
Abstract
Objectives:
Appropriate face covering use at public venues can help mitigate the transmission of SARS-CoV-2 in the absence of widespread vaccination and provide protection when viral variants become more infectious. The objective of this study was to evaluate compliance with a statewide face mask mandate by examining trends in face covering use in publicly accessible spaces in King County, Washington.
Methods:
From November 27, 2020, through May 11, 2021, we conducted a repeated cross-sectional observational study of face covering use across publicly accessible venues (eg, grocery and convenience stores, airport, transit center, post office). Trained observers recorded perceived sex, estimated age group, and face covering use. We calculated estimates of overall face covering use and prevalence ratios (PRs) with 95% CIs.
Results:
We observed 9865 people in 53 unique venues during 229 observation intervals during 6 observation periods. Correct face covering use was 87.2% overall and lowest at semi-outdoor venues such as transit hubs (78.1%) and the pick-up curb of Seattle–Tacoma International Airport (69.0%). Correct face covering use was lowest among men (PR = 1.42; 95% CI, 1.27-1.58) and among people aged 2-11 years (PR = 2.74; 95% CI, 2.37-3.17) and 12-17 years (PR = 1.36; 95% CI, 1.07-1.72). Compliance declined among adults aged ≥60 years and among younger age groups before vaccine eligibility.
Conclusions:
Overall compliance with the statewide face mask mandate in King County was high. Layered mitigation strategies, including but not limited to the use of face coverings, and methods to assess adherence to them are crucial to preventing SARS-CoV-2 transmission.
The Centers for Disease Control and Prevention (CDC) recommends combining evidence-based interventions to reduce transmission of SARS-CoV-2, the virus that causes COVID-19. 1 Universal use of face masks or respirators is a relatively low-cost, effective intervention because the primary transmission mechanism of SARS-CoV-2 is inhalation of virus-laden respiratory aerosols and contact with droplets from infected people.2,3 In addition, this intervention is a key method of source control because half of transmission has been estimated to be attributable to exposure to asymptomatic people who may not be aware that they are infected. 4
County and state face mask mandates are associated with reductions in COVID-19 cases and related deaths.5-8 Following the proclamation of a statewide State of Emergency because of increasing spread of COVID-19 on February 29, 2020, 9 Washington State implemented a statewide mandate on June 26, 2020. The mandate required face coverings in all public settings, such as publicly accessible businesses and transportation hubs, for all people aged ≥5 years. It also defined correct face covering use as using a cloth face covering or other face mask (eg, surgical mask, N95 respirator) over both the nose and mouth. 10 Businesses failing to enforce the face mask mandate with customers and employees as determined by state investigators could be fined up to $7500. 11 While measuring and tracking adherence to face covering policies to inform efforts to improve face covering–wearing behavior can have a beneficial impact on adverse outcomes of COVID-19, they are not well-studied. To evaluate compliance with the statewide mandate and to identify groups and locations with low levels of face covering use that might benefit from targeted efforts to increase use, investigators from the University of Washington (UW) departments of Environmental and Occupational Health Sciences, Global Health, and Epidemiology, in collaboration with staff from the Washington State Department of Health and Public Health–Seattle & King County (PHSKC), conducted a repeated cross-sectional observational study of face covering use in King County.
Methods
PHSKC selected 7 King County health reporting areas 12 for inclusion in the study as a purposive sample to represent areas with a range of COVID-19 incidence, sociodemographic characteristics, and population density (urban/rural). We selected 6 or 7 types of publicly accessible venues per health reporting area for observation, chosen as representative environments under the statewide mandate where assessment of compliance could inform public health efforts. Venue types included grocery stores, small retail stores (eg, hardware and sporting goods stores), transit hubs, indoor and outdoor malls, convenience stores, post offices, and laundromats. The ticketing, baggage claim, and pick-up areas of the Seattle–Tacoma (SeaTac) International Airport were also included. We did not include venues where the statewide mandate did not apply to the public, such as establishments that prepare and serve meals and beverages. PHSKC and community entities (representing equity and social justice teams, environmental health staff, and public transit and airport operations) provided guidance on the selection of sites and observation protocols and provided additional context for the study findings.
