
Abstract
Objectives:
Overnight camps are a setting where COVID-19 can easily spread without the diligent use of layered public health interventions. We evaluated 20 camps in the United States to examine COVID-19 transmission and mitigation strategies during summer 2021.
Methods:
For this descriptive cross-sectional study, we examined self-reported information from 20 camps in 6 predominantly northeastern states on geographic information, tests and testing cadences, vaccination rates, and number of COVID-19 cases during summer 2021. Because the camps had hired public health consultants to guide them on reducing COVID-19 introduction and spread, all camps implemented similar interventions, including encouraging behaviors that lower the risk of COVID-19 transmission prior to camp arrival, use of cohorts, testing before and after arrival, and strong encouragement of vaccination among eligible campers and staff members.
Results:
A total of 9474 attendees at the 20 camps came from geographically diverse regions. Camps generally tested before and at arrival, as well as once or twice after arrival. Rates of vaccination were high among staff members (84.6%) and campers (76.2%). Camps identified 27 COVID-19 cases, with 17 (63.0%) detected after arrival, 3 (7.4%) detected on arrival, and 8 (29.6%) detected prior to arrival.
Conclusions:
The spread of cases detected after arrival to overnight camps was limited by the use of 3 key interventions: (1) high vaccination rates, (2) a rigorous and responsive testing strategy, and (3) ongoing use of public health interventions. These findings have implications for successful operation of overnight camps, residential schools and colleges, and other similar settings.
The COVID-19 pandemic led to the closure of 124 000 public and private schools in the United States, affecting at least 55.1 million students through the 2020-2021 school year. 1 Similarly, many out-of-school programs for young people in the United States, including 82% of 8947 overnight camps, did not operate in summer 2020. 2 Overnight camps that opened in the 2020 season had variable successes with prevention and mitigation of SARS-CoV-2, with some experiencing outbreaks3,4 and others operating successfully with layered strategies to identify and prevent transmission. 2
As many US schools opened for in-person learning during the 2020-2021 school year, the experiences of the summer camps that operated successfully in 2020 laid a foundation for school COVID-19 operations. 2 Subsequently, schools demonstrated that nonpharmaceutical interventions (NPIs; eg, wearing face masks, practicing social distancing, testing), when layered and diligently applied, can prevent and mitigate SARS-CoV-2 transmission among children.5 -9
Overnight camps face unique COVID-19 challenges; for example, wearing a face mask and socially distancing from others cannot be done during activities such as sleeping, eating, and swimming because of space and other logistic reasons. Even as COVID-19 transitions to endemic status, camps must implement strategies to overcome these challenges and provide a healthy environment for children. The experiences of camps in summer 2021 can provide a starting point for implementing plans going forward. Specifically, in a study of 9 camps, high vaccination rates combined with layered NPIs prevented COVID-19 cases through early identification of cases and prevention of spread. 10
In 2021, the more transmissible Delta variant rose from 13% of isolates at the beginning of the camp season to >95% of isolates by late July, while camps were in the midst of their seasons. By that time, multiple outbreaks were reported among summer camps in Missouri, New York, Ohio, and Texas, 11 with scant layering of NPIs, use of testing, and vaccination.
In this study, we examined a group of US camps that operated in summer 2021. We retrospectively surveyed this camp cohort on COVID-19 outcomes to evaluate the effects of various NPIs on camp operations, cases, and outbreaks.
Methods
In this descriptive cross-sectional study, we requested 20 overnight camps in 6 states serving children aged 7-15 years to self-report geographic information, NPIs, tests and testing cadences, vaccination rates, and cases of COVID-19 during summer 2021. Medical directors, health staff, and directors at each camp provided the study information. All 20 camps hired public health consultants to guide them in preparation for COVID-19 during the 2021 camp season. All camps working with consultants agreed to participate in a survey at the end of the summer. Camps and their health staff received monthly consulting sessions before the camp season on up-to-date best practices for NPIs and use of testing in the camp setting. With this training, each camp chose similar public health interventions aligned with state and local guidance, which included practices before and after arrival to camp and guidance on how to respond to symptomatic attendees and close-contact testing. All camps asked attendees to limit activities to behaviors that lower the risk of COVID-19 transmission prior to camp (ie, not attending large groups, wearing a face mask when outside their family unit), and all camps developed protocols that eliminated offsite camp travel until attendees showed negative test results. All camps used hygiene, increased cleaning, and maximized outdoor programming. Camps operated with varying populations, session numbers, and durations. After the end of the summer 2021 camp sessions, all camps submitted self-reported data using a structured Microsoft Excel workbook. Data were collected and verified during August and September 2021. The institutional review board of the University of Virginia determined that the study was exempt from institutional review board review.
