
Abstract
Objectives:
The Advisory Committee on Immunization Practices recommends persons aged ≥6 months receive an influenza vaccination annually, and certain adults aged ≥19 years receive the 23-valent pneumococcal polysaccharide vaccine alone or in series with the 13-valent pneumococcal conjugate vaccine, depending on age, chronic conditions, and smoking status. This study examines the prevalence of influenza and pneumococcal vaccination relative to Healthy People 2020 goals to understand how vaccination receipt differs by veteran status and sociodemographic subgroups.
Methods:
We analyzed pooled data from the 2016-2018 National Health Interview Survey (N = 35 094) in 2021 to estimate the prevalence of influenza and pneumococcal vaccination for men aged 25-64 years and for men aged ≥65 years by veteran status and selected sociodemographic subgroups. We used 2-tailed t tests with an α = .05 to identify significant differences.
Results:
Among men, 44.7% of veterans and 33.5% of nonveterans aged 25-64 years and 71.0% of veterans and 64.9% of nonveterans aged ≥65 years received an influenza vaccine in the past year. Among men aged 25-64 years at high risk for pneumococcal disease, 35.9% of veterans and 20.8% of nonveterans had ever received ≥1 dose of any pneumococcal vaccination. Disparities in the prevalence of vaccination within examined sociodemographic characteristics were often smaller in magnitude among veterans than among nonveterans for both vaccinations.
Conclusions:
Vaccination rates were below Healthy People 2020 targets for both groups, except influenza vaccination among veterans aged ≥65 years. Understanding differences in vaccine uptake may inform efforts to improve vaccination rates by identifying subgroups who are at high risk of disease and have low vaccination rates.
Influenza viruses were responsible for an estimated 400 000 hospitalizations and 22 000 deaths in the United States during the 2019-2020 influenza season. 1 Streptococcus pneumoniae (pneumococcus) was responsible for an estimated 150 000 hospitalizations and approximately 3500 deaths in 2018. 2 To reduce these burdens, the Advisory Committee on Immunization Practices recommends persons aged ≥6 months receive an influenza vaccination annually and certain adults aged ≥19 years receive the 23-valent pneumococcal polysaccharide vaccine (PPSV23) alone or in series with the 13-valent pneumococcal conjugate vaccine (PCV13), depending on age, presence of chronic medical conditions, and smoking status.3,4
Risks for influenza and Streptococcus pneumoniae are higher among adults who are older or have certain medical conditions.5,6 Risk for Streptococcus pneumoniae is also higher among current smokers. 6 On average, veterans are older, have a greater prevalence of chronic health conditions that increase their risk for complications of influenza or pneumococcal disease, and are more likely to smoke than nonveterans.7,8 In the Veterans Health Administration (VHA), influenza and pneumococcal vaccination are performance measures tracked by regional networks to monitor quality of care.9,10
To understand how vaccine uptake differs by veteran status overall and among sociodemographic subgroups, as well as how uptake compares with Healthy People 2020 goals, this study examined self-reported prevalence of influenza and any pneumococcal vaccination among men aged 25-64 and ≥65 years.
Methods
Study Sample
The National Health Interview Survey (NHIS) is a household-based survey of the civilian, noninstitutionalized US population in which 1 sample adult is selected from each family in the household to answer health-related questions. In 2021, we analyzed pooled data from the 2016-2018 NHIS (35 094 total sample adults; average response rate, 53.5%).11-13 The National Center for Health Statistics (NCHS) Ethics Review Board reviewed and approved the 2016-2018 NHIS protocols prior to survey implementation and data collection.
Measures
We ascertained veteran status from the question, “Have you ever served on active duty in the US Armed Forces, military Reserves, or National Guard?” To better compare veterans and nonveterans, we limited the analytic sample to men aged ≥25 years; the sample sizes for female veterans and veterans aged <25 years were small, precluding reliable estimates of vaccination for these groups. We ascertained influenza and pneumococcal vaccination status from the following questions: “During the past 12 months, have you had a flu vaccination?” and “Have you ever had a pneumonia shot?”
