
Abstract
Objectives:
First responders, including firefighters, emergency medical technicians (EMTs), paramedics, and law enforcement officers, are working on the front lines to fight the COVID-19 pandemic and facing an increased risk of infection. This study assessed the seroprevalence of SARS-CoV-2 infection among first responders in northeastern Ohio.
Methods:
A survey and immunoglobulin G antibody test against SARS-CoV-2 nucleocapsid protein were offered to University Hospitals Health System–affiliated first-responder departments during May to September 2020. The survey contained questions about demographic characteristics and history of SARS-CoV-2 infection. A total of 3080 first responders with diverse job assignments from more than 400 fire and police departments participated in the study.
Results:
Of 3080 participants, 73 (2.4%) were seropositive and 26 (0.8%) had previously positive real-time polymerase chain reaction results. Asymptomatic infection accounted for 46.6% (34 of 73) of seropositivity. By occupation, rates of seropositivity were highest among administration/support staff (3.8%), followed by paramedics (3.0%), EMTs (2.6%), firefighters (2.2%), and law enforcement officers (0.8%). Work-associated exposure rates to COVID-19 patients were: paramedics (48.2%), firefighters (37.1%), EMTs (32.3%), law enforcement officers (7.7%), and administration/support staff (4.4%). Self-reported community exposure was positively correlated with self-reported work-associated exposure rate (correlation coefficient = 0.99). Neither self-reported community nor work-associated exposure was correlated with SARS-CoV-2 seroprevalence. We found no significant difference in seroprevalence among sex/gender or age groups; however, Black participants had a higher positivity rate than participants of other racial groups despite reporting lower exposure.
Conclusions:
Despite the high work-associated exposure rate to SARS-CoV-2 infection, first responders with various roles demonstrated seroprevalence no higher than their administrative/supportive colleagues, which suggests infection control measures are effective in preventing work-related infection.
Keywords
First responders include firefighters, emergency medical technicians (EMTs), paramedics, and police officers. There are more than 1 million first responders in the United States, many of whom are working on the front lines fighting the COVID-19 pandemic along with health care workers. Because of the nature of their work, first responders face an increased risk of coming into contact with SARS-CoV-2, the causative agent of COVID-19. While personal protective equipment (PPE) and engineering controls have been used in the health care workplace, data on their effectiveness in preventing infection have not yet been gathered and thoroughly studied. Data gathered on exposure and infection rates among first responders are important for providing information on the totality of undiagnosed infections and could shed light on the associations among seroprevalence, sociodemographic characteristics, and occupation in the frontline workforce.
Many studies have addressed the prevalence of COVID-19 among health care workers in various countries and regions. However, few studies have been conducted on first responders, and most of these studies were limited in sample size and presented a snapshot of a local region during a short period.1-9 The objective of this study was to assess the sero-prevalence of SARS-CoV-2 infection among first responders in northeastern Ohio.
Methods
Study Design and Participants
We aimed to recruit 5000 first responders from emergency medical services (EMS), fire, and police departments affiliated with University Hospitals Health System (UHHS) in northeastern Ohio. All first responders who worked in the region, were aged ≥18 years, and provided consent were eligible to participate. We defined work and community exposure as direct contact with people who had a confirmed positive COVID-19 test result at work or in the community, respectively. The UHHS Institutional Review Board reviewed and approved this study, and participation in this study was voluntary.
Informed Consent, Survey, and Study Workflow
The study requested participants to provide informed consent, complete a survey, and obtain a single blood draw by venipuncture. We used REDCap (Research Electronic Data Capture), a secure web application, to administer informed consent forms electronically, manage the surveys, and store COVID-19 antibody test results.
We emailed department heads of UHHS-affiliated first-responder departments about the study and asked them to respond affirmatively if their departments would be willing to participate. A poster describing the study was then provided to interested departments to inform potential participants about study details. We visited interested first-responder departments to meet with potential participants to describe the study, answer questions, allow subjects to read and complete an informed consent form, and then complete the electronic survey. UHHS hospital phlebotomists or paramedics at the first responder’s workplace collected a blood sample from each participant. After the blood draw, participants received an email providing instructions for accessing results and a copy of frequently asked questions about SARS-CoV-2 antibody testing. Participants accessed their SARS-CoV-2 test results confidentially via a secure UHHS patient portal. Participants’ employers or supervisors did not have access to the results.
Specimen Collection and Processing
A minimum of 1 mL of blood was collected into a serum separator tube by venipuncture. Serum samples were allowed to clot adequately before centrifugation and then centrifuged at 3000 rpm for 6 minutes. After centrifugation, samples were tested within the stability time frame specified by the assay manufacturer (up to 2 days if stored at room temperature [15 °C to 30 °C] or up to 7 days at 2 °C to 8 °C]).
SARS-CoV-2 Antibody Testing
Antibody testing was conducted at the University Hospitals Cleveland Medical Center core laboratory, which is certified under the Clinical Laboratory Improvement Amendments of 1988 to perform high-complexity testing. The testing was performed using the Abbott SARS-CoV-2 immunoglobulin G (IgG) assay (Abbott Laboratories Inc), a chemiluminescent microparticle immunoassay, on Architect i1000SR analyzers for detecting IgG antibodies against the nucleocapsid protein of SARS-CoV-2. This assay has been approved by the US Food and Drug Administration for use under an Emergency Use Authorization. 10 Test results were reported qualitatively as negative or positive based on index values, using a cutoff of ≥1.4 per the manufacturer’s instructions.
