
Abstract
Objective
Higher mortality among full-term infants (term infant deaths) contributes to disparities in infant mortality between the United States and other developed countries. We examined differences in the causes of term infant deaths across county poverty levels and urban–rural classification to understand underlying mechanisms through which these factors may act.
Methods
We linked period birth/infant death files for 2012-2015 with US Census poverty estimates and county urban–rural classifications. We grouped the causes of term infant deaths as sudden unexpected death in infancy (SUDI), congenital malformations, perinatal conditions, and all other causes. We computed the distribution and relative risk of overall and cause-specific term infant mortality rates (term IMRs) per 1000 live births and 95% CIs for county-level factors.
Results
The increase in term IMR across county poverty and urban–rural classification was mostly driven by an increase in the rate of SUDI. The relative risk of term infant deaths as a result of SUDI was 1.6 (95% CI, 1.5-1.8) times higher in medium-poverty counties and 2.3 (95% CI, 1.2-2.5) times higher in high-poverty counties than in low-poverty counties. Cause-specific IMRs of congenital malformations, perinatal conditions, and death from other causes did not differ by county poverty level. We found similar trends across county urban–rural classification. Sudden infant death syndrome was the main cause of SUDI across both county poverty levels and urban–rural classifications, followed by unknown causes and accidental suffocation and strangulation in bed.
Conclusions
Interventions aimed at reducing SUDI, particularly in high-poverty and rural areas, could have a major effect on reducing term IMR disparities between the United States and other developed countries.
Information on mortality patterns is key to understanding changes in the health and well-being of a population. Mortality among full-term infants (term infant deaths) has garnered increasing interest in recent years in light of cross-country comparisons, which have identified high mortality rates among this subpopulation of births as the leading contributor to the poor US infant mortality rate (IMR) ranking in international comparisons. 1,2 The Centers for Disease Control and Prevention estimates that approximately 50% of the difference in infant mortality between the United States and Sweden was the result of the higher US mortality rate among term infants. 1 Several studies have investigated the drivers of term infant deaths in the United States. Their findings suggest that individual-level factors, such as maternal education, age, and marital status, alone cannot explain the high term infant mortality rate (term IMR) observed in the United States and that geographic area factors—including those affecting quality and access to health care and social services (eg, state of birth)—might play a role. 2,3 To our knowledge, however, no research has examined whether IMRs from the causes of term infant death differ across geographic area factors.
In this study, we build on recent findings showing that high-poverty and rural counties, 2 geographic area factors consistently linked with adverse birth outcomes, 4,5 are independently associated with term infant death. 6 By investigating differences in the underlying causes of term infant deaths across county poverty and urban–rural classifications, we sought to inform future research on the potential mechanisms through which these geographic area factors may lead to term infant deaths.
Methods
This cross-sectional study used linked birth and death records of all infants born in the United States from January 1, 2012, through December 31, 2015. We used federal information-processing standards county codes indicating mother’s county of residence to link birth/infant death data with 2012-2015 model-based county poverty estimates produced by the US Census Bureau 7 and the 2013 National Center for Health Statistics (NCHS) urban–rural classification scheme for counties using the Office of Management and Budget February 2013 delineation of metropolitan statistical areas, micropolitan statistical areas (derived according to the 2010 Office of Management and Budget standards for defining these areas), and vintage 2012 post–US Census estimates of the resident US population. 8 All infants in the birth/death records could be directly linked to the county identifiers in these data sets (100% match rate). County-identified infant birth/death records were provided with permission from the National Association for Public Health Statistics and Information Systems as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. This project was considered exempt by the University of Wisconsin–Madison Institutional Internal Review Board.
