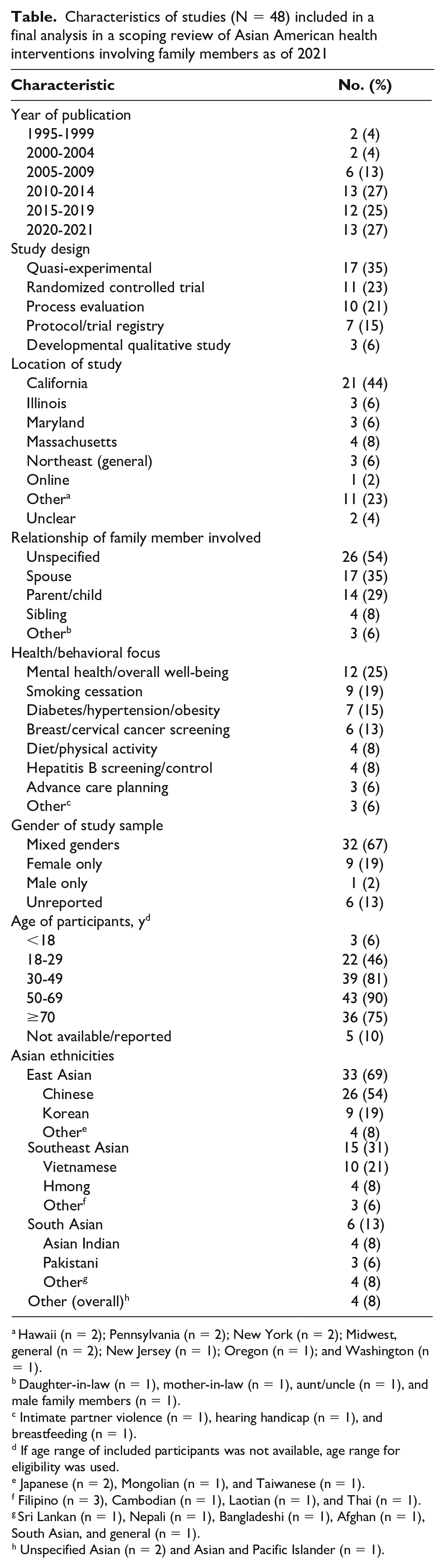
Hawaii (n = 2); Pennsylvania (n = 2); New York (n = 2); Midwest, general (n = 2); New Jersey (n = 1); Oregon (n = 1); and Washington (n = 1).
Daughter-in-law (n = 1), mother-in-law (n = 1), aunt/uncle (n = 1), and male family members (n = 1).
Intimate partner violence (n = 1), hearing handicap (n = 1), and breastfeeding (n = 1).
If age range of included participants was not available, age range for eligibility was used.
Japanese (n = 2), Mongolian (n = 1), and Taiwanese (n = 1).
Filipino (n = 3), Cambodian (n = 1), Laotian (n = 1), and Thai (n = 1).
Sri Lankan (n = 1), Nepali (n = 1), Bangladeshi (n = 1), Afghan (n = 1), South Asian, and general (n = 1).
Unspecified Asian (n = 2) and Asian and Pacific Islander (n = 1).
