
Abstract
Objectives:
Medicaid provides health insurance for low-income people meeting specific eligibility requirements. It is funded and administered by both the federal and state governments; this decentralization leads to vastly different programs across the country. The objective of this legal surveillance project was to describe state-by-state differences in podiatric care coverage for nonelderly adults across Medicaid programs.
Methods:
We used policy surveillance, a form of advanced legal mapping. It is the systematic collection and analysis of written policies across jurisdictions. Policy surveillance captures the important features of law through a rigorous scientific process to turn these policies into structured, quantitative legal data that are suitable for further evaluation or modeling. Data for the 51 jurisdictions were current as of September 1, 2020.
Results:
The vast majority of jurisdictions (82%) covered podiatric services for all classes of Medicaid beneficiaries, but the rules, restrictions, and limitations around coverage differed. Twenty-five jurisdictions had no limits on the number of podiatric visits during a specified period; 26 jurisdictions indicated a cap. Ten jurisdictions had no explicit limitations on coverage of routine foot care, whereas 33 jurisdictions covered routine foot care only when medically necessary or with a triggering condition. Eight jurisdictions did not cover routine foot care at all, and 28 jurisdictions required prior authorizations.
Conclusions:
Podiatric care coverage, which is often preventive, varies greatly by state. This variability in coverage, which has not been previously tracked at the level of detail provided in our study, has implications for cost and health outcomes. The value of podiatric care is especially apparent in Medicaid populations. The compilation of these data can serve as a valuable resource for clinicians, researchers, and policy makers.
Medicaid was established to provide health insurance for low-income people, including children, parents, pregnant women, older adults, and those with disabilities. 1 The program is funded by both the federal and state governments based on a formula (Federal Medical Assistance Percentages) that varies by state, with poorer states receiving a higher percentage of federal funding. Based on federal guidelines, all state Medicaid programs are required to provide 15 specific services as covered benefits. These mandatory benefits include such things as hospital services; the Early and Periodic Screening, Diagnostic, and Treatment Services benefit; laboratory and x-ray services; and transportation to medical care. As of 2020, states could opt to cover an additional 28 services. 2 Of these optional covered benefits, prescription drug coverage is one that all states cover to some extent. Many states also include benefits for services such as vision coverage, dental care, and respiratory care. Podiatric care is one of the optional covered benefits that states provide to varying degrees. 3 Optional Medicaid-covered podiatric services generally include nail debridement, cutting/trimming of corns or calluses, treatment of mycotic nails, and preventive services related to diabetes or peripheral neuropathy.
Because states share in the cost of coverage, economic downturns and state Medicaid budgets are linked. Medicaid is countercyclical to the economy: costs typically increase during a recession as a result of unemployment and increased program enrollment, whereas the ability of states to pay these costs decreases through lost tax revenue. 4 To cope, states have few options. They can reduce benefit eligibility, make cuts to services, renegotiate Medicaid managed care contracts, and/or cut payments to health care providers. 5 If states determine that cutting services is necessary, they often focus on optional covered benefits, such as podiatry. The clinical and economic implications of cutting services, particularly optional benefits such as podiatric care, can be substantial. 3
Podiatric care has been linked to improved health outcomes, reduced hospitalizations, and a lower overall cost for the health care system in general and individual patients, especially as it relates to the management of chronic conditions such as diabetes, obesity, and vascular conditions.6,7 Preventive podiatric care such as nail debridement and treatment of calluses is particularly essential for people susceptible to foot problems and conditions such as diabetic foot ulcers, because identifying problems before they worsen is key.8,9
The Medicaid population typically comprises people experiencing poverty and those at increased risk for health complications, including low-income adults, pregnant women, children, older adults, and people with disabilities. Communities of color are overrepresented among Medicaid recipients. In 2019, 41% of Medicaid beneficiaries nationwide were categorized as non-Hispanic White, 20% as non-Hispanic Black, and 29% as Hispanic, whereas in the overall population, about 60% are categorized as non-Hispanic White, 13.4% as non-Hispanic Black, and 18.5% as Hispanic or Latino. 10
Poverty is well established as having a major impact on health. Low-income Americans have higher rates of chronic conditions such as heart disease, diabetes, and stroke than their higher-income counterparts. 11 Communities of color also have higher rates of these 3 chronic conditions. Compared with non-Hispanic White people, African American people have a 77% higher risk and Hispanic people have a 66% higher risk of being diagnosed with diabetes. 12 Given that Medicaid recipients are people with low income and that communities of color are overrepresented in the Medicaid population and more likely to have chronic conditions, it is clear that access to podiatric care is a health equity issue.
