
Abstract
Objectives:
We examined sociodemographic, clinical, and behavioral factors associated with previous incarceration among people with diagnosed HIV to inform HIV care efforts for this population.
Methods:
We used 2015-2017 data from a cross-sectional, nationally representative sample of US adults with diagnosed HIV (N = 11 739). We computed weighted percentages and 95% CIs to compare the characteristics of people with HIV incarcerated in the past 12 months (ie, recently) with people with HIV not recently incarcerated. We used adjusted prevalence ratios (aPRs) with predicted marginal means to examine associations between selected factors and incarceration status.
Results:
Adults with HIV who were recently incarcerated, when compared with those who were not, were more likely to be aged 18-29 years (prevalence ratio [PR] = 2.51), non-Hispanic Black (PR = 1.39), less educated (<high school diploma; PR = 1.41), unemployed (PR = 1.32), or living at or below the federal poverty level (PR = 1.64); to have recently experienced homelessness (PR = 4.56); and to have recently used drugs (PR = 1.68). Clinically, they were more likely to have been diagnosed with HIV in the past 5 years (aPR = 1.26), have lower CD4 counts (aPR = 1.45), have recently used the emergency department (aPR = 1.15), and have experienced severe anxiety (aPR = 1.50) and less likely to be retained in care, be recently virally suppressed, or have sustained viral suppression.
Conclusions:
Among people with HIV, recent incarceration was associated with increased health risks and worse health outcomes. Pre- and postrelease linkage-to-care interventions and reentry services might improve the health of recently incarcerated people with HIV.
The United States has the largest correctional population in the world; approximately 6.3 million people were supervised by adult correctional systems as of 2019.1,2 In the last 4 decades, the rate of incarceration in the United States increased >700%, and although the total number of people supervised by adult correctional systems decreased annually by 1.3% from 2009 to 2019, approximately 2 million people are incarcerated on any given day.2-5 Among people who were in prison in 2015, >17 000 had a diagnosed HIV infection. 6 HIV prevalence in correctional facilities is generally 5 times higher than in the general US population; 1 in 7 people with HIV infection is incarcerated and released each year.7-10 Furthermore, people who experience incarceration have a disproportionately high risk of HIV infection and often have risk factors associated with underuse of antiretroviral therapy (ART). 11 A history of incarceration negatively influences community-based HIV care and treatment postrelease.11-13
Every year, millions of people are released from correctional facilities, return to their communities, and encounter social, economic, and health system–related challenges affecting their ability to access and maintain HIV care.14-16 Understanding the social and clinical challenges of people with HIV who have been recently released from incarceration may inform interventions to provide appropriate HIV care and wraparound services (ie, nonmedical tailored services that fit one’s specific needs, such as housing and transportation) to improve their health outcomes. While prior studies have been limited to specific correctional facilities, cities, or populations (ie, injection drug users, patients currently receiving HIV care), our study used data from a nationally representative sample of US adults with diagnosed HIV, regardless of their HIV care status. We describe sociodemographic and clinical characteristics of recently incarcerated people with diagnosed HIV to identify factors associated with recent incarceration status.
Methods
Medical Monitoring Project
The Medical Monitoring Project (MMP) is an HIV surveillance system designed to collect annual nationally representative estimates of clinical and behavioral characteristics of people with diagnosed HIV infection in the United States. 17 From 2005 to 2014, MMP sampled people from HIV care facilities, and recruitment was limited to those who were receiving HIV medical care. To improve the usefulness of MMP data, in 2015, MMP began a new sampling method that included all adults diagnosed with HIV in the United States, regardless of HIV care status. These changes were made in response to recommendations that stemmed from an Institute of Medicine review of national HIV data systems; MMP methods are described elsewhere.17-20 Sampling eligibility required the participant to be alive, aged ≥18 years, diagnosed with HIV, and a resident of an MMP area (ie, 23 state and local health departments) at the time of sampling. Participants completed an interviewer-administered telephone or in-person survey, and medical records from their usual source of care were later abstracted. Incarcerated people may consider the care that they received in jail or prison as their usual source of care, in which case clinical data were requested from the correctional facility. Approximately 9700 people were sampled each year, and the response rates for the 3 samples included in this analysis were 40% (2015), 44% (2016), and 46% (2017).