Family Involvement Across the 3 Stages of Interventions
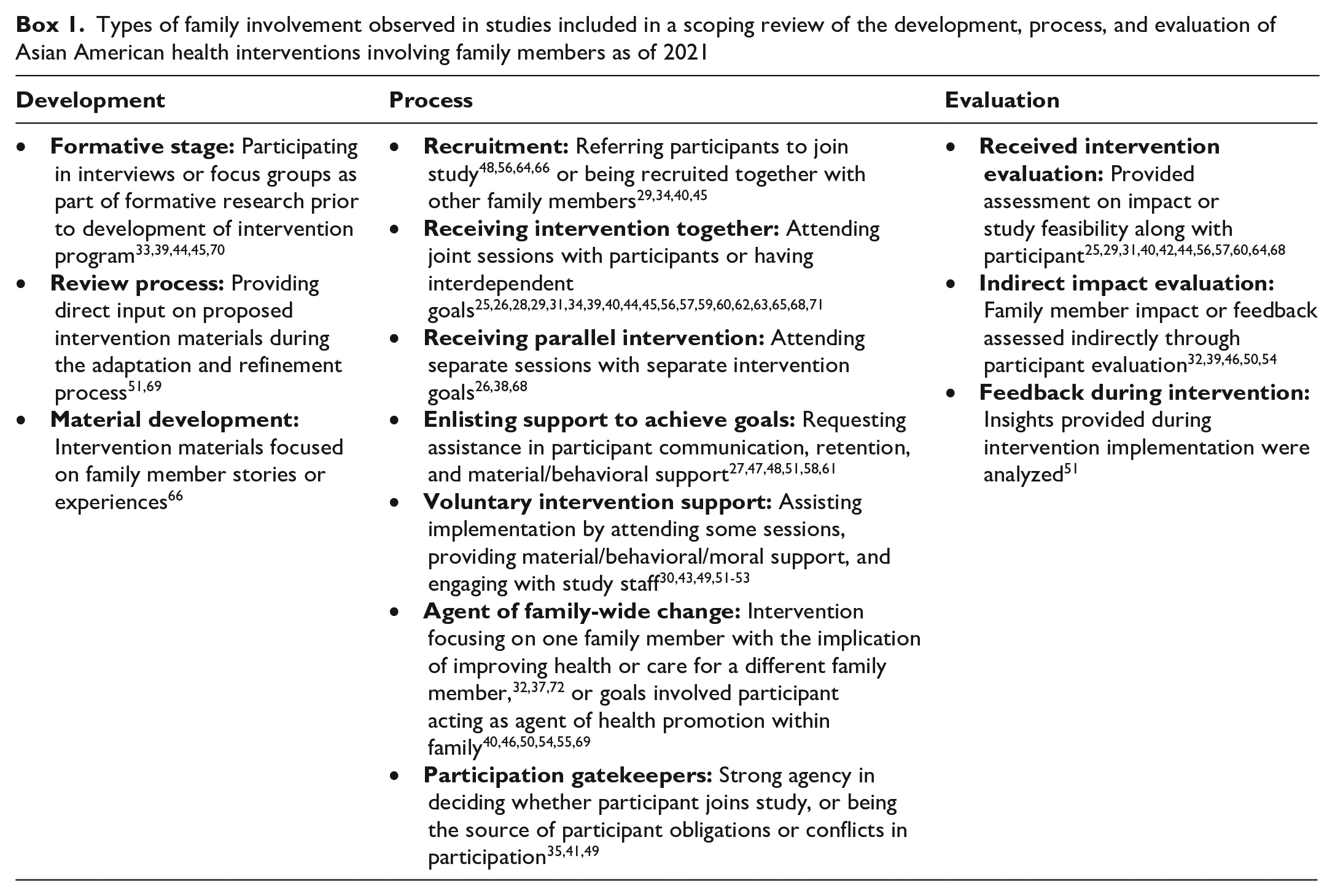
We observed different types of family member involvement in the development, process, and evaluation of included interventions (Box 1). The development stage included involvement in formative research or in the review or development of intervention materials. The process stage included involvement in recruitment, receipt of the same or a parallel intervention, provision of support during the intervention (either enlisted or offered voluntarily), or actual implementation of the intervention. Finally, the evaluation stage included providing direct or indirect feedback on the intervention.