A growing body of research is demonstrating the relationship between Medicaid coverage for podiatry services and clinical outcomes for patients with diabetes, peripheral vascular diseases, and other chronic conditions of the foot. 3 Associated with these clinical outcomes, dramatic cost savings have been realized in the reduction of amputations and other severe clinical outcomes, and when podiatric coverage is eliminated, costs increase in the long term. For example, the Arizona legislature eliminated Medicaid reimbursement for podiatric coverage effective in 2010. This cut was part of a larger package of Medicaid changes designed to help address a budget shortfall associated with the Great Recession that began in 2007. Eliminating podiatric coverage saved the state an estimated $351 000. 13 Although appearing to save money on the front end, the elimination of podiatric coverage ultimately had the opposite effect. A multivariate analysis associated the elimination of podiatric coverage with changes in outcomes related to diabetic foot ulcers, a condition commonly treated by podiatric physicians. Relative to the years before the elimination of podiatric coverage, hospital admissions increased (36.7%), as did charges (37.5%), lengths of stay (22.5%), and severe aggregate outcomes such as mortality, amputation, sepsis, and surgical complications (49.0%). 13 Estimates place the financial toll of the elimination of podiatric coverage at approximately $16.7 million. 13 Ultimately, for every dollar saved by cutting podiatric coverage, the state of Arizona spent $48 to treat preventable complications. Podiatric coverage was ultimately restored in Arizona on October 1, 2016. 14 Studies in California 15 and Texas 16 yielded similar conclusions.
As illustrative as these study results are, their generalizability is limited beyond the few states studied. To fully understand the impact of Medicaid coverage, large-scale, quasi-experimental, multijurisdictional studies are required. To undertake this type of research, a granular understanding of Medicaid reimbursement schemes beyond the binary coverage/no coverage distinction is needed. A more complete picture will enable researchers to study the effects of multiple features and patterns in coverage across all jurisdictions. For example, how do age restrictions in coverage affect cost and outcomes? Does the requirement for a primary care referral act as a barrier to consumption of podiatric services? No completely comprehensive accounting of these policies exists.
Two previous projects aimed to catalog information on Medicaid coverage for podiatric services. The first was undertaken by the Kaiser Family Foundation in 2003 as part of its Medicaid Benefits Survey completed by state Medicaid directors. 17 The seventh, and most recent, update was completed in 2018. Although helpful as a summary, the data are updated infrequently, lack detail, and do not cite primary sources. The second project was a database (unpublished) compiled by the American Podiatric Medical Association in 2012. The manual was intended as a policy guide for association members and an educational resource when meeting with legislators and policy makers on issues related to podiatry. Although much more detailed than the KFF database, this manual was not shared widely with the research community and has not been updated since 2012.
The objective of this study was to fill the gaps in knowledge about Medicaid coverage for podiatric services by creating a comprehensive accounting of all available statutory, regulatory, and programmatic documentation related to fee-for-service Medicaid coverage for podiatric services in the United States. In addition to collecting the data, the project has made citations and full text available to researchers, policy makers, and the public through the LawAtlas system.
Methods
We used methods outlined in Anderson et al 18 to develop the policy surveillance mapping strategy. Policy surveillance, a form of advanced legal mapping, is the systematic collection and analysis of written policies across jurisdictions. Policy surveillance captures the important features of law through a systematic process to turn these policies into structured, quantitative legal data that are suitable for further evaluation or modeling. The iterative process uses a well-defined research methodology to track key elements of relevant policy across multiple jurisdictions, with an emphasis on quality control measures. These rigorous quality control methods ensure reliable and valid legal data. Policy surveillance builds on this reliability through emphasis on replicability and transparency, including the publication of a research protocol that includes descriptions of the project scope; the research process, including search terms and inclusion criteria; coding conventions used to create the data; and detailed tracking of quality control results.