Nine observers, consisting of graduate and undergraduate students from UW, underwent standardized training by study staff to ensure consistency of observations and field safety, including conducting practice observations with study staff. Observers visited venues each month and observed either single people at the point at which they entered a venue (for venues with a defined entrance) or a subsample of people (eg, every third or fourth person, if volume was high) passing through a fixed point or field of view in 1 direction (for venues without a defined entrance) to reduce the likelihood of repeat observations. At each venue, observations were made for 30 minutes from locations where the venue entrance was visible as much as possible and as safely as possible (eg, nearby parking stall or bench) or in common areas outside of stores at indoor malls. For each observed person, observers recorded perceived sex (female, male, or unknown); estimated age group (2-11, 12-17, 18-30, 31-59, ≥60 years); and use of face covering (correct, incorrect, or none).
We based age groupings on typically identifiable physical and life-stage characteristics that would facilitate categorization and minimize misclassification of people. We defined correct use of face coverings as a cloth face covering, surgical mask, or N95 respirator (or device offering a similar level of protection) completely covering both the nose and mouth, with ear or head loops on, consistent with the Washington State Department of Health face mask mandate. 10 We also considered gaiters, bandanas, and headscarves or niqabs that covered the mouth and nose to be a correct use of face coverings; we considered just a face shield but no mask as no face covering use. Observations were initially collected on paper forms and subsequently collected electronically on Android tablets via the ODK Collect app (Get ODK Inc.). The project manager followed up with observers after every observation assignment to address questions that may have affected the quality of the observation. We validated paper form data by entering the data electronically into a spreadsheet with built-in logic checks.
To evaluate noncausal broad associations with nonuse or incorrect use of face coverings, we calculated prevalence ratios (PRs) with 95% CIs using an unadjusted Poisson regression model. We used segmented Poisson time-series regression that accounted for clustering by venue to determine significance of change in face covering use over time, with P < .05 considered significant. We conducted all analyses in Stata version 14.2 (StataCorp LLC). The UW Institutional Review Board considered this study not human subjects research because of the lack of interaction with or collection of identifiable information about human subjects and because it was conducted as part of public health surveillance.
Results
From November 27, 2020, through May 11, 2021, researchers observed 9865 people during 229 distinct observation intervals conducted across 53 unique venues. The overall rate of correct face covering use was 87.2% (Table 1). Use of face coverings was high at small retail stores (94.6%) and grocery stores (94.2%); correct use of face coverings at grocery stores was >85% throughout the observation periods (Figure, Panel A). Use of face coverings at transit hubs was relatively low overall (78.1%) and dropped to 66.9% in late November 2020.