To align with vaccination recommendations, 3 estimates of influenza vaccination included all men aged 25-64 and ≥65, whereas estimates of pneumococcal vaccination included men aged 25-64 who were defined as high risk for pneumococcal disease based on the Healthy People 2020 definition and criteria, and all men aged ≥65. 14 Consistent with Healthy People 2020 and a previously published definition, we classified men aged 25-64 as high risk for pneumococcal disease if they had ever been told by a health professional that they had diabetes, emphysema, chronic obstructive pulmonary disease, coronary heart disease, angina, heart attack, other heart condition, lymphoma, leukemia, or blood cancer; in the past year had an asthma attack, had a cancer diagnosis (excluding nonmelanoma skin cancer), or had been told by a health professional that they had chronic bronchitis or weak or failing kidneys; or were current smokers.14,15
We examined vaccination by various sociodemographic characteristics, including age, race and Hispanic origin, educational attainment, and poverty status. Poverty status was based on federal poverty level (FPL). Income was imputed for approximately 20% of adults.16-18 Health conditions included chronic heart disease (ever diagnosed with coronary heart disease, angina, heart attack, or other heart condition), chronic lung disease (ever diagnosed with emphysema, chronic obstructive pulmonary disease, chronic bronchitis, or having an asthma attack in the past year), diabetes, cancer (ever diagnosed with lymphoma, leukemia, or blood cancer or having been diagnosed with any cancer other than nonmelanoma skin cancer in the previous year), and current cigarette smoking (smoked 100 cigarettes in their lifetime and currently smoke). Access-to-care variables included having seen a doctor or other health care professional in the past 12 months, as well as having a usual place of care. Dental care was not included in having seen a health care professional in the past 12 months nor were doctors or other health professionals seen while hospitalized overnight, visits to the emergency department, home visits, or telephone calls. Adults who reported the emergency department as their usual place of care were defined as not having a usual place of care.
Statistical Analysis
We generated weighted estimates stratified by age and veteran status by using SUDAAN release 11.0.3 (RTI International). We used the Korn–Graubard method to generate 95% CIs. We suppressed estimates that did not meet NCHS Data Presentation Standards. 19 We used 2-tailed t tests with an α of .05 to identify significant differences by veteran status.
Results
Among men aged 25-64, 44.7% (95% CI, 42.5%-47.0%) of veterans and 33.5% (95% CI, 32.6%-34.3%) of nonveterans received an influenza vaccination in the past year (Table 1). The prevalence of influenza vaccination was significantly higher among veterans aged 25-64 than among nonveterans aged 25-64 across all sociodemographic and health-related subgroups other than the groups with chronic lung disease or diabetes (Table 1). Differences in the prevalence of influenza vaccination by sociodemographic characteristics (eg, non-Hispanic White vs non-Hispanic Black) were often smaller in magnitude among veterans than among nonveterans for men aged 25-64.
