
Abstract
Objectives:
Nearly 1 in 3 people with hepatitis C virus (HCV) infection pass through the criminal justice system annually; the system is a crucial location for HCV screening, education, and linkage to care. We aimed to (1) determine the prevalence and incidence of HCV antibody positivity and (2) evaluate the demographic characteristics of people with HCV in a large urban jail.
Methods:
We offered universal opt-out HCV testing to any person undergoing a routine blood test at the Dallas County Jail from June 2015 through December 2019 (N = 14 490). We extracted data on demographic characteristics from the electronic medical record and collected data on risk factors from people with HCV antibody positivity. We performed univariate and multivariate analyses.
Results:
The prevalence of HCV antibody positivity was 16.7%; the incidence was 13.5 cases per 1000 person-years. HCV antibody positivity was significantly associated with older age (P < .001), female sex (P = .004), non-Hispanic White race versus non-Hispanic Black race (P < .001), and being released to prison versus not (P < .001). Among people born after 1965, those who were HCV antibody–positive were more frequently non-Hispanic White and Hispanic women, whereas among those born in 1965 or before, those who were HCV antibody–positive were more frequently non-Hispanic Black men.
Conclusions:
The high prevalence and incidence of HCV antibody positivity in a large county jail argue for routine, universal HCV testing and prevention counseling in criminal justice settings. Changing demographic characteristics mirror those of the national injection drug use epidemic and shed insight into designing interventions for risk reduction, education, linkage to care, and treatment.
Keywords
Nearly 2.4 million people in the United States have hepatitis C virus (HCV) infection, the leading cause of infection-related mortality in the country.1,2 Without treatment, HCV can lead to cirrhosis and hepatocellular carcinoma, contributing to morbidity and mortality and increased health care utilization.2,3 Treatment for HCV infection is highly effective, requires 8 to 12 weeks to complete, and can prevent HCV-associated morbidity and mortality. 4 People living with HCV infection are disproportionately affected by social determinants of health such as poverty, low educational attainment, systemic racism, lack of social support, and substance use. 5 These health inequities contribute to multiple barriers to diagnosis: half of people living with HCV infection may be unaware of their diagnosis.1,6 Once diagnosed, people living with HCV infection face numerous barriers to treatment, including access to care, societal stigma, and financial burden, and often injection drug use (IDU), the most common risk factor for HCV.7,8
Eradicating HCV requires identifying populations at high risk of acquiring HCV and populations with a high prevalence of HCV infection. Compared with the general population, people involved in the criminal justice system are more commonly infected with HCV because of such risk factors as IDU, mental health issues, poverty, and stigma. Nearly 1 in 3 people living with HCV infection passantibody–positive, the average age through the criminal justice system each year; people who are incarcerated are 9 times more likely than the general population to be living with HCV infection.1,9,10 Although several studies demonstrated successful HCV testing and a high HCV antibody prevalence in the criminal justice system,1,11-20 including studies from our own institution,21,22 limited data exist about the incidence of HCV in criminal justice settings or which demographic subgroups are at increased risk of HCV infection.
Establishing the epidemiology of HCV provides insights into the burden, ramifications, and transmission of HCV among people involved in the criminal justice system. In this study, we aimed to (1) determine the prevalence and incidence of HCV antibody positivity among people incarcerated at a large urban jail and (2) identify the demographic trends of HCV antibody positivity to inform screening and treatment interventions for populations at risk for HCV.
Methods
Study Setting
The Dallas County Jail serves as a city and county jail; it had an average daily population of 5200 and 66 277 bookings in 2017 (personal communication, Mr. Pat Jones, vice president of correctional health services, Dallas County Jail, October 2020). The jail population is primarily male (78%) and Black (47%); the mean age is 34.9 years. About 10% of people passing through the jail require blood tests for chronic conditions such as diabetes, HIV, hypertension, or mental health conditions.
Study Population and Data Collection
We conducted a retrospective analysis of opt-out HCV testing in 4 discrete testing cycles from June 2015 through December 2019 (N = 14 490). The testing cycles were June 2015–July 2016, April–November 2017, January 2018–January 2019, and April–December 2019. In June–November 2015, we offered opt-out HCV testing at intake, and 13% to 30% of people accepted testing. In November 2015, we converted to opt-out testing during any routine blood test, and >80% of people accepted testing. In April 2017, we added confirmatory reflex HCV RNA testing to measure the presence of active HCV infection. We removed all duplicate HCV antibody tests (n = 1234) during the same jail stay and testing year (Figure 1). We kept duplicate tests on the same people between testing years because these people may have had repeat incarcerations and ongoing potential HCV exposures, thus providing an opportunity to examine incidence of HCV infection. Our nurse navigator educated people who were HCV antibody–positive, surveyed them for HCV risk factors, and contacted them upon release to link to HCV care. The University of Texas Southwestern Medical Center Institutional Review Board considered this study exempt because of implementation of guideline-recommended practice (HCV testing in criminal justice facilities).