Use of face coverings during the COVID-19 pandemic, by venue type, King County, Washington, November 27, 2020–May 11, 2021 a
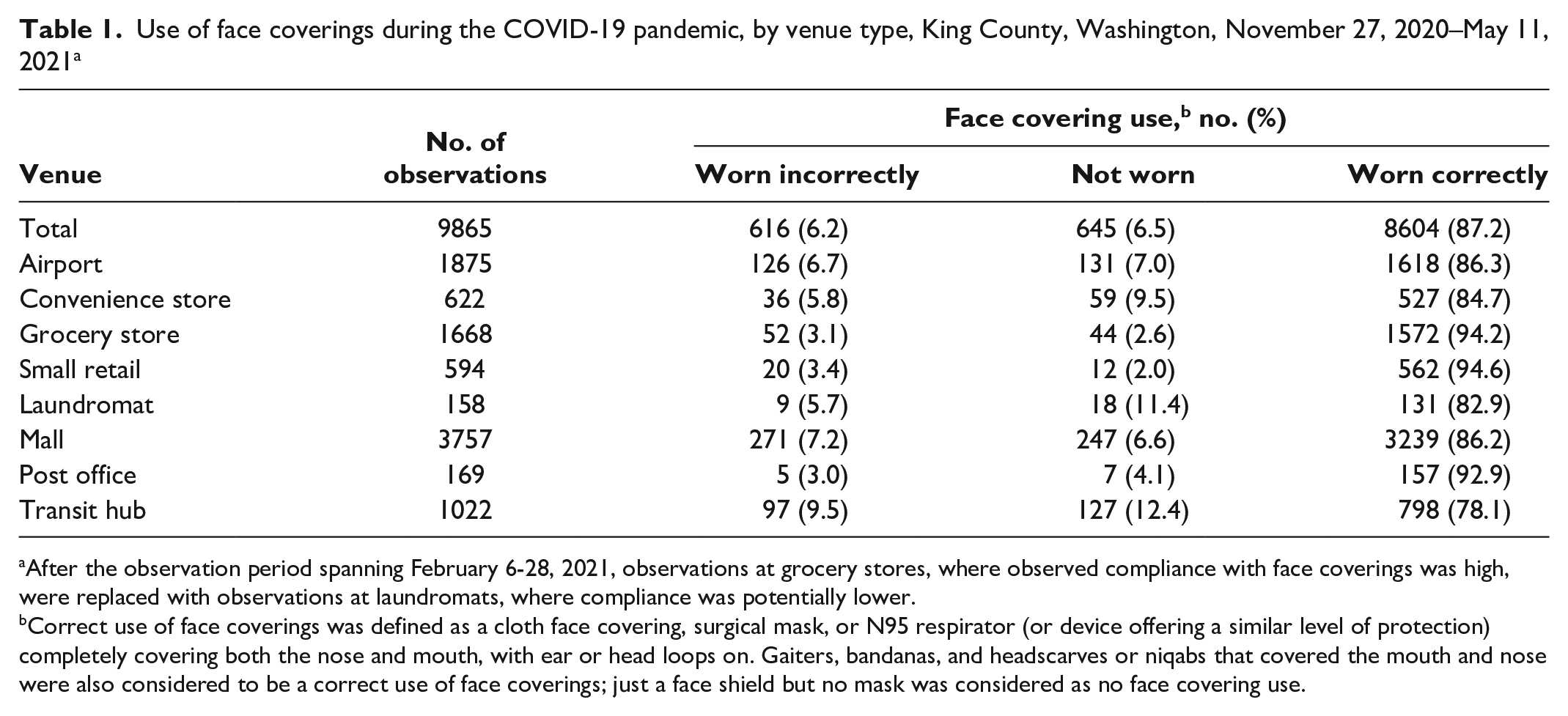
After the observation period spanning February 6-28, 2021, observations at grocery stores, where observed compliance with face coverings was high, were replaced with observations at laundromats, where compliance was potentially lower.
Correct use of face coverings was defined as a cloth face covering, surgical mask, or N95 respirator (or device offering a similar level of protection) completely covering both the nose and mouth, with ear or head loops on. Gaiters, bandanas, and headscarves or niqabs that covered the mouth and nose were also considered to be a correct use of face coverings; just a face shield but no mask was considered as no face covering use.