Measures
Recent incarceration was defined as responding yes to the survey question “During the past 12 months, have you been arrested and put in jail, detention, or prison for longer than 24 hours?” among those whose survey setting was not “prison or jail facility.” We measured all covariates during the past 12 months except where otherwise noted. Sociodemographic factors included in this analysis were self-reported during the survey and included participants’ current sex/gender (male, female, transgender), age (18-29, 30-39, 40-49, ≥50 y), race and ethnicity (non-Hispanic White, non-Hispanic Black, Hispanic/Latino, other [American Indian/Alaska Native, Asian, Native Hawaiian/other Pacific Islander, or >1 race]), sexual orientation (lesbian, gay, bisexual, or something else; heterosexual or straight), education (<high school diploma, high school diploma/GED [General Educational Development], >high school diploma), marital status (married or in a civil union or domestic partnership, previously married [includes widowed, separated, and divorced], never married), employment status (employed, unemployed), household poverty level based on the US poverty guidelines 21 (>federal poverty level, ≤federal poverty level), type of health insurance (Ryan White or AIDS Drug Assistance Program, Medicare, Medicaid, or other public health insurance; private health insurance), and housing status (homeless or not homeless in the past 12 months; homelessness was defined as living on the street, in a shelter, in a single-room–occupancy hotel, or in a car at least once in the past 12 months).
The survey also assessed whether the person had ever taken or was currently taking ART, ART dose adherence (defined as 100% adherence to ART doses in the past 30 d), emergency department (ED) visits, hospital admissions, binge drinking (defined as ≥5 drinks in a single sitting for men and ≥4 drinks for women) in the past 30 days, and drug use. Responses to the items on the Patient Health Questionnaire were used to define depression during the past 30 days according to criteria from the Diagnostic and Statistical Manual of Mental Health Disorders, Fourth Edition. 22 Responses to the Generalized Anxiety Disorder Scale were used to measure mild, moderate, and severe anxiety during the past 30 days according to criteria from the diagnostic manual. 23 Health care discrimination was defined as experiencing any of 7 experiences of discrimination in an HIV care setting in the past 12 months. 24
HIV-related stigma was measured using a 10-item Likert scale (from 0 = no stigma to 100 = highest stigma) and encompassed the following stigma domains: personalized, disclosure, negative self-image, and public attitudes. 25 Clinical factors were abstracted from participants’ medical records from their usual source of HIV care during the 24 months prior to the MMP interview. Abstracted data included the following: retention in care in the last 12 and 24 months, defined as 2 elements of outpatient HIV care ≥90 days apart in each 12-month period (outpatient HIV care was defined as any documentation of the following: encounter with an HIV care provider, viral load test result, CD4 test result, HIV resistance test or tropism assay, ART prescription, pneumocystis pneumonia prophylaxis, or mycobacterium avium complex prophylaxis); CD4 count (CD4 T-lymphocyte count; cells/μL); viral load data, which included recent viral suppression (defined as HIV viral load undetectable or <200 copies/mL) and sustained viral suppression (defined as all viral loads in the last 12 months undetectable, <200 copies/mL); prescribed ART in past 12 months; and testing for gonorrhea, chlamydia, or syphilis.
Data Analysis
For this study, we analyzed matched data from surveys and medical record abstraction from 3 combined data collection cycles: 2015, 2016, and 2017 (data collected from June 2015 through May 2018) (N = 11 865). We removed participants who were currently incarcerated (n = 126) from the sample, resulting in a final sample of 11 739. We computed weighted estimates of percentages and 95% CIs to describe the characteristics of people with HIV by incarceration status, and we compared groups using prevalence ratios (PRs) with predicted marginal means and 95% CIs to assess significant differences; P < .05 was considered significant.
