
Abstract
Objective:
Transgender women with diagnosed HIV experience social and structural factors that could negatively affect their overall health and HIV-related health outcomes. We describe estimates from the Centers for Disease Control and Prevention Medical Monitoring Project (MMP) of sociodemographic characteristics, HIV stigma, discrimination, and mental health outcomes among transgender women with diagnosed HIV.
Methods:
We analyzed pooled data of all transgender women with diagnosed HIV (N = 217) from the 2015 through 2018 MMP cycles. We reported unweighted frequencies, weighted percentages, and 95% CIs for all characteristics. We post-stratified data to known population totals by age, race and ethnicity, and sex at birth from the National HIV Surveillance System.
Results:
Approximately 46% of transgender women with diagnosed HIV identified as Black or African American, 67% lived at or below the federal poverty level, 18% had experienced homelessness in the past year, 26% experienced mild to severe symptoms of depression, 30% experienced mild to severe anxiety symptoms, 32% reported physical violence by an intimate partner, and 30% reported forced sex during their lifetime. Despite 80% being very satisfied with their current HIV care, 94% experienced current HIV stigma and 20% experienced health care–related discrimination since being diagnosed with HIV. Among transgender women with diagnosed HIV who experienced discrimination, 46% and 51% experienced health care discrimination attributed to their gender and sexual orientation or sexual practices, respectively.
Conclusions:
Our findings underscore a need to address unmet ancillary services, such as housing, intimate partner violence, and mental health needs, and the need for strategies to reduce experiences with HIV stigma and discrimination in care for transgender women with diagnosed HIV in the United States.
Transgender women in the United States experience substantial health disparities, in part due to social and structural factors, including homelessness,1,2 poverty,2,3 lack of health insurance, 4 and lack of access to health care and preventive services. These social and structural disadvantages are often related to stigma and discrimination.1,5-8 Transgender women also experience HIV-related disparities. For example, from 2014 to 2018, the proportion of transgender women with diagnosed HIV infection increased 24%; in contrast, among cisgender men and cisgender women, respectively, comparative increases were 11% and 6%. 9 An estimated 14% of transgender women in the United States have diagnosed HIV; a higher percentage of Black or African American (44%) and Hispanic/Latina (26%) transgender women have diagnosed HIV compared with transgender women in other racial and ethnic groups. 1 Therefore, HIV treatment and care efforts for transgender women with HIV must address social and structural factors to reduce these disparities and improve health outcomes.
Transgender women with diagnosed HIV experience HIV stigma and health care discrimination due to the convergence of multiple marginalized social identities, which include their HIV status and gender identity. 10 Stigma is a complex and dynamic social process, where societal beliefs and attitudes reject and interpret “selective” human differences as inferior or of lower social value as a form of social control.10-12 Discrimination is the behavior that results from stigma, which translates into the act of treating people unfairly due to their human differences. 11 Transgender women experience discrimination at health care settings from physicians, health care providers, and other staff. Examples of health care discrimination include not receiving transition-related health care, being asked invasive questions about being transgender, and having to teach the health care provider about transgender people to receive appropriate care. 6 Stigma and discrimination in health care settings are associated with poor mental health and HIV treatment and care outcomes,13-16 including low adherence to antiretroviral therapy (ART) and reduced viral suppression.13,16,17
Disproportionate experiences with stigma, health care discrimination, and poor mental health outcomes have been reported among transgender women in the United States.6,15,18-21 However, limited studies are available on transgender women from population-based samples of people with diagnosed HIV.2,13,22 Here, we describe sociodemographic characteristics, HIV stigma, health care discrimination, and mental health outcomes among transgender women with diagnosed HIV using data from the Centers for Disease Control and Prevention’s (CDC’s) Medical Monitoring Project (MMP).23,24 Our results could inform future interventions and strategies to address stigma and discrimination and improve HIV-related health outcomes for transgender women with diagnosed HIV.