We conducted policy surveillance on state-level statutes, regulations, and agency documents in the 50 states and the District of Columbia. The scope, or inclusion criteria, used were any state-level statutes, regulations, and agency documents related to Medicaid coverage of services provided by a podiatric physician. Data collection, cleaning, and validation took place from October 15, 2019, through October 1, 2020. The dataset as it exists at the time of release is cross-sectional, and information cited is current as of September 1, 2020.
After conceptualizing the scope of the project, we began an iterative process of identifying and recording citations of relevant statutes and regulations from Westlaw Next, a legal research database. We used keyword searches to identify relevant sources. The keyword terms included “podiatry,” “podiatrist,” “podiatric,” and “Podiatr*.” We reviewed the search results to ensure the information captured was in scope. We excluded results related to topics such as state licensure for podiatric physicians, professional board oversight, and podiatric scope of practice. When these searches yielded a relevant source, we examined the headings, chapter, and section titles containing the law to determine if any of the surrounding statutes or regulations were also relevant. When relevant information was limited or nonexistent in statutes and regulations, we executed the same keyword search terms on state Medicaid agency websites. We collected relevant documents, including health care provider billing manuals, fee schedules, member handbooks, state plan amendments, and agency training documents. If necessary, we reached out to state Medicaid agencies directly.
This process took place in iterative samples of 10 jurisdictions (5 jurisdictions for each research team member). After each batch of 10 jurisdictions’ information was compiled, the entire research team, including the principal investigator (T.W.B.), met to review the results. This discussion focused on what information could be gleaned from the collected data. In the early stages of the scoping process, sometimes a new aspect of a state’s Medicaid coverage scheme would present itself in the data. The researchers would then discuss the relative importance of the information and whether it would be possible to reliably collect this same information across all other jurisdictions. If the team decided the information was both important and able to be reliably collected, researchers returned to the already sampled jurisdictions, collected the new information, and added it to the coding sheet going forward. If the team decided against collecting a piece of information at the scoping stage, it was not included. This iterative scoping process ensured that important data elements were not ignored because of a priori decisions made by researchers. It also limited the data collection to elements that were consistently and reliably obtainable across all jurisdictions.
When all the statute and regulation text was collected, we created a coding sheet for each jurisdiction containing the agreed-upon data elements. Research staff members then independently coded the data for all 51 jurisdictions into an electronic database. Two researchers (G.K.B., J.S.C.) independently reviewed each other’s coding entries to ensure accuracy and consistency with agreed-upon coding guidelines. The 2 researchers then met to compare coding results. Any divergences were discussed and, if possible, resolved. If a resolution could not be reached, the 2 researchers and the principal investigator discussed the issue. If questions remained about the data, the team reached out to state officials or others for clarification and additional documentation. We used the final coding table during entry of the final data into the LawAtlas software (MonQcle; Temple University Center for Public Health Law Research). Each final data entry was subject to a final comparison against the original primary data source by the researcher uploading the record. Before publication, the research team made a final check of the data on MonQcle and discussed and resolved any final coding errors and discrepancies.
Through this process, the research team developed a research protocol document to outline the coding scheme, definitions, and scoping parameters, including any relevant inclusion and exclusion criteria. The research protocol ensured that the project is replicable and transparent.
Results
Forty-two of 51 jurisdictions covered podiatric services for all classes of Medicaid beneficiaries as of September 1, 2020 (Figure 1). We defined “all classes of Medicaid beneficiaries” as coverage of podiatric services extended to any individual enrolled in a state Medicaid program, as opposed to coverage of podiatric services limited by categorical factors such as age, medical diagnosis, and/or Medicare/Medicaid dual eligibility.