Next, we assessed associations between clinical, behavioral, and mental health factors and incarceration status while controlling for potential sociodemographic confounders and variables selected a priori based on literature and previous MMP studies: age, race, education, marital status, federal poverty level, drug use, and homelessness. We performed multivariate logistic regression to compute adjusted PRs and 95% CIs to assess the independent associations of selected dependent variables with incarceration status. We performed all analyses using SAS version 9.3 (SAS Institute, Inc) and SAS-callable SUDAAN (RTI International). The Centers for Disease Control and Prevention determined that the MMP was a public health surveillance, nonresearch activity. 26 Local institutional review board approval was obtained from each MMP project area when required. Informed consent was obtained from all participants. 17
Results
Sociodemographic Factors
Of 11 739 US adults with HIV who were not currently incarcerated, 475 (weighted 4.2%; 95% CI, 3.6%-4.7%) had experienced incarceration in the past 12 months. Among adults who were recently incarcerated, approximately 80% had been incarcerated 1 time in the past 12 months, 85% reported their last length of stay was ≤6 months (45.3% reported <1 week), and 42.8% reported being released >7 months prior to taking the MMP survey. Most (79.9%) recently incarcerated people were male, and 28.2% were aged ≥50 years (Table 1). More than half (55.9%) of recently incarcerated people identified as non-Hispanic Black, and 54.0% identified as heterosexual or straight. More than two-thirds (69.8%) of recently incarcerated people were unemployed, and 68.6% were living in a household at ≤federal poverty level. Approximately one-third (34.0%) had experienced homelessness in the past 12 months.
Characteristics of people diagnosed with HIV (N = 11 739), by incarceration status, Medical Monitoring Project, United States, 2015-2017 a
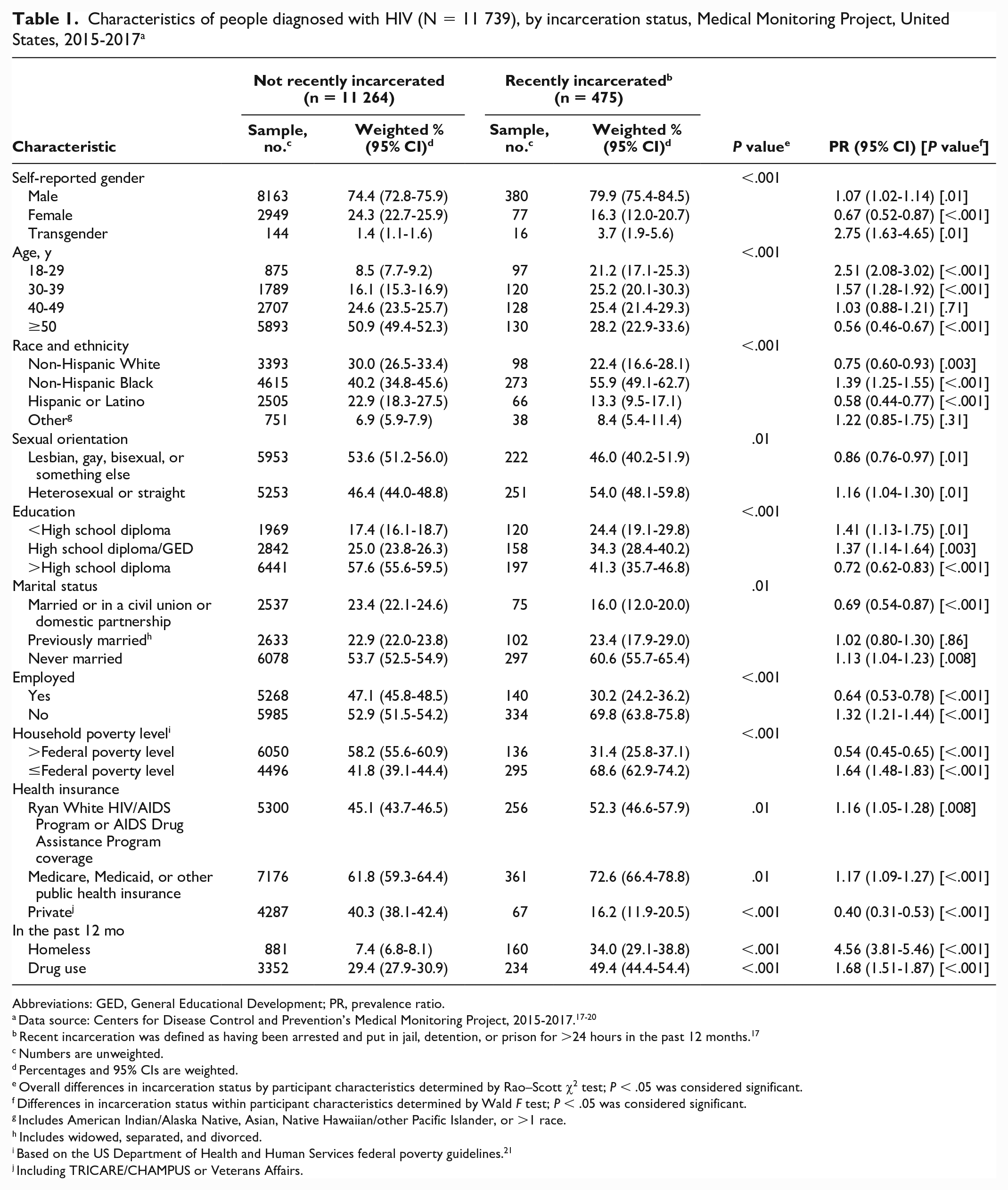
Abbreviations: GED, General Educational Development; PR, prevalence ratio.
