
Abstract
When the COVID-19 pandemic hit the United States, the number of people confined in correctional facilities on a single day numbered 1.8 million. Incarcerated people are at an increased risk of contracting and spreading SARS-CoV-2. Recommendations from the Centers for Disease Control and Prevention on case recognition, management, isolation, and contact tracing are particularly challenging in jails because of the high turnover of incarcerated people. Beginning in late February 2020, the Department of Correctional Health Services in the Los Angeles County Jail system implemented a multipronged COVID-19 mitigation plan that was progressively amended in accordance with local and national recommendations. This plan entailed the creation of housing for people under investigation, SARS-CoV-2 screening upon entry, a mass-testing program, and identification and monitoring of medically vulnerable people. After the identification of the first laboratory-confirmed case on March 29, 2020, predictive models were generated to visualize potential disease spread and gain support for mitigation strategy planning, which forecasted approximately 3300-4600 cumulative cases during a 278-day period. From March 7 through December 31, 2020, the percentage positivity among unique people tested for SARS-CoV-2 was 11.6% (3933 of 33 921 tested). Among those screened at intake, the percentage positivity was 2.0% (502 of 25 702 tested). The ethnic distribution among people with a positive SARS-CoV-2 test result was largely representative of the overall jail population, and most people were asymptomatic. A sustainable, multifaceted mitigation plan that relies on collaboration among medical, custodial, and local public health personnel is essential for limiting the spread of SARS-CoV-2 infection in correctional facilities.
The COVID-19 pandemic presents unique challenges for correctional health care providers and the patients they serve. 1 Jails, in contrast to prisons, face additional issues because of the transient nature of their populations. Jails have a daily turnover that is similar to that of a revolving door, which makes efforts to control the spread of SARS-CoV-2 challenging; new people are constantly added to the pool of potential COVID-19 patients while others are released into the community.2-4 The movement of incarcerated people inside, within, and outside the jail also presents inevitable delays and barriers to communicable disease testing, disease disclosure, follow-up, and education, all of which impact overall disease surveillance.
In addition to the constantly fluctuating census, both the jail population and the setting itself have multiple risk factors. 4 Incarcerated people tend to be disproportionately affected by both chronic and communicable diseases, which are further exacerbated by conditions such as overcrowding, dormitory housing, poor ventilation, and a lack of resources for proper hygiene.3,5,6 The Centers for Disease Control and Prevention (CDC) and Morbidity and Mortality Weekly Report provide guidance on COVID-19 in correctional settings,7,8 but it is essential for institutions to use these recommendations to create their own novel preparedness plans and mitigation strategies that are tailored to the feasibility and conditions of their facilities.
Purpose
In late February 2020, the Los Angeles County Jail (LACJ), the largest jail system in the United States, began preparing for the COVID-19 pandemic. The jail instituted an official plan to combat the spread of the virus, support patients diagnosed with COVID-19, and prevent the spread to the most medically vulnerable populations. The highlights of the plan were consistent with CDC recommendations. 7 We report on the use of these mitigation strategies and the cumulative incidence of COVID-19 in this jail system.
Methods
The LACJ has approximately 115 000 bookings per year and an average daily census of approximately 17 500 people spread across 6 facilities: Men’s Central Jail, Inmate Reception Center, Twin Towers Correctional Facility, Century Regional Detention facility, Pitchess Detention Center, and the Correctional Treatment Center, which functions as a skilled nursing facility. The Inmate Reception Center serves as the entry/processing point for men. Men are housed in Men’s Central Jail, Twin Towers Correctional Facility, and Pitchess Detention Center. All women are processed and most women are housed at Century Regional Detention facility. Both men and women are housed at the Correctional Treatment Center. Health care is provided by Correctional Health Services (CHS), a department within the larger Los Angeles County Department of Health Services (DHS). Compared with Los Angeles County, people who are African American, Latino, male, and unhoused are overrepresented in the LACJ population.
