
Abstract
Adolescence, a critical and rapid stage of human development, requires innovative approaches in the provision of health care. With considerable mental health issues occurring among adolescents, an urgent need exists to address their mental and behavioral health. School-based health centers can provide an important safety net, particularly for young people who lack access to comprehensive and behavioral health care. We describe the design and implementation of behavioral health assessment, screening, and treatment services in a primary care school-based health center. We reviewed primary care and behavioral health measures as well as the challenges and lessons learned of this process. Five hundred and thirteen adolescents and young adults aged 14-19 years from an inner-city high school in South Mississippi were screened for behavioral health issues from January 2018 through March 2020, and all 133 adolescents deemed at risk for behavioral health issues received comprehensive health care. Lessons learned included the importance of recruiting behavioral health providers to ensure sufficient staff, establishing academic–practice arrangements to ensure funding, increasing student enrollment by improving the return rate of consent for care, and enhancing data collection through process automation. This case study may help inform the design and implementation of integrated primary and behavioral health care in school-based health centers.
Adolescence calls for innovative health care approaches. 1 Mental health disorders are the most common childhood disorders. Depression is the fourth leading cause of illness and disability among adolescents in the United States 2 ; 1 in 15 US high school students attempts suicide annually. 3 Almost half (49.5%) of adolescents meet diagnostic criteria for a behavioral health disorder, including mood or attention-deficit disorders and substance use. 4 Compared with adolescents who have a positive outlook on life, adolescents with a poor outlook on life are more likely to take part in behaviors that put them at high risk for compromised health and show the propensity for many high-risk health behaviors and behavioral health, problems that often overlap. 5 Persistent feelings of depression, anxiety, and inattention are often associated with early alcohol and drug use among adolescents. 6
Young people living in poverty often face stress related to food insecurity and violence, contributing to poor mental health and academic outcomes. Chronic childhood trauma, poverty, latent neighborhood violence, and disparities in health care access contribute to poor behavioral health and academic outcomes. 7 Adolescents in racial and ethnic minority populations face additional health risks, such as being less likely to have a consistent medical home and more likely to experience chronic stressor issues in accessing health care than non-Hispanic White adolescents.8,9
In the United States, an urgent need exists to address mental health, which has been exacerbated by COVID-19. School-based health centers (SBHCs) provide an important primary care safety net, particularly for young people living in areas with a shortage of health care providers.9,10 About 40 years ago, the first SBHCs addressed contraceptive needs of adolescents and were later recognized as locations to improve access to primary care.11,12 As school-related mental health needs increased, SBHCs integrated mental health services, which may include screening, diagnosing, and treating common mental health illnesses and substance use disorders as well as promoting behaviors that affect an individual’s overall well-being. 13 Historically, nurse-led SBHCs have been successful in addressing the health needs of young people and are positioned to identify mental health problems, provide treatment, and make appropriate referrals. 14 Behavioral health services in SBHCs can reduce depressive episodes, decrease suicidal ideation, and improve level of functioning.9,15 -17 In addition, adolescents attending a school where an SBHC is present are 10 times more likely to seek care for behavioral health and substance use than adolescents attending schools that do not have an SBHC. 9 SBHCs can be used to provide effective, comprehensive, and integrated primary and behavioral health care.
Background
Many children and adolescents in Mississippi have severe and persistent behavioral health needs. 18 In 2017, almost 11% of adolescents in Mississippi reported a major depressive episode, while 18.2% of adolescent girls aged 13-17 years reported a depressive episode. 19 During 2019, about 19% of Mississippi teenagers aged 13-17 years considered suicide and 9% attempted suicide. 18 In 2019, nearly 9000 children and adolescents aged 12-17 years in Mississippi lived with diagnosed alcohol or illicit drug dependence, and 11 000 reported illicit prescription drug use, but only 270 received treatment for these conditions. 18
In 2014, a primary care SBHC, open during school hours, was established in a dedicated space in an inner-city Mississippi high school (grades 9-12). In this school, average enrollment is 650, 100% of the student population is Black, all students are eligible for free lunch, 20 and 98% of the clinic population is Medicaid eligible (unpublished data, SBHC, Mississippi, 2020).
Once the SBHC was established, the behavioral health needs of students became evident, prompting integration of behavioral health services. While most US schools provide some form of school-based screening for mental health services, many lack immediate assessment and treatment on site or crisis referrals by health care professionals. 11 Data from the 2015-2016 School Survey on Crime and Safety indicate that 62% of US schools do not provide behavioral health services on site. Most schools provide diagnostic assessments by outside school-funded professionals. Furthermore, only one-third of schools provide on-site treatment for behavioral health. 21 Research found that when primary care and mental health care are offered together rather than separately, they result in more integrated care and decreased stigma for those seeking behavioral health services. 22 To our knowledge, this is the first SBHC in Mississippi to implement integrated care. This clinic is uniquely associated with the state’s only academic medical center and provides an interprofessional training site. Literature is sparse on how SBHCs may be used as clinical training environments, faculty practice sites, and centers for research, all of which have implications for program effectiveness, offerings, and sustainability. Preliminary effectiveness on professional student outcomes and program outcomes should be determined in future work.