Statistical Analysis
We performed statistical analyses using SigmaPlot version 11.0 (Systat Software Inc). We summarized categorical variables as percentages, and we used the Pearson χ2 test with Yates’ correction or the Fisher exact test to determine significance; P < .05 was considered significant. SigmaPlot software automatically analyzes data for their suitability for χ2 or Fisher exact tests and suggests the appropriate test based on the sample size of each group. We assessed possible associations between exposures and seroprevalence using relative risk (RR). We expressed continuous variables as mean along with SDs or medians with interquartile ranges (IQRs). We compared differences between 2 groups using the t test or Mann-Whitney rank-sum test, depending on whether the normality test (Shapiro-Wilk) passed or failed. We compared differences among ≥3 groups using 1-way analysis of variance (ANOVA) or Kruskal–Wallis 1-way ANOVA on ranks depending on the result of the normality test. We used Spearman rank-order correlation to assess the correlation between variables such as seroprevalence and exposure to COVID-19. P < .05 was considered significant.
Results
Seroprevalence and Self-Reported Exposure by Occupation
A total of 3275 first responders from 415 fire and police departments in Ohio consented to the study from May 22 through September 15, 2020, of whom 195 (6.0%) did not have blood drawn for antibody testing and were excluded from data analysis. A total of 3080 participants completed the SARS-CoV-2 antibody test and were included in the study. These participants had diverse occupations and job assignments within first-responder departments (online-only Supplemental Figure 1). Firefighters (n = 1439), paramedics (n = 705), police officers (n = 358), and EMTs (n = 303) accounted for 91.1% (n = 2805) of participants, and administrative and support staff (ie, office or field staff, such as ambulette drivers and sanitation workers) working in fire and law enforcement departments accounted for 5.2% of participants; the remaining 2.6% were health care workers, rescuers, and other–unspecified (online-only Supplemental Figure 2). We found no significant difference in seroprevalence or exposure between administrative and support staff; as such, we combined the 2 groups because of the small sample size.
By occupation, the highest level of reported work-related exposure was among paramedics (48.2%), firefighters (37.1%), and EMTs (32.3%), and the lowest level of reported work-related exposure was among law enforcement officers (7.7%) and administrative/support staff (4.4%) (Figure 1).
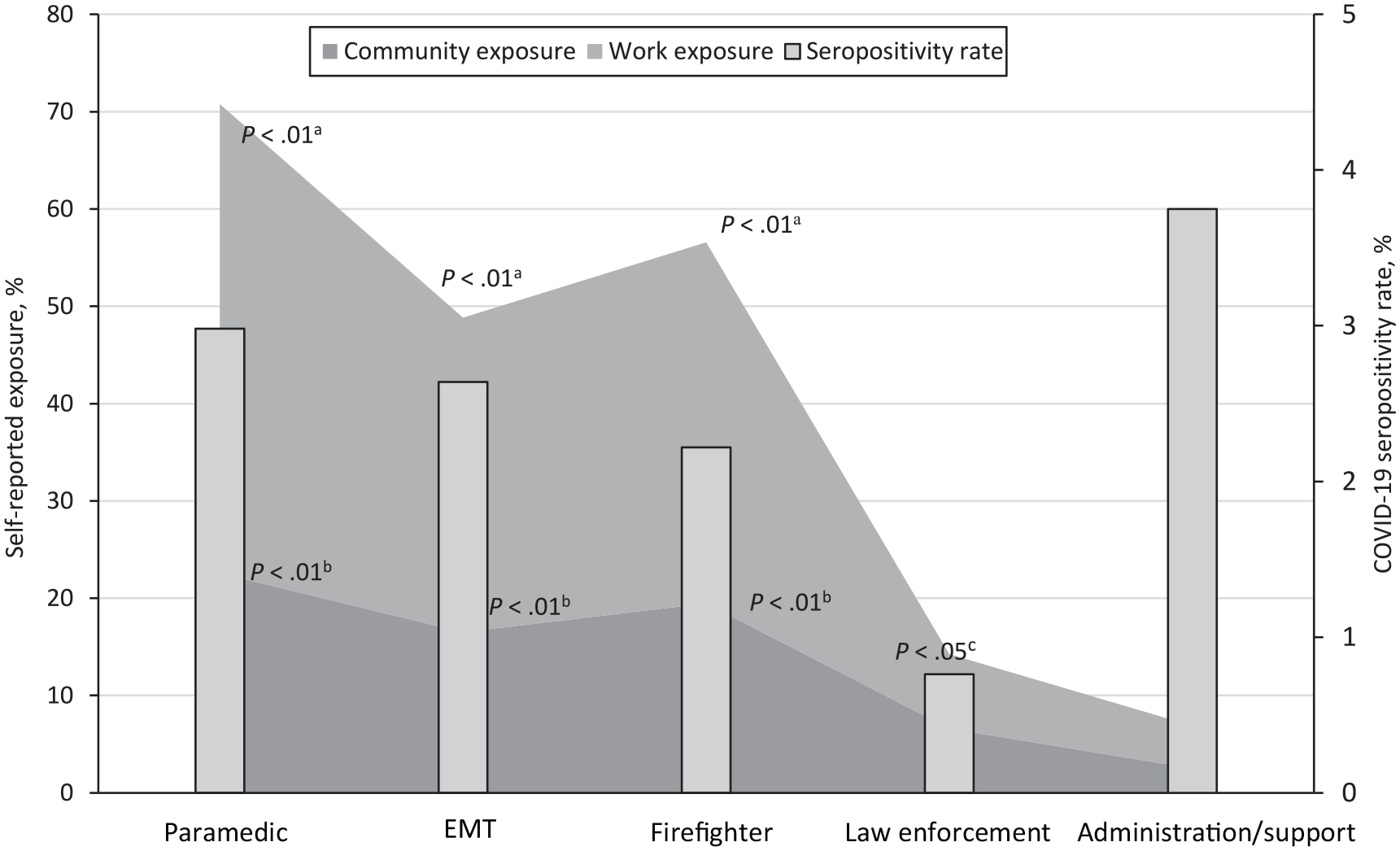
Seropositivity rate and exposure to SARS-CoV-2 infection by occupation among 3080 first responders who participated in a study on SARS-CoV-2 seroprevalence, northeastern Ohio, May–September 2020. Abbreviation: EMT, emergency medical technician.