Data source: Centers for Disease Control and Prevention’s Medical Monitoring Project, 2015-2017.17-20
Recent incarceration was defined as having been arrested and put in jail, detention, or prison for >24 hours in the past 12 months. 17
Numbers are unweighted.
Percentages and 95% CIs are weighted.
Overall differences in incarceration status by participant characteristics determined by Rao–Scott χ2 test; P < .05 was considered significant.
Differences in incarceration status within participant characteristics determined by Wald F test; P < .05 was considered significant.
Includes American Indian/Alaska Native, Asian, Native Hawaiian/other Pacific Islander, or >1 race.
Includes widowed, separated, and divorced.
Based on the US Department of Health and Human Services federal poverty guidelines. 21
Including TRICARE/CHAMPUS or Veterans Affairs.
In bivariate analyses, when compared with people who had not experienced incarceration in the past 12 months, recently incarcerated people were significantly more likely to identify as male or transgender, as non-Hispanic Black, or as heterosexual or straight; have never been married; be unemployed; be living in a household at ≤federal poverty level; have Ryan White or AIDS Drug Assistance Program assistance, Medicare, or Medicaid; have experienced homelessness; and have used drugs (Table 1). In contrast, recently incarcerated people were significantly less likely to be aged ≥50 years, have >high school diploma, be married or in a civil union or domestic partnership, and have private health insurance.
Clinical, Behavioral, and Mental Health Factors
In multivariate analysis, people with HIV who had been recently incarcerated, as compared with those who had not been recently incarcerated, were significantly more likely to have been diagnosed with HIV in the last 5 years, have a geometric mean CD4 count <200 copies/mL, have visited the ED in the past 12 months, have been admitted into a hospital in the past 12 months, and have experienced severe anxiety in the past 2 weeks (Table 2). When compared with people who had not been recently incarcerated, people who had been recently incarcerated were significantly less likely to be retained in care in the past 12 and 24 months, have a geometric mean CD4 count ≥500 copies/mL, be virally suppressed, and have sustained viral suppression.