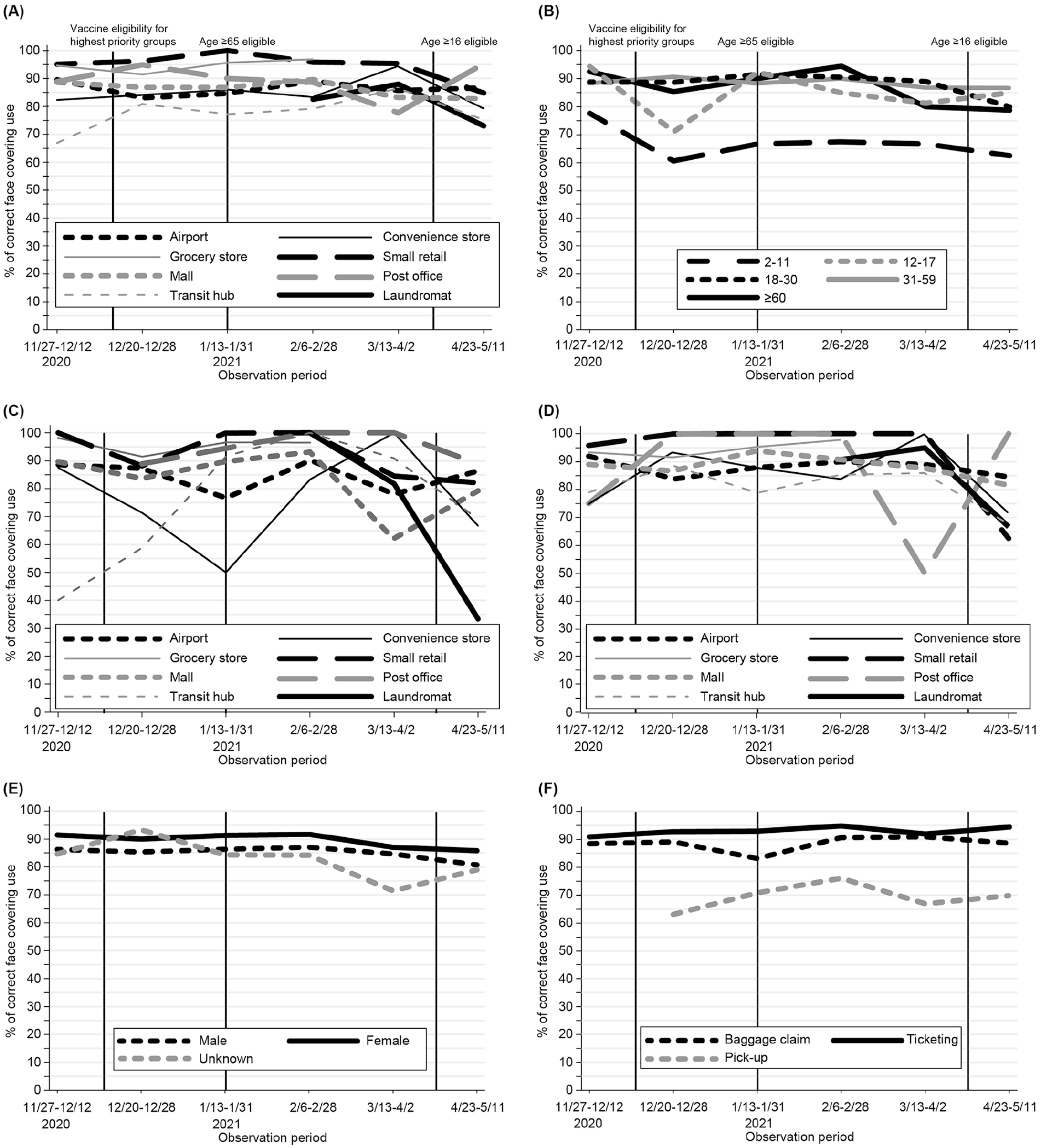
Trends in proportion of correct face covering use, King County, Washington, November 27, 2020–May 11, 2021. A, By venue type. B, By age. C, By venue type among adults aged ≥60 years. D, By venue type among adults aged 18-30 years. E, By gender. F, By airport venue. Correct use of face coverings was defined as a cloth face covering, surgical mask, or N95 respirator (or device offering a similar level of protection) completely covering both the nose and mouth, with ear or head loops on. Gaiters, bandanas, and headscarves or niqabs that covered the mouth and nose were also considered to be a correct use of face coverings; just a face shield but no mask was considered as no face covering use.
