
Abstract
More than 500 single-room occupancy hotels (SROs), a type of low-cost congregate housing with shared bathrooms and kitchens, are available in San Francisco. SRO residents include essential workers, people with disabilities, and multigenerational immigrant families. In March 2020, with increasing concerns about the potential for rapid transmission of COVID-19 among a population with disproportionate rates of comorbidity, poor access to care, and inability to self-isolate, the San Francisco Department of Public Health formed an SRO outbreak response team to identify and contain COVID-19 clusters in this congregate residential setting. Using address-matching geocoding, the team conducted active surveillance to identify new cases and outbreaks of COVID-19 at SROs. An outbreak was defined as 3 separate households in the SRO with a positive test result for COVID-19. From March 2020 through February 2021, the SRO outbreak response team conducted on-site mass testing of all residents at 52 SROs with outbreaks identified through geocoding. The rate of positive COVID-19 tests was significantly higher at SROs with outbreaks than at SROs without outbreaks (12.7% vs 6.4%; P < .001). From March through May 2020, the rate of COVID-19 cases among SRO residents was higher than among residents of other settings (ie, non–SRO residents), before decreasing and remaining at an equal level to non–SRO residents during later periods of 2020. The annual case fatality rate for SRO residents and non–SRO residents was similar (1.8% vs 1.5%). This approach identified outbreaks in a setting at high risk of COVID-19 and facilitated rapid deployment of resources. The geocoding surveillance approach could be used for other diseases and in any setting for which a list of addresses is available.
Across the United States, rates of COVID-19 infection are highest in neighborhoods with people with low incomes and high proportions of people from racial and ethnic minority groups.1-4 Crowded, multigenerational housing conditions have been an important driver of these disparities.5,6 In San Francisco, single-room occupancy hotels (known as SROs) make up the largest supply of low-cost housing; SRO residents include older adults, adults with disabilities, people living with HIV, migrant workers, and children. 7 Most SROs in San Francisco were built in the early 20th century; have communal toilets, showers, and kitchens; and are located in neighborhoods with high rates of chronic health conditions that increase the risk of COVID-19 morbidity, 8 including asthma, diabetes, and hypertension. 7 Although intended to house 1 or 2 individuals, a single 8 × 10-foot room in an SRO is often shared by multigenerational families or workers with low incomes. 7
Given the shared rooms and facilities and often poorly ventilated conditions in SROs, SRO residents are less able than people in traditional housing (ie, non–SRO residents) to adhere to and benefit from nonpharmaceutical interventions (NPIs), for example, social distancing and sheltering in place, which were the primary tools for COVID-19 infection prevention in the prevaccine era. To guide the deployment of preventive interventions in SROs, the San Francisco Department of Public Health (SFDPH) implemented a geocoding strategy to proactively identify COVID-19 outbreaks in SROs. Geocoding has been used to identify influenza outbreaks in long-term care facilities 9 but has not previously been used as part of communicable disease surveillance and response in SROs.
Purpose
At the onset of the COVID-19 pandemic, in March 2020, SFDPH’s COVID Command Center established an SRO outbreak response team, and in May 2020, the San Francisco Board of Supervisors passed an emergency ordinance aimed at preventing COVID-19 in SROs. 10 The SRO outbreak response team aimed to identify SRO outbreaks with the use of geocoding, deploy outbreak-responsive field testing to identify cases, and use results to support isolation and quarantine to mitigate spread. We describe the SRO outbreak response team’s multipronged response to COVID-19 prevention and outbreak control and the epidemiology of COVID-19 among people living in SROs, during a period that preceded widespread availability of COVID-19 vaccines in San Francisco.