Types of family involvement observed in studies included in a scoping review of the development, process, and evaluation of Asian American health interventions involving family members as of 2021
Intervention development
Relatively few (n = 8; 17%) included studies involved family members during the development and refinement of interventions. Much of this involvement was reflected through interviews or focus groups with family members or potential participants and centered on better understanding the health issue or behavior being intervened upon. However, some studies involved family members in the review of adaptation of preliminary intervention materials or protocols; Wang and Abbott conducted an individualized hypertension prevention program among Chinese adults in Hawaii, involving iterative tailoring of intervention content to participant needs. 51 In addition, family members were observed to contribute to the intervention materials themselves; Juon et al described a hepatitis B screening program in which family testimonials were included in intervention materials. 66
Intervention process
In most studies (n = 41; 85%), family members were involved in some aspect related to the processes or implementation of intervention activities. Family members were commonly the recipients of an intervention together with participants, such as dyadic interventions aimed at smoking cessation25,26,28,29,57 or breast cancer screening.34,56,62,63 In such interventions, family dyads attended intervention sessions together, set shared goals, or completed discussion and homework activities to foster mutual support in achieving shared intervention goals. Some interventions took a family-wide approach to health promotion, involving the promotion of a singular intervention to an entire family unit (eg, hepatitis B prevention interventions involving the promotion of screening across a family unit).65,71
Family members were also indirect recipients of some interventions, generally manifested in 1 of 2 ways. First, some interventions focused on the needs of a single member in a family unit, with the implication that improving their health would directly affect the needs of other family members. For example, some Asian American family caregiver interventions focused on caregiver health outcomes32,37,72 in consideration of their ramifications for both the caregiver and family member. Second, some interventions involved participants who were active health promoters within their families by providing them the tools to change a particular family dynamic. Chesla et al described a diabetes management intervention among Chinese adults that focused on training participants in family communication and conflict resolution to improve diabetes self-efficacy, knowledge, and distress. 50
Moreover, family involvement also occurred voluntarily, particularly in the form of moral support or encouragement by, for example, joining participants in sessions or changing behaviors with them.49,53 Even when voluntary, this involvement was at times crucial to an intervention’s impact; Tuttle and Dewey described a breastfeeding promotion program for Hmong women in which direct communication with participants and health care staff was minimal unless a family member was present to assist in translation. 30