In late February 2020, CHS worked with the Los Angeles County Sheriff’s Department (LASD), the Los Angeles County Department of Public Health (LACDPH), and DHS infection control specialists to create a mitigation plan detailing several proactive steps that attempted to slow the introduction and control the spread of SARS-CoV-2 in the jail population.
Mitigation Plan
The mitigation plan included the following: prescreening arrestees for COVID-19–associated symptoms (eg, fever, cough, other upper respiratory infection [URI] symptoms); universal wearing of face masks by both staff members and incarcerated people and temperature screening of employees before entering the facility; isolating people suspected to have COVID-19 using CDC guidance, which was adjusted accordingly for changes in criteria; monitoring the electronic health record (EHR) for elevated temperatures; isolating and/or housing together people with laboratory-confirmed COVID-19; implementing a rigorous quarantine strategy for housing modules and subpopulations that contained persons under investigation (PUIs) and/or people with confirmed COVID-19; identifying and monitoring people with an elevated risk for poor outcomes from COVID-19 8 ; assigning consistent work locations for staff members and detainee workers; decreasing patient movement by restructuring clinic visits and placing medical holds on PUIs and people with confirmed COVID-19 to prevent infection transmission; maintaining an up-to-date surveillance system to capture all SARS-CoV-2 test results and housing locations; and discontinuing all continuous positive airway pressure therapy and routine handheld nebulizer treatments, 9 with people requiring continuous positive airway pressure therapy or handheld nebulizer treatments moved to a negative pressure isolation room.
Beginning on March 7, 2020, CHS began to monitor incarcerated people upon entry for symptoms associated with COVID-19. All incarcerated people were also educated on COVID-19 by medical personnel and told to report any symptoms. PUIs were tested and isolated, and if they came from dormitory housing, their original housing unit was placed on quarantine for ≥14 days. An additional 14 days of quarantine was added for each person who had a positive test result in the same unit. Quarantined housing modules were regularly monitored for additional people displaying URI-like symptoms. When identified, these people were designated as PUIs, transferred to PUI housing, and tested for SARS-CoV-2. All people housed in quarantined dormitories were also monitored with twice-daily temperature, heart rate, and pulse oximeter screenings. People who had shortness of breath and pulse oximeter readings <94% were transferred to a hospital as emergency referrals, with oxygen orders entered upon return if needed. People who were isolated with confirmed SARS-CoV-2 infection were cleared from PUI/medical isolation housing using CDC guidelines on discontinuing home isolation for people with COVID-19. 10 Nasopharyngeal swab specimens were collected and analyzed for the presence of SARS-CoV-2 RNA using reverse transcription polymerase chain reaction tests. All specimens were processed by externally contracted laboratories.
As testing capacity increased, all people arriving at the Inmate Reception Center were screened beginning March 5, 2020, and mass screening upon entry to Century Regional Detention facility was implemented on May 8, 2020. Mass testing of all asymptomatic people began on May 11, 2020, and lasted until July 7, 2020. Concerns about delayed results from conventional assays and their impact on disease control efforts led to the use of vetted rapid testing algorithms from laboratories contracted by the larger Los Angeles County DHS. When mass testing concluded, EHR data were used to designate and track all incarcerated people with health conditions that put them at elevated risk for poor outcomes from COVID-19. 8 Once identified, these designated medically vulnerable patients had weekly wellness checks, which entailed assessments of COVID-19–associated symptoms and the offer of COVID-19 testing. Furthermore, people were transferred to PUI housing if determined to be a PUI. All releasees (PUIs, people with positive SARS-CoV-2 test results, people with negative SARS-CoV-2 test results, untested people) were discharged with face masks and counseled on COVID-19 symptoms, prevention, isolation, and quarantine upon their return to the community. Isolation was emphasized to people who were released after diagnosis and PUIs who were released before receiving SARS-CoV-2 test results. Contact information for releasees from quarantined areas who were not tested were provided to LACDPH. In addition, a comprehensive list of all swab results, including people who had a positive test result and were released and people who were released before receiving their results (in addition to contact information when available), were provided to LACDPH daily.
