
Abstract
In the United States, the public health response to control COVID-19 required rapid expansion of the contact tracing workforce from approximately 2200 personnel prepandemic to more than 100 000 during the pandemic. We describe the development and implementation of a free nationwide training course for COVID-19 contact tracers that launched April 28, 2020, and summarize participant characteristics and evaluation findings through December 31, 2020. Uptake of the online asynchronous training was substantial: 90 643 registrants completed the course during the first 8 months. In an analysis of a subset of course participants (n = 13 697), 7724 (56.4%) reported having no prepandemic public health experience and 7178 (52.4%) reported currently serving as case investigators, contact tracers, or both. Most participants who completed a course evaluation reported satisfaction with course utility (94.8%; 59 497 of 62 753) and improved understanding of contact tracing practice (93.0%; 66 107 of 71 048). These findings suggest that the course successfully reached the intended audience of new public health practitioners. Lessons learned from this implementation indicate that an introductory course level is appropriate for a national knowledge-based training that aims to complement jurisdiction-specific training. In addition, offering a range of implementation options can promote course uptake among public health agency staff. This course supported the emerging needs of the public health practice community by training a workforce to fill an important gap during the COVID-19 pandemic and could serve as a feasible model for enhancing workforce knowledge for future and ongoing public health threats.
Contact tracing, a fundamental component of communicable disease prevention,1,2 is a key strategy for containment and suppression of SARS-CoV-2, the virus that causes COVID-19.3-6 Before the COVID-19 pandemic, contact tracing—primarily for tuberculosis, HIV, and other sexually transmitted infections—was routinely carried out in state, tribal, local, and territorial health agencies by disease intervention specialists. This workforce is charged with notifying individuals of their test results; eliciting names of their exposed contacts; locating, notifying, and interviewing those contacts; and connecting people to care and social supports. Disease intervention specialists are skilled in communication, interviewing, and community engagement. Before the COVID-19 epidemic, an estimated 2200 disease intervention specialists were employed in public health agencies in the United States. 7
With the onset of the COVID-19 epidemic, public health agencies redirected existing disease intervention specialists from their routine work to support COVID-19 contact tracing efforts.8,9 Public health leaders also called for substantial workforce expansion by adding 100 000 new contact tracers to meet response needs. 10 To support this call, the Association of State and Territorial Health Officials (ASTHO) and the National Coalition of STD Directors, with funding from the Centers for Disease Control and Prevention (CDC), developed and launched an online course intended for COVID-19 contact tracers with limited previous public health experience.
Purpose
ASTHO and the National Coalition of STD Directors developed the course, Making Contact: A Training for COVID-19 Contact Tracers (hereinafter, Making Contact), 11 to assist public health agencies in their efforts to rapidly integrate and mobilize an expanded workforce into the COVID-19 response. Our goal was to provide an entry-level, knowledge-based course that was freely available nationally and that state, tribal, local, and territorial public health agencies could use as a foundation to complement their jurisdiction-specific orientation and training. We describe the rapid development and implementation of Making Contact and share lessons learned during this work to support the pandemic response workforce. While examples of locally based contact tracing training programs are described in the literature,12-15 to our knowledge, this case study is the first US study summarizing the development and implementation of a nationwide knowledge-based COVID-19 contact tracer training program.
Methods
Course Development
During 14 days in April 2020, we designed and launched Making Contact, an introductory knowledge-based training course for COVID-19 contact tracers. The course drew on established work functions of disease intervention specialists, in addition to emerging public health protocols specific to COVID-19. In developing the course, we reviewed the Public Health Accreditation Board’s job task analysis for disease intervention specialists 16 and existing CDC trainings17,18 to identify core learning objectives and relevant content. We also incorporated emerging COVID-19 contact tracing resources and protocols from CDC and state and local public health agencies. Course content underwent rapid review from national partners with expertise in the material, including CDC, the Council of State and Territorial Epidemiologists, and the National Association of County and City Health Officials.
The resulting online asynchronous training course consisted of 4 lessons that included foundational information on COVID-19, contact tracing procedures, effective communication and interviews, cultural sensitivity, and case monitoring and support services. We offered the training in English, at approximately an eighth-grade literacy level. The course had an estimated duration of 3 hours, with progress measured as participants completed end-of-lesson quizzes and functionality that allowed participants to stop and resume the course at their convenience. The course used a range of interactive components, including digital flashcards, case-based scenarios, and knowledge checks to deliver and provide opportunities to review core principles. Videos and job aids were also included to reinforce lesson content. The course and its interactive components supported compatibility with a variety of devices and screen sizes and were positioned to meet the Americans With Disabilities Act standards of accessible or accommodating design.