To maintain confidentiality, we deidentified data for the analyses. To ensure reproducibility, we used R version 4.1.1 (R Foundation for Statistical Computing) and related software and packages to combine, clean, and analyze the data.12,13 Our study team evaluated the data for completeness, uniqueness, validity, accuracy, and consistency before and during formal analyses. We contacted camps to provide any missing information and to resolve erroneous data entries. Because of personal preferences of individual analysts working on the project and institutional analytic verification recommendations, we also used SAS version 9.4 (SAS Institute, Inc) and Microsoft Excel for further analysis and verification.
Results
Among the 9474 attendees in the 20 overnight camps included in the study, 6814 were campers and 2660 were staff members. Camps averaged 435 attendees (range, 201-1463). The campers’ home regions were as follows: 23.0% Northeast, 41.0% mid-Atlantic, 13.4% South, 7.9% Midwest, 9.5% West and West Coast, and 4.6% international (Table 1). Fourteen camps conducted 2 or 3 camp sessions (range, 1-5 sessions). The average duration of full sessions was 49 days (range, 28-56 days), and the average duration of half sessions was 28 days (range, 21-35 days). Camps offering other session lengths averaged 22.4 days (range, 21-35 days; Table 2).
Home region and vaccination status of campers and staff members from 20 overnight camps, United States, summer 2021 a
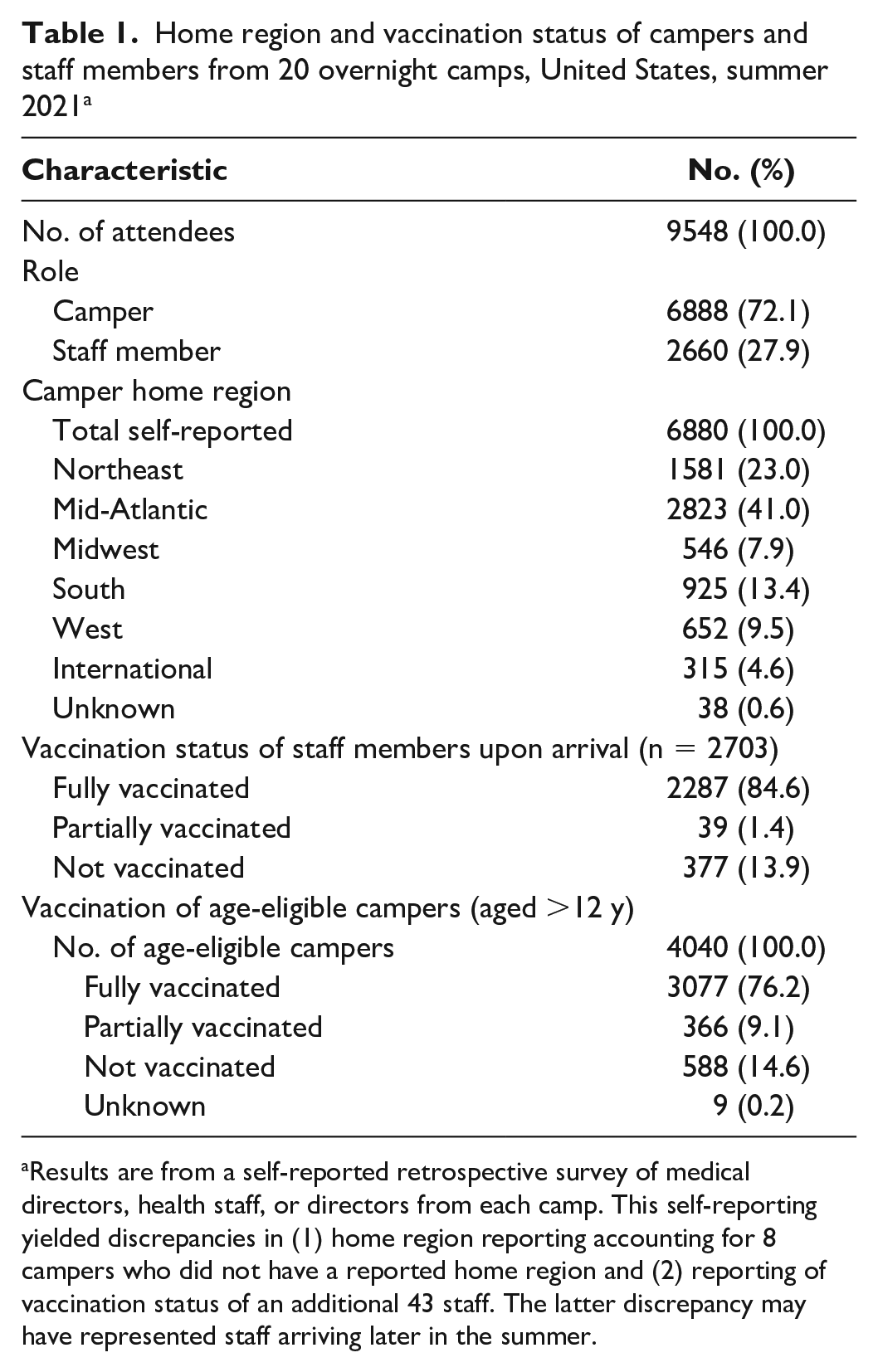