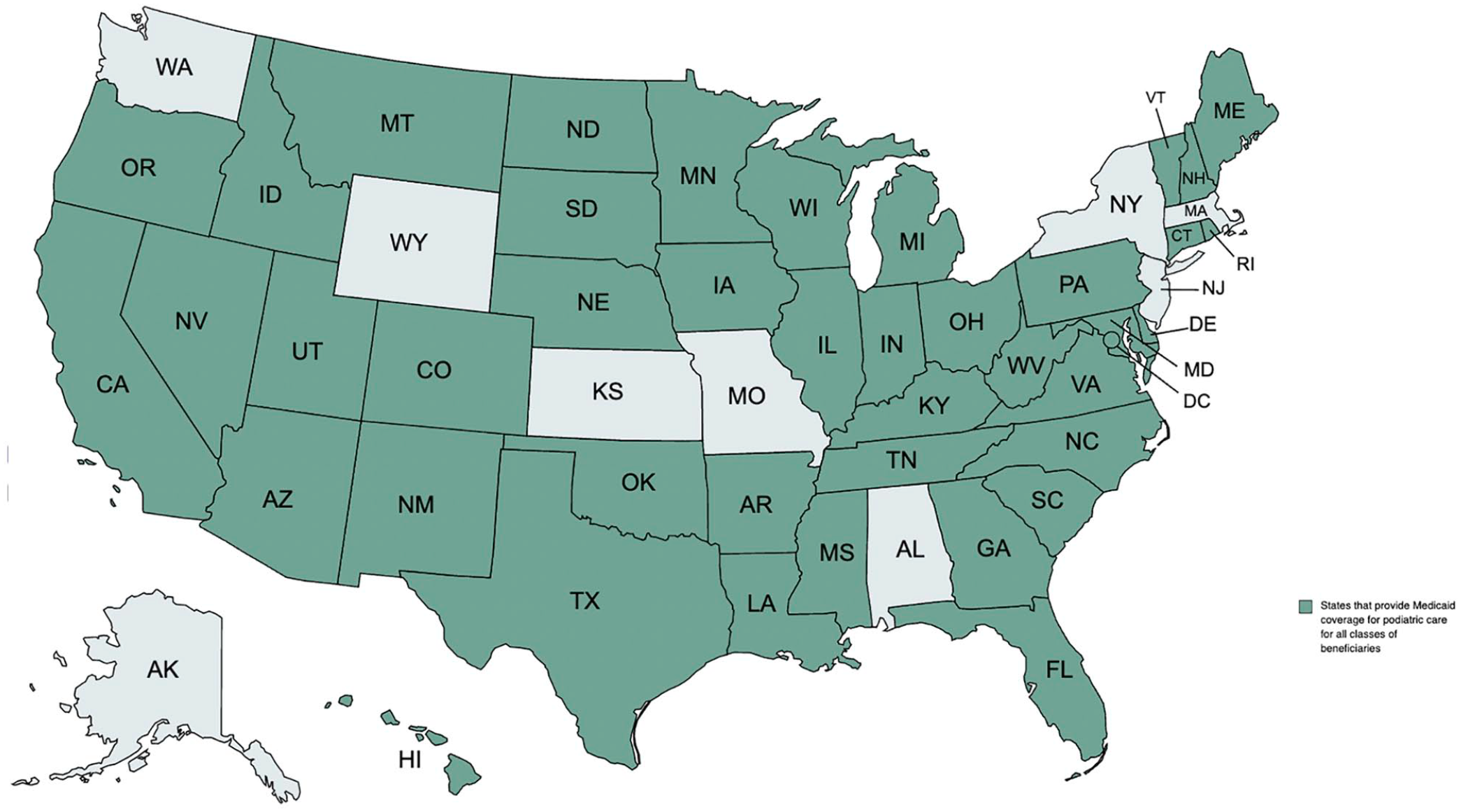
US states that provide Medicaid coverage for podiatric care for all classes of beneficiaries. Data were compiled by the research team through surveillance mapping, the systematic collection and analysis of written policies across jurisdictions, October 15, 2019, through October 1, 2020.
The number of states placing limits on the number of podiatric visits during a specified period was nearly split, with 25 jurisdictions placing no limits and 26 jurisdictions indicating a cap. Ten jurisdictions had no explicit limitations on coverage of routine foot care (Figure 2), whereas 33 jurisdictions covered routine foot care only when medically necessary or with a triggering condition. Eight jurisdictions did not cover routine foot care at all.