Nonuse or incorrect use of face coverings was associated with being aged 2-11 years (PR = 2.74; 95% CI, 2.37-3.17) and 12-17 years (PR = 1.36; 95% CI, 1.07-1.72) versus 31-59 years (Table 2). Face covering use was relatively low among people aged 2-11 years, with <70% correct use throughout most observation periods (Figure, Panel B). Correct face covering use declined during the observation period among adults aged ≥60 years (from 94.5% in February to 78.7% in late April to mid-May), among people aged 12-17 years (from 92.3% in late January to 81.3% in mid-May), and among people aged 18-30 years (from 88.7% in late January to 80.0% by mid-March) (Figure, Panel B). Significant declines in correct face covering were observed only during selected periods. Intervals of significant decline in correct face covering use occurred among people aged ≥60 years from mid-February to late March (P < .001), among people aged 12-17 years from late January to late March (P = .019), and among people aged 18-30 years from late March to mid-May (P = .002). Declines in correct face covering use among people aged ≥60 years and 18-30 years were observed qualitatively in most venues (Figure, Panels C and D).
Characteristics associated with nonuse or incorrect use of face coverings a during the COVID-19 pandemic, overall and at Seattle–Tacoma (SeaTac) International Airport, King County, Washington, November 27, 2020–May 11, 2021
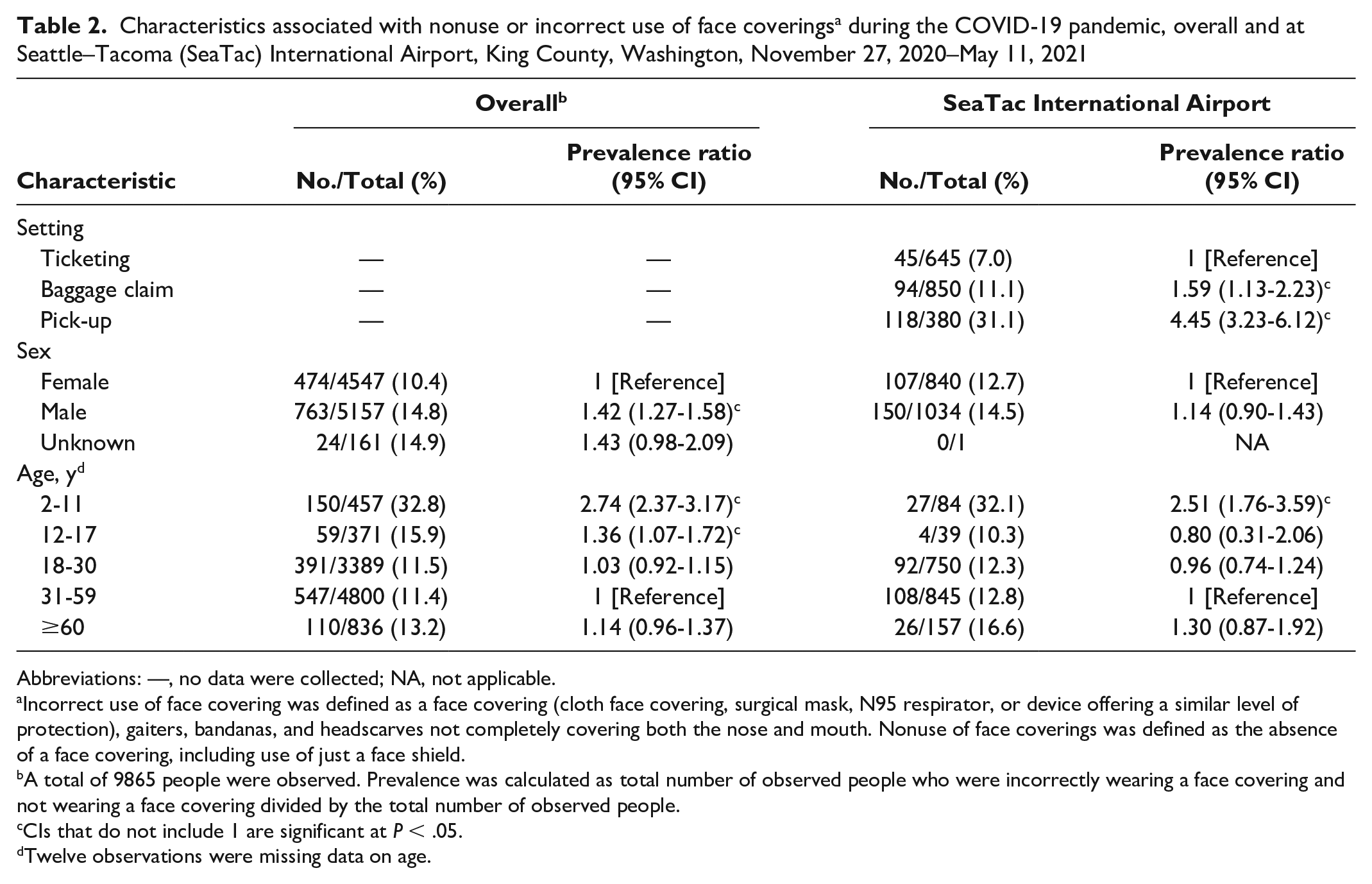
Abbreviations: —, no data were collected; NA, not applicable.
Incorrect use of face covering was defined as a face covering (cloth face covering, surgical mask, N95 respirator, or device offering a similar level of protection), gaiters, bandanas, and headscarves not completely covering both the nose and mouth. Nonuse of face coverings was defined as the absence of a face covering, including use of just a face shield.
A total of 9865 people were observed. Prevalence was calculated as total number of observed people who were incorrectly wearing a face covering and not wearing a face covering divided by the total number of observed people.
CIs that do not include 1 are significant at P < .05.
Twelve observations were missing data on age.