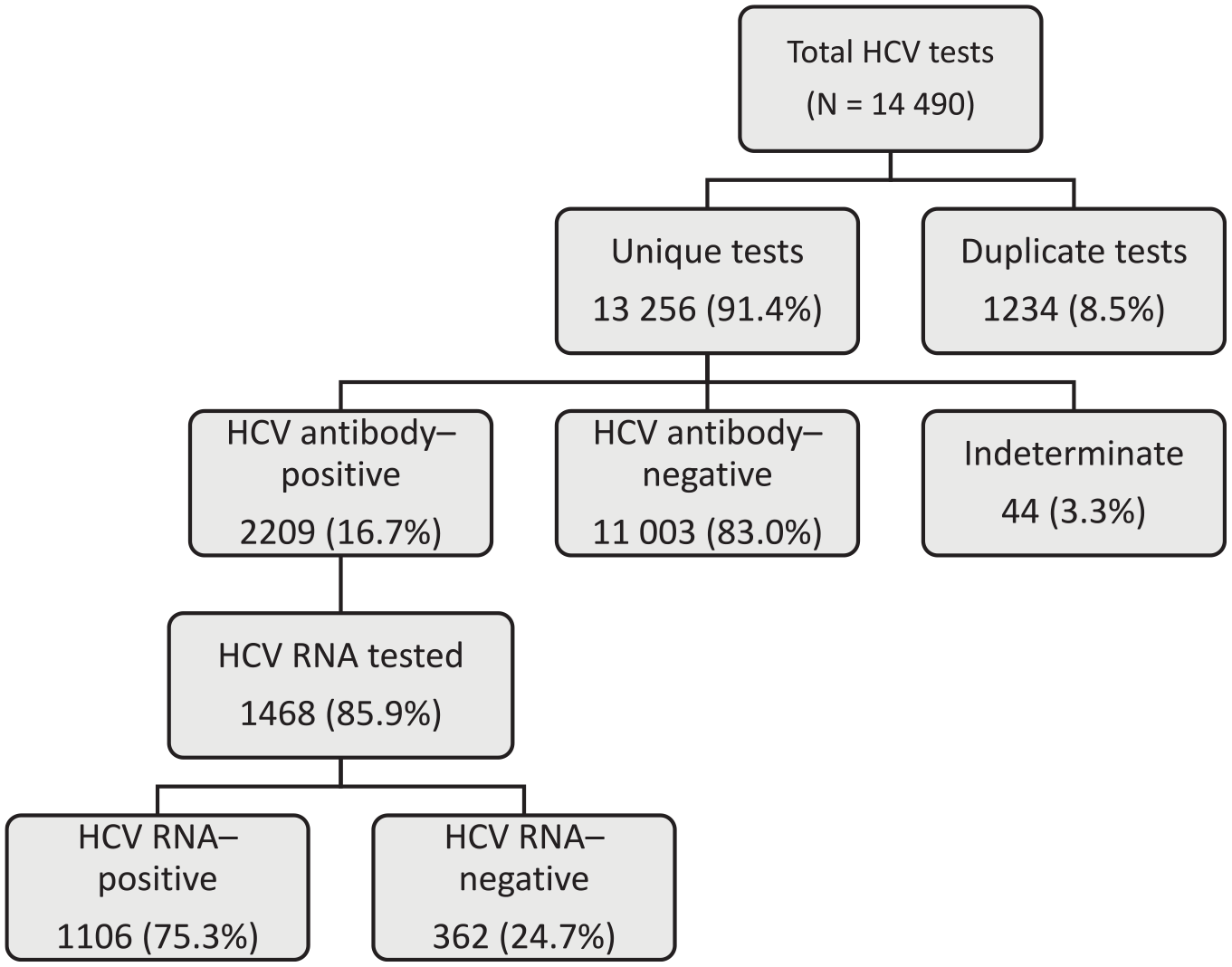
Hepatitis C virus (HCV) antibody and HCV RNA positivity among people screened for HCV in the Dallas County Jail from 2015 to 2019 (N = 14 490). From 2017 to 2019, reflex HCV RNA testing was incorporated into HCV testing. Data were collected by the authors from electronic medical records and release records.
Measures
We extracted data on demographic characteristics, including age, year of birth, sex, and self-identified race and ethnicity (non-Hispanic Black, Hispanic, “other” [includes Asian, American Indian, Pacific Islander, mixed race, or race not specified], and non-Hispanic White), months in jail, and release location (eg, released to prison vs not [ie, released to community or community-based program]) from electronic medical records and release records. We defined birth cohort as anyone born during 1945-1965. A nurse navigator collected data on risk factors (IDU, transfusion history, sexual contact, tattoos) and pre-incarceration health insurance status (Parkland financial assistance, government funded [Veterans Affairs, Medicare, or Medicaid], private, or none) from people who received a positive HCV antibody test result in 2017.
For HCV testing, we used HCV antibody enzyme immunoassay (F. Hoffmann–La Roche Ltd) and HCV RNA Cobas AmpliPrep/Cobas TaqMan HCV Test version 2.0 (F. Hoffmann–La Roche Ltd). We defined a positive HCV antibody test result as >0.9 signal-to-cutoff ratio and a positive HCV RNA (HCV viremia) as any detectable RNA (>15 IU/mL). We defined the prevalence of HCV infection as the number of positive HCV antibody test results divided by the number of total tests; we then multiplied this number by the proportion of positive RNA test results. To calculate HCV incidence (ie, seroconversion), we first identified the number of unique individuals tested during multiple testing cycles (n = 1185). We then determined the number who were originally HCV antibody–negative and became antibody–positive (n = 16) and divided that by the number tested during at least 2 testing cycles. We used testing cycles (every year) to compute the incidence. We used prevalence ratios (defined as the proportion with disease/proportion of the general jail population for each demographic group) to determine how HCV antibody prevalence changed as year of birth progressed by demographic subgroup. We defined demographic groups as non-Hispanic Black (female and male), Hispanic (female and male), and non-Hispanic White (female and male). This process allowed us to graphically depict the increase in prevalence of HCV antibody positivity in certain demographic groups compared with the overall prevalence.