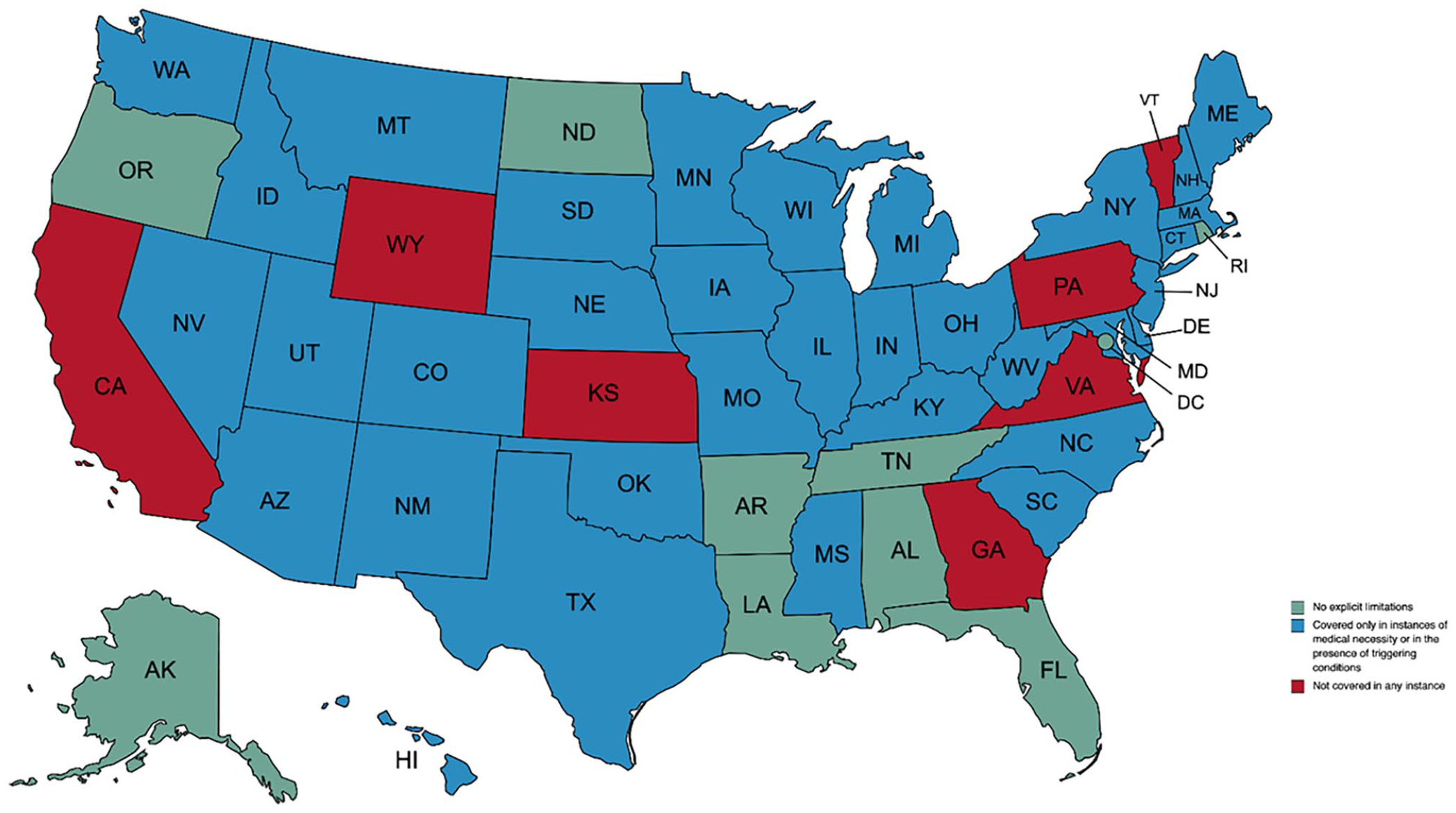
State policies on Medicaid coverage for routine foot care. Data were compiled by the research team through surveillance mapping, the systematic collection and analysis of written policies across jurisdictions, October 15, 2019, through October 1, 2020.
We found other restrictions on podiatric care as well; 28 jurisdictions required prior authorizations (Figure 3). Of the 50 jurisdictions for which we could find reliable information, 23 indicated out-of-pocket costs were associated with podiatric care. Finally, 38 jurisdictions specified at least 1 noncovered podiatric service; of these, 25 indicated they would cover the service in a medical emergency (Table).