Seventy-three participants had a positive test result, giving an overall seropositivity rate of 2.4% (Table). Seroprevalence was highest among participants holding administrative/support positions (3.8%) and paramedics (3.0%) and lowest among law enforcement officers (0.8%) (Figure 1). The RR among law enforcement officers was 0.26 (95% CI, 0.08-0.85; P = .03) lower than among paramedics. Further analysis showed no correlation between the work exposure rate and seroprevalence among various occupations (P = .82).
Sociodemographic characteristics and COVID-19 seropositivity rates of first responders who participated in a survey assessing SARS-CoV-2 seroprevalence, northeastern Ohio, May–September 2020 (N = 3080)
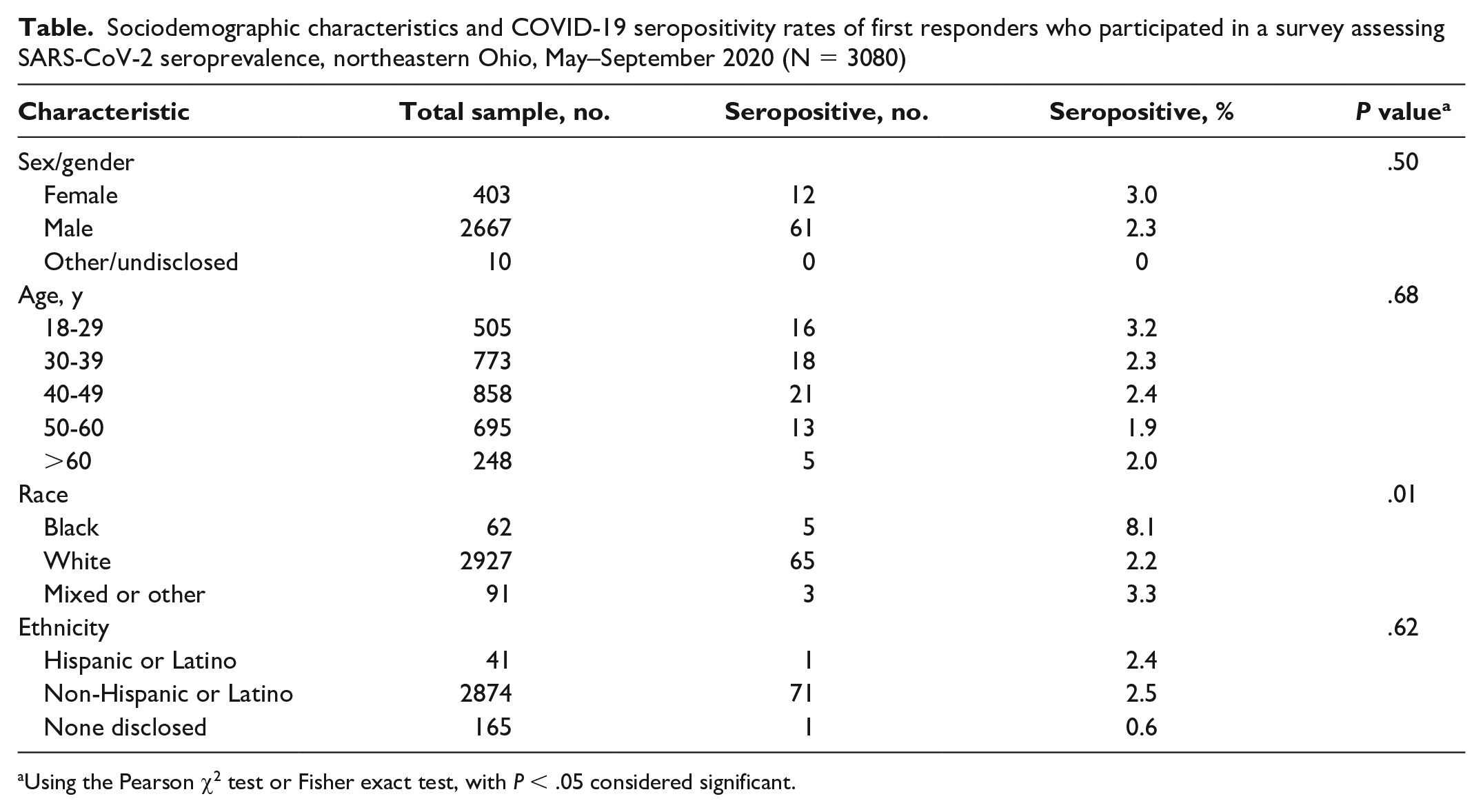
Using the Pearson χ2 test or Fisher exact test, with P < .05 considered significant.