Methods
COVID-19 Case Identification and Investigation
All laboratory-based COVID-19 test results among San Francisco residents are mandated to be reported to the SFDPH (California Code of Regulations §2500, §2593, §2641.5-2643.20, and §2800-2812 reportable diseases and conditions). As of March 2020, there were 521 SROs in San Francisco according to a list maintained by the San Francisco Department of Building Inspection. 11 The SRO outbreak response team geocoded and geospatially matched the addresses of all newly reported COVID-19 test results to that list. 12 First, after the SRO outbreak response team deidentified the address data within a secure structured query language (SQL) server within the SFDPH, the team extracted data using feature manipulation engine software and geocoded the data using ArcGIS World Geocoder (Esri) and the Geocoding Application Programming Interface (Google). Once the SRO outbreak response team uploaded the geocoded data back to the SQL server, an automated SQL server agent job notified the team about all people with positive test results who resided at addresses matching SRO buildings.
For each new COVID-19 case during the analytic period (from March 1, 2020, through February 28, 2021), a case investigator elicited information on close contacts and referred the close contacts to testing. 13 For people with positive COVID-19 test results who were unable to safely isolate at home, including residents who shared a bedroom or bathroom, the SRO outbreak response team offered referrals to an isolation and quarantine hotel in San Francisco and to a wage-replacement program from the San Francisco Office of Economic and Workforce Development. 14 Household contacts of SRO residents were also referred to these hotels, when available. SRO residents with positive COVID-19 test results and their contacts who declined rooms at isolation and quarantine hotels were offered delivery of food and other supplies.
SRO Outbreak Response Team Response Protocol
The SRO outbreak response team comprised multidisciplinary staff members trained in case investigation, contact tracing, and field-based outreach and education and included nurses, social workers, health workers, and staff from partnering community-based organizations. The team reviewed daily the automated list of all newly diagnosed COVID-19 cases at SRO addresses. When a first COVID-19 case was identified at an SRO address, team staff notified the property manager (without disclosing identifying information) and provided guidance about mitigating the spread of COVID-19 in SROs. 15 When members of 3 households in an SRO building received a positive test result for COVID-19 within 14 days, the building was identified as experiencing an outbreak, which initiated the mobilization of field-based staff to conduct voluntary on-site testing and provide residents with COVID-19 education, supplies (eg, face masks, hand sanitizer), and referrals to resources. During on-site testing, field team nurses collected swabs for polymerase chain reaction testing for SARS-CoV-2. Additional rounds of on-site testing were conducted if COVID-19 cases suggested within-building transmission.
An outbreak was deemed to be resolved when 28 days passed with no new cases of COVID-19 among residents in the building. An SRO could have multiple outbreaks during the analytic period. The SRO outbreak response team considered all COVID-19 cases identified from the date of an on-site SRO testing event until the outbreak had resolved as “SRO outbreak cases,” regardless of whether residents were tested on-site or at another location.
Outcome Measures and Data Analysis
We selected the analytic period as the first year of the COVID-19 pandemic because NPIs, case findings, and isolation and quarantine were the primary tools for the mitigation of COVID-19 and COVID-19 vaccines were not yet widely available. For our analyses, we used both San Francisco citywide laboratory test result data and information obtained during the case investigation interview. We identified 3 groups of COVID-19 cases in San Francisco for our comparison: (1) all COVID-19 cases, (2) COVID-19 cases among people who resided at an SRO while that building was experiencing an outbreak (SRO outbreak cases), and (3) all COVID-19 cases among people who resided at an SRO while that building was not experiencing an outbreak (SRO non-outbreak cases). Each person was counted as a case only once.