Prior to implementation of the SBHC, adolescents in need of behavioral health services received care at local emergency departments regardless of acuity or waited up to 6 months for outpatient counseling or medication referrals (unpublished data, SBHC, Mississippi, 2020). With financial support from the Health Resources & Services Administration (HRSA) Nurse Education, Practice, Quality and Retention Interprofessional Collaborative Practice Program, behavioral health services were integrated into the high school SBHC. The goal of this 3-year program was to increase access to behavioral health services in interprofessional nurse-led primary care teams.
This case study describes our process in implementing behavioral health services into the primary care SBHC, initial outcomes, and lessons learned. Our work may provide guidance for other schools that wish to develop similar programs. In addition, our model prepares the workforce to address the primary and behavioral health care needs of adolescents and inform further research to evaluate the effectiveness of behavioral health programs in schools.
Methods
During planning for implementation of behavioral health care, we became aware of the need for additional personnel and a guiding model of care. The Interprofessional Collaborative Practice (IPCP) model guided the integration of behavioral health care into existing primary services. Building on the Health Disparities Collaborative Model, this model emphasizes transitional care coordination for medically underserved populations while using various disciplines of health care working together to deliver safe, effective, efficient, and equitable care. 23 Our program delivers comprehensive, team-based care while addressing the social determinants of health. An added benefit of using the IPCP model in our program was that the SBHC served as an interdisciplinary training site for health sciences students, including undergraduate and graduate nurses, psychiatric mental health nurse practitioners (PMHNPs), social workers, occupational therapists, and predoctoral psychology interns. The students representing academic institutions across the state gained knowledge and skills needed to implement an IPCP model.
Program Outcome Measures
In this article, we report data on 2 program indicators: primary care encounters and behavioral health encounters. Data on primary care encounters included number and type of visit (wellness and sports physicals, family planning, or sick visits); demographic characteristics (annual household income, health insurance, and housing status); prevalence of infectious, respiratory, and chronic conditions; level of prenatal care; immunization status; and screenings for cervical and breast cancer, weight and nutrition, and tobacco use. Data on preliminary behavioral health measures included the number of behavioral health screenings, positive screenings requiring further assessment, and behavioral health referral completion. We assessed behavioral health screenings using evidence-based, age-appropriate instruments with demonstrated clinical utility in primary care. We conducted assessments using the Patient Health Questionnaire (PHQ-9) for depressive symptoms, 24 Generalized Anxiety Disorder (GAD-7) for anxiety, 25 Center for Youth Wellness’ Adverse Childhood Experiences (ACE) Questionnaire for trauma exposure, 26 and Screening to Brief Intervention Tool to identify substance use. 27 Patients with scores ≥5 on the PHQ-9 or GAD-7 or a Center for Youth Wellness’ ACE Questionnaire score of ≥1 warranted referral to the interprofessional team. We also tracked referrals to the interprofessional team or the patient’s existing behavioral health provider.
Implementation
After obtaining written consent to treat from a parent or guardian, each student was invited to enroll as a patient in the SBHC. Nursing, social work, occupational therapy, and psychology interns collaborated with SBHC staff to provide care. During these encounters, the team further assessed symptoms of depression, anxiety, substance use, and trauma as well as social and academic functioning using semistructured interviews. Brief individualized behavioral interventions such as those for sleep hygiene, relaxation, emotion regulation, distress tolerance, and behavioral activation were implemented as needed. If an adolescent patient expressed suicidal or homicidal ideation, the SBHC used a documented safety plan to identify warning signs, distraction techniques, crisis resources, and means restriction. SBHC staff coordinated follow-up visits with the interprofessional team and off-site clinic referrals for medication and counseling evaluations as needed. SBHC staff addressed social determinants affecting health and immediate needs through the distribution of hygiene kits, access to a clothes closet (an on-site closet containing donated clothes), and the establishment of an on-site food pantry for all students. Social services professionals were on site daily to provide assistance with housing, domestic concerns, and health insurance applications. The purpose of this project was program development and treatment and not research. As such, this case study did not meet the criteria for research involving human subjects as per the University of Mississippi Medical Center Institutional Review Board.