We developed Making Contact as an introductory course, with the intent that it be supplemented by additional skills-based training and mentorship at the jurisdiction level. Because the training was intended to support training of personnel who might not have had previous experience in public health, course length and level of complexity were key considerations in the program design.
Implementation
Making Contact launched on April 28, 2020, and was offered at no cost through the online ASTHO learning management system and subsequently via the CDC Training Finder Real-time Affiliate Integrated Network (TRAIN) and University of California San Francisco learning management systems. ASTHO and the National Coalition of STD Directors promoted Making Contact through calls with their members and featured the course on their websites, newsletters, social media, and joint press releases. CDC also included the course on its COVID-19 contact tracing training resources webpage, 19 further amplifying reach to potential course participants. We regularly updated the course to ensure content was accurate for the evolving COVID-19 pandemic. We also supported a range of options for the course to serve as a prerequisite for instructor-led skills-based training or to be customized for jurisdiction-specific training. For example, California positioned Making Contact as a prerequisite for its virtual skills-based training academy, and North Carolina included Making Contact as a module in its contact tracing training orientation.14,20,21
Data Collection
We captured course registration and completion numbers across all 3 learning management systems. For detailed analyses, we used data collected via the ASTHO learning management system, as this system captured in-depth data. Two measures of participant characteristics were consistently available via ASTHO’s online registration form between April 28 and December 31, 2020: contact tracing experience and education level. In September 2020, the registration form expanded data collection on participant characteristics (ie, age, race and ethnicity, education level, and public health background).