We used logistic regression models to compare COVID-19 cases among SRO residents with COVID-19 cases among non–SRO residents and COVID-19 cases in SRO outbreak buildings with COVID-19 cases in SRO non-outbreak buildings, by demographic characteristics and comorbidities. We used robust SEs in all models to account for case clustering by address. We compared testing, case, and death rates of SRO residents with those of all San Francisco residents, with San Francisco population of 870 044 used as a denominator. 16 We calculated a rate range for SRO residents based on an assumed SRO resident population of 18 000 to 28 000 people, which we estimated based on a 2016 report that was compared with an updated list from 2021 of SROs registered with the San Francisco Department of Building Inspection (D. Morris, BS, email communication, May 2021). 7
We compared rates of COVID-19 incidence (diagnosed cases per 100 000 population) for all COVID-19 cases among San Francisco residents versus COVID-19 cases among SRO residents during four 3-month periods: spring (March through May 2020), summer (June through August 2020), autumn (September through November 2020), and winter (December 2020 through February 2021). We described change over time as relative to the spring period. We considered rates with nonoverlapping 95% CIs to be significantly different. To assess for differences in incidence attributable to differential rates of testing, we compared the 3-month testing rate (number of tests per 1000 population) among SRO residents versus San Francisco residents. We calculated only annual case fatality rates (deaths among diagnosed cases) and death rates (deaths per 100 000 population) because rates with fewer than 20 observations are considered unstable. 17 Given that each person could be diagnosed as a case only once, we adjusted the denominators for the summer through winter period to reflect the population at risk by subtracting cases already diagnosed from the population count.