Methods
MMP Design and Data Collection
The MMP is an annual, cross-sectional survey designed to produce nationally representative estimates of behavioral and clinical characteristics among adults with diagnosed HIV in the United States. Briefly, MMP uses a 2-stage sampling method. In the first stage, 16 states and Puerto Rico were sampled from all 50 states, the District of Columbia, and Puerto Rico. In the second stage, simple random samples of people with diagnosed HIV aged ≥18 years were drawn annually for each participating jurisdiction from the National HIV Surveillance System, a census of people with diagnosed HIV in the United States. This analysis was conducted in 2020, using combined annual data from the 2015 through 2018 MMP cycles. For each annual cycle, interview and medical record data were collected from June of each cycle year through May of the following year. The MMP had response rates of 100% at the jurisdiction level and from 40% to 46% at the person level. MMP data collection is a part of routine public health surveillance and, thus, determined to be non-research by CDC. 25 Participating jurisdictions obtained local institutional review board approval to collect data when required. Informed consent was obtained from all participants.
People were classified as transgender women if they reported that their sex assigned at birth was male and their gender was female or transgender (N = 217). From MMP data, we calculated weighted percentages of transgender women among all adults with diagnosed HIV by yearly cycle as follows: 1.23% (95% CI, 0.72%-1.74%) in 2015, 1.05% (95% CI, 0.69%-1.41%) in 2016, 1.51% (95% CI, 1.06%-1.97%) in 2017, and 1.63% (95% CI, 1.26%-2.01%) in 2018.
Measures
The MMP survey used 10 items, with responses measured on a 5-point Likert scale (from 1 [strongly disagree] to 5 [strongly agree]), to measure HIV stigma that encompassed 4 domains: personalized stigma, disclosure concerns, negative self-image, and public attitudes. 26 The personalized stigma domain measures the perceived negative experiences of other people knowing of their HIV status. The disclosure concerns domain is related to feelings of worry and being careful about disclosing their HIV status. The negative self-image domain measures the internalized stigma, feelings of guilt, blame, or shame due to HIV status. The public attitudes domain measures concerns about how others view people with HIV. 27 Other studies that used MMP data have previously used the HIV stigma scale for transgender women with diagnosed HIV.28,29 In addition, in a national community-based research study that used this HIV stigma scale for transgender women with HIV, Cronbach α values ranged from 0.76 to 0.88 for the 4 domains. 30 Respondents experienced overall stigma if they responded with “somewhat agree” or “strongly agree” to any of the 10 items. Respondents experienced any stigma within each domain if they responded with “somewhat agree” or “strongly agree” to any of the items within that domain.
The MMP measured discrimination by using 3 yes/no questions about discrimination experienced in the health care system since the person first tested positive 31 ; these questions had been asked only during the 2015 through 2017 MMP cycles. Respondents experienced any discrimination in the health care system if they responded “yes” to any of the following 3 questions: (1) Since testing positive for HIV, has anyone in the health care system exhibited hostility or a lack of respect for you? (2) Since testing positive for HIV, has anyone in the health care system given you less attention than other patients? (3) Since testing positive for HIV, has anyone in the health care system refused you service? If respondents reported discrimination, they were asked whether they attributed the discrimination to their gender and/or their sexual orientation/sexual practices.
We categorized generalized anxiety disorder and depression symptoms in the previous 2 weeks based on clinically meaningful cutoff points from the Generalized Anxiety Disorder 7-item scale 32 and the Patient Health Questionnaire 8-item scale, 33 respectively. Respondents were categorized as having “severe anxiety” if they had a score of ≥15 according to the Generalized Anxiety Disorder 7-item scale and were categorized as having “mild to moderate anxiety” if they had a score of 5 through 14. Respondents were categorized as having “severe depression” if they had a score of ≥15 according to the Patient Health Questionnaire 8-item scale and as having “mild to moderate depression” if they had a score of 5 through 14.