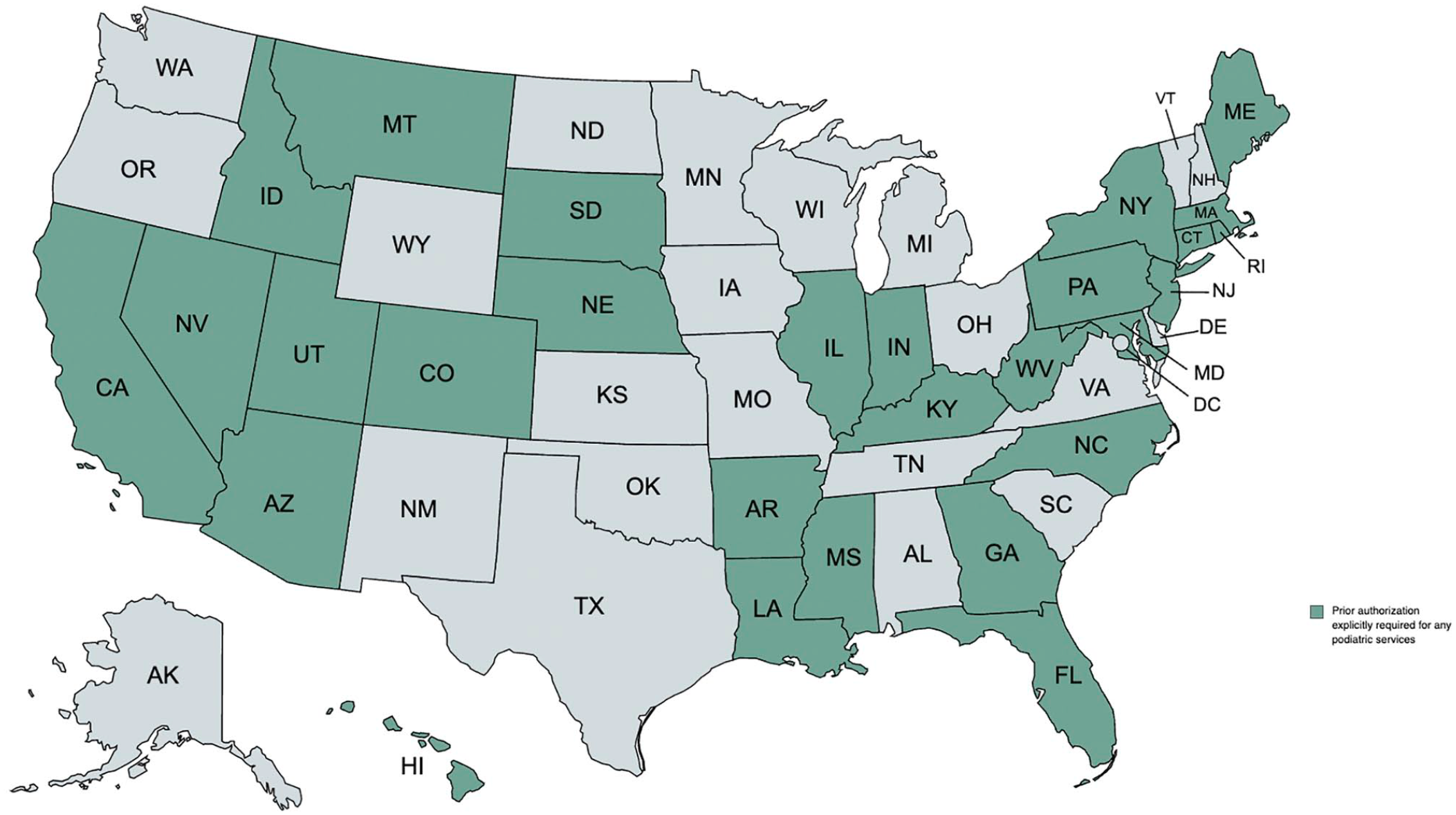
US states explicitly requiring prior authorization for any podiatric services. Data compiled by the research team through surveillance mapping, the systematic collection and analysis of written policies across jurisdictions, October 15, 2019, through October 1, 2020.