To describe the efficiency of outbreak-responsive on-site testing in SROs, we compared the 3-month test positivity rate among 3 groups: (1) non–SRO residents, (2) SRO residents in buildings with an outbreak where the SRO outbreak response team conducted on-site testing, and (3) SRO residents living in buildings with no outbreak. We calculated the 3-month test positivity rate as follows: number of positive tests/(number of positive tests + number of negative tests). We calculated test positivity from all conclusive tests reported to SFDPH, which may have included multiple test results per person. This work was conducted as part of SFDPH COVID-19 surveillance; per SFDPH guidelines, institutional review board approval was not required (45 CFR §46.102[l][2]).
Outcomes
Among 843 302 COVID-19 test results reported to SFDPH during the analytic period, 34 155 were positive for COVID-19. During this period, 525 people died from COVID-19; 64% of deaths occurred during the winter period.
COVID-19 Testing, Cases, Deaths, and Test Positivity at Outbreak Sites
In spring 2020, the 3-month testing rate (number of tests per 1000 population) was higher among SRO residents than among San Francisco residents, ranging from 46.8 (95% CI, 44.3-49.4) to 72.8 (95% CI, 68.9-76.8) among SRO residents versus 33.8 (95% CI, 33.4-34.2) among San Francisco residents. During the summer and autumn periods, the 3-month testing rate for SRO residents was similar to the San Francisco citywide testing rate. In the winter period, the 3-month testing rate among SRO residents ranged from 360.9 (95% CI, 353.9-368.0) to 561.4 (95% CI, 550.5-572.4), which was lower than the citywide testing rate of 597.9 (95% CI, 596.3-599.6).
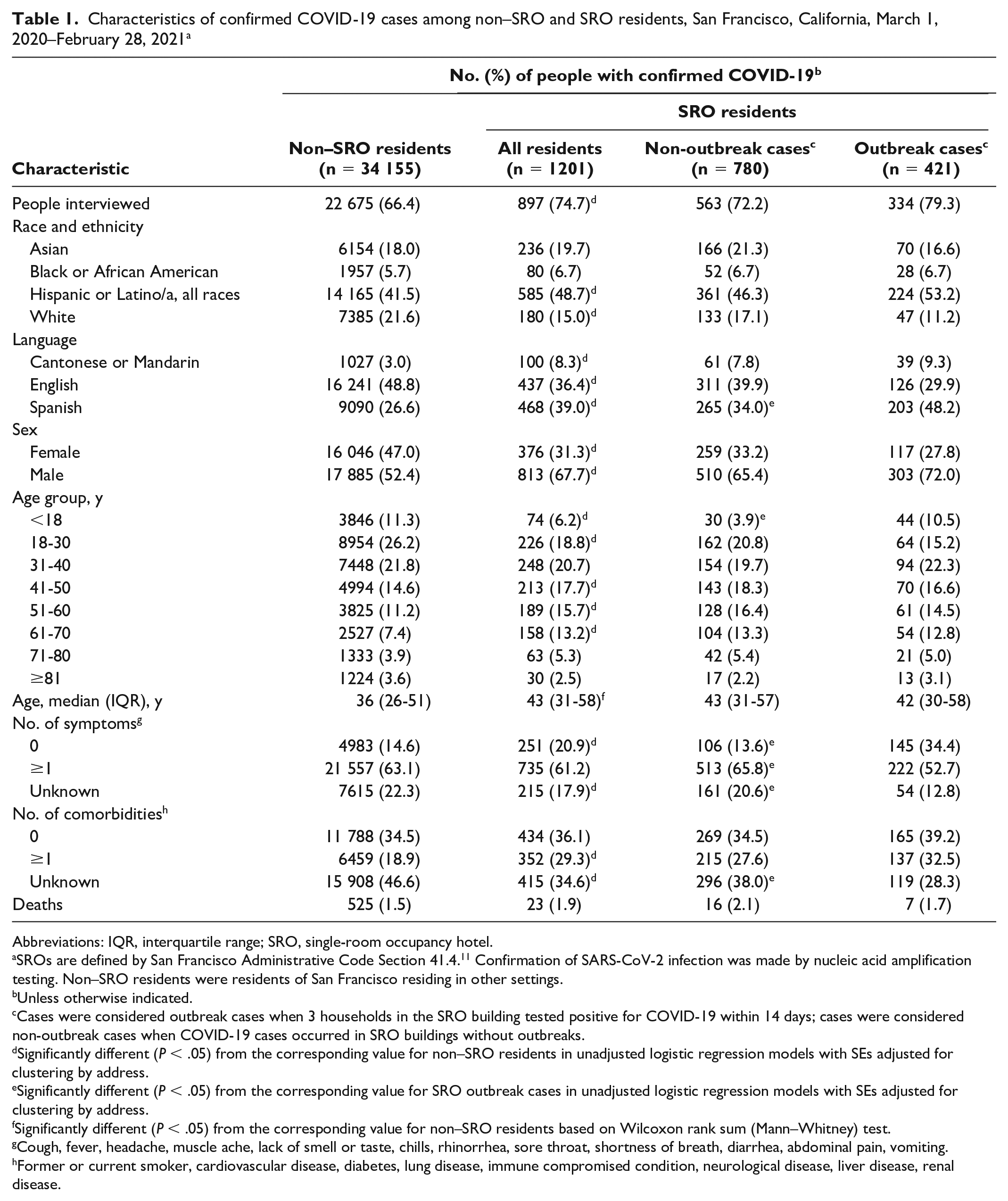
During the analytic period, the SRO outbreak response team confirmed 1201 cases of COVID-19 in SRO residents in 265 distinct SROs. SRO residents experienced 3 waves of infection that paralleled the overall epidemiologic curve for San Francisco (Figure). Compared with the overall number of COVID-19 cases in San Francisco, and reflective of the SRO population in general, SRO residents with COVID-19 were older and significantly more likely to be male, be Latinx, and speak Spanish, Cantonese, or Mandarin. SRO residents with COVID-19 were more likely than non–SRO residents to have 1 or more comorbidities and be asymptomatic at the time of the case interview (Table 1). Among SRO residents, SRO outbreak cases did not differ from SRO non-outbreak cases in median age, sex, race and ethnicity, or known comorbidity, but were more likely to speak Spanish.