Respondents were categorized as experiencing physical violence by an intimate partner if they had been slapped, punched, shoved, kicked, choked, or otherwise physically hurt by a romantic or sexual partner. Respondents were categorized as experiencing forced sex if they had been threatened with harm or physically forced to have unwanted vaginal, anal, or oral sex. The MMP adapted the physical violence and forced sex questions from the National Intimate Partner Violence Survey. 34
The MMP used 1 item to measure sexual identity among respondents: “Do you think of yourself as,” with response options of “lesbian or gay”; “straight, that is, not gay”; “bisexual”; or “something else.” All examined covariates were collected via interview and were measured during the past 12 months, except where otherwise noted. Household poverty level was defined based on US Department of Health and Human Services guidelines. 35 For example, a single person with no other people in the family or the household who had an annual income ≤$11 880 was considered at or below the federal poverty level. Respondents were categorized as experiencing homelessness if they lived on the street, in a shelter, in a single-room occupancy hotel, or in a car. Health insurance coverage was categorized as having any private health insurance, public health insurance only, or Ryan White HIV/AIDS Program (hereinafter, Ryan White) coverage, or AIDS Drug Assistance Program only/uninsured. Respondents who had Ryan White or AIDS Drug Assistance Program coverage only and respondents who had no health insurance were combined because of small sample sizes and because both categories indicated a need for health insurance. Respondents were categorized as having an unmet need for ancillary services if they reported a need but did not receive any of a range of services (eg, substance use counseling or treatment, adherence support counseling, dental care). 36
Statistical Analysis