Nonuse or incorrect use of face coverings was associated with being male versus female (PR = 1.42; 95% CI, 1.27-1.58) (Table 2). An apparent difference in the use of face coverings was observed between males and females throughout the observation periods (Figure, Panel E).
At SeaTac International Airport, most correct face covering use was observed at indoor areas (ticketing and baggage claim, 93.0% and 88.9%, respectively), while outdoor areas (pick-up) had 63.2% to 76.1% compliance throughout the study period (Figure, Panel F). Compared with the ticketing area, the baggage claim area (PR = 1.59; 95% CI, 1.13-2.23) and pick-up area (PR = 4.45; 95% CI, 3.23-6.12) had a higher prevalence of nonuse or incorrect use of face coverings (Table 2). Unlike observations conducted at other publicly accessible spaces, we found no significant differences between males and females at the airport (PR = 1.14; 95% CI, 0.90-1.43).
Lessons Learned
The findings from this study suggest that overall compliance with the statewide face mask mandate at public venues in King County from November 27, 2020, through May 11, 2021, was high and stable during the study period, with some evidence of declines later in the study period, particularly among adults aged ≥60 years. These findings are consistent with a similar study that conducted observations in commercial venues in Wisconsin after a statewide face mask mandate was enacted. 13 Self-reported data aggregated from online surveys conducted around the same time also found similar levels of face covering use. 14
Compliance was lowest in venues that were outdoors or incompletely enclosed, such as transit hubs and the pick-up area at SeaTac International Airport. Similarly, a Gallup Poll conducted from July through August 2020 in the western region of the United States found that only 49% of respondents reported wearing a face mask in outdoor settings compared with 86% in indoor settings. 15 Lower face covering compliance in outdoor settings may be driven by a perceived lower risk of SARS-CoV-2 transmission in outdoor conditions, as well as federal and local guidelines not requiring the use of face coverings outdoors under most circumstances. Lower compliance was also observed in convenience stores and laundromats, which were indoors. However, we had few observations in these venues because they had few customers.