A COVID-19 surveillance system was developed by extracting data on swab results from the EHR into a shared file that was updated daily and made available to medical and nursing administration. The number of unique people tested for SARS-CoV-2 was determined by only accounting for the first positive test result among those who had a positive test result (negative results obtained before a positive test were excluded) and only accounting once for those who had a negative test result and remained negative throughout the study period. All laboratory results and demographic data were obtained from the EHR. Multivariate logistic regression analysis was used to estimate odds ratios (ORs) and 95% CIs for associations between SARS-CoV-2 infection as a binary dependent variable (yes/no) and age (18-24, 25-34, 35-44, 45-54, ≥65 years), race and ethnicity (non-Hispanic Black, non-Hispanic White, Hispanic, Other [includes American Indian/Alaska Native, Chinese, Japanese, Filipino, all others, and Native Hawaiian/Other Pacific Islander]), and sex (male, female) for all people tested and those tested upon entry, with significance defined as P < .05. Study approval was obtained from the Los Angeles County Public Health, Ambulatory Care Network, and Health Services Administration Institutional Review Board.
Predictive Data Modeling
Given the initially limited testing capabilities and, therefore, low number of people with confirmed COVID-19, presenting a visualization of the potential spread of SARS-CoV-2 in the jail population to medical and custodial leadership was essential in gaining support for mitigation strategy planning. Two methods were used to create data simulations. The first was a susceptible–infected–recovered model adapted from an application for modeling epidemics. 11 The model limitations were noted, as the model did not account for mitigation measures and assumed a closed population, meaning it would be biased toward fewer cases and could not be used to assess effects of mitigation efforts. Because of daily jail census fluctuations, several model iterations were generated using a range of R0 and daily jail census values and compared with our case data. Values that demonstrated congruency with the existing data (model assumptions: R0 ~ 2.8; infectious period = 10 days; N = 17 000, 15 000, and 12 000) were then used to predict maximum case numbers during a forecasted period from March 29 through December 31, 2020. The number of predicted cases, actual cases, and the daily jail census were all used as parameters to generate predictive cumulative incidence curves during the same period of 278 days. 12 We used the mean absolute error (MAE) to measure the accuracy of each predictive model.
Outcomes
On March 7, 2020, LACJ began testing people for SARS-CoV-2, and the first positive test result was received on March 29, 2020. Case numbers peaked toward the end of May 2020 after implementation of asymptomatic mass testing (Figure). As of December 31, 2020, a total of 33 921 unique people had been tested for SARS-CoV-2, of whom 3933 (11.6%) had a positive test result (Table 1). Among those tested both overall and upon entry, most people were Hispanic and aged 25-34 years. We found similar proportional groupings among people who received a positive test result. Of 3933 people who received a positive test result, 131 (3.3%) had oxygen orders and 563 (14.3%) had emergency referrals. Of 25 702 people screened upon entry, 502 (2.0%) had a positive test result.