Clinical, behavioral, and mental health characteristics of people diagnosed with HIV, by incarceration status, Medical Monitoring Project, United States, 2015-2017 a
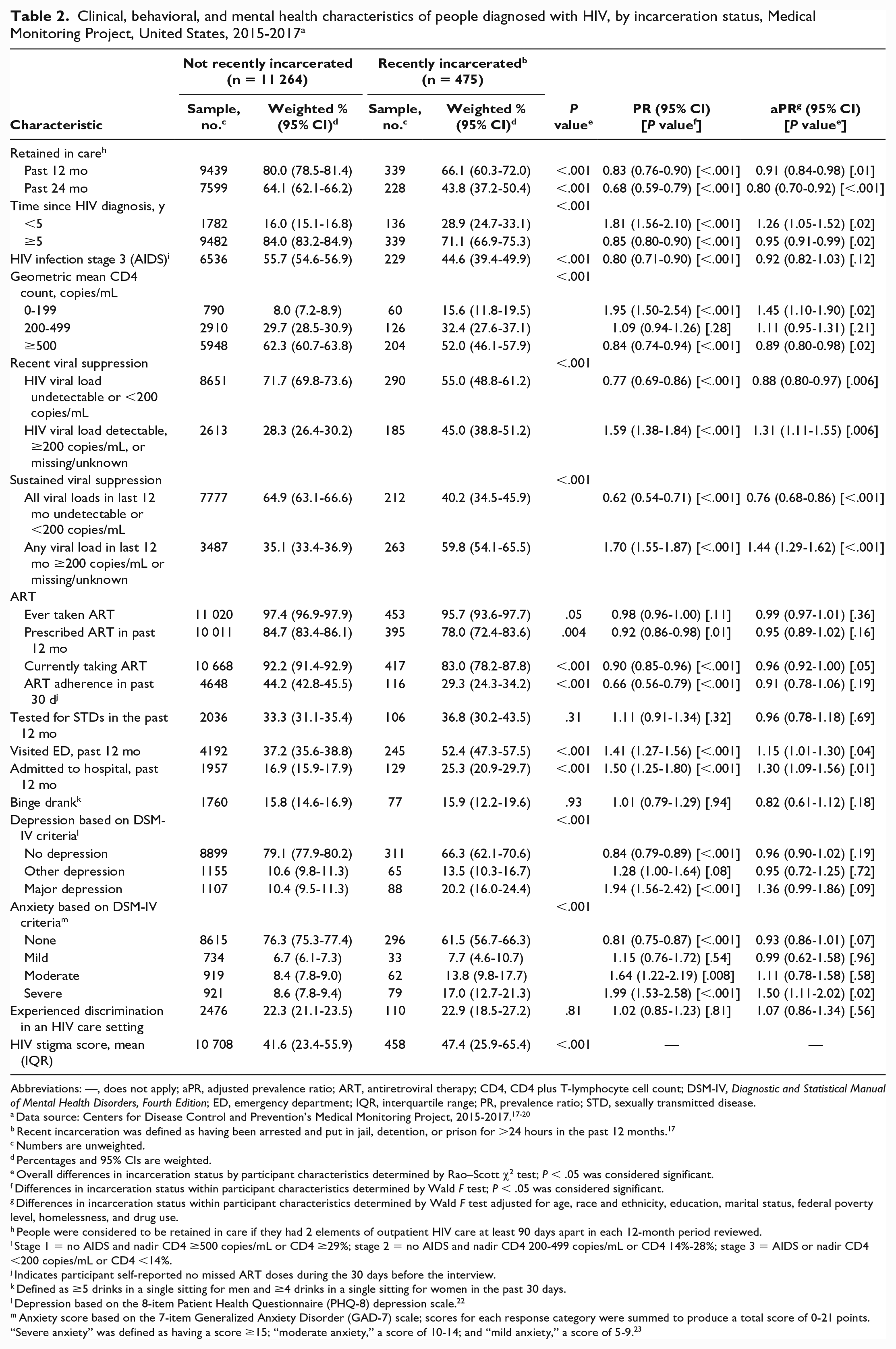
Abbreviations: —, does not apply; aPR, adjusted prevalence ratio; ART, antiretroviral therapy; CD4, CD4 plus T-lymphocyte cell count; DSM-IV, Diagnostic and Statistical Manual of Mental Health Disorders, Fourth Edition; ED, emergency department; IQR, interquartile range; PR, prevalence ratio; STD, sexually transmitted disease.
Data source: Centers for Disease Control and Prevention’s Medical Monitoring Project, 2015-2017.17-20
Recent incarceration was defined as having been arrested and put in jail, detention, or prison for >24 hours in the past 12 months. 17
Numbers are unweighted.
Percentages and 95% CIs are weighted.
Overall differences in incarceration status by participant characteristics determined by Rao–Scott χ2 test; P < .05 was considered significant.
Differences in incarceration status within participant characteristics determined by Wald F test; P < .05 was considered significant.
Differences in incarceration status within participant characteristics determined by Wald F test adjusted for age, race and ethnicity, education, marital status, federal poverty level, homelessness, and drug use.
People were considered to be retained in care if they had 2 elements of outpatient HIV care at least 90 days apart in each 12-month period reviewed.
Stage 1 = no AIDS and nadir CD4 ≥500 copies/mL or CD4 ≥29%; stage 2 = no AIDS and nadir CD4 200-499 copies/mL or CD4 14%-28%; stage 3 = AIDS or nadir CD4 <200 copies/mL or CD4 <14%.
Indicates participant self-reported no missed ART doses during the 30 days before the interview.
Defined as ≥5 drinks in a single sitting for men and ≥4 drinks in a single sitting for women in the past 30 days.