We collected postcourse evaluation data via ASTHO’s learning management system. The electronic evaluation survey included open-text questions and a series of 4-point Likert scales measuring perceptions of course utility (1 = not useful, 2 = somewhat useful, 3 = useful, 4 = extremely useful) and level of agreement with statements related to perceived understanding and participant experience (1= strongly disagree, 2 = somewhat disagree, 3 = somewhat agree, 4 = strongly agree).
We cleaned the data and performed quantitative analyses (ie, counts, percentages) in SPSS version 27 (IBM Corp). We used MapChart (MapChart.net) to map the distribution of US-based course completers.
Outcomes
From April 28 through December 31, 2020, a total of 125 850 people registered for Making Contact. Of those, 90 643 (72.0%) completed the course. Uptake of the course was rapid, with 97 924 (77.8%) participants registering during the first 4 months of the study period. A total of 88 468 course completers were based in the United States (Figure). An additional 766 participants completed the course from US territories or freely associated states.
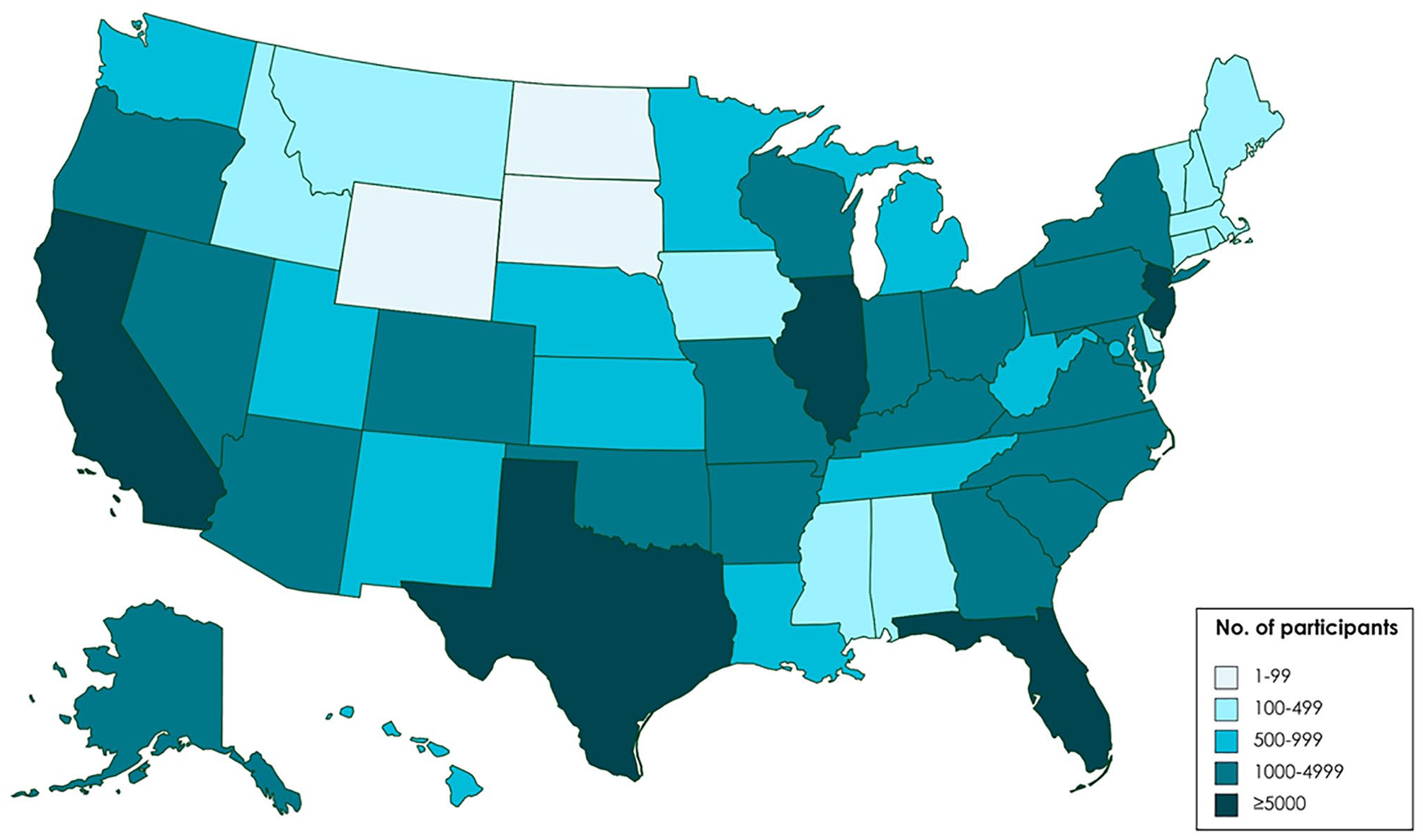
Distribution of participants (n = 88 468) who completed the online knowledge-based course, Making Contact: A Training for COVID-19 Contact Tracers, 11 United States, April 28–December 31, 2020.
Of the 125 850 registrants, 96 200 (76.4%) accessed the course via the ASTHO learning management system; these registrants represented 78.5% (71 124 of 90 643) of all course completions.
Participant Characteristics
From April 28 through December 31, 2020, 67.0% (64 502 of 96 200) of registrants via the ASTHO learning management system reported no prior contact tracing experience, and 28.6% (27 501 of 96 200) indicated no college degree. Implementation of an expanded registration form in September 2020 provided further detail on the later subset of 13 697 participants (Table). In this subset, 35.5% (n = 4863) worked in a local, state, or territorial health department, and 52.4% (n = 7178) reported currently serving as case investigators, contact tracers, or a combination of both. In addition, 27.7% (n = 3790) spoke a language other than English fluently enough to use in a contact tracing practice setting.