Self-reported community exposure differed significantly by occupation (Figure 1). Most first responders who reported community exposure to COVID-19 were paramedics (22.6%), firefighters (19.5%), and EMTs (16.5%), whereas only 6.6% of law enforcement officers and 2.5% of administrative/support staff reported community exposure. We found no correlation between community exposure rate and seropositivity rate (P = .73). However, we did find a strong correlation between work exposure rate and community exposure rate across occupations (correlation coefficient = 0.99; P = .001).
Seroprevalence and Self-Reported Exposure by Age, Gender, and Race
Female participants had a numerically higher seropositivity rate than male participants did, but the difference was not significant (Figure 2). Seroprevalence was numerically higher among younger participants (aged 18-30 years) than among other age groups, but the difference was not significant. Black participants had a significantly higher positivity rate than White participants did (RR = 3.63; 95% CI, 1.52-8.70; P = .01).
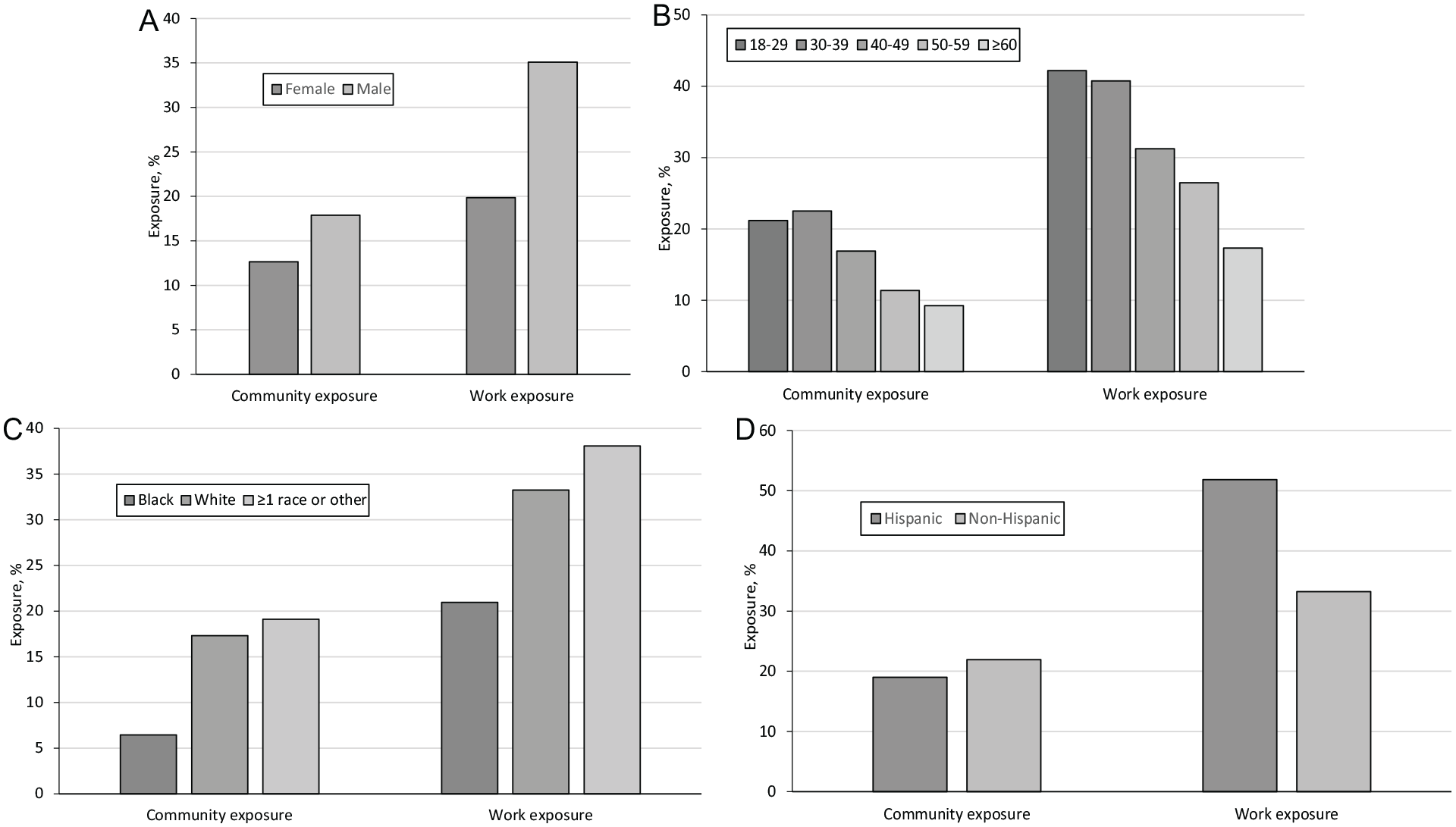
Participants’ self-reported exposure to COVID-19 patients at work and in the community, by age, gender, race, and ethnicity, among 3080 first responders in northeastern Ohio, May–September 2020. (A) Male participants had a significantly higher self-reported exposure rate associated with work than female participants did (P = .001 for work exposure; P = .012 for community exposure). (B) Younger participants (aged <50 years) had a significantly higher exposure rate than older participants (aged ≥50 years) both at work and in the community (P = .001 for work exposure; P = .001 for community exposure). (C) Black participants reported a notably lower community exposure rate than participants who were White or mixed race (P = .04). (D) Hispanic and non-Hispanic groups had similar self-reported exposure. Overall, the self-reported work exposure and community exposure rates were strongly correlated (correlation coefficient = 0.81; P = .001) regardless of sex/gender, age, or race. Comparisons were made using the Pearson χ2 test or Fisher exact test, with P < .05 considered significant.