Intervention evaluation
Family member involvement in the evaluation of intervention efficacy, fidelity, or implementation was most evidenced through postintervention assessments of how the family member experienced or was affected by the intervention.29,36 Moreover, family member effect or insight was also measured indirectly; as part of a hepatitis B screening intervention, participants were asked to indicate whether their family members, upon their referral, had tested positive for the virus. 46 Finally, first- and second-hand family member experiences were also documented throughout an intervention period. Wang and Abbott described a hypertension management intervention in which reflections on interactions made with family members were documented by researchers; the article also described the feedback of family members on the intervention content and its impact. 51
Effect of Family Member Involvement on Intervention Goals
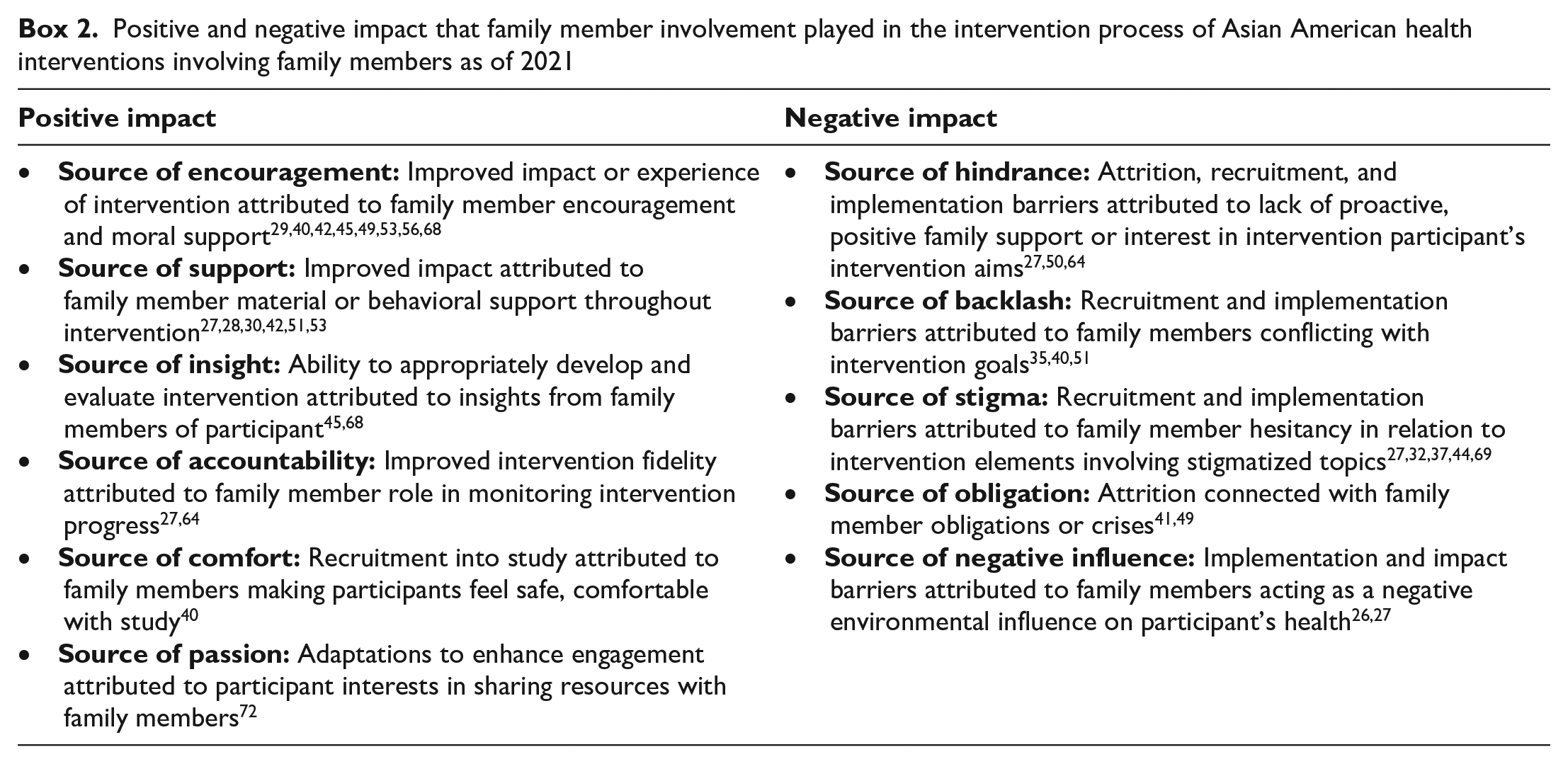
Aside from describing different ways family members were involved in an intervention, multiple studies also documented the effect of this involvement on achieving intervention goals, which we categorized into positive and negative effects (Box 2).
Positive and negative impact that family member involvement played in the intervention process of Asian American health interventions involving family members as of 2021
Positive impact on intervention goals
The positive impact of family members was particularly evidenced through their roles as sources of emotional encouragement and behavioral support for participants. Intervention fidelity was also connected with the involvement of family members; in tobacco cessation interventions for Korean and Chinese Americans, the wives of participants were observed to play important roles in monitoring their adherence to the intervention.27,36 Family members were also credited with bringing important insights during different stages of the intervention; a community-based advocacy and learning program for Hmong refugees credited the involvement of family members with uncovering many unmet needs of participants throughout the intervention. 45 Finally, the trust and close bond with family members also manifested positively in interventions. Kung et al described a family psychoeducation intervention for Chinese Americans with schizophrenia in which 1 participant required the accompaniment of her daughter to sessions because she was a “relatively new immigrant who needed the reassurance from her more educated daughter to feel ‘safe’ about the program and the study.” 40
Negative impact on intervention goals
Multiple studies also documented family members playing a detrimental role in implementing the intervention or achieving its desired impact. For example, lack of family emotional support was associated with attrition in a study on diabetes management among Chinese Americans. 