Results are from a self-reported retrospective survey of medical directors, health staff, or directors from each camp. This self-reporting yielded discrepancies in (1) home region reporting accounting for 8 campers who did not have a reported home region and (2) reporting of vaccination status of an additional 43 staff. The latter discrepancy may have represented staff arriving later in the summer.
Selected characteristics of 20 overnight camps, United States, summer 2021 a
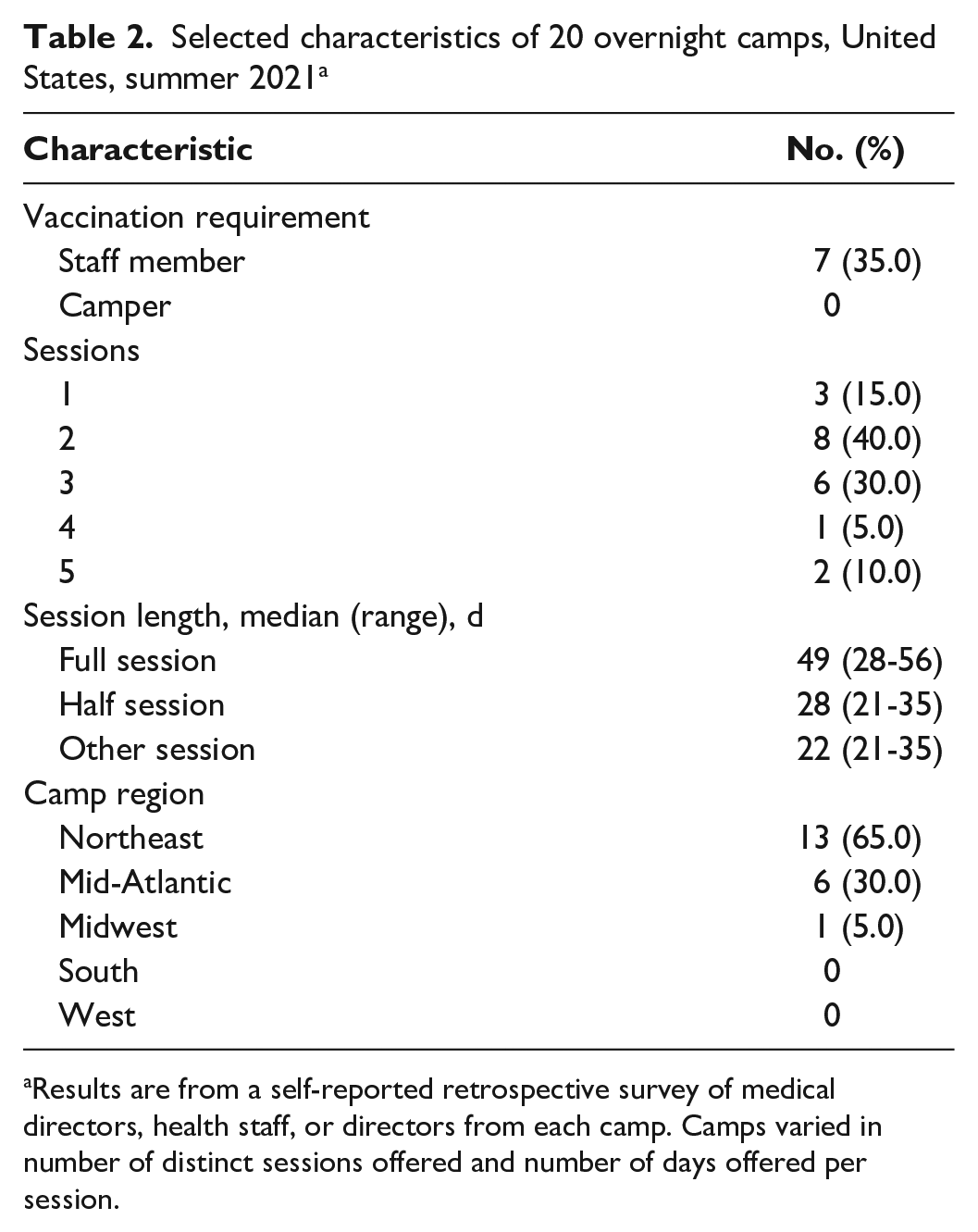
Results are from a self-reported retrospective survey of medical directors, health staff, or directors from each camp. Camps varied in number of distinct sessions offered and number of days offered per session.
All camps recommended COVID-19 vaccination for staff members and age-eligible campers (ie, children aged ≥12 y). Seven camps required vaccination for their staff as a condition of employment, and 1 camp required vaccination for age-eligible campers. Across all camps, 84.6% of staff members were fully vaccinated at the beginning of camp, 1.4% were partially vaccinated at the beginning of camp, and 13.9% arrived unvaccinated but were vaccinated while at camp; 1.0% of staff members remained unvaccinated throughout the camp season. Of the 6814 campers, 59.3% (n = 4040) were aged ≥12 years at the beginning and, thus, eligible for the Pfizer BioNTech vaccine. Among eligible campers, 3077 (76.2%) were fully vaccinated at the beginning of camp and 366 (9.1%) were partially vaccinated at arrival (Table 1), with 21 (0.5%) starting vaccination while at camp.