Outcomes
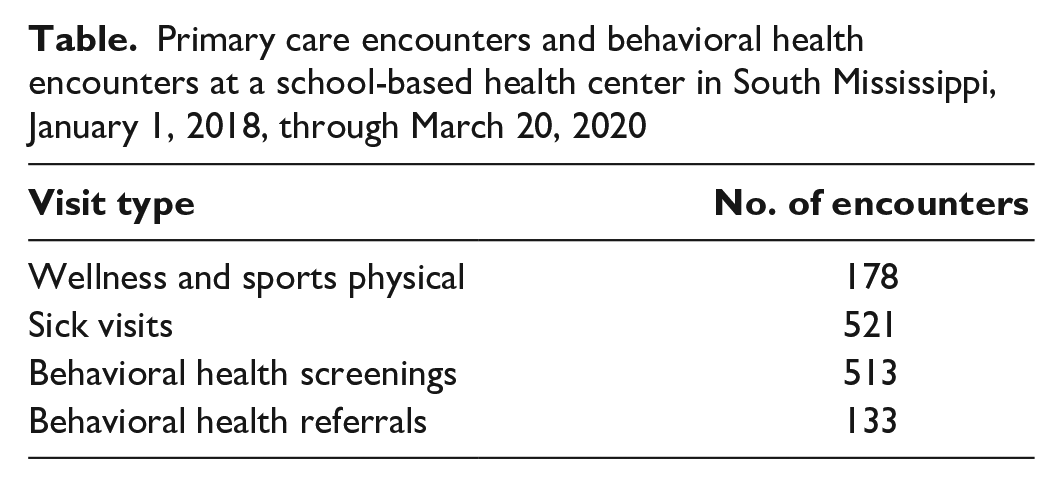
From January 1, 2018, through March 20, 2020, 178 wellness and sports physicals, 86 family planning visits, and 521 sick visits were provided as primary care encounters (Table). Of the total number of primary care encounters, 513 adolescents aged 13-17 years were screened for behavioral health risks, including depression, anxiety, substance use, and ACEs. Adolescents not screened were usually because they were too sick, the student refused screening, time limitations, or the clinic was over capacity. Among these 513 students, 133 (26%) had a preliminary positive screen for a behavioral health risk, and all were evaluated by the interprofessional educational team or a behavioral health provider. Subsequently, individualized plans of care were developed for each adolescent referral (n = 133, 100%).
Primary care encounters and behavioral health encounters at a school-based health center in South Mississippi, January 1, 2018, through March 20, 2020
Lessons Learned
Several lessons learned may be helpful to consider for those interested in replicating or developing a similar program. Staffing, student enrollment, student consent, and data collection recommendations are discussed.
Behavioral Health Professional Recruitment and Retention
A substantial challenge was recruitment and retention of staff, particularly a PMHNP and a social worker. In a recent review of national trends, only 3% of SBHCs with mental health services employed a PMHNP, mirroring the recruitment and retention challenges we faced.22,28,29 Lack of a PMHNP challenges continuity of care. Our solution was to develop screening criteria and a treatment algorithm that could be implemented by the primary care team, which provided the primary care nurse practitioner with guidance on interpretation of screening results and identification of referral needs. Second, our clinical psychologist team member served as an expert faculty and facilitator of the interprofessional education cohorts in the absence of the PMHNP. Access to a clinical psychologist was possible because of the affiliation with a local academic health science center. To ensure access to social services, we established a partnership with the Mississippi State Department of Health to provide a licensed social worker on site and interprofessional team participation.
A frequently reported concern for potential PMHNP and social work candidates was the temporary nature of grant-funded programs, highlighting the need for future diversification and stability of funding and academic–practice arrangements with the supporting institution. Struggles with SBHCs’ financial sustainability have been reported in the literature, with multiple funding sources presented as one solution.12,30,31 A robust academic–practice partnership with the state’s only academic health science center benefits our SBHC by providing a sustainable means of health care provider service and access to specialists who may not be available in the community setting. This partnership also allows for interprofessional training of future health professionals. Lastly, clinical questions may lead to research directions, which could open opportunities for funding. Academic–practice arrangements that allow nurse faculty to deliver patient care can support maintenance of professional certification for practice faculty. SBHCs can formalize partnerships with academic health centers to serve as practice sites for those who want trainees to have experience in SBHCs and consider partial buyout (ie, redirecting institutional funding allocation) of mental health professionals who can also serve as preceptors to students.