We conducted our data analyses in 2020. We reported unweighted frequencies, weighted percentages, and 95% CIs for demographic characteristics, mental health outcomes, and experiences of violence victimization, stigma, and discrimination. The MMP used weighted data based on known probabilities of selection at state or territory and person levels, adjusted for nonresponse.23,37 For the nonresponse adjustment, the MMP based weighting classes on variables related to person-level responses, which were assessed annually; more details on the variables used to create weighting classes are described elsewhere. 38 We post-stratified the data to known population totals by age, race and ethnicity, and sex assigned at birth from the National HIV Surveillance System. We conducted the data analysis using weighting procedures that accounted for the complex sample design using the survey procedures in SAS version 9.4 (SAS Institute, Inc).
Results
We found that 46.1% of transgender women with diagnosed HIV identified as non-Hispanic Black or African American (Table 1). More than one-fourth (26.2%) of transgender women with diagnosed HIV experienced mild to severe symptoms of depression, and nearly one-third (30.0%) experienced symptoms of mild to severe anxiety in the 2 weeks before the interview (Table 2). Almost 1 in 10 transgender women (9.2%) reported having an unmet need for mental health services in the 12 months before they were interviewed.
Sociodemographic characteristics among transgender women with diagnosed HIV in the United States, Medical Monitoring Project, 2015-2018 a
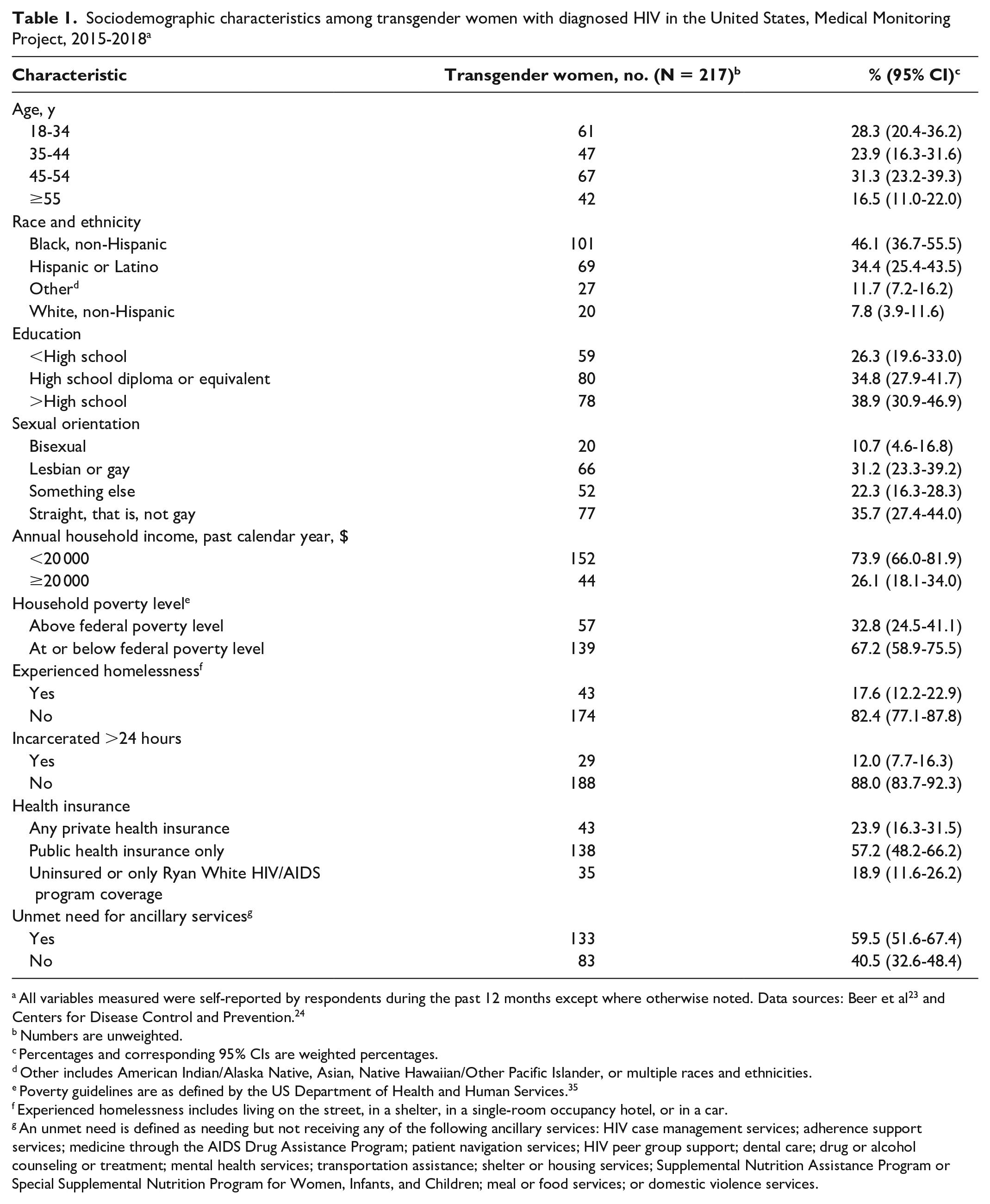
All variables measured were self-reported by respondents during the past 12 months except where otherwise noted. Data sources: Beer et al 23 and Centers for Disease Control and Prevention. 24
Numbers are unweighted.
Percentages and corresponding 95% CIs are weighted percentages.
Other includes American Indian/Alaska Native, Asian, Native Hawaiian/Other Pacific Islander, or multiple races and ethnicities.
Poverty guidelines are as defined by the US Department of Health and Human Services. 35
Experienced homelessness includes living on the street, in a shelter, in a single-room occupancy hotel, or in a car.