Camps implemented similar NPIs. Seventeen camps required attendees to engage in low-risk behaviors, and 19 camps (95%) screened for symptoms that could be concerning for COVID-19. In addition, all camps used cohorts to limit the spread of COVID-19, with a median initial cohort size of 14 children (range, 6-40 children). The initial cohort was by cabin for 17 camps (85%) and by age group for 2 camps, with the remaining camp using cohorts defined by age ranges. After test results for COVID-19 came back negative, 18 camps expanded cohorts and 10 camps eliminated cohorts. Eight camps limited the capacity of the camp to leave bunk space for potential isolation or quarantine if needed.
Camps did not require face masks when attendees were within their cohort because of the inability to wear face masks while sleeping and eating. Camps required face masks generally when attendees interacted with others outside their cohorts, with differences in requirements for face masks according to vaccination status and indoor versus outdoor activities. For example, for unvaccinated attendees outside their cohort, 8 camps required face masks in both indoor and outdoor settings, whereas 11 camps required them only in indoor settings. Similarly, when vaccinated attendees were outside their cohort, 6 camps required attendees to wear face masks indoors and outdoors and 10 camps required them indoors only. Four camps did not require face masks for vaccinated attendees at all. With negative testing, camps often would increase the cohort size, allowing for unmasked interactions among larger groups of campers and staff members.