Male participants reported a similar community exposure rate but significantly higher work exposure rate than female participants did (Figure 2). The work exposure rate was 35.1% among male participants and 19.9% among female participants. Black participants reported significantly lower community exposure than White participants did (6.5% vs 17.3%; P = .04). Older participants (aged ≥50 years) had lower rates of work and community exposure than younger participants did. The work exposure rate was positively correlated with the community exposure rate (correlation coefficient = 0.81; P = .001), independent of sex/gender, age, or race. However, neither the self-reported work exposure rate nor the community exposure rate correlated with the seropositivity rate. The seropositivity rate was not significantly different between participants with and without self-reported exposure (Figure 3).
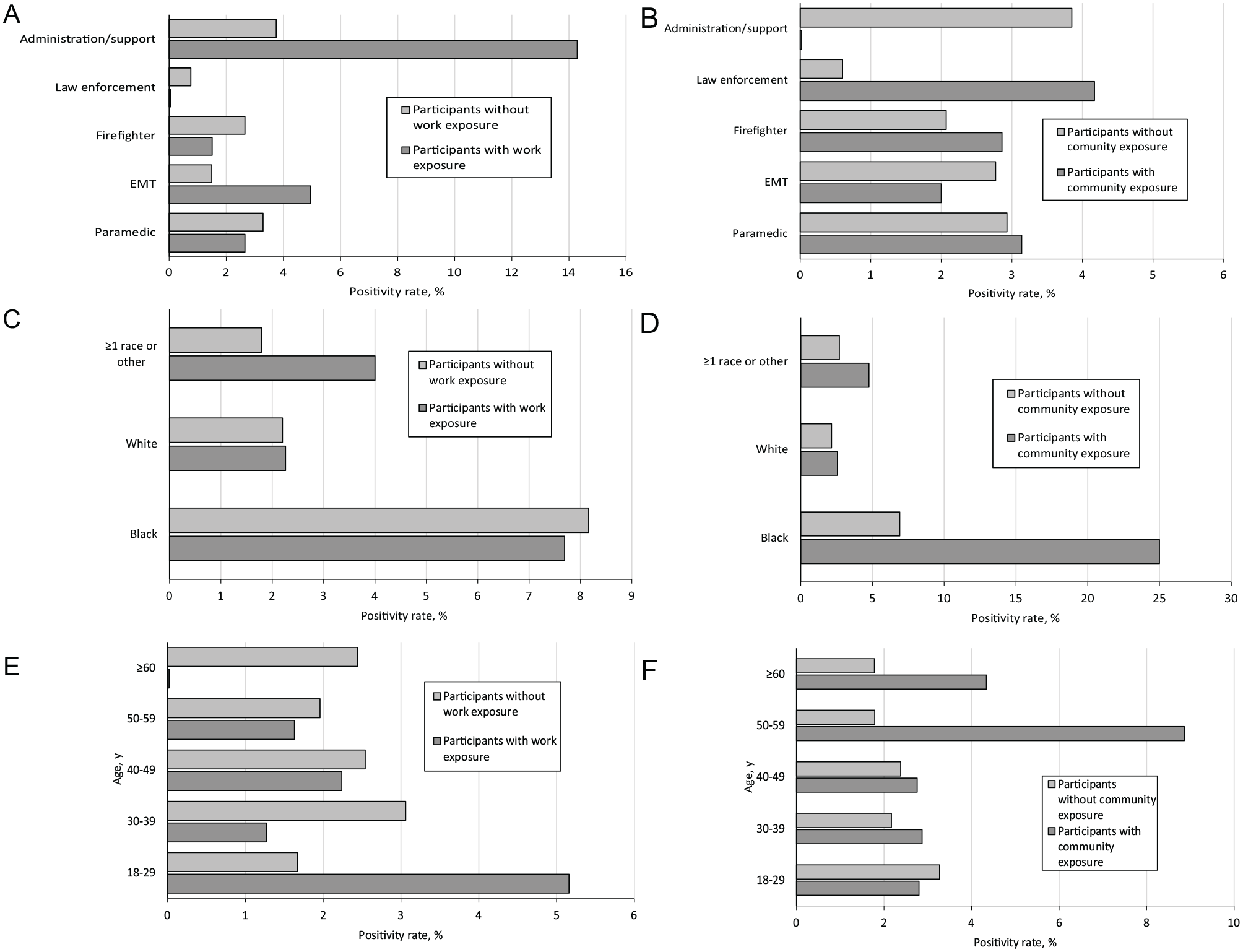
Self-reported exposure and SARS-CoV-2 seropositivity rate by occupation, race, and age, among 3080 first responders in northeastern Ohio, May–September 2020. The seropositivity rate between participants with and without SARS-CoV-2 exposure was not significantly different by occupation, race, or age. Seropositivity rate between participants with and without work exposure by occupation (A), race (C), and age (E). Seropositivity rate between participants with and without community exposure by occupation (B), race (D), and age (F). Some subgroups had a numerically higher seropositivity among exposed participants than among participants who were not exposed. However, the difference was not significant. Comparisons were made using the Pearson χ2 test or Fisher exact test, with P < .05 considered significant. Abbreviation: EMT, emergency medical technician.