Limitations of state Medicaid coverage for podiatric services as of September 1, 2020, United States a
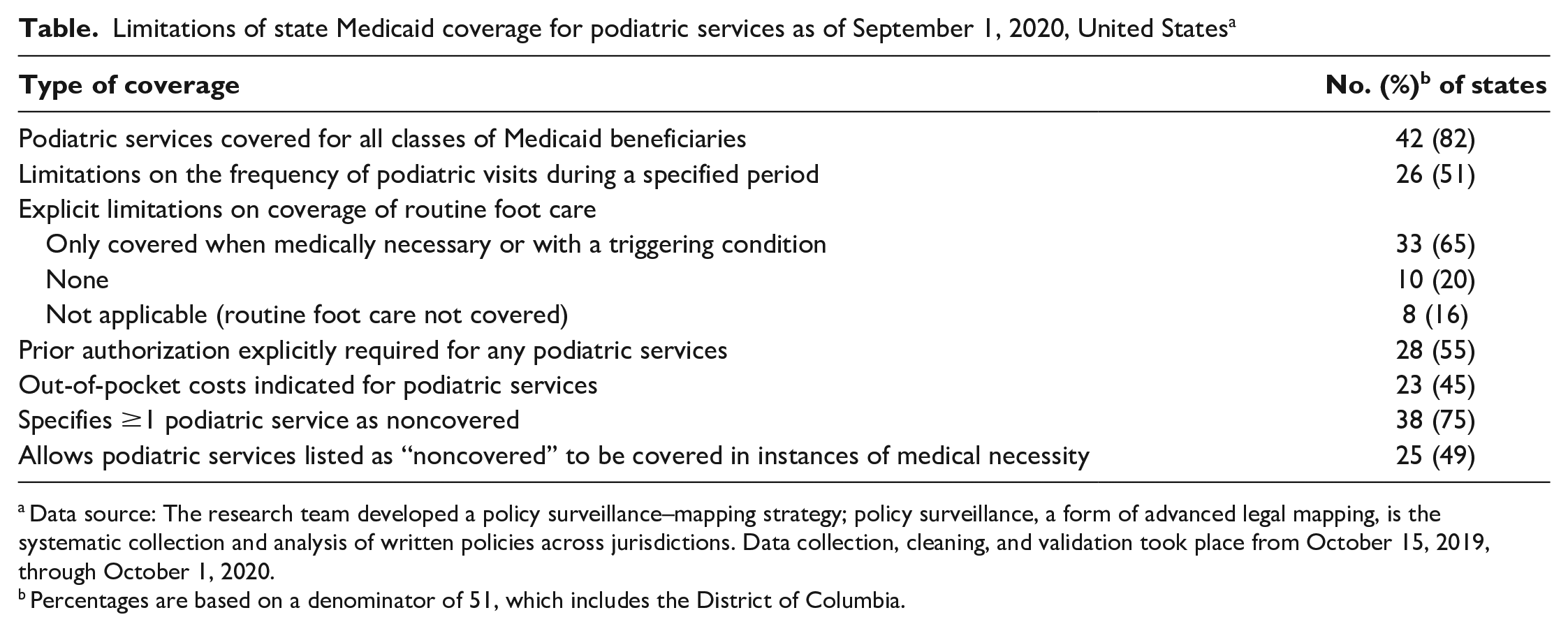
Data source: The research team developed a policy surveillance–mapping strategy; policy surveillance, a form of advanced legal mapping, is the systematic collection and analysis of written policies across jurisdictions. Data collection, cleaning, and validation took place from October 15, 2019, through October 1, 2020.
Percentages are based on a denominator of 51, which includes the District of Columbia.
Discussion
Medicaid coverage varies greatly across the 51 jurisdictions in the United States. What is covered, under what circumstances, and to what extent it is covered depends on where you live. Podiatric care exemplifies this variability. Multiple layers of statutes, regulations, program documentation, and other factors must be examined to compare coverage across the 50 states and the District of Columbia. Program variability can be a strength because it allows states to experiment with coverage options and try to direct resources where they can do the most good. It also has a big impact on patient care and, therefore, most certainly on health outcomes.
Our findings indicate that although most jurisdictions (82%) covered podiatric services for all classes of Medicaid beneficiaries, we found major differences in the rules, restrictions, and limitations related to this coverage. Twenty-five jurisdictions had limitations on the frequency of podiatric visits, and only 10 had no explicit limitations on the coverage of routine foot care.
Out-of-pocket costs have been shown to be a barrier to accessing health care for people with low income, 19 who would be part of the Medicaid population. The differences across programs for cost sharing will likely affect the health outcomes of beneficiaries in states that require cost sharing for podiatric care. Prior authorization requirements also create an additional barrier to receiving care; in 2020, the Centers for Medicare & Medicaid Services submitted a proposed rule to address this pervasive issue. 20 For Medicaid beneficiaries, who in general have greater health needs and lower income than the overall US population, any additional barriers to routine foot care can negatively impact overall health outcomes.