Lower compliance among males than among females and among younger age groups than among older age groups in our study is also consistent with other studies that relied on observational or self-reported data. A June 2020 study in Wisconsin observing grocery store shoppers found that face mask use increased with age and was 1.5 times more likely among women than among men. Face mask use continued to be higher among women than among men during observations in August 2020 after implementation of a face mask mandate. 13 Similarly, a nationally representative Gallup Poll measuring trends in self-reported face mask use outside the home found a 9 percentage-point gap between men and women in June 2020 (78% vs 87%) and a 4 percentage-point gap in September 2020 (89% vs 93%). 16
Exclusion of people aged 2 to 4 years from the state face mask mandate may explain the lower overall observed face covering use among the youngest age group (2-11 years). An order issued by CDC during the study period on January 29, 2021, which exempted children aged <2 years from wearing a face mask on conveyances and at transportation hubs including airports, 17 may explain the weaker association (PR = 2.51 vs 2.74) of the youngest age group with nonuse or incorrect use of face coverings at SeaTac International Airport. Stricter guidelines and enforcement at the airport also likely explain the attenuation of associations with nonuse or incorrect use of face coverings by sex.
The significant decline in face covering use among adults aged ≥60 years coincided with mass vaccination of people in this age group in King County and with a fourth wave of infections. Washington State Department of Health opened vaccination eligibility to all adults aged ≥65 years on January 18, 2021, and adults aged ≥60 years on March 31, 2021. As of May 17, 2021, 92% of adults aged 65 to 74 years and 98% of adults aged ≥75 years in King County had received ≥1 documented vaccine dose. 18 Declines in face covering use may have been partly driven by perceptions that vaccination-conferred immunity eliminated the need for face coverings. Of note, COVID-19 cases in King County increased during March 2021 and peaked in late April 2021. 19 Similar declining patterns in use of face coverings were observed among participants of a cross-sectional study in Israel, where rates of vaccination coverage are high. 20 In contrast, declines in the use of face coverings among younger age groups occurred before April 15, 2021, when vaccine eligibility was opened to people aged ≥16 years.
Limitations
Our findings were subject to at least 4 limitations. First, the observational design of the study could limit the accuracy of associations between reported characteristics and face covering use. We did not perform χ2 tests to validate the significance of overall face covering use because we could not confirm whether people were re-observed. Because of safety concerns, observers remained outside most venues while recording face covering use as people were entering businesses and, thus, were only able to approximate indoor face covering use. Despite observer training, estimated age group and sex of observed people could be subject to misclassification, and information on conditions that would exempt an individual from the mandate, such as a medical condition, mental health condition, or disability that prevents wearing a face covering, was not captured. Selection bias may have been present in the observed data if certain people were preferentially observed during high-volume observation periods, when observing every person was not possible. Second, certain observation intervals at some venues had low volume (<10 people), which could have affected the precision of observed trends, and further stratification by age, location, and observation period would have led to imprecise estimates and wide 95% CIs. Confounder adjustment was also limited by sample size and the variables that could be assessed under the study design.
Third, observations in this study were limited to publicly accessible venues selected purposively. Thus, they did not capture data on face covering use in private settings, where compliance may be lower and risk of SARS-CoV-2 transmission may be higher, 21 and may not represent broader face mask use behavior in King County. Finally, we could not assess the quality of the face covering (filtration and fit) the person was wearing in this observational study. As seen with the highly transmissible Omicron variant, the quality of the face covering could influence transmission and has led to guidance from public health agencies to upgrade face coverings to be more protective. 22 In addition, different types of face masks might be associated with different levels of compliance.