History of COVID-19 RT-PCR Test Among Study Participants
Among the 3080 participants, 267 reported a history of being tested using the COVID-19 real-time polymerase chain reaction (RT-PCR) test. The RT-PCR testing rate among participants with symptoms was 29.3%. Of 3080 participants who were tested, 26 (0.8%) reported a positive RT-PCR test result, 17 (65.4%) of whom were also seropositive.
Antibody Index Values
The antibody index among seropositive participants was significantly higher than the index among seronegative participants (P = .001; Figure 4). Among seropositive participants, the median antibody index was 3.5 for participants without a PCR test result, 6.4 for participants with a negative PCR test result, and 4.5 for participants with a positive historical PCR test result. The difference associated with PCR testing status was not significant. Among seronegative participants, the median index was 0.03 for participants without a PCR test result, 0.03 for participants with a negative PCR test result, and 0.65 for participants with a positive PCR test result. The median index of PCR-positive but antibody-negative participants was significantly higher than other seronegative participants who were either negative or not tested by a PCR test (P = .01; Figure 4). Their antibodies were tested 39 to 142 days after the positive PCR test result. Without longitudinal data, we could not determine if the elevated-but-below cutoff index values represented waning antibody levels over time, less robust initial humoral immune response, or both. In addition, the antibody index was not significantly different between seropositive participants with or without symptoms.
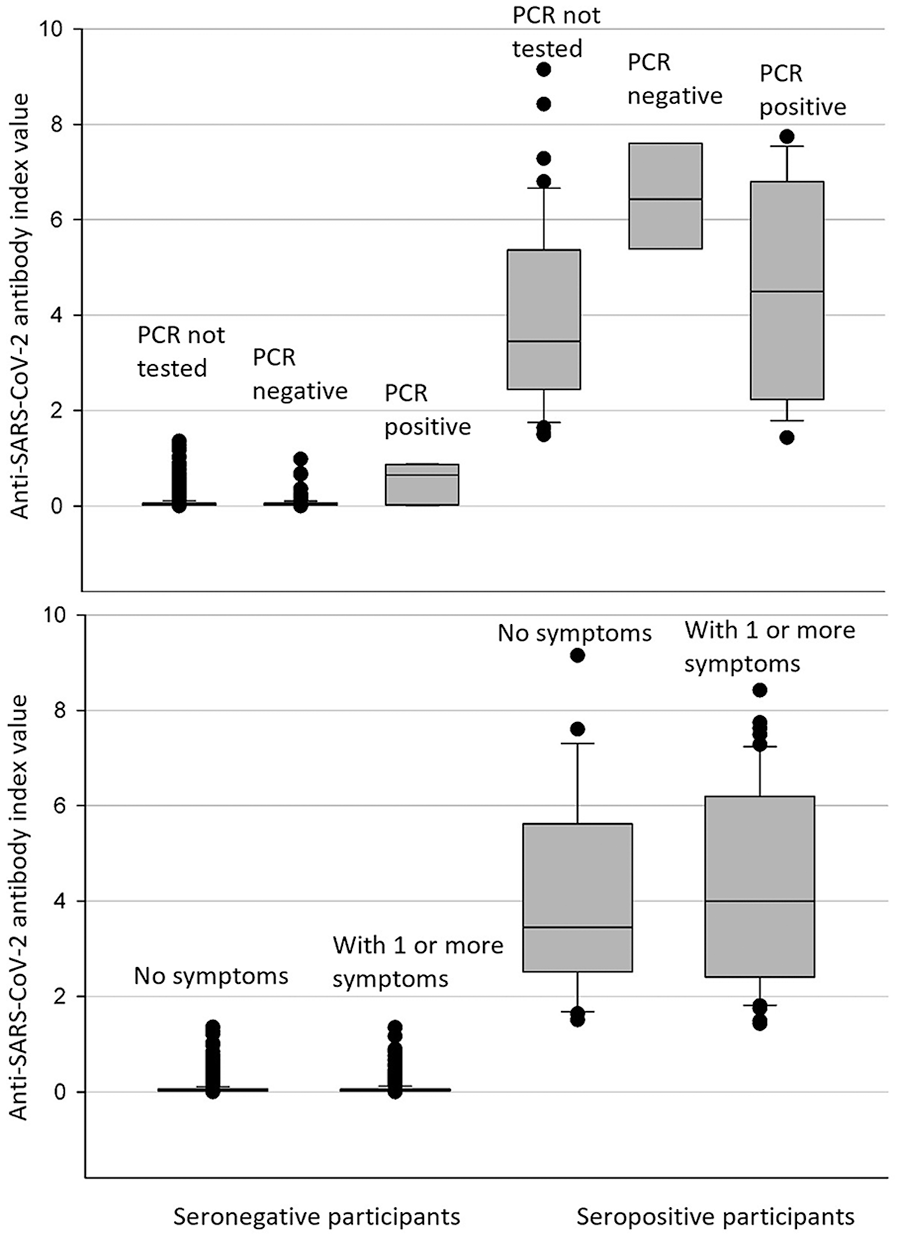
Anti–SARS-CoV-2 immunoglobulin G antibody index values by polymerase chain reaction (PCR) testing status and COVID-19–related symptoms among 3080 first responders in northeastern Ohio, May–September 2020. (Top) Index value among PCR-positive, PCR-negative, or PCR–not performed participants. Among antibody-negative participants, those with a previous positive PCR test result had a higher median index (0.65) than those who were PCR negative (0.03) or not tested seronegative (0.03). No significant difference in index values was found among seropositive participants regardless of PCR testing status. (Bottom) The median antibody index was slightly higher among seropositive participants who reported ≥1 COVID-19–related symptom than among seropositive participants who had no symptoms, but the difference was not significant. The boundary of the box closest to zero indicates the 25th percentile, a line within the box marks the median, and the boundary of the box farthest from zero indicates the 75th percentile. Error bars indicate the 90th and 10th percentiles. The circles indicate outlying points. Comparisons between 2 groups were made using the Mann–Whitney rank-sum test. Comparisons among 3 groups were made using 1-way analysis of variance (ANOVA) or Kruskal–Wallis 1-way ANOVA on ranks. P < .05 was considered significant.