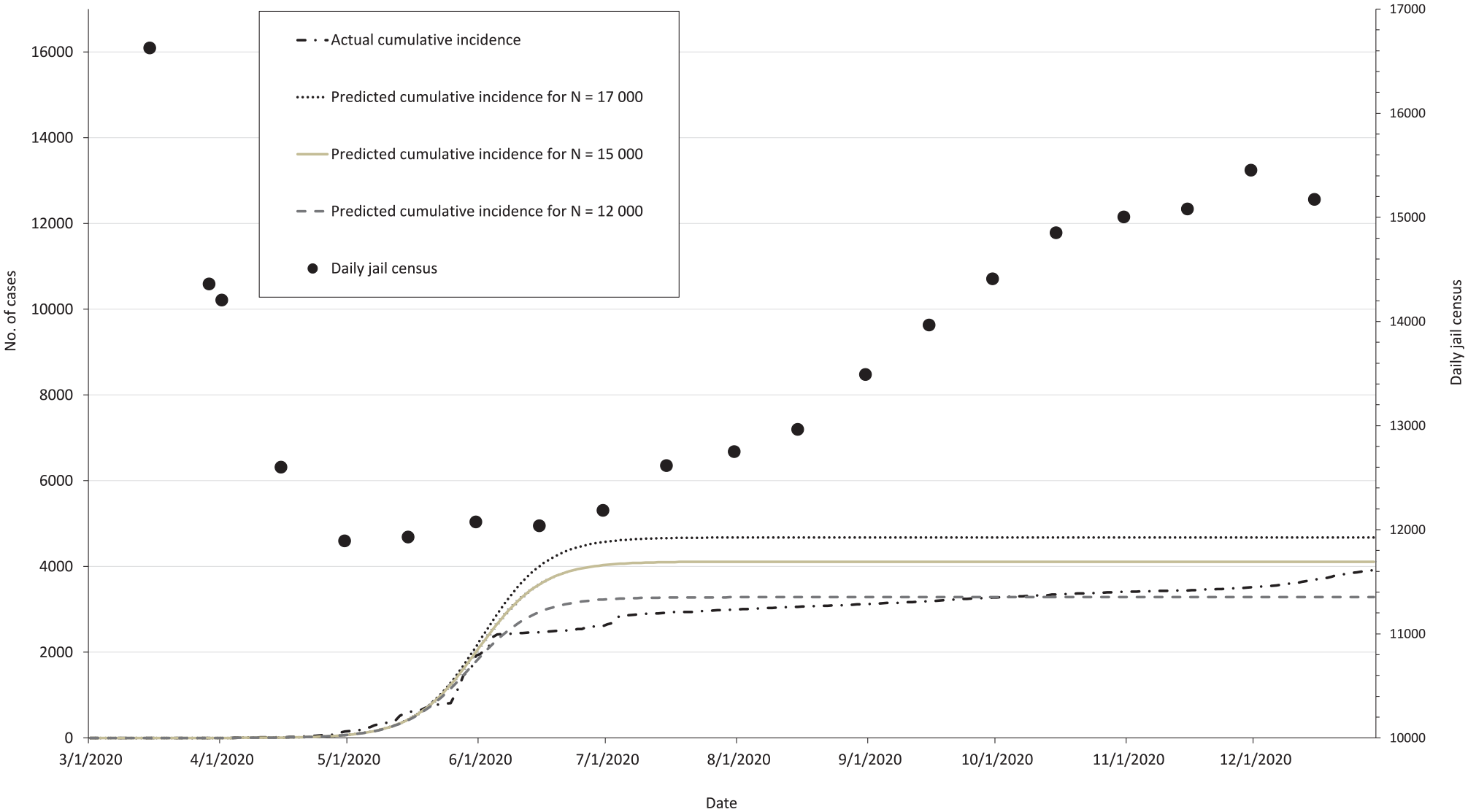
Actual and predicted cumulative COVID-19 cases and change in daily census at the Los Angeles County Jail, March 29 through December 31, 2020, for N = 17 000 (mean absolute error [MAE] = 1088.9), N = 15 000 (MAE = 671.4), and N = 12 000 (MAE = 206.5).