50 At times, family members resisted intervention implementation; Lee-Lin et al described a breast cancer screening intervention for Chinese Americans in which a participant’s mammogram appointment was canceled by her daughter because of concern about the participant’s “old age.” 35 Stigmatization of intervention topics within families was also observed; a recruited individual in a caregiver intervention declined to participate as a result of not wanting to talk with the family member who had dementia.32,37 Finally, family members at times acted as negative environmental influences; the ability of Korean American women to achieve intervention goals in a smoking cessation intervention was substantially limited because many of their husbands smoked and were not interested in quitting. 27
Discussion
Family involvement was observed to play a powerful role in diverse interventions aimed at improving the health of Asian American communities (Figure 2). Analyzing involvement mechanisms across the sample revealed multiple methods of systematic family member involvement across various intervention stages. Family involvement may occur in 1 or multiples stages of an intervention and could also involve the simultaneous participation of the participant. For example, formative research or review of intervention materials with family members may occur with the participant. However, regardless of where, when, why, and how family members are involved in an intervention, it is important to consider that this involvement may have either a positive or negative impact on the ability of the intervention to meet its goals. Documentation and assessments conducted during the development, process, and evaluation of an intervention are, thus, crucial to reveal the potentially multifaceted implications of family involvement in Asian American health interventions.
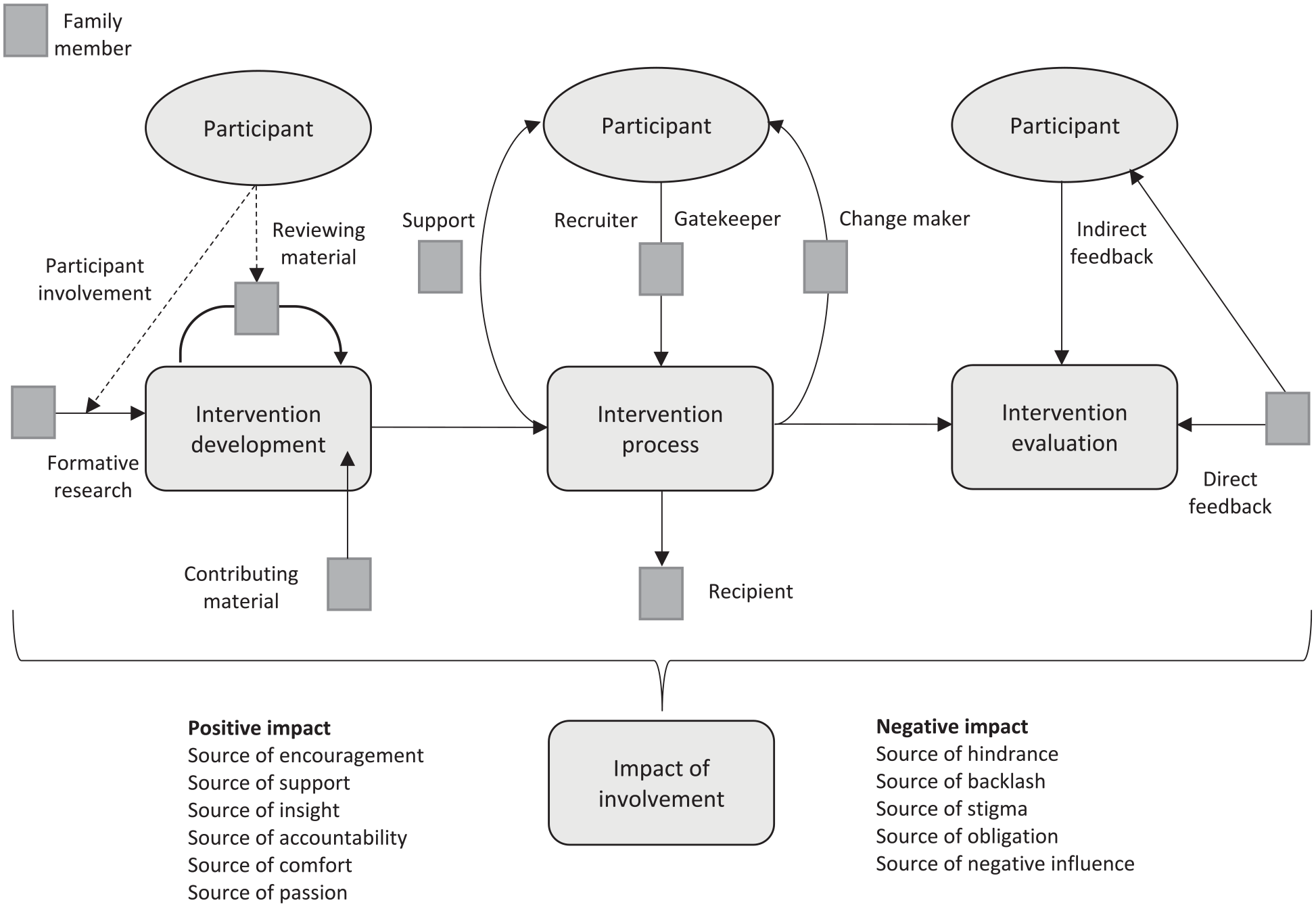
Conceptual model of methods and impact of family involvement in Asian American health interventions involving family members as of 2021. Solid-filled arrowed lines indicate involvement of a family member, whereas dotted arrowed lines describe when participants themselves may also play a role within a particular type of family member intervention involvement. An arrow going through a family member symbolizes their strong agency or responsibility in the type of involvement (eg, as a changemaker, recruiter, or gatekeeper), whereas an arrow in close proximity to the family member symbolizes a more secondary, optional, or voluntary type of involvement (eg, as support).
While East and Southeast Asian populations were strongly represented in the study sample, few studies included or focused on South Asians. South Asians are now one of the fastest growing subgroups of Asian Americans, increasing 40% in size from 2010 to 2017, 73 and they have a disproportionate share of chronic diseases (such as diabetes and hypertension) compared with other Asian American subgroups.2,74 Given that family engagement was also influential in chronic disease interventions, further family-involved intervention efforts aimed at South Asian health needs are warranted.