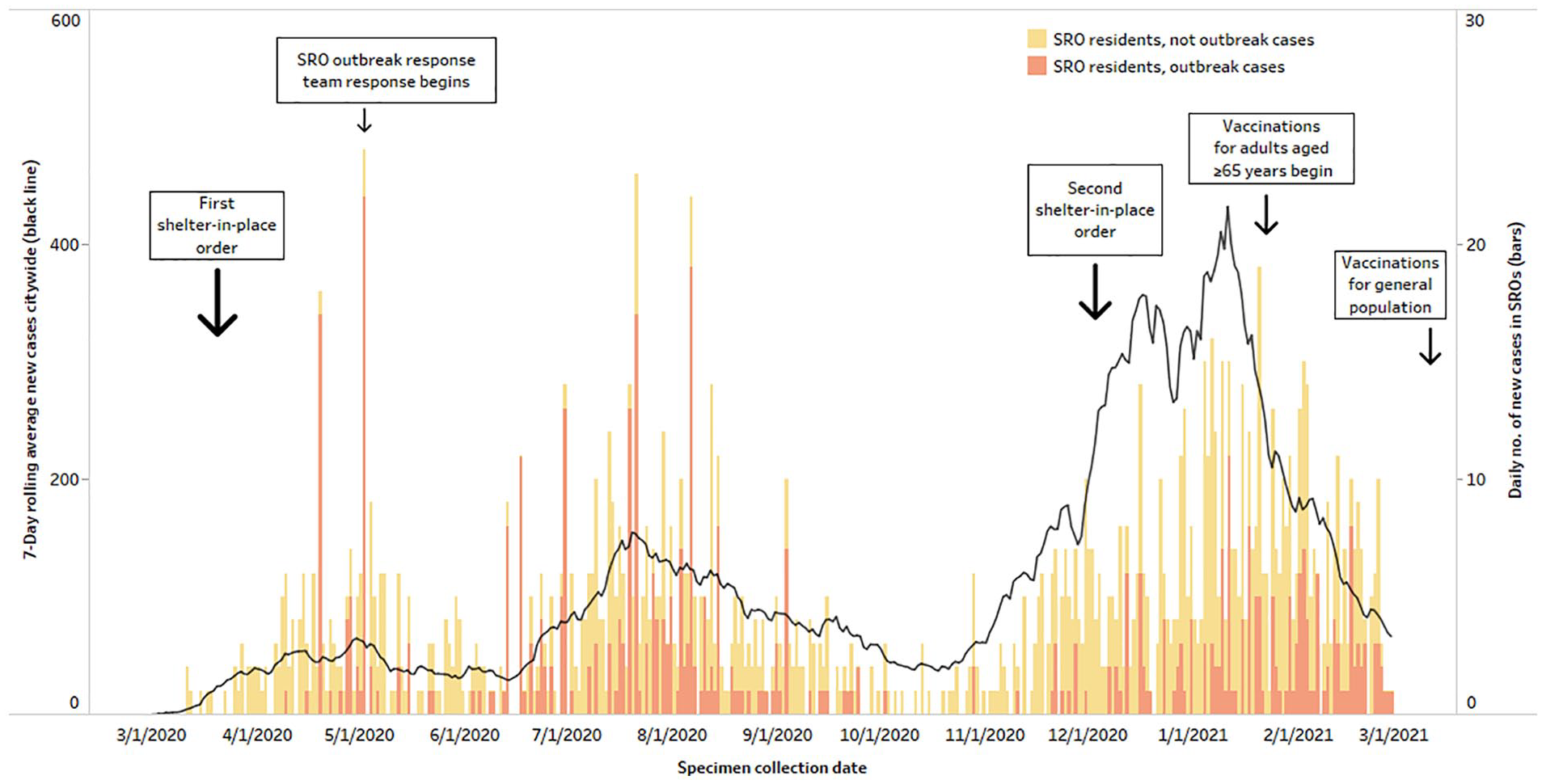
Seven-day rolling average of new COVID-19 cases in San Francisco, California, and number of daily outbreak and non-outbreak cases among single-room occupancy hotel (SRO) residents, March 1, 2020–February 28, 2021. Data source: DataSF. 12
Characteristics of confirmed COVID-19 cases among non–SRO and SRO residents, San Francisco, California, March 1, 2020–February 28, 2021 a
Abbreviations: IQR, interquartile range; SRO, single-room occupancy hotel.
SROs are defined by San Francisco Administrative Code Section 41.4. 11 Confirmation of SARS-CoV-2 infection was made by nucleic acid amplification testing. Non–SRO residents were residents of San Francisco residing in other settings.
Unless otherwise indicated.