Receipt of influenza vaccination among all men aged 25-64 years and pneumococcal vaccination among men aged 25-64 years at high risk of pneumococcal disease, a by veteran status and selected sociodemographic and health-related characteristics, National Health Interview Survey, United States, 2016-2018 b
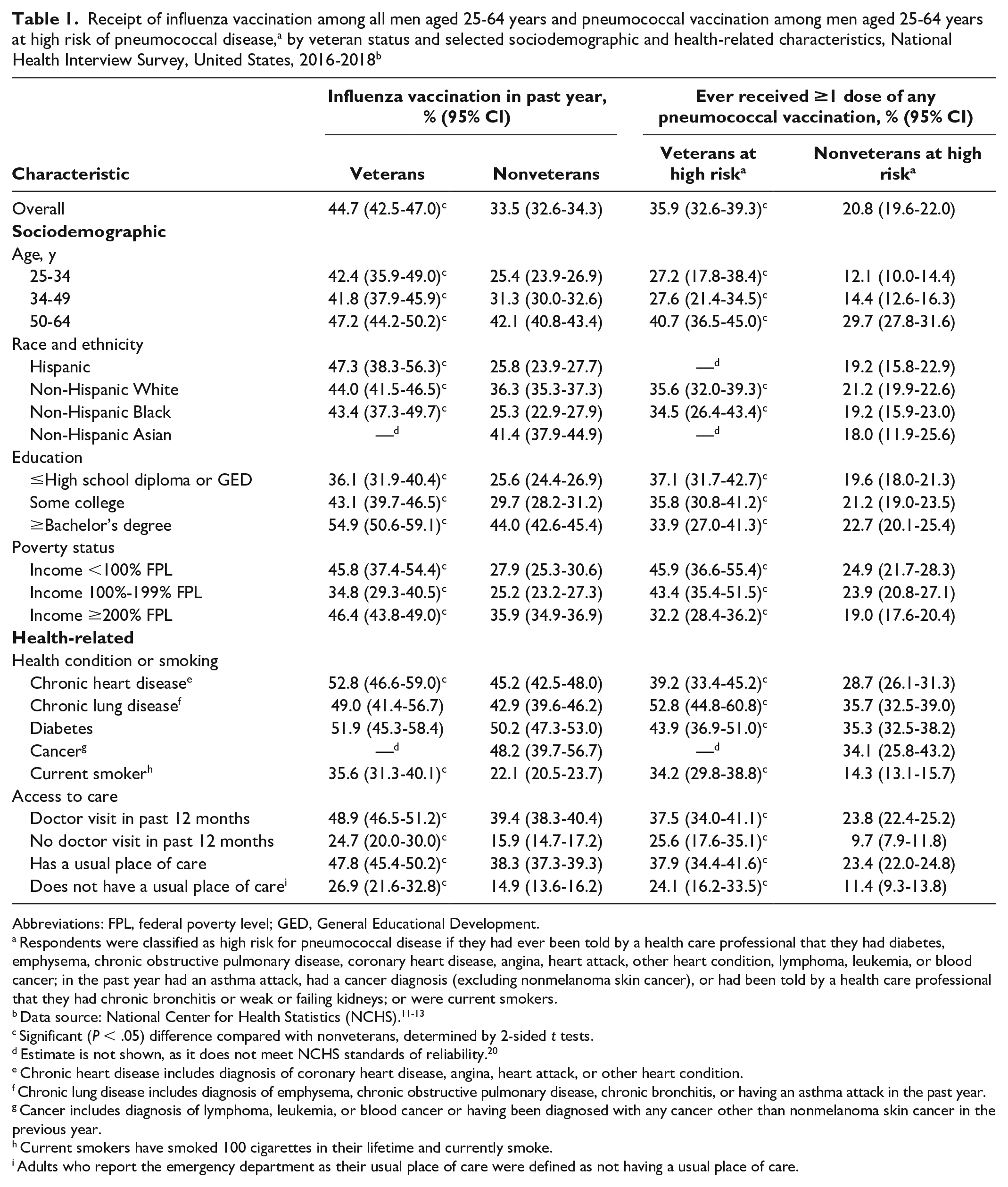
Abbreviations: FPL, federal poverty level; GED, General Educational Development.
Respondents were classified as high risk for pneumococcal disease if they had ever been told by a health care professional that they had diabetes, emphysema, chronic obstructive pulmonary disease, coronary heart disease, angina, heart attack, other heart condition, lymphoma, leukemia, or blood cancer; in the past year had an asthma attack, had a cancer diagnosis (excluding nonmelanoma skin cancer), or had been told by a health care professional that they had chronic bronchitis or weak or failing kidneys; or were current smokers.
Significant (P < .05) difference compared with nonveterans, determined by 2-sided t tests.