Moreover, most interventions focused on the health of older Asian Americans (eg, programs involving caregivers). However, attention is increasing on the family role in the health of young adult or second-generation Asian Americans, who also face a growing range of complex mental and physical health issues.75,76 The experiences of socialization and acculturation are different for young and older Asian Americans, which may contribute to unique implications in how best to involve family members and their biggest domains of influence75-77; further efforts to systematically document the development, process, and evaluation of family member involvement in young Asian American adult interventions is needed.
Limitations
While a strength of this study was its inclusion of diverse article types, health issues, and intervention models to comprehensively assess diverse types of family member involvements in Asian American health interventions, some limitations must be acknowledged. First, some Asian American interventions may have involved participant family members but did not explicitly report on this involvement, limiting the evaluation of such interventions. Second, in many studies, family member involvement was documented briefly; we found no details on scope, method, or impact, similarly limiting the ability to provide further nuanced insights. Third, unlike systematic reviews, evaluating study quality is not a primary aim of scoping reviews (which are exploratory), and, thus, coupled with the heterogeneity of the included studies, we did not conduct a formal quality assessment.21,78
Public Health Implications
This review highlights diverse ways in which types of family members can be involved in interventions. Although most interventions did not specify the relationship of involved family members, those that did largely focused on spousal and parent/child relationships. A unique facet of the Asian American experience is the strong connectivity with family members traditionally considered to be “extended,” such as grandparents, cousins, or aunts and uncles, often a result of living in multigenerational homes or principles of Asian American familism.16,79,80 Grandparents, for example, have been observed 81 to play a caregiving role in Asian American communities similar to that of parents and have been observed to substantially influence family dietary behaviors in multigenerational Asian households. 82
This review also provided preliminary insights into age- and ethnicity-related disparities across interventions involving either spouses or parents/children, much of which was connected with different interventional aims or culture-specific behavioral dynamics. For example, older Asian American adult interventions focusing on caregiving or involving technology often involved adult children, given their greater physical or technical capacity to assist with the intervention. Moreover, spousal involvement was particularly common among smoking interventions for Chinese and Vietnamese men, which may be a result of women being substantially less likely to smoke than men in East and Southeast Asia. 83 However, while the observed differences in spousal and parent/child involvement may in part be explained by these interventional aims, further efforts are needed to expand the types of family members involved in Asian American interventions (eg, extended family or siblings) to make stronger conclusions on the implications of engaging with spouses, parents, or other family members in interventions (across diverse ages and Asian American ethnicities).