Characteristics of a subset of participants (n = 13 697) in a nationwide online knowledge-based training for COVID-19 contact tracers, a September 16–December 31, 2020
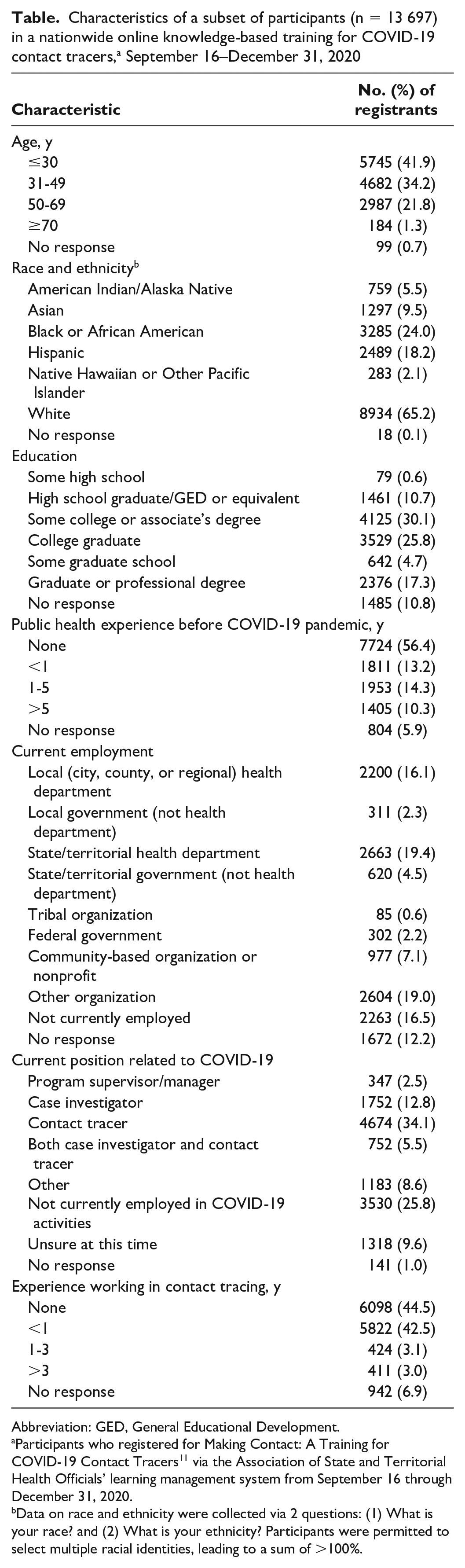
Abbreviation: GED, General Educational Development.
Participants who registered for Making Contact: A Training for COVID-19 Contact Tracers 11 via the Association of State and Territorial Health Officials’ learning management system from September 16 through December 31, 2020.
Data on race and ethnicity were collected via 2 questions: (1) What is your race? and (2) What is your ethnicity? Participants were permitted to select multiple racial identities, leading to a sum of >100%.
Course Evaluation
A total of 71 124 participants on ASTHO’s learning management system completed an electronic evaluation survey following completion of the final lesson. Most respondents (94.8%; 59 497 of 62 753) indicated that the training was “useful” or “extremely useful,” and 93.0% (66 107 of 71 048) “somewhat agreed” or “strongly agreed” that they better understood what it meant to be a contact tracer as a result of the training. Additional evaluation measures also received high scores: most respondents agreed that the training was easy to understand (91.9%; 61 181 of 70 906), had the appropriate level of detail (92.0%; 65 217 of 70 854), was an appropriate length (89.5%; 63 171 of 70 555), and was offered on a platform that was easy to navigate (87.2%; 58 088 of 66 578).
Lessons Learned
Findings suggest that a widely accessible online asynchronous training course was a successful strategy for rapid workforce development during a public health emergency. In the 8 months after course launch, Making Contact generated substantial interest and uptake, with more than 125 000 registrations and 7 of 10 registrants going on to complete the course. Eight states with the highest number of course completions were among the 10 states with the highest total COVID-19 case counts as of April 2021, 22 suggesting alignment with jurisdictions having a greater need for trained contact tracers. Furthermore, the racial, ethnic, and linguistic diversity of people accessing Making Contact suggests they might have been able to engage effectively with some of the communities most impacted by COVID-19.23-27 In the subset of participants with detailed data available, racial minority populations were overrepresented relative to national estimates—particularly for people who self-identified as Black/African American or Asian, who comprise 24.0% and 9.5% of registrants, compared with 13.4% and 5.9% of the US population, respectively. 28
The national scope, knowledge-based focus, and design considerations concerning course complexity and length distinguish Making Contact from other trainings developed for COVID-19 contact tracers. Our course was developed to complement jurisdiction-specific trainings and serve as a foundation for local or national skills-based trainings. Furthermore, our aim to support rapid training of personnel who might not have had previous experience in public health influenced design decisions related to course content level and length, an approach that differentiates Making Contact from longer, more complex trainings.