Characteristics of people who were tested (March 7 through December 31, 2020) and tested upon entry (May 5 through December 31, 2020) for SARS-CoV-2, Los Angeles County Jail a
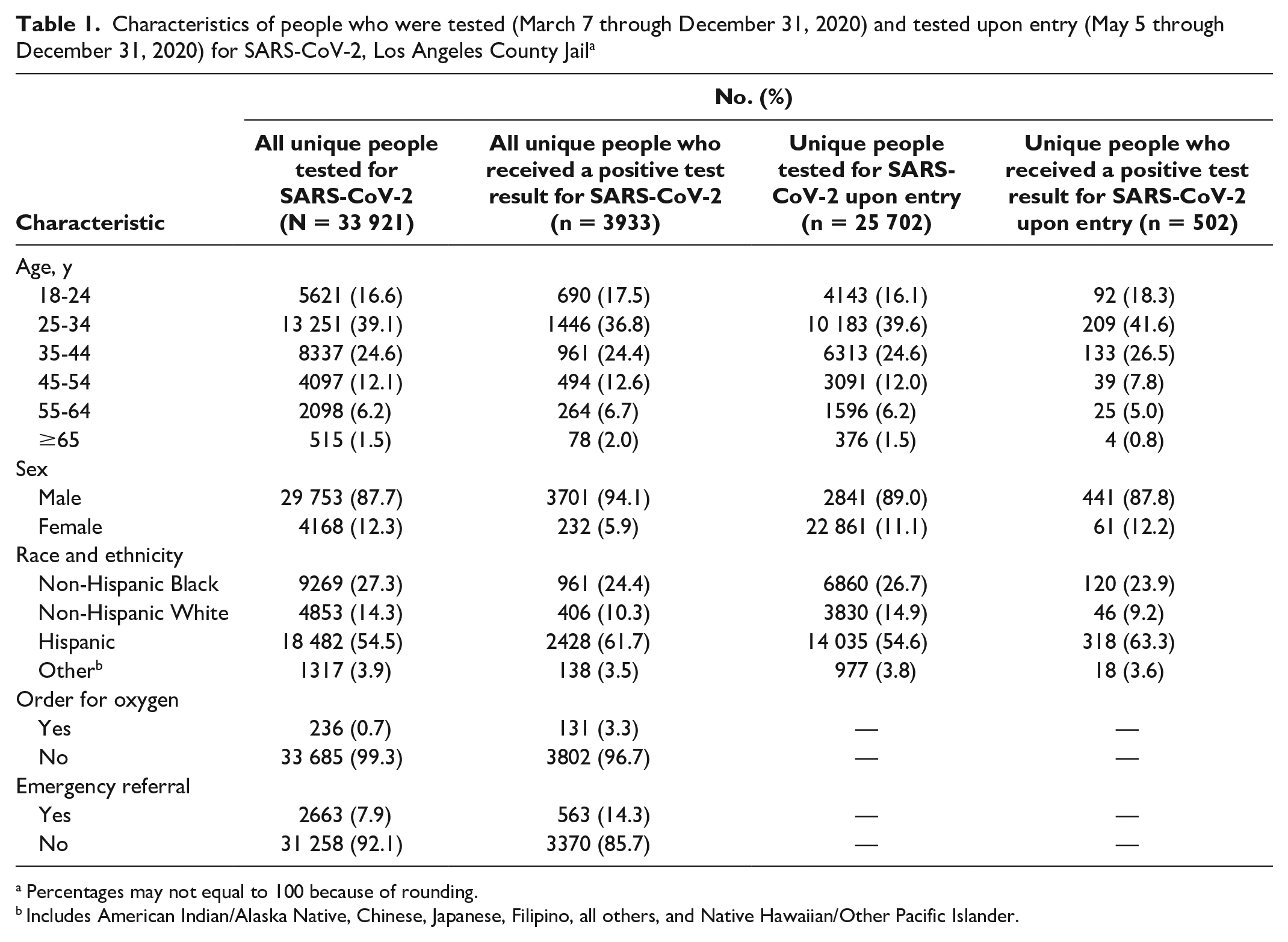
Percentages may not equal to 100 because of rounding.
Includes American Indian/Alaska Native, Chinese, Japanese, Filipino, all others, and Native Hawaiian/Other Pacific Islander.