Cases were considered outbreak cases when 3 households in the SRO building tested positive for COVID-19 within 14 days; cases were considered non-outbreak cases when COVID-19 cases occurred in SRO buildings without outbreaks.
Significantly different (P < .05) from the corresponding value for non–SRO residents in unadjusted logistic regression models with SEs adjusted for clustering by address.
Significantly different (P < .05) from the corresponding value for SRO outbreak cases in unadjusted logistic regression models with SEs adjusted for clustering by address.
Significantly different (P < .05) from the corresponding value for non–SRO residents based on Wilcoxon rank sum (Mann–Whitney) test.
Cough, fever, headache, muscle ache, lack of smell or taste, chills, rhinorrhea, sore throat, shortness of breath, diarrhea, abdominal pain, vomiting.
Former or current smoker, cardiovascular disease, diabetes, lung disease, immune compromised condition, neurological disease, liver disease, renal disease.
Although SRO residents accounted for 2.1% to 3.2% of the total San Francisco population, in spring 2020, they represented 7.2% of people in San Francisco diagnosed with COVID-19. The proportion of COVID-19 cases among SRO residents decreased during the analytic period (4.8% in summer, 2.4% in autumn, and 2.9% in winter). The 3-month case rate per 100 000 population in spring 2020 was significantly higher among SRO residents (671.4 [95% CI, 575.4-767.4] to 1044.4 [95% CI, 895.1-1193.7]) than among San Francisco residents overall (301.9 [95% CI, 290.4-313.5]). For the remainder of the analytic period, the 3-month case rate among SRO residents was lower or not significantly different from San Francisco residents, based on nonoverlapping 95% CIs (data not shown).