Implementation Considerations
Implementation lessons from this case study may inform considerations for other public health professionals establishing training programs, especially in the context of workforce expansion during public health emergencies. First, our analysis suggests that a short, introductory asynchronous course is appropriate for a national knowledge-based training for new public health response workers. In the subset of Making Contact participants with more detailed data available, more than half reported no prepandemic public health experience, reinforcing the importance of offering foundational training. High levels of participant satisfaction on measures related to ease of understanding, level of detail, and course length also suggest that course complexity and duration were appropriately calibrated. In addition, the asynchronous delivery modality provided flexibility for learners incorporating the course into their schedules. 14
Second, offering a range of implementation options and sharing the training with key public health leaders can promote course utilization among the practice community. We supported robust uptake of the course among public health agency staff by providing a range of options for state and local training providers to adapt and integrate the course into their jurisdiction-specific curricula and supplement with more in-depth trainings, such as those released by Johns Hopkins University. 29 We also leveraged ASTHO and the National Coalition of STD Directors’ ability to engage with public health officials in key roles leading and operationalizing expansion of the contact tracer workforce to promote the training. More than one-third of Making Contact participants worked in a local, state, or territorial health department, and more than half reported currently serving as case investigators and/or contact tracers, demonstrating that the course reached people positioned to immediately apply knowledge from the course to their COVID-19 work. Some health departments also listed the training as a preferred qualification for contact tracers in their staffing documents, further promoting the course among key groups.30,31 These observations suggest that a freely available, online, knowledge-based course can complement jurisdiction-specific workforce training and mentorship during a public health emergency.
Third, our experience implementing Making Contact underscores the importance of developing flexible approaches to maintain and manage the course over time, to accommodate the dynamic nature of an emergency response. Rapidly emerging science and evolving public health guidance posed an early challenge in maintaining the accuracy and relevance of course content. To address this challenge, we implemented a process for regular review of course content to ensure Making Contact was aligned with current CDC information. The unanticipated volume and variety of support and information needs from course participants and partners presented another challenge. We responded by adapting our implementation strategy over time. For example, to address the high volume of user support requests from course participants, we created a frequently asked questions resource, expanded the number of staff available to respond to user requests, and developed a process to triage questions about the course. When state and local training providers requested additional flexibility in the approaches available to integrate Making Contact into jurisdiction-specific trainings, we developed a menu of options to support incorporation and adaptation of the course for local implementation.
Limitations and Next Steps
Making Contact was developed and implemented to address evolving COVID-19 response needs; as such, this case study had several limitations. Because more detailed participant data were available only for people accessing the training via the ASTHO learning management system toward the end of 2020, the participant characteristics we describe may not be representative of the total population of course registrants. In addition, we did not collect data on whether participants took the training voluntarily or as part of an employer-mandated training, which are factors that could affect course uptake and completion. A true measurement of knowledge change was not possible, because participants were given an unlimited number of attempts to reach a required passing score. We therefore relied on a self-reported measure of understanding as a proxy. Finally, we did not collect information on long-term learner outcomes, which would help ascertain how participants working as contact tracers are applying information from the training on the job.
Making Contact met initial demands of the COVID-19 public health workforce, and ongoing course updates and evaluation efforts are planned to keep the course current and further assess the competencies of participants. In 2021, we launched an expanded version of the course, which includes more detailed instruction on discrete case investigation and contact tracing processes, underlying epidemiologic concepts, and communication techniques to build rapport. We incorporated additional interactive and video features and implemented a revised post-assessment approach to facilitate measurement of changes in knowledge. Future evaluation efforts will explore long-term participant outcomes (ie, employment setting after course completion and application of knowledge gained from the course in practice settings), in addition to how public health agencies are using and adapting the course to meet their needs.
This course supported emerging public health practice needs by training an eligible contact tracing workforce during the COVID-19 pandemic. A rapidly developed widescale training offered via online asynchronous instruction is a feasible model for enhancing workforce development efforts during future public health threats.
Footnotes
Acknowledgements
The authors thank colleagues from the Centers for Disease Control and Prevention (CDC) for their review of and contributions to the training program content and evaluation strategy: Marion Carter; Blanche Collins; Frances Rucker-Bannister; Melinda Salmon; and staff on the COVID-19 Contact Tracing and Innovations Section. The following partners provided input, expert review, and/or source material for training development: Cardea Services; Council of State and Territorial Epidemiologists; Michigan Department of Health and Human Services; National Association of County and City Health Officials; National Coalition of STD Directors’ Disease Intervention Specialist Committee; Public Health Foundation; Resolve to Save Lives; Texas Department of State Health Services; Virginia Department of Health; and Washington State Department of Health. The authors are also grateful for the partnership of the Training Finder Real-time Affiliate Integrated Network (TRAIN), powered by the Public Health Foundation, and the University of California San Francisco for assisting with data collection on course uptake.
Disclaimer
The findings and conclusions of this article are those of the authors and do not necessarily represent the official position of CDC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by CDC grant number 6 NU38OT000290-02-08.