Statistical Analysis
We compared the demographic characteristics of people who had a positive HCV antibody test result and people who had a negative HCV antibody test result (N = 13 212). We excluded from analysis people who had an indeterminate HCV antibody test result or were tested multiple times in 1 year. We also compared people who had positive HCV RNA and positive HCV antibody (ie, HCV viremia) with people who had negative HCV RNA and positive HCV antibody. We performed univariate and multivariate analysis on nearly all variables. Because of incomplete data, we excluded intake data from 2015-2016 and the variable for release location. We analyzed IDU by race and ethnicity and sex. We considered P < .05 to be significant. We performed all analyses using SPSS version 25 (IBM Corporation).
Results
From 2015 through 2019, the prevalence of HCV antibody positivity was 16.7% (2209 of 13 256) among people tested at the Dallas County Jail (Figure 1). Of those eligible for RNA testing, 85.9% (n = 1468) were tested and 3 of 4 people (n = 1106) were HCV RNA–positive. The HCV antibody incidence was 13.5 per 1000 person-years from 2017 through 2019. Of the 16 people who converted from HCV antibody–negative to HCV antibody–positive, the average age was 37.5 years; 13 were men, 6 identified as non-Hispanic Black, 5 identified as Hispanic, and 5 identified as non-Hispanic White.
People who were HCV antibody–positive were more often older (odds ratio [OR] = 1.08 [95% CI, 1.07-1.08]; P < .001), more frequently either non-Hispanic White (OR = 1.88 [95% CI, 1.67-2.11]; P < .001) or Hispanic (OR = 1.32 [95% CI, 1.14-1.52]; P < .001) than non-Hispanic Black, and born during 1945-1965 (OR = 6.47 [95% CI, 5.73-7.33]; P < .001) than after 1965; less likely to be tested in 2018 (OR = 0.85 [95% CI, 0.75-0.95]; P = .005) or 2019 (OR = 0.79 [95% CI, 0.69-0.91]; P = .001) than in 2017; and more likely to be released to prison (OR = 1.43 [95% CI, 1.25-1.63]; P < .001) than those who were HCV antibody–negative (Tables 1 and 2). However, after adjustment for other variables in multivariate analysis, female sex was associated with HCV antibody positivity (adjusted OR = 1.24 [95% CI, 1.08-1.44]; P = .003), and year of test was no longer significantly associated with HCV antibody positivity (Table 2).
Demographic characteristics of people who were HCV antibody–positive (n = 2209) and the total population (N = 13 212) with routine blood tests at the Dallas County Jail, 2015-2019 a
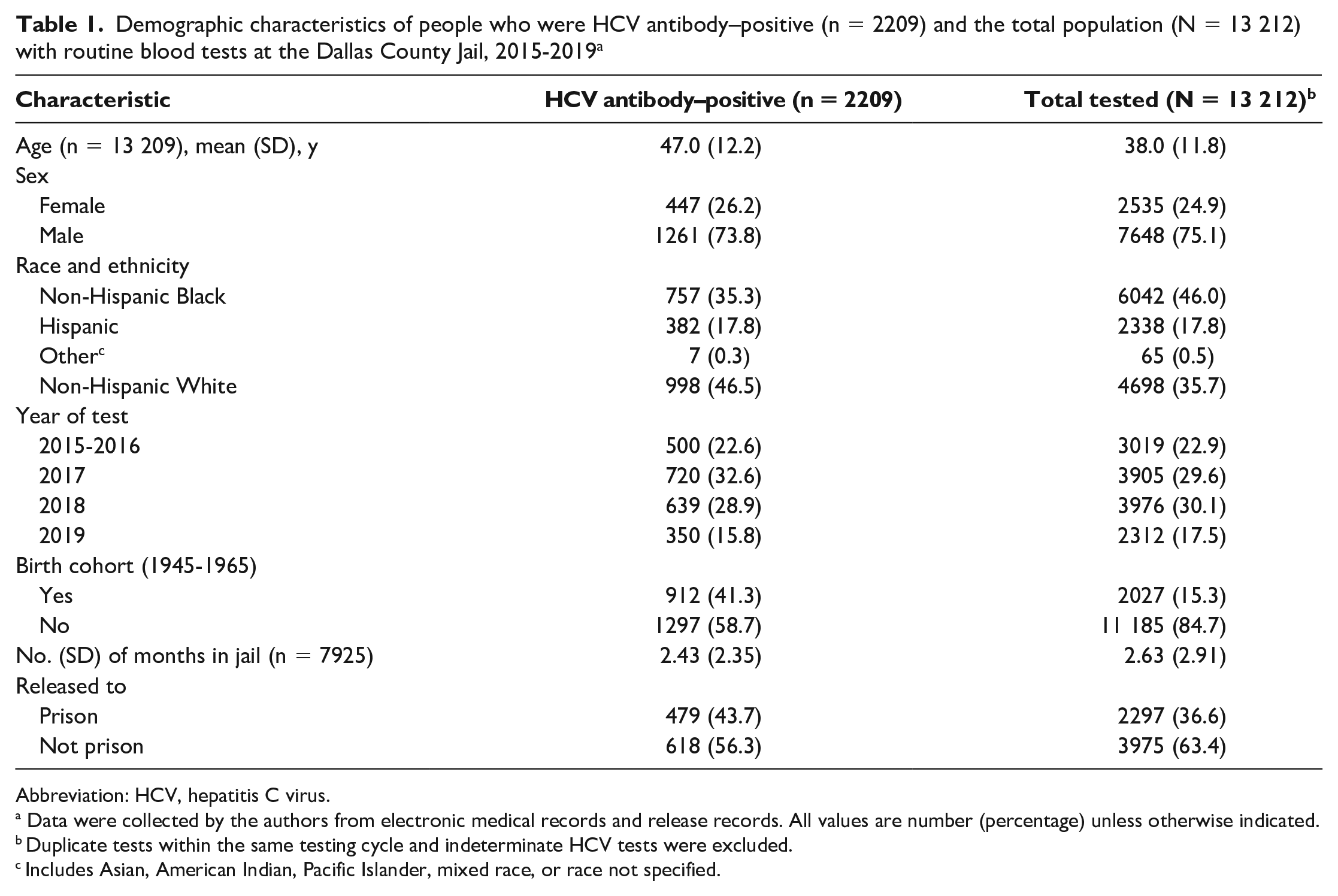
Abbreviation: HCV, hepatitis C virus.