An unmet need is defined as needing but not receiving any of the following ancillary services: HIV case management services; adherence support services; medicine through the AIDS Drug Assistance Program; patient navigation services; HIV peer group support; dental care; drug or alcohol counseling or treatment; mental health services; transportation assistance; shelter or housing services; Supplemental Nutrition Assistance Program or Special Supplemental Nutrition Program for Women, Infants, and Children; meal or food services; or domestic violence services.
Mental health outcomes and experiences with violence among transgender women with diagnosed HIV in the United States, Medical Monitoring Project, 2015-2018 a
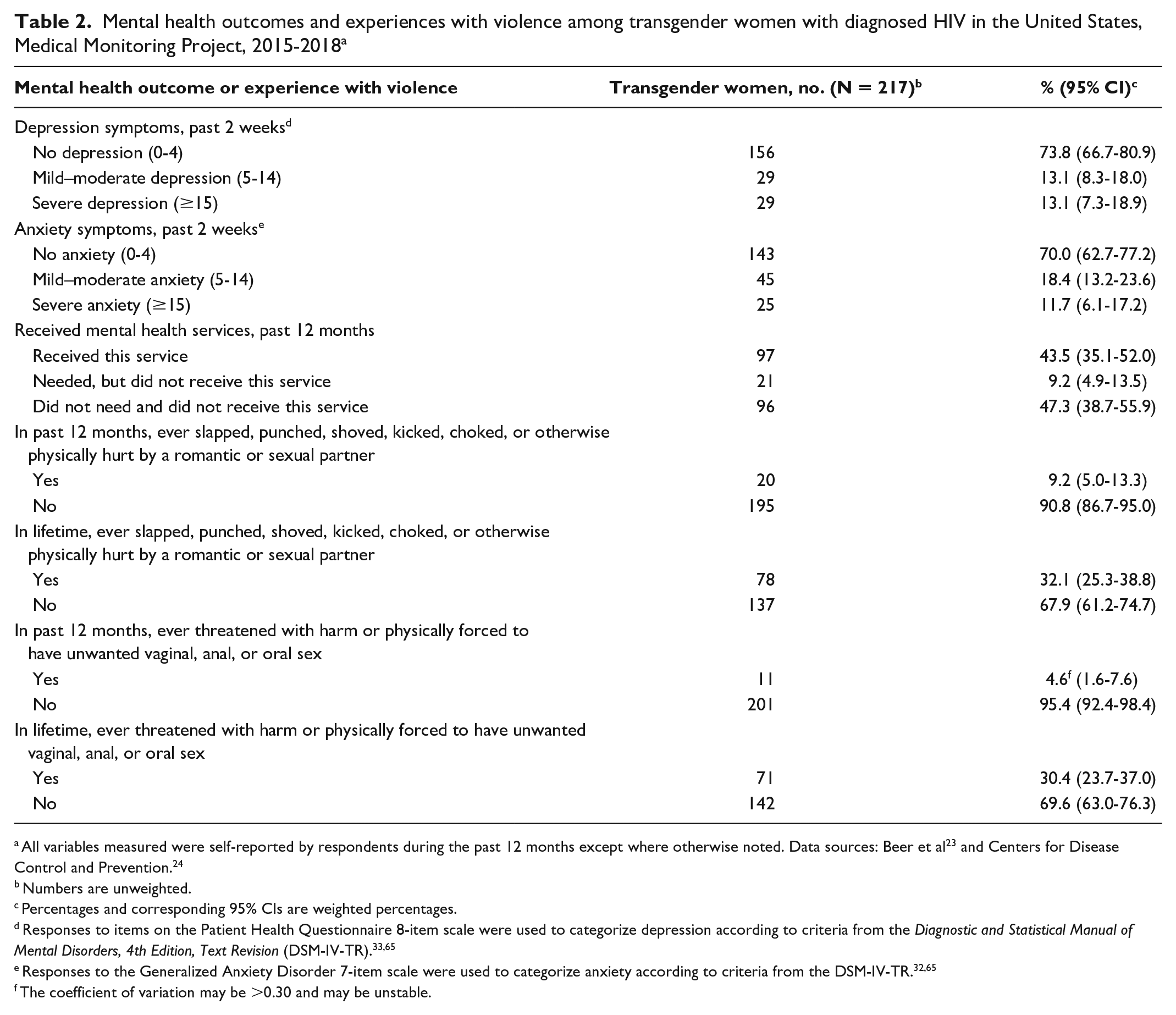
All variables measured were self-reported by respondents during the past 12 months except where otherwise noted. Data sources: Beer et al 23 and Centers for Disease Control and Prevention. 24
Numbers are unweighted.
Percentages and corresponding 95% CIs are weighted percentages.
Responses to items on the Patient Health Questionnaire 8-item scale were used to categorize depression according to criteria from the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR).33,65
Responses to the Generalized Anxiety Disorder 7-item scale were used to categorize anxiety according to criteria from the DSM-IV-TR.32,65
The coefficient of variation may be >0.30 and may be unstable.
Nearly all transgender women with diagnosed HIV experienced some aspect of HIV-related stigma (93.6%) (Table 3). More than half (51.7%) experienced personalized stigma, 86.9% experienced HIV disclosure stigma, 27.4% experienced stigma related to negative self-image, and 69.3% experienced stigma related to perceived public attitudes about people with HIV. Nearly 1 in 5 transgender women (19.8%) experienced discrimination in a health care setting since testing positive for HIV. Among those who reported any discrimination, health care–related discrimination attributed to gender and sexual orientation/sexual practices was also high (45.8% and 50.8%, respectively). Despite the high prevalence of experiencing any discrimination in the health care system, 80.1% of transgender women with diagnosed HIV were very satisfied with their current HIV care and 15.5% were somewhat satisfied.