The proportion of deaths from COVID-19 among SRO residents, by period, was 5.8% in spring, 7.5% in summer, 2.7% in autumn, and 3.6% in winter. During the entire analytic period, the case fatality rate among SRO residents was 1.8% (95% CI, 1.1%-2.6%) compared with 1.5% (95% CI, 1.4%-1.7%) citywide. The death rate per 100 000 population was either the same or higher among SRO residents (78.6 [95% CI, 45.7-111.4] to 122.2 [95% CI, 71.1-173.3]) compared with San Francisco residents (60.3 [95% CI, 55.2-65.5]). During the worst COVID-19 surge of the year, if the upper limit of the citywide death rate of 39.1 (95% CI, 34.9-43.3) (ie, 43.3 deaths per 100 000 people) was applied to the upper estimate of the SRO population (28 000), at most 12 deaths would be expected. During this period, 12 residents of SROs had died.
The SRO outbreak response team responded to outbreaks at 52 SROs, which involved 421 cases of COVID-19 (35% of all SRO resident cases). The proportion of positive test results was consistently and significantly higher in outbreak SROs than in non-outbreak SROs and versus non–SRO residents throughout the analytic period (Table 2).
Average COVID-19 positivity rate by single-room occupancy hotel (SRO) residency and outbreak status, San Francisco, California, March 1, 2020–February 28, 2021 a
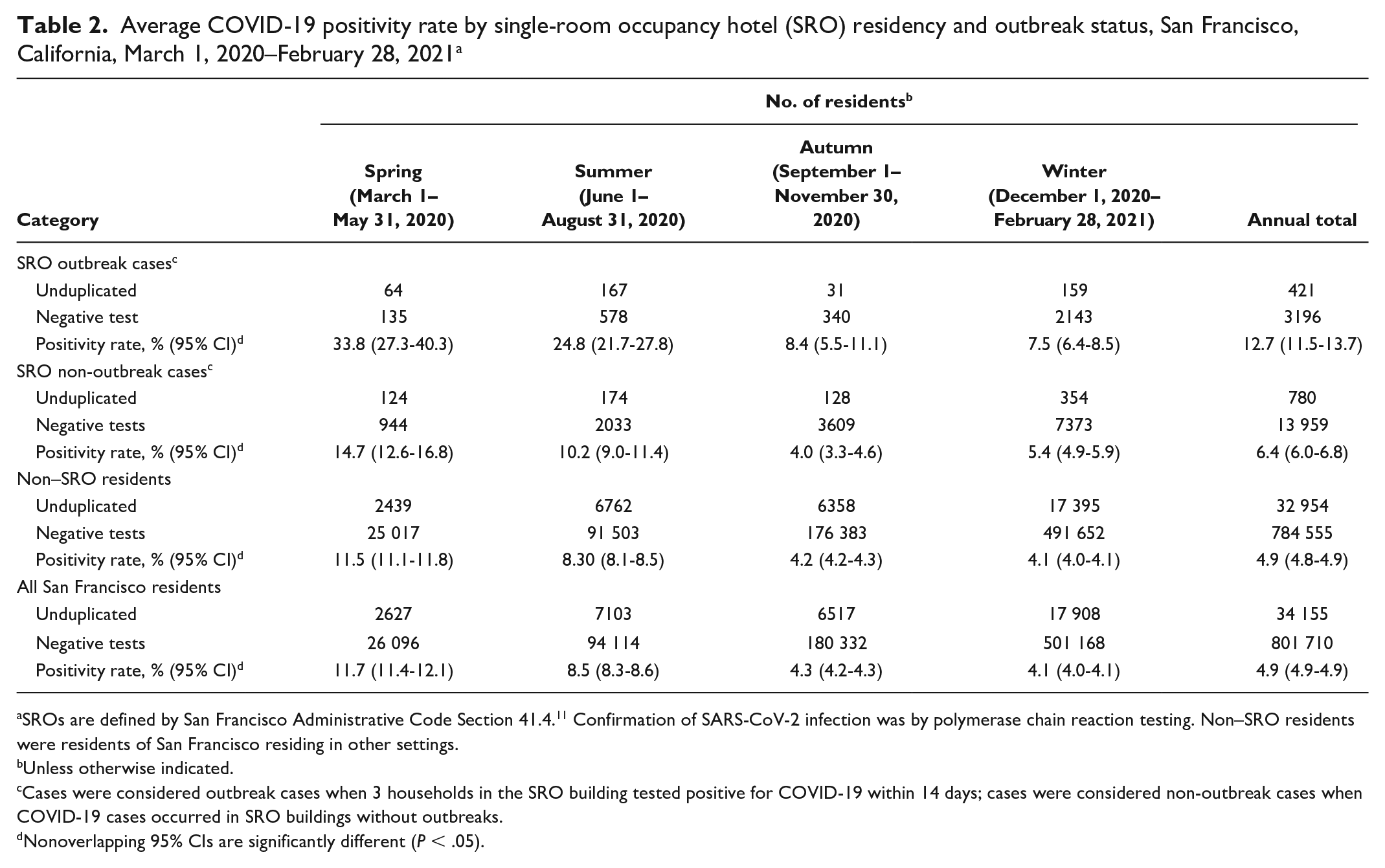
SROs are defined by San Francisco Administrative Code Section 41.4. 11 Confirmation of SARS-CoV-2 infection was by polymerase chain reaction testing. Non–SRO residents were residents of San Francisco residing in other settings.
Unless otherwise indicated.
Cases were considered outbreak cases when 3 households in the SRO building tested positive for COVID-19 within 14 days; cases were considered non-outbreak cases when COVID-19 cases occurred in SRO buildings without outbreaks.
Nonoverlapping 95% CIs are significantly different (P < .05).