Data were collected by the authors from electronic medical records and release records. All values are number (percentage) unless otherwise indicated.
Duplicate tests within the same testing cycle and indeterminate HCV tests were excluded.
Includes Asian, American Indian, Pacific Islander, mixed race, or race not specified.
Association of demographic characteristics with HCV antibody positivity among people with routine blood tests at the Dallas County Jail, 2015-2019 a
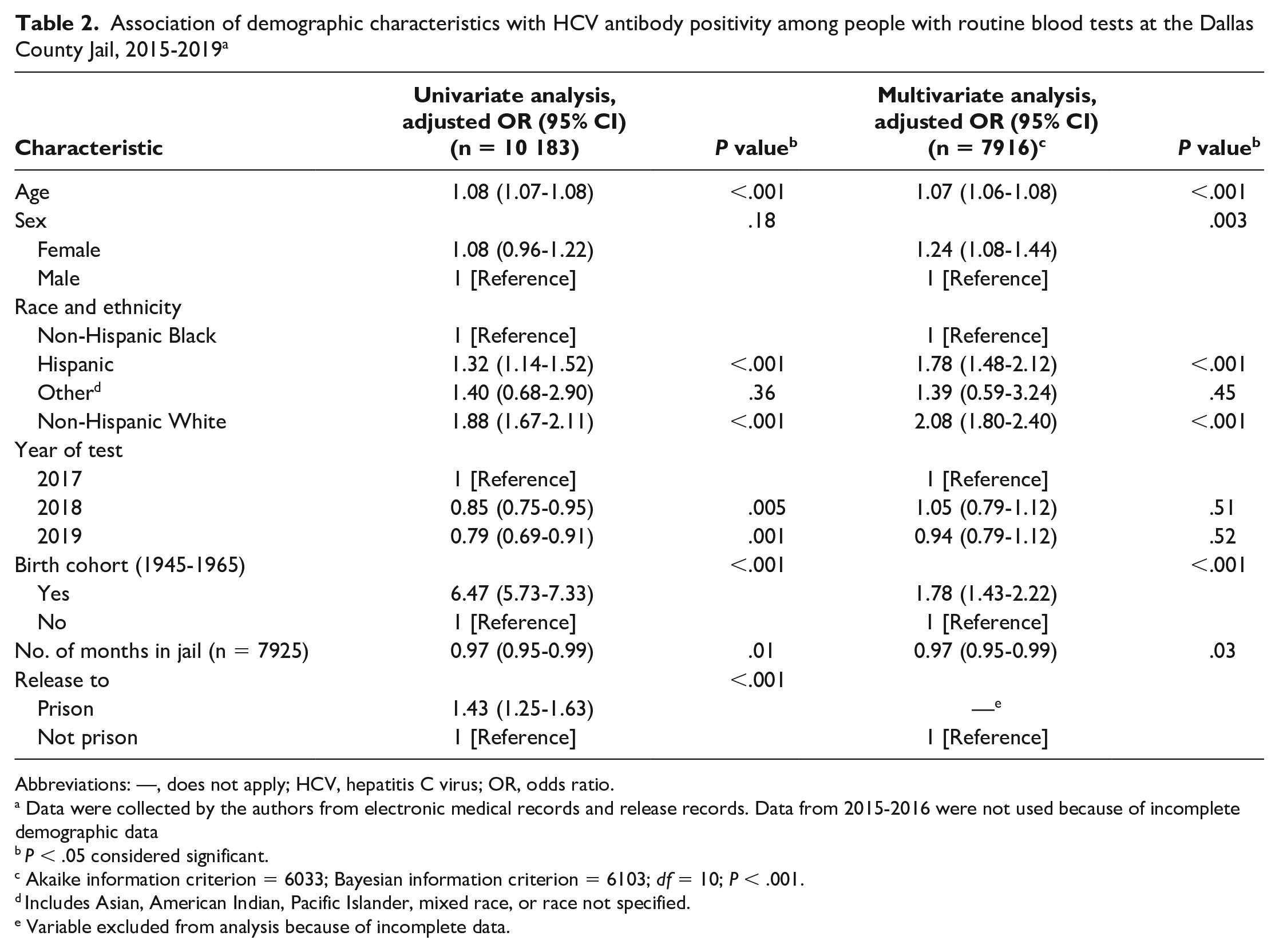
Abbreviations: —, does not apply; HCV, hepatitis C virus; OR, odds ratio.