Depression based on the 8-item Patient Health Questionnaire (PHQ-8) depression scale. 22
Anxiety score based on the 7-item Generalized Anxiety Disorder (GAD-7) scale; scores for each response category were summed to produce a total score of 0-21 points. “Severe anxiety” was defined as having a score ≥15; “moderate anxiety,” a score of 10-14; and “mild anxiety,” a score of 5-9. 23
Discussion
Recently incarcerated people with diagnosed HIV were sociodemographically distinct and fared worse on several clinical, behavioral, and mental health indicators than people without a history of recent incarceration. Despite a change in MMP methods (revised sampling and weighting and inclusion of those who were not receiving HIV care), our study findings were similar to those of a previous MMP publication 27 ; in both studies, recently incarcerated people were more likely to use the ED and not be virally suppressed than those who were not recently incarcerated. Additionally, our study found that recently incarcerated people were more likely than people who were not recently incarcerated to experience severe anxiety, a factor that the previous study did not examine. Furthermore, our study examined variables that the prior publication did not, such as stigma and discrimination.
In our study, recently incarcerated people fared worse than people who were not recently incarcerated across several dimensions of HIV care. Recently incarcerated adults with HIV were less likely than not recently incarcerated people with HIV to have been retained in HIV care in the last 24 months. Other studies had similar findings, indicating low retention in HIV care among people who recently experienced incarceration.12,28,29 One study found retention in HIV care after release declined gradually during a 3-year time span, resulting in less than half (42.5%) of the original cohort retained at year 3. 30 During incarceration, a person might be more engaged in HIV care because correctional facilities may provide an opportunity to offer HIV testing, linkage to care, and access to ART; they might not have the same opportunities in their community. 12 However, once released from custody, many people prioritize basic life necessities when first transitioning and fall out of care, which leads to loss of viral suppression. 11 Another study found that receiving ART while incarcerated and being linked to care promptly after release were highly correlated with better treatment outcomes. 30
Furthermore, we found that recently incarcerated people were more likely to have lower CD4 counts (<200 copies/mL) and were less likely to have recent and sustained viral suppression than people who had not experienced recent incarceration. Adherence to treatment is vital to achieving viral suppression. Studies found that people who experienced incarceration were less adherent to ART, 31 and nearly 40% of recently incarcerated people were not adherent to ART 6 months after release. 29 We found that recently incarcerated people were less likely to adhere to ART in the past 30 days, though not after adjusting for other factors that can negatively affect adherence, such as homelessness and drug use. After release, recently incarcerated people often face challenges filling their prescriptions, enrolling in HIV care, or enrolling in public health insurance programs (eg, Medicare, Medicaid), all of which can lead to disruptions in HIV treatment and, overall, a loss of viral suppression. Prison and jail discharge planners can help people find postrelease linkage-to-care interventions that immediately connect them to health care providers and clinics, which is crucial to improving health outcomes for those diagnosed with HIV. Health care providers at HIV care and sexually transmitted infection clinics might benefit from training in recognizing previous incarceration as a possible barrier to retention in care and discuss solutions at the client’s initial visit. Clinics also should consider enhanced monitoring of missed visits, appointment adherence, visit frequency, and gaps in care for people with diagnosed HIV who have been recently incarcerated and consider referrals to wraparound services, such as community support groups, transportation support, mental health providers, substance use programs, and case management services, as appropriate.
According to a 2017 study by Bronson and Berzofsky, at the time of incarceration, 37% of people incarcerated in prisons and 44% of people incarcerated in jails had a history of mental health disorders; 1 in 7 (14%) state and federal prisoners and more than one-quarter (26%) of people incarcerated in jails have serious mental illness. 32 Our study found that people who had been recently incarcerated were more likely to experience severe anxiety than people who had not been recently incarcerated. In a recent MMP study, Beer et al 33 found that people with generalized anxiety disorder experienced significantly lower ART prescription and adherence, medical care engagement, and sustained viral suppression than people who did not have generalized anxiety disorder. Although anxiety symptoms are related to HIV medication nonadherence, 34 the limited number of studies focusing on the association between anxiety and HIV in the last decade indicates a need for additional exploration to understand this association, including the effects of stigma on HIV care. We found that HIV stigma scores were also significantly higher among recently incarcerated people than among people who had not been recently incarcerated. Kemnitz et al 35 found that stigma related to HIV can exacerbate mental health issues and hinder continuous engagement in HIV care; others found that it was negatively associated with ART adherence. 36 In addition to efforts from health care professionals in clinical settings, community-based organizations could help people who were recently incarcerated transition to their communities by connecting them to mental health, housing, and other support services, and they could facilitate programs that address stigma that people may experience based on their HIV status, substance use, recent incarceration, discrimination, and the potential intersection of these factors.