Self-Reported Symptoms and Correlation With Seroprevalence
Of 73 seropositive participants, 39 (53.4%) reported ≥1 symptom and 34 (46.6%) were asymptomatic. Nearly one-third of seronegative participants (943 of 3007, 31.4%) also reported diverse symptoms. Loss of smell or taste was a common and relatively specific symptom for COVID-19, with an odds ratio of 19.99 (95% CI, 11.08-36.07; online-only Supplementary Table). Shortness of breath, fever, muscle ache, and diarrhea occurred 2 or 3 times more frequently among seropositive participants than among seronegative participants. Cough, sore throat, and runny or stuffed nose were common and presented at a similar rate among seropositive and seronegative participants. Conjunctivitis or red eye was rare (<5%) and had no strong correlation with COVID-19 seropositivity in this population.
Discussion
Epidemiologic studies assessing SARS-CoV-2 exposure and infection rates among first responders are limited. Even though each study generates only a snapshot, combining snapshots from various time frames, demographic regions, and organizations could provide comprehensive information to counter future emerging infections. Our study evaluated COVID-19 seroprevalence and exposure among first responders with 3080 participants across diverse job duties during the first and second waves of the pandemic in the United States.
Despite their limitations, serological tests are important tools for assessing SARS-CoV-2 infection and potential immunity. Ninety antibody assays had received Emergency Use Authorization from the US Food and Drug Administration by November 6, 2021. 10 In general, laboratory-based assays, especially chemiluminescent microparticle immunoassay performed on fully automated analyzers, have higher specificity than rapid tests (later flow immunoassay) according to performance characteristics. 11 Assay specificity is critical for reducing false-positive rates in large-scale surveys among populations with a low prevalence of disease. Per the manufacturer’s package insert, the assay used in our study was estimated to have 100% sensitivity (>14 days after symptom onset) and 99.6% specificity. An independent evaluation study by Bryan et al also confirmed excellent specificity (99.9%) of this assay. 12 The estimated positive predictive value and negative predictive value at a prevalence of 5% were calculated to be 93.4% and 100.0%, respectively. 12
By occupation, paramedics, EMTs, and firefighters showed similar seropositivity rates of 2% to 3%, which were slightly lower than seropositivity rates among administrative or support staff. Our analysis of self-reported exposure confirmed that these 3 occupations had high work-related exposure to COVID-19 patients. The average exposure rate of these 3 occupations (39.2%) was about 5 times higher than the exposure rate among occupations (eg, administrative/support staff) that do not need to encounter known or suspected COVID-19 patients. Although the study survey did not assess PPE use, proper PPE wearing is part of the required training and workplace policy at UHHS and its affiliated facilities. Taken together, the results suggest the effectiveness of the safety measures and PPE in protecting first responders from work-related infection. This notion is also supported by comparing COVID-19 prevalence in the general population. The Ohio statewide prevalence of current and past COVID-19 infection was estimated to be 0.9% and 1.5%, respectively, by the end of July 2020. 13 These data were from a study conducted by the Ohio Department of Health and The Ohio State University during July 9-28, 2020, on 727 Ohio adults using PCR and antibody tests in combination with mathematical models. In our study, 2413 participants had been tested by the end of July, with a positivity rate of 2.2%.