The multivariate logistic regression model demonstrated that SARS-CoV-2 positivity was significantly associated with being Hispanic, non-Hispanic Black, Other, male, and aged ≥65 years for all people tested, and being Hispanic or non-Hispanic Black for people tested upon entry (Table 2). From March 7 through December 31, 2020, eleven COVID-19–related deaths were noted. Weekly lists generated of medically vulnerable patients after mass testing concluded demonstrated that approximately 3%-4% of the total jail population was consistently classified as medically vulnerable, 15% of whom had ever had a positive test result for SARS-CoV-2, with approximately 6% who were tested through follow-up.
Results of multivariate logistic regression analysis of SARS-CoV-2 positivity among all incarcerated people tested (March 7 through December 31, 2020) and screened upon entry (March 5 through December 30, 2020), Los Angeles County Jail
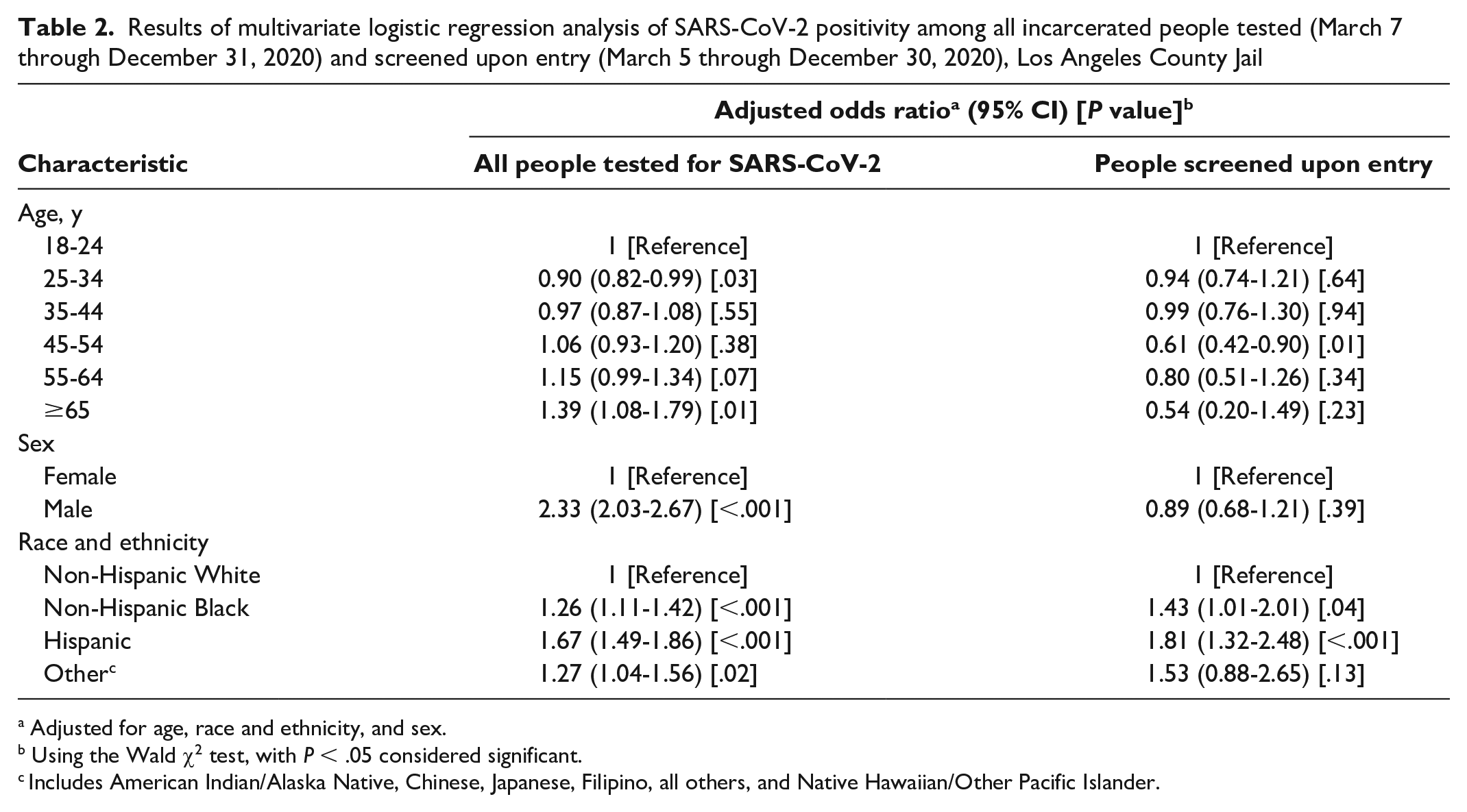
Adjusted for age, race and ethnicity, and sex.