Data were collected by the authors from electronic medical records and release records. Data from 2015-2016 were not used because of incomplete demographic data
P < .05 considered significant.
Akaike information criterion = 6033; Bayesian information criterion = 6103; df = 10; P < .001.
Includes Asian, American Indian, Pacific Islander, mixed race, or race not specified.
Variable excluded from analysis because of incomplete data.
The multivariate analysis revealed complex relationships between race and ethnicity, sex, year of birth, and HCV antibody status. As year of birth progressed, the prevalence of HCV antibody positivity decreased (Figure 2). The prevalence of HCV antibody positivity ranged from approximately 50% to 70% among people born during 1945-1965 but dropped to <10% among people born in the 1990s. However, more tests were performed among people born after 1965.
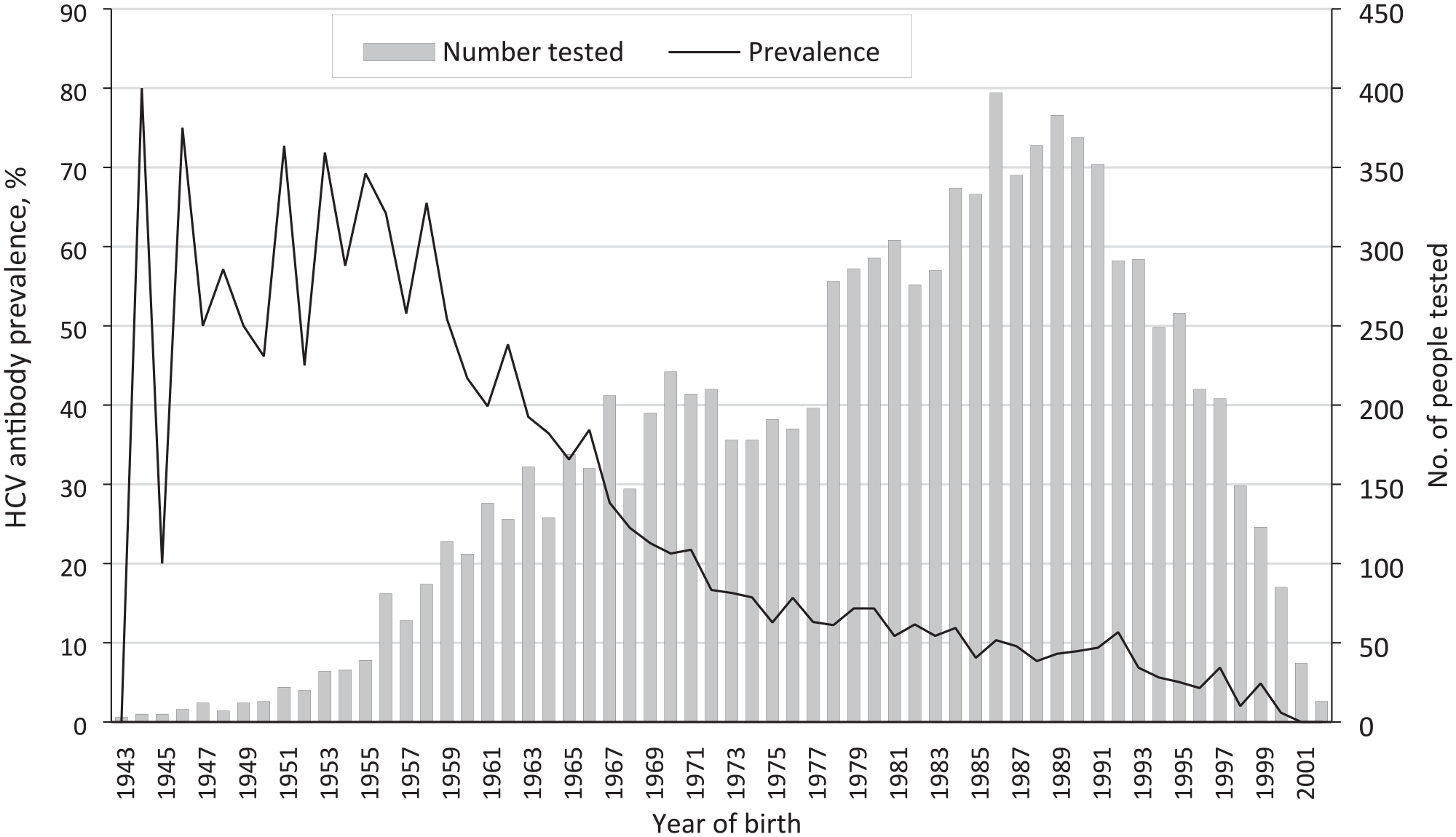
Hepatitis C virus (HCV) antibody prevalence and number of people tested for HCV by birth year among people (n = 10 183) at the Dallas County Jail screened from 2017 to 2019. Data were collected by the authors from electronic medical records and release records.