Our analysis contributes to the wider community of research related to access to podiatric care, health care coverage, Medicaid research, and policy analysis. The dataset that was compiled during this process is essential for comparing podiatric-related health outcomes for Medicaid beneficiaries as well as costs associated with podiatric-related health issues. The data can be accessed via the LawAtlas site. 21
Our project can also be used as an example of how to operationalize a policy surveillance mapping strategy to categorize optional covered benefits, in addition to podiatry, where Medicaid coverage differs from state to state. Our example can assist researchers and policy makers in tracking the impact of policy changes that could affect access to services for Medicaid beneficiaries.
Limitations
Our study had several limitations. First, our data did not contain information on individual managed care organization (MCO) plan coverage for podiatric services. According to the Kaiser Family Foundation Medicaid managed care state-level data, 290 MCOs existed in 39 states in 2018 (including the District of Columbia). 22 These plans cover an estimated 54 million Medicaid beneficiaries, representing approximately 69% of that beneficiary population. 23 Medicaid MCOs consist of private for-profit plans, private nonprofit plans, and various government plans, which vary greatly within states and across the nation. The process of developing MCO contracts is driven by federal policy and the Medicaid policy of each state. 24 Therefore, examining podiatric coverage at the state level, rather than per individual MCO, was more consistent and reliable. The decision was made early in the project-scoping process that including information on MCO plans would not be feasible given time and staffing constraints. We chose to focus instead on mandatory provisions outlined in statutes and regulations. In a brief review of selected MCO plans, we did find situations in which benefits exceeded state minima. For example, an MCO in Virginia provides added benefits that it describes as “extra benefits and services not generally covered through Medicaid.” 25 Routine foot care for diabetic patients is one such benefit. Given the prevalence of MCOs, future research focusing on detailed analysis of state coverage should include information on MCO coverage.
Second, although the variability in Medicaid programs can be a strength, it does complicate the task of systematically collecting these data. The state-level differences go beyond merely variability in coverage. No systematic statutory or regulatory structure exists for how states authorize and define their Medicaid programs. Some states choose to reserve much of the task of defining coverage to legislative prerogative through statutes. Other states give Medicaid agencies broader discretion to define the plan through regulations. A handful of states (eg, Georgia, Michigan, Nevada, South Carolina, West Virginia) take a less centralized approach and spread out plan details in health care provider manuals, agency websites, and fee schedules. We also encountered situations in which information conflicted between sources. In those instances, investigators reached out directly to state officials for clarification. In one instance, a new regulation conflicted with the existing authorizing statute. When contacted, the Medicaid official acknowledged the error and stated the need to prompt the legislature to amend the statute.
Finally, given the variability in policies from state to state, we may have missed or recorded details incorrectly. The potential for miscoding was particularly acute when recording a negative finding (eg, cases in which we coded a particular service as not covered). It is difficult to prove a negative, especially with such disparate sources. Every effort was made to limit mistakes by careful documentation, outreach to state officials, exhaustive research, and double coding by researchers.
Conclusion
Despite these limitations, our data represent the most comprehensive compilation of information on the topic. Thanks to the Centers for Medicare & Medicaid Services state plan amendment filing and approval process, and the relative ease with which new entries can be identified, keeping the data up to date should be possible into the foreseeable future. The process of collecting the data also highlighted avenues for future research. For example, services included in the definition of “routine foot care” vary widely from state to state. These differences highlight important variability in how states provide preventive services for patients with chronic conditions that can be mitigated through podiatric coverage. It is hoped that these data will serve as a valuable resource for researchers in the clinical, policy, and economic fields as they attempt to balance the competing demands of Medicaid policy.
Footnotes
Acknowledgements
The authors thank Nina Patterson, BSPH, for research assistance in the preliminary stages of the project. Ms Patterson was an undergraduate in the College of Public Health at Kent State University at the time of her contribution.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Podiatry Foundation. The Podiatry Foundation played no role in the design or conduct of the study; the collection, management, analysis, or interpretation of the data; the preparation, review, or approval of the article; or the decision to submit the article for publication.