Using the Wald χ2 test, with P < .05 considered significant.
Includes American Indian/Alaska Native, Chinese, Japanese, Filipino, all others, and Native Hawaiian/Other Pacific Islander.
Predictive Model Outcomes
The susceptible–infected–recovered model had predicted that in a population of approximately 17 000 people, an estimated 4672 (27.1%) would become infected by the end of the forecasted period. For the reduced populations of 15 000 and 12 000 people, an approximated 4112 (27.3%) and 3283 (27.5%) cases, respectively, were predicted. These numbers were used to fit 3 cumulative incidence curves, and the accuracy of the predictive values was measured using MAE. The MAE values of the predictive curves were 1088.9 (N =17 000), 671.4 (N = 15 000), and 206.5 (N = 12 000) (Figure).
Lessons Learned
The primary goal of CHS was to protect medically vulnerable patients by trying to slow the introduction of SARS-CoV-2 into the facilities, as it was assumed that the COVID-19 trends in Los Angeles County would likely be reflected in the jail population, both due to the instability of the population itself and exposure from custodial and medical staff members. This assumption proved true, as an increase in the number of cases observed at LACJ from May to July 2020 and in mid-November 2020 mirrored the case curve in Los Angeles County. 13 Our predictive models, although limited, forecasted visuals of potential cumulative incidence of disease and helped justify the need for multifaceted mitigation efforts when information was initially scarce. It was understood that preventing the spread of SARS-CoV-2 would be difficult given the inherent challenges of communal housing, the revolving door of incarcerations and releases, and the necessary movement of people to and from court and other facilities; therefore, realistic decisions had to be made about the implementation of feasible infection control and mitigation efforts.
Routine temperature screening and required facial coverings for CHS and LASD employees served as early employee-wide efforts to help reduce the introduction and transmission of SARS-CoV-2. A census decrease from 17 200 to 11 800 by late April 2020 initiated by LASD and the court system, however, had a major impact, because it reduced the amount of people at risk for infection. A joint LASD/CHS prescreening procedure was implemented to decrease COVID-19 exposure from the community by requiring the completion of a prescreening form by all arresting agencies prior to any booking. Arrestees exhibiting any COVID-19–related symptoms were isolated prior to entry and sent via a secure entrance to a designated isolation location within the respective facilities. Over time, additional PUI housing locations were created, because the original locations could no longer accommodate the number of PUIs. Several dormitory settings were also reserved for patients with confirmed COVID-19.