Conclusions
Trends in face covering use will continue to fluctuate as federal, state, and local guidance and individual behaviors change in response to fluctuating incidence of COVID-19 as new variants of concern emerge and as vaccine eligibility and access expand. At the end of our data collection, the face mask mandate was lifted as Washington State adopted CDC guidance 23 released on May 13, 2021, recommending that fully vaccinated people no longer needed to use face coverings in most indoor settings. 24 Meanwhile, King County continued to urge the use of face masks indoors until vaccination coverage among adults aged ≥16 years reached 70%. 25 With the emergence and rapid spread of the Delta variant causing surges in COVID-19 incidence nationwide, CDC reversed this recommendation at the end of July 2021, urging fully vaccinated people to wear a face mask in indoor public settings in areas of substantial or high transmission. 26 Washington State responded by reinstituting a statewide face mask mandate in indoor public settings regardless of vaccination status on August 23, 2021. 27 The governor issued a mandate for all Washington State employees, health care workers, and employees in kindergarten through grade 12 schools and higher education to be fully vaccinated as of October 18, 2021. 28 Statewide vaccine eligibility for the Pfizer-BioNTech vaccine was also expanded to people aged ≥12 years on May 11, 2021, 29 and to people aged ≥5 years on November 3, 2021, 30 and COVID-19 booster shots were recommended to people aged ≥12 years and immunocompromised people aged ≥5 years on January 6, 2022. 31
Directing tailored public health messaging to males and younger people and their guardians and improving enforcement in areas with a low use of face coverings could further mitigate the risk of SARS-CoV-2 community transmission, particularly in high-risk settings such as crowded indoor venues with poor ventilation, and among people who are unvaccinated, immunocompromised, or at elevated risk of infection. More importantly, reinforcing the face mask mandate through public health messaging urging people, regardless of vaccination status, to continue using face coverings in indoor settings is especially urgent in the context of local increases in cases and hospitalizations as vaccination coverage is expanded.
Validated methodologies for surveillance of face covering use, promotion, and impact evaluation that can be rapidly rolled out during an outbreak may be important in controlling respiratory-related pandemics in the future. The protocols and systems we have developed here to assess trends in face covering use can be tailored and deployed by local health jurisdictions for their surveillance needs, provide a model to measure adherence to face mask policies, and allow adherence data to be linked with relevant COVID-19 outcomes, such as cases and hospitalizations.
As SARS-CoV-2 and emerging variants continue to circulate and cause infections, it is crucial to maintain, monitor, and provide tailored interventions to optimize the use of layered mitigation strategies, including mandatory and recommended face mask policies, while striving to maximize vaccination nationally and globally.
Footnotes
Acknowledgements
The authors thank Amanda M. Besel, C. Addison Houston, and Lin Song (Public Health–Seattle & King County); Doug Loates (Tacoma-Pierce County Health Department); Joshua Marcy (Seattle–Tacoma International Airport); and Anida Hanifa, Casey Adams, Gabriel Blanchet, Callie Rockey-Bartlett, Karsyn Suhadolnik, Daaniya Iyaz, Sabrina Liu, Josephine Yen, and Shadi Henchiri (University of Washington student volunteer observers) for their assistance with the design and/or implementation of data collection.
Authors’ Note
Lorenzo Tolentino and Brandon Guthrie contributed equally to this article as co–first authors. Martin Cohen and Judith Wasserheit contributed equally to this article as co–senior authors.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marissa G. Baker received payment from the National Institute of Occupational Safety and Health via an Intergovernmental Personnel Act to support the federal, county, and city government with COVID-19 response, and provides paid consulting to Sony TV on its COVID-19 protocols, including advice on wearing face masks.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: Lorenzo Tolentino, Brandon Guthrie, Marissa G. Baker, Nicola K. Beck, Martin A. Cohen, and Judith N. Wasserheit received funding from the Washington State Department of Health to support manuscript-related activities.