Camps also varied on how they handled the behavior of unvaccinated staff members. Fifteen camps required unvaccinated staff members to remain on site throughout the camp season, and 15 camps also required limited interactions between unvaccinated staff members and other unvaccinated individuals on and off campus.
Unlike the 2020 season, in 2021, camps could generally access testing as needed, including both on-site and laboratory-based approaches. All 20 camps required a written prearrival negative polymerase chain reaction (PCR) test result for SARS-CoV-2 at the start of the first session, with 13 camps requiring testing for unvaccinated attendees only and 7 camps requiring testing regardless of vaccination status. Camps collected results of 5509 prearrival tests (median = 270). Eighteen camps tested attendees upon arrival, with 12 testing unvaccinated attendees only and 6 testing both vaccinated and unvaccinated attendees. Among the camps that tested on arrival, 17 camps used rapid antigen tests and 1 used molecular tests. Camps performed 5173 arrival tests (median = 272; range, 0-900).
Camps generally implemented serial testing after arrival in 1 of 2 ways (Table 3). At the start of the summer, 10 camps tested twice after arrival and 10 camps tested once after arrival. Camps performed 6252 tests (median = 317) after arrival. Two camps also conducted ongoing serial testing of unvaccinated staff members by testing them either weekly or twice per week even if asymptomatic.
SARS-CoV-2 testing cadence after arrival to overnight camps (n = 20), United States, summer 2021 a
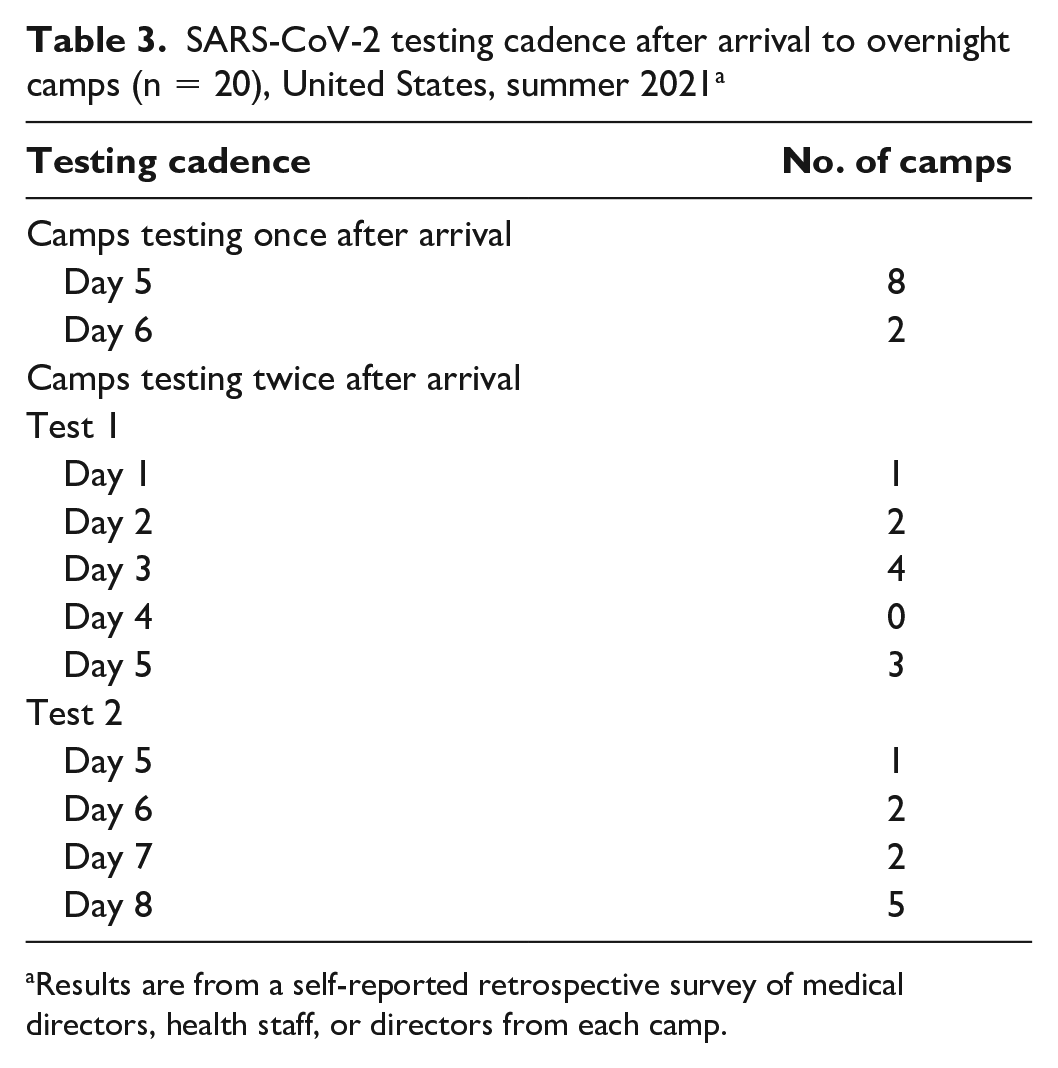
Results are from a self-reported retrospective survey of medical directors, health staff, or directors from each camp.