HCV antibody positivity among non-Hispanic White and Hispanic women was inversely associated with age (Figure 3). Prevalence ratios were 0 for women born in the 1940s and increased to approximately 2 (twice the prevalence of the general jail population) for women born in the 1990s. HCV antibody positivity among non-Hispanic Black men was lower in younger age groups than in older age groups; the prevalence ratio was 1 for non-Hispanic Black men born in the 1940s to approximately 0.5 (half the prevalence of the general jail population) for non-Hispanic Black men born in the 1990s (Figure 3). We found HCV viremia (n = 889) more frequently among men than among women (76.8% vs 69.0%; P = .02) and among non-Hispanic Black people than among non-Black people (83.3% vs 72.0%; P = .003). Among people who were HCV antibody–positive, non-Hispanic White and Hispanic people were more likely than non-Hispanic Black people to report IDU (non-Hispanic White, 62%; Hispanic, 59%; non-Hispanic Black, 44%; P < .001). In addition, women were more likely than men to report IDU (61% vs 51%; P = .03).
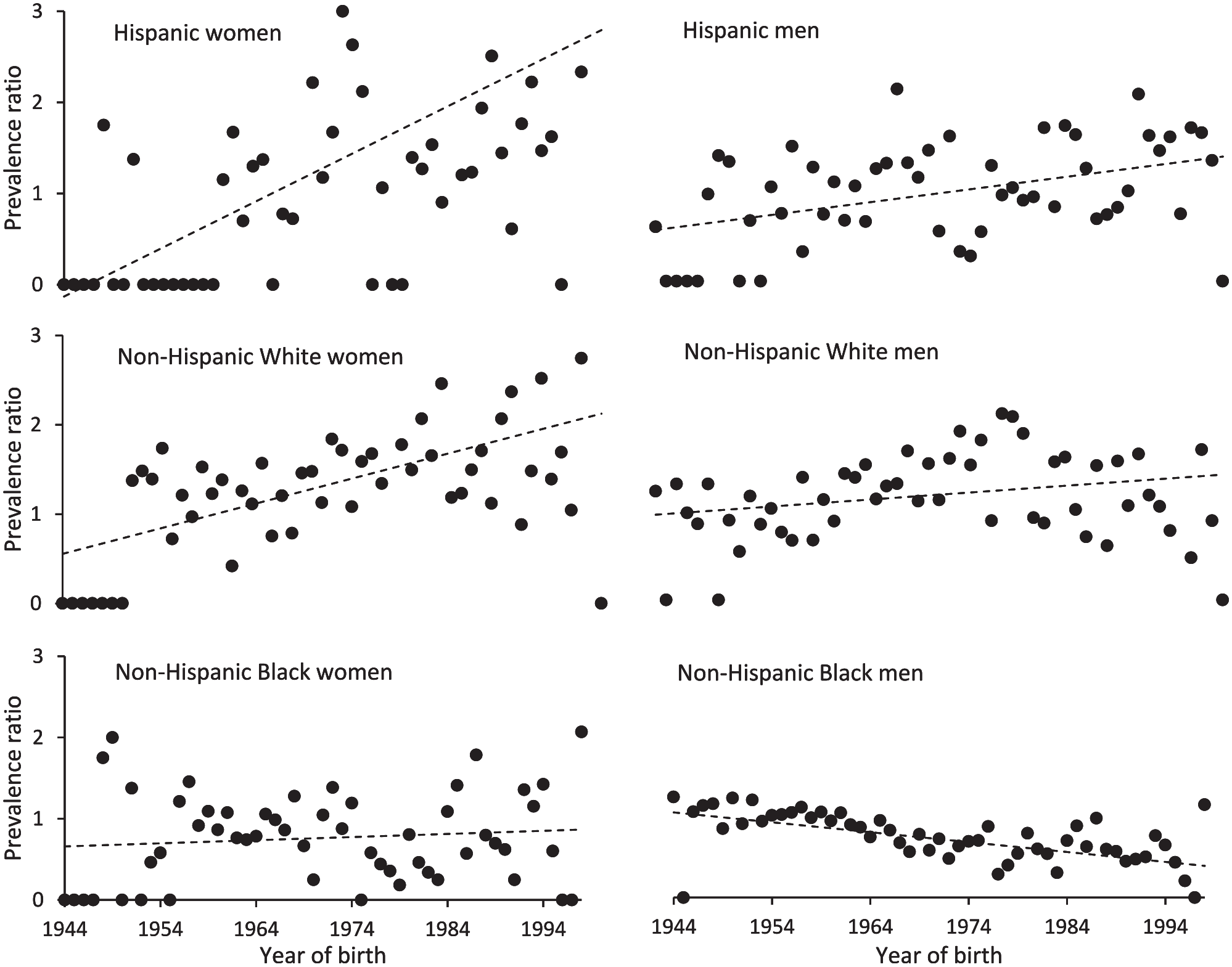
Demographic epidemiological trends in hepatitis C antibody prevalence by year of birth among people at the Dallas County Jail screened from 2017 to 2019 (n = 10 183). Prevalence ratios per birth year were calculated by dividing the prevalence in each demographic group by the prevalence in the general jail population in that year. Dots indicate prevalence ratio in each year; dashed line indicates trend line. Data were collected by the authors from electronic medical records and release records.