Estimate is not shown, as it does not meet NCHS standards of reliability. 20
Chronic heart disease includes diagnosis of coronary heart disease, angina, heart attack, or other heart condition.
Chronic lung disease includes diagnosis of emphysema, chronic obstructive pulmonary disease, chronic bronchitis, or having an asthma attack in the past year.
Cancer includes diagnosis of lymphoma, leukemia, or blood cancer or having been diagnosed with any cancer other than nonmelanoma skin cancer in the previous year.
Current smokers have smoked 100 cigarettes in their lifetime and currently smoke.
Adults who report the emergency department as their usual place of care were defined as not having a usual place of care.
Among men aged 25-64 at high risk for pneumococcal disease, 35.9% (95% CI, 32.6%-39.3%) of veterans and 20.8% (95% CI, 19.6%-22.0%) of nonveterans reported ever having received ≥1 dose of any pneumococcal vaccination (PCV13 or PPSV23). The prevalence of pneumococcal vaccination was significantly higher among veterans aged 25-64 than among nonveterans aged 25-64 in every sociodemographic and health-related subgroup.
Among men aged ≥65, 71.0% (95% CI, 69.3%-72.7%) of veterans and 64.9% (95% CI, 63.3%-66.5%) of nonveterans received an influenza vaccination in the past year, and 74.5% (95% CI, 72.7%-76.1%) of veterans and 60.4% (95% CI, 58.6%-62.2%) of nonveterans had ever received ≥1 dose of any pneumococcal vaccination (Table 2). Disparities in the prevalence of vaccination by sociodemographic characteristics were often smaller in magnitude among veterans than among nonveterans for both vaccinations among men aged ≥65. The prevalence of influenza vaccination was significantly higher among veterans aged ≥65 than among nonveterans aged ≥65 across most sociodemographic subgroups, but it was similar among men with chronic lung disease and cancer and current smokers. Among men aged ≥65, the prevalence of influenza vaccination was significantly higher among veterans than among nonveterans among men with a doctor visit in the past 12 months (73.2% vs 67.7%) and among men with a usual place of care (72.4% vs 67.0%). However, the prevalence of vaccination was not significantly higher among veterans compared with nonveterans without a doctor visit in the past 12 months (37.5% vs 32.4%) or without a usual place of care (35.0% vs 27.7%). The prevalence of pneumococcal vaccination was significantly higher among male veterans aged ≥65 than among male nonveterans aged ≥65 across all sociodemographic and health condition subgroups other than cancer. Among men aged ≥65, the prevalence of pneumococcal vaccination was significantly higher among veterans than among nonveterans with a doctor visit in the past 12 months (76.6% vs 62.9%), with a usual place of care (75.5% vs 62.4%), and without a usual place of care (46.8% vs 24.4%). However, pneumococcal vaccination did not differ significantly by veteran status among men without a doctor visit in the past 12 months (40.6% vs 32.3%).