To date, studies have reported a wide range of seroprevalence among first responders. The lowest positivity rate was 0.73% in a serosurvey conducted in Texas in May 2020. 4 The highest positivity rate was 22.5% in a study conducted in New York City from May to July 2020. 14 The study in New York City was 1 of 2 large-scale studies that had more than 1000 first-responder participants. Besides the overall high seroprevalence, the study in New York City reported notably higher seroprevalence among EMTs (38.3%) compared with administrative staff (18.6%). It highlights increased occupational risk when facing overwhelming population infection. The other large-scale study, which was conducted by the Centers for Disease Control and Prevention (CDC) from May to June 2020, included about 2000 first responders in the Detroit metropolitan area and Michigan. The reported seropositivity rate was 5.2%. Similar to our results, the seropositivity rate among first responders was lower than among administrative staff/clerks (8.0%). 15 Among the various occupations, law enforcement officers had the lowest sero-prevalence (0.8%) in our study. This finding is also consistent with the CDC study, which reported low seroprevalence among police/corrections officers as compared with EMS, firefighters, and health care workers. 15 Similar to other studies,16 -18 our results also showed a trend of higher sero-prevalence among Black participants than among other racial and ethnic groups. The self-reported exposure at work and community was much lower among Black participants compared with White participants. The notably lower exposure, unlikely to reflect the actual risk, may rather suggest unrecognized exposure related to potentially low access to diagnostic testing and a high rate of asymptomatic infection in the community.
The finding of a significantly higher seropositivity rate compared with PCR positivity rate (2.4% vs 0.8%, P = .001) is consistent with other serology surveys.16,19,20 In addition, we found a strong correlation (r = 0.83; P = .006) between the seropositivity rate and PCR positivity rate across occupations, race, and gender. The seropositivity rate was estimated to be 3.2 ± 0.9 times the PCR positivity rate. This estimation is similar to the 2.5 ratio in the CDC study, which reported 6.9% seroprevalence among 16 403 health care workers and first responders, with 2.7% having a history of a positive RT-PCR test result. 15 There are multiple potential underlying reasons for the higher seroprevalence rate versus PCR positivity rate. First, nearly half of seropositive participants (46.6%) reported no COVID-19–related symptoms. These asymptomatic participants were unlikely to seek diagnostic testing. Second, the PCR testing rates among symptomatic participants were as low as 30% among first responders. Finally, 7 PCR-negative participants were seropositive. Given the high specificity of the antibody assay and high SARS-CoV-2 index values of those samples, these PCR-negative but seropositive participants are likely to be true positives missed by the RT-PCR test or infected after RT-PCR testing, which accounts for 9.6% of seropositive participants.
Limitations
This study had several limitations. First, 9 of 26 (34.6%) participants with previous positive COVID-19 PCR test results were seronegative, indicating that the seropositivity rates among first responders may have been underestimated in our study. The underestimation may be attributed to attenuated antibody concentration over time, a weak humoral immune response associated with mild symptoms, or production of antibodies not targeting the nucleocapsid protein. Second, self-reported exposure was not further categorized by duration, distance, or PPE use. Third, the survey questions were designed to balance between information collection and time constraints. Some valuable details were challenging to collect from busy first responders during a pandemic.
Conclusion
This study showed that first responders in northeastern Ohio had a similar infection rate to their coworkers whose duties did not involve direct patient contact. The results may reflect the effectiveness of infection control practice during the first 9 months of the pandemic. In addition, the high rate of asymptomatic infection and miscorrelation between seropositivity rate and self-reported exposure might underscore a risk posed by undiagnosed COVID-19 infections. With the emergence of the highly transmissible SARS-CoV-2 Omicron variants in fall 2021, future studies investigating post–Omicron-era seroprevalence will be beneficial for evaluating and improving infection control measures for first responders.
Supplemental Material
sj-docx-2-phr-10.1177_00333549221119143 – Supplemental material for SARS-CoV-2 Seroprevalence Among First Responders in Northeastern Ohio, 2020
Supplemental material, sj-docx-2-phr-10.1177_00333549221119143 for SARS-CoV-2 Seroprevalence Among First Responders in Northeastern Ohio, 2020 by Xiaochun Zhang, Elie Saade, Jaime H. Noguez and Christine Schmotzer in Public Health Reports
Supplemental Material
sj-jpeg-1-phr-10.1177_00333549221119143 – Supplemental material for SARS-CoV-2 Seroprevalence Among First Responders in Northeastern Ohio, 2020
Supplemental material, sj-jpeg-1-phr-10.1177_00333549221119143 for SARS-CoV-2 Seroprevalence Among First Responders in Northeastern Ohio, 2020 by Xiaochun Zhang, Elie Saade, Jaime H. Noguez and Christine Schmotzer in Public Health Reports
Supplemental Material
sj-xlsx-3-phr-10.1177_00333549221119143 – Supplemental material for SARS-CoV-2 Seroprevalence Among First Responders in Northeastern Ohio, 2020
Supplemental material, sj-xlsx-3-phr-10.1177_00333549221119143 for SARS-CoV-2 Seroprevalence Among First Responders in Northeastern Ohio, 2020 by Xiaochun Zhang, Elie Saade, Jaime H. Noguez and Christine Schmotzer in Public Health Reports
Footnotes
Acknowledgements
The authors thank all participants for their contribution in expanding our knowledge about COVID-19 epidemiology. We also thank the UH EMS Training and Disaster Preparedness Institute, Eileen Terrell and the Harrington Heart and Vascular Institute Research staff, University Hospitals Laboratories staff, and the RedCap team, whose efforts made this study possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This study was supported by the generosity of independent donors who were interested in funding COVID-19–related diagnostics for first responders and health care workers. The fund was given to the University Hospitals Internal Office of Development. The study team has no knowledge of the identity of the donors. The study team independently designed the study, selected assay reagents, and executed the study. Due to the anonymous nature of the donation, further conflicts of interest cannot be determined.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.