Discussion
We provide one of the few epidemiological studies of HCV antibody prevalence in the criminal justice system and, to our knowledge, the first calculation of HCV antibody incidence as people cycle through the criminal justice system. These data extend our previous findings21,22 and demonstrate dynamic interactions between race, sex, ethnicity, and birth year and HCV antibody prevalence that provide insights into developing future HCV prevention, surveillance, and treatment programming in the criminal justice system.
People in the criminal justice system experience alarmingly high rates of new and chronic HCV infection. In our study, the prevalence of HCV antibody was 16.7%; previous reports of HCV antibody prevalence in jails and prisons ranged from 9.6% to 41.1%.1,9,11,15,16,18,21-23 On average, this prevalence is 10 times the estimated national HCV antibody prevalence. 1 We also established that people leaving and returning to jail, as often happens in the criminal justice system, were frequently exposed to HCV. The estimated national HCV incidence in 2018 was 0.15 per 1000 person-years; in comparison, our incidence (13.5 per 1000 person-years) was 90 times higher. 24 The burden of new and chronic HCV infection in the criminal justice system underscores the value of risk reduction, education, and prevention initiatives during incarceration, especially given potential post-release barriers to care.
The epidemiology of HCV exposure similarly informs resource allocation for HCV health care in the criminal justice system. Similar to past studies, our study reproduced the well-known association between HCV antibody positivity and birth from 1945 through 1965; nearly half of the people tested in the birth cohort were HCV antibody–positive.11,25 Although unadjusted data would suggest differences in HCV antibody prevalence based on year of testing, adjusted data showed that those differences merely represent changing demographic characteristics of the tested population. We identified differences when we compared HCV antibody positivity by demographic group (sex, race, and ethnicity). For example, among older age groups, non-Hispanic Black men constituted the majority of HCV antibody–positive people in their age group, whereas in younger age groups, Hispanic and non-Hispanic White women made up the majority.
These results suggest that the demographic groups at highest risk for HCV exposure vary by age. Perhaps risk behaviors among older non-Hispanic Black men happened decades earlier, whereas Hispanic and non-Hispanic White women were exposed to HCV more recently. We identified an association between female sex and HCV antibody positivity. Other studies also showed higher HCV antibody prevalence among women than among men involved in the criminal justice system,17-19,26,27 particularly during the recent opioid epidemic.28-30 Compared with men, women involved in the criminal justice system more frequently experience health inequities,31-34 use substances, and engage in risky sexual activity and drug use. 35 Furthermore, among people involved in the criminal justice system who are living with HCV, IDU is more commonly reported among women, 36 a finding replicated in our study. Women involved in the criminal justice system and women who use drugs both report that intimate relationships are integral to their drug use and criminal justice system involvement 37 ; this population may be at heightened risk of acquiring HIV/HCV because of the “second on the needle phenomenon,” whereby women are frequently injected by their partners and after their partners,38,39 and intimate partner violence may decrease autonomy over safe sex and drug practices.40-44 Furthermore, women who use drugs or are involved in the criminal justice system face stigma 45 and engage in treatment for their drug use less often than men involved in the criminal justice system. Unfortunately, few interventions focus on the unique needs of women.46,47
We also identified an association between race and ethnicity and HCV exposure among Hispanic and non-Hispanic White people. Our results concur with a meta-analysis of racial and ethnic disparities in HCV antibody prevalence among people involved in the criminal justice system that showed the weighted HCV prevalence estimates to be 22% among Black people, 28% among Hispanic people, and 35% among White people. 48 However, as observed in several other studies, HCV viremia was more common among people who identified as Black.49-51 The differences in HCV clearance by sex and race may be related to differences in receipt of HCV treatment. However, given the low rates of treatment in incarcerated populations, these disparities could also stem from differences in major histocompatibility complex genes related to spontaneous HCV clearance by demographic group. 52 Nationally, the opioid epidemic has led to increased HCV prevalence among Hispanic and White people. 28 Likewise, some chronic conditions such as cancer, heart disease, and liver disease also occur more frequently among White people than among racial and ethnic minority populations in the criminal justice system.53,54 It has been postulated that these associations could be related to the over-incarceration of racial and ethnic minority populations, 55 thereby concentrating illness and poor health outcomes among people who are White and incarcerated.48,54,56 However, the overall number of people living with HCV and involved in the criminal justice system is higher among racial and ethnic minority populations because of the systemic incarceration of racial and ethnic minority populations in the United States. 55
The high HCV incidence and prevalence among all people at our large county jail argue for the implementation of universal opt-out screening at all criminal justice system locations in concordance with the Centers for Disease Control and Prevention and US Preventive Services Task Force recommendations for universal HCV screening.57,58 Risk-based or birth-cohort screening is inadequate: simulated models estimate targeted screening misses approximately 50% of HCV infections.11,21,25,59 In our study, birth-cohort screening would have overlooked 59% of HCV infections because we more frequently tested people with later birth years. Universal opt-out screening in the criminal justice system paired with HCV treatment can also improve population health by reducing HCV transmission with the achievement of sustained virologic response (SVR).59,60