Student Enrollment
Written consent for treatment is a substantial barrier to accessing services in many SBHCs. One recent quality improvement assessment of return rates of written consents recommends strategies such as personal follow-up by SBHC staff, mailing consent forms, and creating competition for the most consents forms returned per student grade. 31 It is important to note that this quality improvement assessment was published before the COVID-19 pandemic and did not discuss options such as electronic consent forms; having that option may facilitate an increase in consent completion and improve access to services. Currently, our consent forms are included in paper packets that require parents to update the adolescent’s medical, surgical, and social history; health insurance status; and privacy agreements annually. This paperwork can be cumbersome, particularly for families with multiple children in the SBHC network. A shift to virtual learning has increased the comfort level among our patient population with electronic communication, including providing consent for medical care. Exploring electronic means of document exchange may be one way to increase the return rate of consent for care. Furthermore, policies to accept consent packets for the duration of a child’s time in a school (eg, a single consent form for students in 9th-12th grade), with the option to opt out each year, could be considered. Regularly scheduled drives to encourage the completion of consent forms were also key strategies in successful enrollment. These drives, which were held by SBHC staff at the Mississippi high school during special events such as football games and back-to-school celebrations, gave parents and students the opportunity to meet the staff and obtain information about the services offered through the SBHC. In years 2 and 3 (ie, academic years 2018-2019 and 2019-2010), only 26% to 30% of students had completed consent for services. Future strategies to increase the percentage of students providing consent for services may include further community engagement and the identification of consent champions but with considerations for COVID-19–related social distancing.
Marketing and public relations are also key to promoting the services of the SBHC. Information for parents about SBHC services, confidentiality, and operational and administrative separation of the clinic should be clearly communicated by school officials. Developing close working relationships with school personnel such as counselors, resource officers, and administration is critical, reinforcing how the clinic can provide integrated care to help students remain healthy and stay in school. Similar recommendations for sustaining SBHCs through alignment with school registration events are noted in previous work. 32 Relationship-building strategies included participation in school and community events such as homecoming parades, health fairs, schoolwide screenings, and, most recently, a resource drive to provide food, hygiene products, household cleaning supplies, and face masks in response to the COVID-19 pandemic.
Data Collection
Data collection, particularly abstracting quality improvement data from the electronic medical record, was challenging. Patient encounters in the clinic, behavioral health activities, and continuity were assessed through multiple sources. Information often required manual data entry into several data-tracking systems. Program evaluation and other data-collection needs are often underestimated. One strategy for enhancing data collection is to include dedicated personnel to enter, track, and evaluate data. Of note, a team well versed in data collection from electronic medical records and variables such as academic outcomes, student experiences, and financial variables is important. Automating this process can strengthen consistency and data quality. Furthermore, an expansion of data collection beyond the total number of behavioral health screenings, patient encounters, referrals, and follow-up is recommended.
Evaluating pre- and postbehavioral health risk scores by individuals and groups, as well as determining other physical and social determinants affecting health, may lead to additional targeted interventions to reduce risks. SBHCs should critically evaluate which data are collected. For example, academic variables such as attendance rates, truancy, high school graduation rates, and discipline problems might be affected by the presence of an SBHC and would be important to school officials.
Implications for Program Continuation
Recently acquired HRSA funding has allowed for continuation and expansion of services in the middle and elementary feeder schools where anxiety and depression are substantial problems. Discussions are under way to coordinate with hospital emergency departments, the state’s mental health rapid response teams, and participating schools in state mental health regions to extend the continuum of care into the community. Evidence-based smartphone applications connecting young people to coaching and quick psychoeducational interventions will also be implemented.
In the wake of the COVID-19 pandemic, the possibilities of providing telehealth services in the SBHC have increased access to specialists via telehealth, will help situate our SBHC within the larger health care system, and will help diversify income sources. In the long term, telehealth and access to specialists may decrease inappropriate and stressful mental health–related admissions to the emergency department.
The impact of this program has been substantial for adolescents with previously undiagnosed behavioral health concerns. The adolescents in our program were screened for behavioral risks, and 100% of those who screened positive received follow-up care with an individual plan. We suspected that the rates of symptoms of depression and anxiety and positive ACE scores would be high in our medically underserved student population; however, no formalized screening had previously been conducted, highlighting the need for this program. It is important to note that conducting screenings requires a mechanism of follow-up, which is possible in schools that have school nurses, SBHCs, and interdisciplinary teams, such as the school described here. Resource-limited schools face challenges with screening and response to mental health needs of students, and SBHCs provide a safety net. This screening informed future grant applications and clinic processes. Despite the challenges, SBHCs possess opportunities to meet students where they are and to create healthy schools and healthier communities.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This program is supported by the Health Resources & Services Administration (HRSA) of the US Department of Health and Human Services (HHS) as part of an award totaling $1 147 819 with 0% financed with nongovernmental sources. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, HRSA, HHS, the US government, or the National Institutes of Health. Angela A. Duck is partially supported by the National Institutes of Health/National Cancer Institute under award no. 5P30CA013148-47S.