Lastly, our analysis indicated that ED visits and hospital admissions were more common among recently incarcerated people with HIV than among people with HIV who had not been recently incarcerated. These findings echo results of previously published studies27,37 and 1 study that found that recently incarcerated people frequently use EDs as a source of health care. 38 As compared with people with HIV who have not been recently incarcerated, people with HIV who have been recently incarcerated are at greater risk for unstable living conditions, which can be influenced by previous or current drug use, mental illness, and homelessness, leading them to use the ED more often than the general population. Studies have also found that many people who have experienced recent incarceration did not have health insurance or had a lapse in health insurance coverage at the time of release,39,40 which can affect access to needed medications, including ART. History of incarceration should be considered for inclusion on ED intake forms; if the ED is able to identify recently incarcerated people, then it can reduce their use of ED services by properly referring them to HIV care providers and other support services.
Limitations
This study had several limitations. First, MMP is an observational cross-sectional study; therefore, causality could not be established. Second, the findings cannot be attributed to incarceration in any specific type of correctional facility (jail or prison) because information on correctional facility type was not ascertained. Third, records were abstracted from the facility that participants identified as their usual source of HIV care, which can include jails or prisons, during the 12 months prior to their interview, and results may not reflect all HIV care received during the prior 12 months for people who received care from multiple facilities. We examined results for those who reported having >1 usual source of care (7% of the study population), and these analyses demonstrated similar findings to the main analyses. Fifth, although we collected information on duration of incarceration, frequency of incarceration, and time since release, the findings may be more reflective of experiences of jail rather than prison. We did not look at these variables as explanatory factors in any of the analyses because that was not the intent of this study. Sixth, a small percentage (3%) of participants completed surveys but did not have a medical record abstraction. Participants without a medical record abstraction are considered not retained in care or virally suppressed; however, some participants in this category might have received care and been misclassified, leading to potential underestimation of retention in care and viral suppression. Lastly, the data derived from the survey were self-reported and may be subject to response and/or recall bias.
Conclusions
Recently incarcerated people represent a part of the HIV community with poor health outcomes, and their release has implications for people in the communities to which they return; understanding how to improve services for them is crucial for everyone. Ensuring that recently incarcerated people are linked to and retained in care so that they stay virally suppressed is vital for increasing their quality of life and helping reduce community transmission. Implementing and evaluating strategies such as health care during incarceration, structured discharge planning, proper referrals to support services in the community, and overall inclusive wraparound services can improve the HIV health outcomes of this socioeconomically and medically marginalized population. Additionally, HIV care providers and community-based organizations should find ways to address the social determinants of health (eg, unemployment, poverty, exposure to crime and violence, availability of resources to meet daily needs), 41 because these factors influence people who have experienced recent incarceration. Examining the social determinants of health may inform interventions and wraparound services, which could improve HIV health among those who are reentering their communities.
This analysis and others suggest an important role for evidence-based reentry programs for people with HIV. 42 Federal programs have exemplified this notion. The Office of Minority Health initiated the HIV/AIDS Health Improvement for the Re-entry Population grant program, which aimed to improve health outcomes for recently incarcerated people with HIV, and the Re-entry Community Linkages program, which focused on improving health outcomes for people who are transitioning from jail to their communities.43-45 Incorporating detailed data elements of incarceration into population health surveys and health surveillance data would allow for deeper analyses. Future research examining HIV health outcomes among recently incarcerated people with HIV based on their care status could improve our understanding of factors associated with retention in care and inform long-term care efforts. Additional research is needed to identify and address barriers to retention in care, including the social determinants of health, in this population.
Footnotes
Acknowledgements
The authors thank Medical Monitoring Project participants, project area staff, and Provider and Community Advisory Board members. They also acknowledge the contributions of the Clinical Outcomes Team and Behavioral and Clinical Surveillance Branch at the Centers for Disease Control and Prevention.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.