Beyond harnessing epidemiological trends to create tailored HCV prevention paradigms, testing for HCV and implementation of HCV treatment in the criminal justice system align with public health priorities. 61 For people living with HCV, treatment offers numerous benefits, including improved clinical outcomes, increased quality of life, and decreased health care–related costs,3,4 and treatment fulfills the obligation of the criminal justice system to provide health care equivalent to the community standard. 62 Moreover, universal provision of HCV treatment would lead to substantial decreases in community HCV infections. 59 Unfortunately, fewer than 1% of incarcerated individuals with known HCV infection are being treated. 63 The most frequently cited barriers to HCV treatment in criminal justice systems are cost, unpredictable movement within the system, and stigma associated with treatment.61,64 However, models suggest that HCV treatment in criminal justice systems is highly cost effective 59 by preventing end-stage liver disease and subsequent infections in the community and demonstrates high rates of attaining SVR during incarceration.65,66
Additional attention needs to be directed toward connections to care and HCV prevention, particularly for people released from jail, whose stays are generally short. The HCV care cascade includes testing, diagnosis, referral to a subspecialist, appointment scheduling, initiation of treatment, and achieving SVR. 6 Most data on linkage to care come from the HIV literature, which stresses the importance of integrated social, financial, behavioral health, substance use, and primary care services. 67 The limited available data on HCV treatment after incarceration demonstrate room for improvement: 10% of patients initiated treatment and 4% achieved SVR.68,69 Multiple barriers to successful connection to community-based HCV care and prevention exist. First, HCV treatment lacks the federal funding structure that supports access to HIV treatment. 70 In addition, states that did not expand Medicaid and have high rates of uninsured residents, such as Texas, will have limited access to HCV treatment for people released from the criminal justice system.71,72 For those who are covered by Medicaid, treatment eligibility may vary; for example, it may cover HCV treatment only for advanced liver disease, despite proven benefits for all patients.3,73 Finally, needle exchange programs are illegal in many states, including Texas, limiting harm reduction initiatives and increasing the risk of re-infection in patients who are successfully treated. These logistical barriers to improving both the HCV care cascade and HCV prevention highlight the importance of implementing national evidence-based interventions to address HCV from prevention to treatment.
Limitations
Our study had several potential limitations. First, most patients who were tested were already undergoing a blood test, which could have resulted in a higher estimated prevalence and incidence of HCV by selecting for a group with more chronic medical conditions. In addition, the incidence was only calculated for people who had entered and left the jail multiple times during our study period, which could have resulted in an overestimation of incidence by concentrating people with HCV risk behaviors or alternatively an underestimation given that HCV prevalence was significantly higher among those who were released to prison rather than not. Second, we had HCV risk factor data only from HCV antibody–positive individuals, thereby limiting comparisons between the groups, and the risk factor data were limited to 1 year. Because risk behaviors were self-reported in a criminal justice facility, they were likely underreported. Lastly, our study was conducted at a single institution; therefore, our findings may not be generalizable to other criminal justice settings, although the differences in HCV antibody positivity by demographic groups were consistent with national data on HCV prevalence and incidence.
Conclusions
A multipronged approach in criminal justice systems that involves harm reduction, universal testing, education, and linkage to care is vital to decreasing the spread of HCV. Our data argue for investment in HCV prevention and treatment by demonstrating a persistently high prevalence and high incidence of HCV at a large urban jail. We found that women, particularly non-Hispanic White women and younger women, were increasingly affected by HCV, in alignment with national surveillance data in the context of the national IDU epidemic. Our findings are related to the overlapping epidemics of substance use and incarceration and have implications for implementation of interventions for universal screening, connection to care, treatment, and risk reduction in the criminal justice system to address HCV as a matter of public health.
Footnotes
Acknowledgements
The authors acknowledge Gilead Sciences, Inc, FOCUS Program. The FOCUS Program is a public health initiative that enables partners to develop and share best practices in routine blood-borne virus (HIV, hepatitis C, hepatitis B) screening, diagnosis, and linkage to care in accordance with screening guidelines promulgated by the Centers for Disease Control and Prevention, the US Preventive Services Task Force, and state and local public health departments. FOCUS funding supports HIV, hepatitis C virus, and hepatitis B virus screening and linkage to the first medical appointment after diagnosis. FOCUS partners do not use FOCUS awards for activities beyond linkage to the first medical appointment.
The authors also acknowledge the following Parkland Health and Hospital Systems staff members who contributed to this project: Patrick M. Jones, vice president; Tina M. Hill, correctional health administrator/population health contract administrator; Michelle Zhao, associate director of performance improvement; Samsher Rawal, correctional health laboratory section supervisor; Drew Esseltine, medical assistant; Jeanette Hill, phlebotomy specialist II; Ulysses Prioleau, phlebotomy specialist II; Ken Dobbs, departmental systems manager; Kyung Tae Kim, departmental systems administrator; and Kiki Teal, MSN, RN, CCHP-RN, director of nursing–correctional health and FOCUS project manager. The authors also acknowledge the Parkland Health and Hospital System’s Correctional Care team and security staff at the Dallas County Jail for their assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A.N. is supported by funding from the National Institutes of Health (R34 DA 045592, U01 DA 045592). A.W., R.T., and A.N. received research funding from the Gilead Sciences, Inc. FOCUS program, which partners with health care organizations in implementing hepatitis C virus screening, linkage to first appointment in development of best practice models. FOCUS supports activities up to first medical appointment and, thus, was not involved in Parkland Health and Hospital System correctional health’s decisions for subsequent patient care, the design of this study, or preparation of this article.