Overall, camps reported 27 confirmed COVID-19 cases (7 staff members, 20 campers). Eight asymptomatic cases were identified through prearrival testing (1 staff member, 7 campers), and 2 asymptomatic cases were identified through on-arrival testing (2 staff members). Attendees identified with prearrival and on-arrival testing were denied entry into camp until they had isolated in accordance with guidelines from the Centers for Disease Control and Prevention (CDC). Testing after arrival identified 17 cases (4 staff members, 13 campers). Among these, 10 attendees were asymptomatic and had tested negative with a rapid test on arrival; however, serial testing within 6 days after arrival identified them as positive for SARS-CoV-2. Accordingly, these 10 cases had either not yet turned positive or the rapid test conducted on arrival was a false-negative result. The remaining 7 cases were symptomatic staff members with off-camp exposure (n = 3) or who had close contacts with asymptomatic cases through secondary transmission within a cabin (n = 4). These 7 cases are further described hereinafter. Nine of 17 COVID-19 cases identified through testing after arrival were isolated at camp, and 8 cases were sent home to isolate.
Contact tracing identified close contacts of all 17 cases identified after arrival, with a mean of 13 attendees quarantined (range, 3-39). Consistent with CDC guidance at the time, fully vaccinated attendees were not quarantined. Among the 11 camps that identified cases of COVID-19 through postarrival testing, 8 camps quarantined exposed attendees on campus and 3 camps sent attendees home to quarantine. Some local public health officials required unvaccinated exposed attendees to quarantine at home.
Three camps reported 1 case each where a vaccinated staff member was exposed to a COVID-19 case off campus and became positive; the staff members were tested for COVID-19 because of presence of symptoms. These positive test results all occurred ≥19 days after the start of camp. The 3 vaccinated staff members exposed a median of 13 attendees on campus (range, 10-17), 3 of whom were unvaccinated. No transmission was noted on follow-up testing of these exposed attendees.
Only 1 camp experienced on-campus transmission. An unvaccinated asymptomatic camper who had a negative test result both on day 3 before camp by PCR and on arrival by rapid antigen testing subsequently had a positive PCR test result on day 3 after arrival. Because of strict cohort practices by cabin, only 12 close contacts (9 campers, 3 staff members) were identified by contact tracing within the cohort. Of the 12 close contacts, 3 campers and 3 staff members were fully vaccinated. Four of the 12 exposed close contacts subsequently received a positive test result without symptoms (2 vaccinated, 2 unvaccinated), demonstrating a secondary attack rate of 33% for the cohort. Staff members isolated or quarantined on campus, whereas the original camper and exposed campers went home for isolation and quarantine, respectively. All campers returned to camp after appropriate duration of isolation and quarantine.
Overall, 0.15% of prearrival test results (n = 8 of 5509) were positive, 0.04% (n = 2 of 5173) of arrival test results were positive, and 0.3% of postarrival test results (a combination of scheduled serial, exposure, and symptomatic testing) were positive. Of 27 cases among campers, 21 (77.8%) campers were unvaccinated, 5 (18.5%) were vaccinated, and 1 (3.7%) was partially vaccinated.