Receipt of influenza and pneumococcal vaccination among men aged ≥65 years, by veteran status and selected sociodemographic and health-related characteristics, National Health Interview Survey, 2016-2018 a
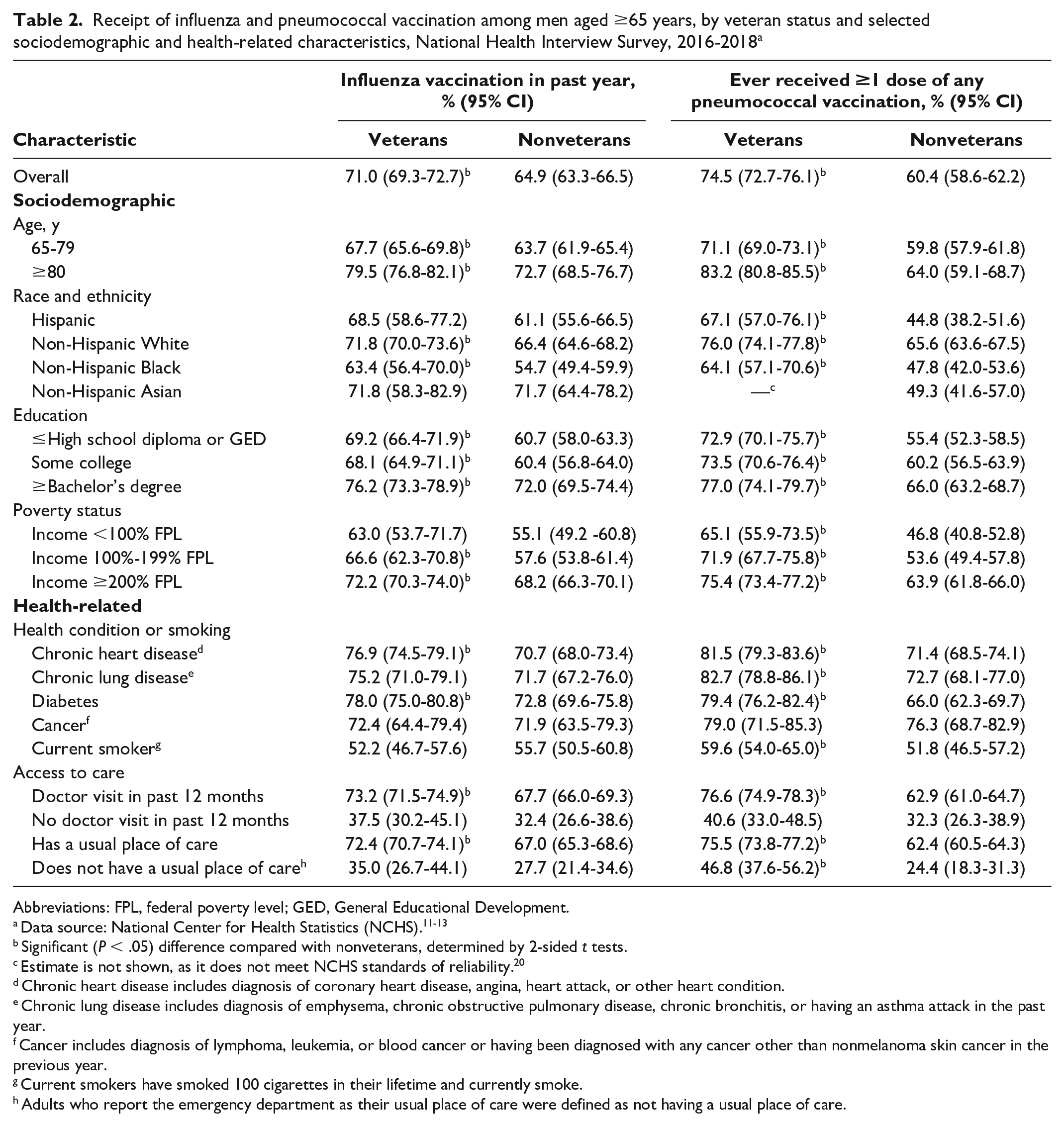
Abbreviations: FPL, federal poverty level; GED, General Educational Development.
Significant (P < .05) difference compared with nonveterans, determined by 2-sided t tests.
Estimate is not shown, as it does not meet NCHS standards of reliability. 20
Chronic heart disease includes diagnosis of coronary heart disease, angina, heart attack, or other heart condition.
Chronic lung disease includes diagnosis of emphysema, chronic obstructive pulmonary disease, chronic bronchitis, or having an asthma attack in the past year.
Cancer includes diagnosis of lymphoma, leukemia, or blood cancer or having been diagnosed with any cancer other than nonmelanoma skin cancer in the previous year.
Current smokers have smoked 100 cigarettes in their lifetime and currently smoke.
Adults who report the emergency department as their usual place of care were defined as not having a usual place of care.