Lessons Learned
Consistent with the concern that SRO residents would be at elevated risk for COVID-19 acquisition and morbidity, in spring 2020, SRO residents had a significantly higher case rate and represented a disproportionate number of COVID-19 deaths as compared with the general population in San Francisco. During this period, citywide shelter-in-place orders were in effect; however, because many SRO residents are essential workers living in a crowded congregate setting, the protective benefit of shelter-in-place was minimal in this population. For the remainder of the analytic period (through February 28, 2021) and despite 2 COVID-19 surges, a disparity in COVID-19 case rates for SRO residents did not occur. The relative incidence of COVID-19 and the proportion of COVID-19 deaths among SRO residents both declined after the first 3 months of the pandemic and was proportionate to the rate among the general population of San Francisco by winter 2021. The Latinx community in San Francisco was disproportionately affected by COVID-19, as reflected in the number of COVID-19 cases among SRO residents and SRO outbreak cases in particular. 18
The use of geocoding to identify SROs with outbreaks and rapidly deploy on-site testing enabled the SRO outbreak response team to promptly identify and isolate cases and quarantine contacts. The higher proportion of asymptomatic (vs symptomatic) COVID-19 cases among SRO residents suggested that an outbreak-responsive, mass testing strategy was effective in identifying people with presymptomatic or asymptomatic COVID-19 who might have experienced delayed diagnosis or none at all without this strategy. Modeling studies support the hypothesis that case finding and contact tracing, when combined with effective isolation and quarantine, can interrupt transmission chains and avert hospitalizations. 19
Bringing linguistically and culturally appropriate testing and prevention services to SROs is an effective way of reaching a population that is vulnerable to acquisition of COVID-19. The SRO outbreak response team and community-based partners provided services beyond testing, such as linkages to eviction prevention and delivery of food, diapers, and formula. A similar “Test to Care” model in San Francisco demonstrated that providing supportive services as part of a package with testing helped facilitate isolation and quarantine. 20
Because our study was an observational analysis, we had several unknowns with regard to the effects that the SRO outbreak response team had on stopping the spread of COVID-19 in SROs and minimizing COVID-19 morbidity and mortality among SRO residents; thus, we cannot claim that the SRO outbreak response team had a causal effect on the epidemiology of COVID-19 in SROs. Although the team encouraged NPIs (eg, social distancing, wearing face masks, seeking testing when symptomatic), we could not differentiate the impact of these NPIs on COVID-19 spread from other efforts of the SRO outbreak response team. Differential changes in testing behavior of SRO residents versus non–SRO residents may have contributed to changes in relative case rates over time. The 4 periods that we compared in this analysis combined months that had different case rates; thus, we may have underestimated magnitudes of differences between the periods. Because of the lack of precise information about the size and demographic characteristics of the SRO population during the analytic period, we could not estimate one rate for SRO residents or determine whether observed differences reflected characteristics of SRO residents in general or characteristics of the subgroup of SRO residents who became infected. Death rates were not age-adjusted, and rates calculated from small numbers of cases may be unstable. Some of the asymptomatic cases identified through mass testing likely represented previous infections rather than recent infections.
Geocoding of newly reported COVID-19 cases facilitates prompt identification of outbreaks in a congregate setting and targets deployment of mass testing, which is critical to controlling outbreaks. Although our group focused on SROs, these methods can be applied to any setting for which a list of addresses is available. This case study illustrates that it is possible to mobilize a multidisciplinary group to reach out to a diverse population at risk of infection and morbidity during a pandemic and provides a foundation for future public health work in this community.
Footnotes
Acknowledgements
The authors acknowledge the following for their participation in the design and implementation of the SRO outbreak response model in San Francisco: David Alfaro, Jessica Bloome, Melissa Brown, Anni Chung, Arianna Cunha, Hany DeLeon, Gregory Fletcher, Gen Fujioka, Michael Grealish, Rachel Grinstein, Elizabeth Imbert, Kara Inglis, Kathy King, Pat Kinley, Jason M. Lee, Kari Lee, Michael Liao, Omar Masry, Ramon Matos, Jamie Moore, Sunny Pak, Raul Peralta, Natalia Ramirez, Andy Scheer, Laura Slattery, Sarah Strieff, Amy Tang, Emily Valadao, Kelly Winter, Jiami Wu, Gina Yam, Jorge Zepeda, Jian Zhang, and Rain Zhang. We also appreciate the collaboration of the following community-based organizations: Alliance Health Project, Chinatown Community Development Center, Chinatown YMCA, Mission Neighborhood Resource Center, NICOS, and Self-Help for the Elderly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.