When the Delta variant became the predominant strain in surveillance, 10 camps altered their testing strategies. Some camps that originally did not require tests for vaccinated campers before camp then required tests for all vaccinated and unvaccinated campers who came to camp in their later sessions. Two camps changed their testing cadence to have 2 postarrival tests (eg, from day 5 tests to both day 3 and day 7 tests). In addition, half of camps added testing to second session staff members returning from off-campus activities during the intersession and increased testing for COVID-19 among those who presented with cold symptoms. Twelve camps reduced the number of campers at the camp in response to the Delta variant.
Discussion
Diligent use of multiple NPIs, high vaccination rates, and early identification of COVID-19 through testing played an important role in preventing SARS-CoV-2 transmission in 20 overnight camps with differing locations and session lengths. Camps did not rely on testing or vaccination as a sole NPI; rather, camps also continued multilayered use of other NPIs. Notably, strict cohort practices allowed camps to successfully stop tertiary transmission by isolating cases to the primary cohort and quarantining exposed cohorts while continuing camp operations in other cohorts. High vaccination rates among staff members and age-eligible campers with early vigorous testing cadences allowed many camps to expand their camps to full cohorts.
Nearly all camps used multilayered NPIs alongside vaccination and testing. Camps screened for symptoms and low-risk behaviors before attendees arrived at camp, used small beginning cohort sizes (especially among unvaccinated age groups), required face masks outside cohorts, promoted hand hygiene, and maximized outdoor dining and programming.
Our study findings affirm that strong testing cadences can identify COVID-19 before camp or quickly upon arrival. All camps used testing before and after arrival, with most camps performing 2 postarrival tests. Among nearly 10 000 attendees, testing identified 27 COVID-19 cases, with only 1 from a transmission within camp. The early diligent use of NPIs, especially the use of cohorts to limit exposure, allowed 18 of 19 COVID-19 cases identified after arrival to result in no tertiary transmission outside the primary cohort. Nearly all staff members and 76% of eligible campers were vaccinated against COVID-19 by the end of summer 2021, which allowed camps to enjoy normalized programming after initial testing periods and likely contributed to lower in-camp transmission rates.
Limitations
This study had several limitations. First, the degree of adherence to NPIs was not measured, and, as such, their self-reported use may not reflect actual practice. Second, attendees were not tested at the end of the sessions, which might have led to missed asymptomatic transmission. Third, the high vaccination rates among staff members may limit the generalizability of these findings to other settings that have lower vaccination rates. Fourth, camps in this study were self-selected and may not be representative of all camps in the United States. In addition, camps included in this study used relatively high levels of NPIs. That is, all 20 camps hired public health consultants to guide them in preparation for COVID-19 during the 2021 camp season and, as such, may not be representative of all overnight camps. Thus, these findings cannot be compared with camps not following these strategies, which would be necessary to fully evaluate NPI effectiveness. Finally, survey responses were self-reported, and aggregate numbers and sums of variables were discordant at times. We found this discrepancy in 2 self-reported variables of camper home region and staff vaccination status on arrival, which likely represented either staff entry after opening of camp or entry errors/misinterpretations by respondents. However, the discrepancy was small and did not alter the overall epidemiologic description of vaccination trends among the sample.
Conclusion
This study adds to previous camp studies on the use of NPIs to prevent SARS-CoV-2 transmission by demonstrating the importance of NPIs across multisession and geographically diverse camp programs in, to our knowledge, the largest analysis of COVID-19 cases in overnight camps to date. The study also highlights the role of vaccination and strong testing programs for preventing transmission at congregate facilities such as overnight camps. The Omicron variant, with its higher breakthrough rates of disease than previous variants, may require testing for symptomatic attendees in the camp setting even if high vaccination rates are achieved in 2022. High community immunity in camps combined with low community transmission may decrease the need for the mass asymptomatic screening testing used in camps in 2021. These findings have important implications for successful operation of overnight camps, residential schools and colleges, and other similar settings.
Footnotes
Acknowledgements
The authors thank the summer camp directors and health teams for their generous contributions to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.