Stigma and discrimination among transgender women with diagnosed HIV in the United States, Medical Monitoring Project, 2015-2018 a
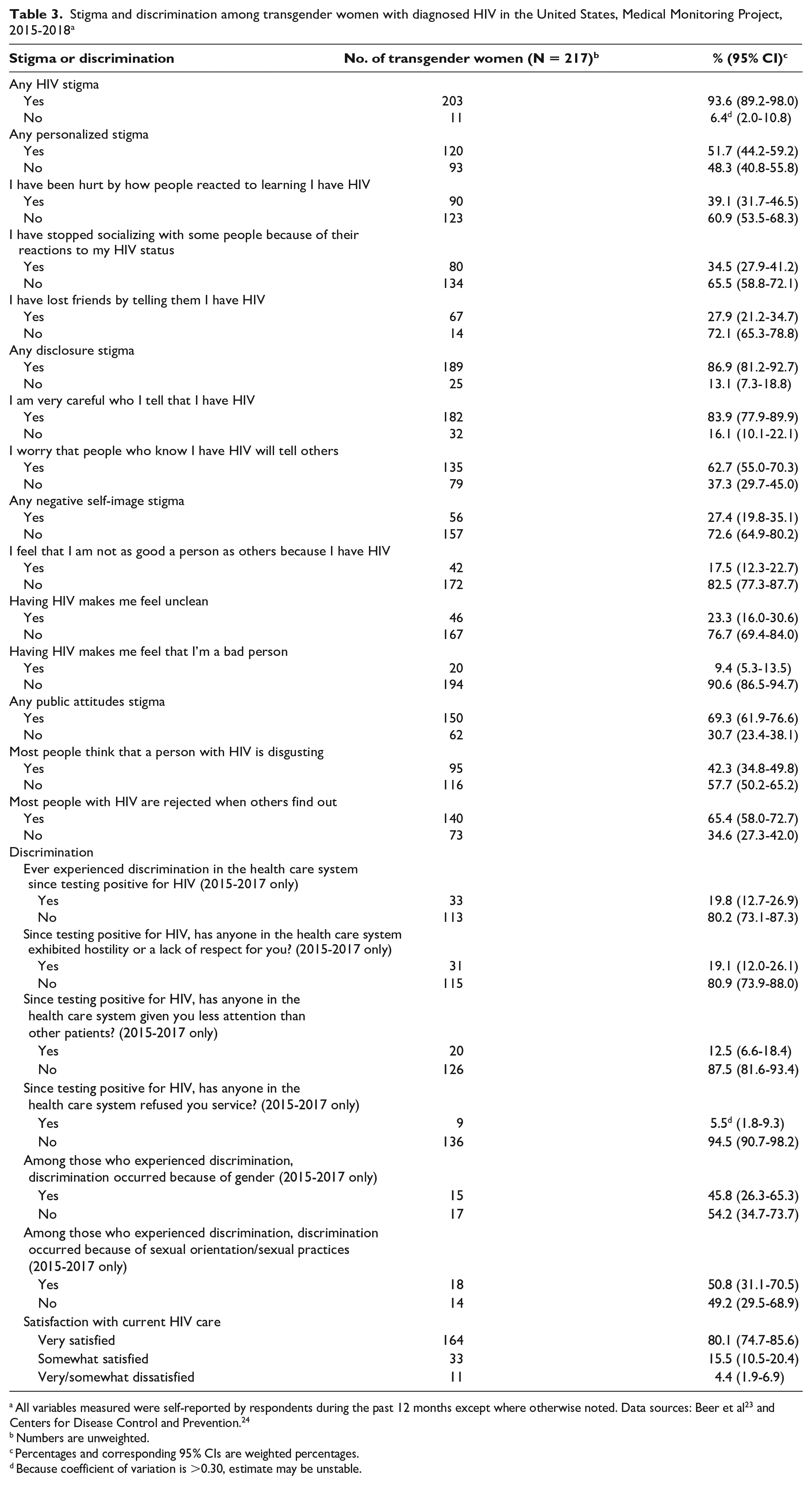
All variables measured were self-reported by respondents during the past 12 months except where otherwise noted. Data sources: Beer et al 23 and Centers for Disease Control and Prevention. 24
Numbers are unweighted.
Percentages and corresponding 95% CIs are weighted percentages.
Because coefficient of variation is >0.30, estimate may be unstable.
Discussion
In this analysis, we found high levels of HIV stigma, discrimination, and poor mental health outcomes among transgender women with diagnosed HIV in the United States. However, most transgender women with diagnosed HIV also reported a high satisfaction level with their current HIV care, which is notable and encouraging. This finding could suggest that HIV care settings are providing needed care for transgender women with diagnosed HIV. By contrast, nearly 20% of respondents also reported health care–related discrimination. It is possible that the reported experiences with health care–related discrimination occurred in the past and/or outside their current HIV health care setting. In addition, it could reflect the resilience of transgender women and the role of peer support in overcoming experiences of discrimination.6,30,39 Reducing stigma and discrimination toward transgender women with diagnosed HIV should be prioritized, as it could ameliorate the general well-being and HIV outcomes of this population.