It was noted early on that the presenting signs and symptoms of COVID-19 originally described (e.g., fever ≥100.4 °F, URI symptoms, dry cough) were too narrow to properly identify the PUI population in the jail setting.14,15 Health care providers in charge of medical screening and individual clinical settings at the Inmate Reception Center were therefore instructed to liberalize criteria for PUI designation, particularly with increased testing capacity. EHR surveillance allowed for early identification of potential PUIs by screening for documented temperatures ≥100.0 °F and by identifying medically vulnerable patients. The greatest proportion of the total COVID-19 cases was identified though the mass screening, which coincided with a case surge in Los Angeles County, 15 but it became unsustainable because of shortages in both staff members and space. In contrast, only 2% of incoming arrestees screened upon entry had a positive test result for SARS-CoV-2. Most people who received a positive test result for SARS-CoV-2 were asymptomatic or mildly symptomatic and did not require emergency referrals or oxygen orders. Although our data are not conclusive, they imply the possibility of disease transmission via both mildly symptomatic and asymptomatic people, for which evidence has been demonstrated previously.16,17
It has also been suggested that COVID-19 disproportionately affects certain racial and ethnic minority populations, with proposed associations including genetic predisposition, pathophysiologic factors, a high rate of underlying medical conditions such as cardiovascular disease or diabetes, and cultural and socioeconomic factors. 18 Survey data obtained from jails, prisons, and juvenile detention centers across the United States also noted higher incidence rates of people receiving a positive test result for SARS-CoV-2 and PUIs among African American people compared with White people. 19 Both the overall and entry screening data from LACJ demonstrated higher odds of infection among non-Hispanic Black and Hispanic people than among non-Hispanic White people, with Hispanic ethnicity being most strongly associated with SARS-CoV-2 positivity. This observation seems to be representative of the overall LACJ population, of which the highest proportion are Hispanic and non-Hispanic Black, respectively. It may also reflect that all people in the correctional setting are generally medically and socioeconomically underserved, have a high proportion of comorbidities, and receive equitable health care while incarcerated.
Lastly, although jails are often categorized as congregate housing locations and are pooled with juvenile custodial settings, prisons, and skilled nursing facilities in the context of infection control guidelines, the risk-reducing strategies aimed toward these populations are not necessarily generalizable to jails. 20 The daily turnover of people being incarcerated and discharged is uniquely challenging to jails. 3 Despite the decarceration effort in April 2020, the census had increased to 15 000 by late October 2020 and remained at approximately that number. Mass testing, which was sustainable for a brief period, required a tremendous amount of coordination from understaffed medical, infection control, and custodial personnel; adequate procurement and provision of personal protective equipment; and an effective surveillance system to capture and disseminate results. In addition, people were periodically released before or shortly after their results were available or discharged before being tested, which created challenges for adequate disease disclosure, education opportunities, and surveillance. The daily census changes also resulted in 100 to 150 people consistently being both added to and removed from the weekly list of medically vulnerable patients, fragmenting the follow-up process.
Despite these challenges, the most sustainable and consistently implemented mitigation efforts were orders to wear face masks, PUI designation and housing creation, intake screening, monitoring of quarantined dormitories, and identification and monitoring of medically vulnerable patients. Other jails may benefit from adapting similar efforts in accordance with their own feasibility and resources. A key lesson from this experience was the impact of using EHR data both for COVID-19 surveillance and monitoring medically vulnerable patients. Investing in technology to automate laboratory data, track patient movement, and create registries based on medical designations can facilitate communicable disease surveillance in the correctional setting, and this will likely be a future undertaking for CHS.
Disease modeling is also a beneficial tool that has been underused in the correctional setting in comparison with hospital and other non–correctional health care settings, especially given the disproportionate prevalence of communicable disease among incarcerated people. 5 Although our limited data models were not intended to assess the effects of mitigation, they helped predict the caseload trajectory, and the predictive curve with a jail census of 12 000 had the lowest MAE value among the 3 predictive curves, indicating that it was the closest predictor of the actual data. Other jails would benefit by securing resources to develop predictive modeling accounting for the open population to produce more accurate estimates of cumulative incidence of disease.
The COVID-19 pandemic is ongoing, and case numbers will increase until enough people become vaccinated. Vaccination of medically vulnerable people at LACJ began in late January 2021 and expanded to all incarcerated people in accordance with local public health guidance. The COVID-19 mortality rate will continue to place this population at risk, requiring expanded vaccination efforts, consistent monitoring and surveillance, and continued vigilance and cooperation with local hospitals and public health agencies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.