Intervention models involving family members as agents of change within their households were explored in some studies and have also been identified as an important area for innovation in past research. 7 The close bond and trust placed with family members can be an asset to an intervention’s success, yet less is known about the direct use of these relationships by having family members themselves be the primary implementation agent. 7 Among the few studies that involved an indirect intervention to family members through the participant, efforts were largely centered on advocating or providing space for participants to engage with family members and promote healthy behaviors as secondary or intermediate goals. However, efforts to evaluate the impact of family member–implemented interventions were less explored. Examples from other Asian settings can be informative in guiding novel intervention development. He et al documented the protocol of an innovative school-based salt reduction program that used the influence of parent–child relationships; this study provided a salt education program to Chinese children, empowering them to educate their family members and persuade them to also reduce their salt intake. 84 Importantly, this intervention involved the comprehensive assessment of impact for both the intervention recipients and family members 84 ; similar models of family member–led interventions warrant further exploration in Asian American settings.
Finally, evidence of both positive and negative influences of family member involvement among Asian Americans emphasizes the need to consider how an intervention can be adapted to maximize the benefit while minimizing the barriers that family member involvement may entail. For example, many impact domains (eg, as sources of encouragement, support, comfort, passion, hindrance, or backlash) can be contingent on existing dynamics between a participant and family members. As such, proactive involvement of family members may also entail an action plan to prepare for various scenarios (including those in which a family member may undermine intervention goals), formative research to understand existing family dynamics in relation to a particular health issue, 69 or the inclusion of communication and conflict-resolution capacity building as part of the intervention. 50 Similarly, generational differences between family members may also contribute to the ability to engage their involvement in an intervention effectively and should be considered. For example, the level of comfort in discussing sexual health among young adults can differ when interacting with parents versus siblings. 85
Through an analysis of diverse Asian American health interventions, we documented family member involvement across intervention development, process, and evaluation. This involvement had a substantial influence on intervention success. We drew on various methods of involvement to synthesize a conceptual model that can help inform new ways of involving family members in diverse types of Asian American health interventions. We identified pathways for future family-involved interventions, including expansion of study populations (notably South Asians and young Asian American adults), innovations in the types of family members involved (eg, extended family) and their method of involvement (eg, family members as implementation agents), and preparing interventions to better harness the benefits and mitigate any barriers related to family member involvement. With greater exploration of family-involved interventions, future research can build on the findings of this scoping review by systematically analyzing whether certain types of family member involvement are most associated with improvements in the effectiveness or sustainability of health interventions and differences in the suitability of involvement methods across interventional structures, health objectives, or Asian American ethnicities.
Supplemental Material
sj-docx-1-phr-10.1177_00333549221138851 – Supplemental material for Family Involvement in Asian American Health Interventions: A Scoping Review and Conceptual Model
Supplemental material, sj-docx-1-phr-10.1177_00333549221138851 for Family Involvement in Asian American Health Interventions: A Scoping Review and Conceptual Model by Shahmir H. Ali, Farhan M. Mohsin, Rejowana Rouf, Ravi Parekh, Biswadeep Dhar, Gurket Kaur, Niyati Parekh, Nadia S. Islam and Ralph J. DiClemente in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.