The high levels of HIV stigma reported by transgender women with diagnosed HIV included personalized stigma, HIV disclosure stigma, and stigma related to public attitudes toward people with HIV. Experiences of HIV stigma among transgender women with diagnosed HIV could derive from devaluing attitudes and beliefs toward people with HIV. Experiences of stigma could also be attributed to public views on identities such as gender and race and ethnicity of people with HIV.10,29,40 These results, which are consistent with the literature,20,21,41,42 are important because experiences with stigma can negatively affect both the physical and mental health of transgender women and limit their access to employment, housing, and health care resources.10,14,41,43,44 The HIV stigma scale used in our study to measure 4 domains of HIV stigma experiences is also used by the National HIV/AIDS Strategy to monitor the prevalence of stigma among people with HIV. 45 Thus, the estimates from our study could provide a benchmark to monitor progress in decreasing the prevalence of HIV stigma among transgender women with diagnosed HIV in the United States.
In studies of patients with HIV, experiences with stigma are associated with low ART adherence, reduced viral suppression, and decreased access to HIV care.5,10,22,42,46,47 Strategies to reduce experiences with stigma could include multilevel approaches that address negative attitudes and beliefs about people with HIV and transgender women.14,46 Lack of awareness and cultural humility—that is, having an other-oriented interpersonal position characterized by respect and lack of superiority toward the cultural background and experiences of individuals 48 —among staff and health care providers could increase experiences with stigma toward transgender women with diagnosed HIV. Although no evidence-based interventions have been designed to reduce experiences with HIV-related stigma among transgender women with diagnosed HIV, a systematic review focused on education training for medical students and residents on transgender health care. Training improved attitudes toward transgender patients and increased knowledge and skills needed for providing competent care to transgender people. 49
Among the transgender women with diagnosed HIV who reported experiences with health care–related discrimination since testing positive for HIV, nearly half reported that the discrimination was attributed to their gender identity and sexual orientation/sexual practices, which is consistent with other studies.1,6,7,15,21,50,51 These findings indicate a multilayered experience of discrimination, which may be based on beliefs, attitudes, and prejudice of health care facility staff and providers. In addition, groups who are socially marginalized, such as transgender women, experience discrimination outside health care systems that could impede access to care.52,53 Discrimination attributed to HIV and gender identity status could increase barriers to care and lead to poor health outcomes among transgender women with diagnosed HIV.10,50,54 These experiences can also impede access to treatment and care in this population.7,14,55,56
Improving knowledge of health care providers through transgender cultural competency training and gender affirmation models in health care settings could reduce the stigma experienced by transgender women in health care settings.7,14,21,57 The CDC website 58 has information, educational materials, and tools for health care providers, whole care teams, and social service providers on delivering care for transgender patients, including transgender women with HIV. These tools, when used consistently and appropriately, can reduce the number of experiences with discrimination among transgender women with diagnosed HIV. 58 Results from a qualitative study of transgender women suggested that systemic changes in health care settings, such as inclusion of transgender people in service delivery, peer support, safe spaces, and education training developed and delivered by transgender people, could also improve health care services for this population. 39
We found that about 1 in 4 transgender women with diagnosed HIV experienced symptoms of depression and anxiety, which aligns with the literature.16,17,21,41,43,59 Transgender women with diagnosed HIV experienced levels of symptoms of depression (26.2% vs 18.0%) and anxiety (30.1% vs 21.7%) that were higher than among all adults with diagnosed HIV during 2018. 36 Although not examined in our study, an association between symptoms of anxiety and depression and experiences of multiple domains of HIV stigma has been found in other studies.29,40 The self-reported mental health symptoms of anxiety and depression among our cohort could be attributed to high levels of socioeconomic challenges, including homelessness, poverty, and exposure to violence victimization. 17 In addition, the transgender women with diagnosed HIV in our study reported substantial unmet needs for mental health services. High levels of anxiety and depression and unmet needs for mental health services highlight the need to improve the delivery of mental health services for transgender women with diagnosed HIV. Experiences with anxiety and depression are associated with poor HIV-related health outcomes, such as lower ART prescription, adherence, and viral suppression.16,17,42,46 Screening for and addressing the mental health needs of transgender women in HIV treatment and care are critical for improving their overall health and well-being.