Discussion
In 2016-2018, among men aged 25-64, 44.7% of veterans and 33.5% of nonveterans received an influenza vaccination in the past year. Among men aged 25-64 at high risk of pneumococcal disease, one-third of veterans and one-fifth of nonveterans had ever received ≥1 dose of any pneumococcal vaccination. Among men aged ≥65, prevalence was close to three-quarters of veterans and close to two-thirds of nonveterans for both vaccinations. Influenza vaccination of veterans aged 25-64 and nonveterans of both age groups fell short of Healthy People 2020 goals (70% of adults aged ≥18). 14 Pneumococcal vaccination of veterans and nonveterans of both age groups fell short of Healthy People 2020 goals (90% of adults aged ≥65; 60% of adults aged 18-64 at high risk of pneumococcal disease). 14
These findings corroborate previous research that found influenza vaccination was higher among veterans than among nonveterans. 20 This finding may be due in part to some veterans having access to affordable preventive care through the VHA, as well as VHA performance measurement programs that have been shown to increase influenza and pneumococcal vaccination rates among VHA users so that vaccination rates are higher than rates among the general population.9,10,20 However, research on whether veterans and nonveterans have different health-seeking behaviors, independent of type of health coverage and health care access, is lacking. As noted by Der-Martirosian et al, 20 future studies (eg, with forthcoming linked administrative and survey data 21 ) that examine differences in vaccination rates and general health-seeking behaviors between VHA users and non–VHA users could further explain overall differences by veteran status.
Prior survey research of the general population found a lower prevalence of influenza vaccination among current smokers compared with never smokers 22 and among adults without a physician visit within the last year compared with adults with a physician visit within the last year. 23 Our study found that the prevalence of influenza vaccination was higher among veterans than among nonveterans among men aged 25-64 who were either current smokers or without a doctor visit within the past 12 months. Among men aged ≥65, the prevalence of influenza vaccination among current smokers and those without a doctor visit in the past 12 months did not differ by veteran status. Black, Hispanic, and Asian veterans who used VHA services were more likely than White veterans to receive a VHA-administered COVID-19 vaccination, whereas Black and Hispanic people in the general population were less likely than their White counterparts to have received a COVID-19 vaccine. 24 Relatedly, in our study, we note that differences in influenza and pneumococcal vaccination prevalence by race and ethnicity were often smaller in magnitude among veterans than among nonveterans.
Limitations
Our study had several potential limitations. First, data were based on self-report, which may have resulted in recall bias.25,26 Despite this limitation, we used NHIS data, rather than data obtained from medical and administrative records, so that estimates could be generalized to all community-dwelling veterans and compared between veterans and nonveterans overall and by sociodemographic subgroup. Second, we evaluated only whether adults received ≥1 dose of any pneumococcal vaccination, not whether adults received the recommended number of doses or the recommended kind of vaccine (PCV13 or PPSV23). Third, data on several indications for pneumococcal vaccination are not captured by NHIS. As a result, not all adults who are at high risk for pneumococcal disease were able to be classified as such in our study.
Conclusion
Except for influenza vaccination among male veterans aged ≥65, overall prevalence of both vaccinations fell short of established Healthy People 2020 goals among veterans and nonveterans of both age groups. We observed this shortfall among many veteran and nonveteran subgroups, including adults who were older or had certain medical conditions, which may increase their risk for medical complications from influenza and Streptococcus pneumoniae,5,6 as well as among adults with limited access to care. Understanding how vaccine uptake differs by veteran status and age across sociodemographic characteristics, health status, and access to care may inform ongoing efforts to improve vaccination rates, such as the VHA performance measurement program, by identifying subgroups who are at high risk of disease and have low vaccination rates.
Footnotes
Acknowledgements
The views expressed in this article are those of the authors and do not necessarily represent the official views of the National Center for Health Statistics, the Centers for Disease Control and Prevention, the US Department of Health and Human Services, the Office of Health Equity, or the Veterans Health Administration.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the Veterans Health Administration Office of Health Equity.