In our examination of the sociodemographic characteristics of transgender women with diagnosed HIV, a greater percentage of transgender women with diagnosed HIV identified as Black or African American and Hispanic/Latina than other races and ethnicities, and most experienced socioeconomic challenges, including living below the federal poverty level, having a past-year income of <$20 000, and experiencing homelessness. We also found that transgender women with diagnosed HIV experienced levels of social and structural factors associated with poor health outcomes that were higher than shown among all adults with diagnosed HIV. Specifically, transgender women with diagnosed HIV had prevalences of homelessness (17.6% vs 10.0%), incarceration (12.0% vs 4.7%), and income below the federal poverty level (67.2% vs 43.0%) that were higher than those reported among all adults with diagnosed HIV.36,50 More than half reported unmet needs for ancillary services, which included shelter or housing services and domestic violence services. These findings support the findings of previous studies on unmet service needs among transgender women with diagnosed HIV and highlight the importance of integrating these services with HIV care.2,4,6,54 In addition, our findings add to the literature by providing estimates for this key population that were drawn from a nationally representative sample of adults with diagnosed HIV.1,6,7,19,22,50,60
Among transgender women with diagnosed HIV, we found that nearly 70% had a lifetime experience with physical violence by an intimate partner and/or forced sex. Specifically, we found prevalences of lifetime physical violence by an intimate partner (32.1% vs 27.5%) and lifetime forced sex (30.4% vs 17.4%) among transgender women with diagnosed HIV that were higher than reported in all adults with diagnosed HIV. 36 Transgender women with diagnosed HIV may experience homelessness, unmet housing needs, and income needs as a result of housing and employment discrimination,6,60 increasing their risk for and experiences with violence and forced sex.5,61 Socioeconomic challenges, including unemployment and homelessness, and experiences with physical violence and/or forced sex are associated with poor health outcomes.60,62 Training health care providers to incorporate screening for employment and housing needs and linking women to appropriate services may assist with addressing these socioeconomic challenges and improving health outcomes among transgender women with diagnosed HIV.50,54,62 Health care providers should also include screening for and linkage to services that address intimate partner violence into health care visits for this population.
Limitations
Our study had 5 limitations. First, the measures used in our study were self-reported, which could have led to an over- or underestimation as a result of recall bias and social desirability bias. Although the MMP used the 2-step method to measure transgender identity, some respondents may not have identified themselves as transgender women, possibly because of fear of stigma. To measure symptoms of anxiety and depression among respondents, the MMP used the Generalized Anxiety Disorder 7-item scale and the Patient Health Questionnaire 8-item scale, which are not equivalent to a clinical diagnosis; however, these measures are linked to the diagnostic criteria used in the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV text revision) and showed good criterion validity.32,33,63-65 Second, 95% CIs for some variables were unstable because of small sample sizes. Because of the small sample size, our ability to examine relationships among sociodemographic characteristics, stigma, discrimination, and mental health outcomes was limited. Third, the stigma measures in this study were focused only on HIV-related stigma and did not measure intersectional stigma, which is stigma due to the convergence of multiple social statuses. 10 The MMP only measured discrimination in health care settings. Broader measures, such as the Everyday Discrimination Scale, 66 could assess experiences of discrimination beyond health care settings. Fourth, the study estimates could vary by geographic area. Fifth, qualitative research exploring the insights of transgender women with diagnosed HIV on the interpersonal and structural factors and the underlying mechanisms of stigma and discrimination in health care settings was beyond the scope of our study.
Conclusions
Our study reported the national estimates of HIV stigma, discrimination, and mental health outcomes among transgender women drawn from a nationally representative sample of people with diagnosed HIV in the United States. Many experienced stigma and discrimination. Our results could inform future interventions and strategies to address stigma and discrimination; addressing stigma and discrimination could lead to improved HIV-related health and overall physical and mental health outcomes for transgender women with diagnosed HIV. About one-fourth of transgender women with diagnosed HIV reported symptoms of anxiety and depression, and 1 in 10 reported unmet mental health needs. Our results suggest a need to integrate mental health needs into HIV treatment and care services to improve the mental health of transgender women with diagnosed HIV. Our findings underscore the need for transgender-sensitive health care settings and providers so that health disparities among transgender women, who are disproportionately affected by HIV in the United States, can be decreased. Future research should explore the associations among stigma, discrimination, and mental health outcomes and the HIV care continuum outcomes among transgender women with diagnosed HIV.
Footnotes
Acknowledgements
The authors thank MMP participants, project area staff, and MMP provider and community advisory board members. We also acknowledge the contributions of the Clinical Outcomes Team and Behavioral and Clinical Surveillance Branch at CDC.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.