Analyses included all term births (37-44 weeks of gestation) born alive to mothers residing in any of the 50 states and the District of Columbia from January 1, 2012, through December 31, 2015. We defined gestational age based on the obstetric estimate. 9 We excluded births that were missing data on gestational age, based on the obstetric estimate. We defined term IMR as the number of deaths in the first year of life per 1000 live births with a gestational age of 37-44 weeks. We based underlying causes of infant death on information from death certificates. According to the recommended protocols, deaths due to violence or suspicious events are further investigated and certified primarily by medical examiners or coroners. 10 NCHS then reviews and codes death certificates using the guidelines of the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM). 11 In this study, we grouped reported underlying causes of term infant death into 4 categories based on previous literature 2 : (1) congenital malformations (ICD-10 codes Q00-Q99), (2) sudden unexpected death in infancy (SUDI; ICD-10 codes V01-Y89 and R00-R99), (3) perinatal conditions (ICD-10 codes P00-P96), and (4) all other causes (all other ICD-10 codes). This grouping was used in a study investigating term infant deaths, which developed the SUDI classification to minimize potential state-level differences in the misclassification of unexplained deaths to sudden infant death syndrome (SIDS) vs “other unexplained causes.” 2 This definition of SUDI is a broader term than the more commonly used definition of SUDI 12 because it encompasses infant deaths resulting from accidents and assault. This definition is further supported by evidence that deaths caused by maltreatment and neglect are often misclassified as violent deaths or accidents, and this misclassification may vary by rurality, geography, and other factors. 13
The primary exposures of interest were county poverty level and urban–rural classification. We defined county poverty level as the percentage of children living in a county at or below the federal poverty level (FPL) obtained from the US Small Area Income and Poverty Estimates for 2012-2015. 7 This measure is not only highly correlated with other poverty measures, such as overall number of people living in poverty, but also is more sensitive to changes in poverty levels 14 and more relevant to the lives of women with newborns. We assigned counties to 1 of 3 poverty groups: <10.0% FPL (low poverty), 10.0%-19.9% FPL (medium poverty), and ≥20.0% FPL (high poverty), as previously established in the literature. 6,15 We also defined county urban–rural classification using the NCHS urban–rural classification with 6 levels: 4 metropolitan (large central metropolitan, large fringe metropolitan, medium metropolitan, and small metropolitan) and 2 nonmetropolitan (micropolitan and noncore) and then further combined into 3 levels: large urban (large central and large fringe metropolitan areas), small–medium urban (small and medium metropolitan areas), and rural (micropolitan and noncore) counties. 8
We calculated cause-specific IMRs and their 95% CIs for the causes of deaths among infants born at term, overall (per 1000 live term births) and across county poverty levels and urban–rural classifications (per 100 000 live term births). We also computed relative risks (RRs) and 95% CIs comparing cause-specific term IMRs across county poverty levels and urban–rural classifications and tested for interactions between county poverty levels and urban–rural classifications on the term IMR using the Wald χ2 test. We considered P < .05 to be significant. In addition, we calculated term IMRs and 95% CIs for each underlying cause of death for the top 4 causes of term infant death categories and computed RRs comparing rates across exposure groups. Finally, we calculated cause-specific excess mortality and 95% CIs for all term births in the United States across counties (2012-2015) using large urban, low-poverty counties as the reference group. We conducted all statistical analyses using Stata version 15.1 (StataCorp LLC).
Results
During calendar years 2012-2015, a total of 15 862 689 infants were born in the United States, of whom 14 038 594 (88.5%) were born at term. The overall IMR in the pooled data was 5.9 (95% CI, 5.8-5.9) per 1000 term live births. The term IMR was 2.1 (95% CI, 2.1-2.2) per 1000 term live births. The ranking of the causes of term infant death was the same for all 3 county poverty groups: SUDI, congenital malformations, perinatal conditions, and all other causes (Table 1). The RR of death due to SUDI was 1.6 (95% CI, 1.5-1.8) in medium-poverty counties and 2.3 (95% CI, 1.2-2.5) in high-poverty counties as compared with low-poverty counties. The rate of congenital malformations and perinatal conditions and deaths due to other causes increased slightly across county poverty levels (from low poverty to high poverty). Across the county urban–rural continuum, births in small–medium urban counties had a high risk of mortality due to SUDI (RR = 1.4; 95% CI, 1.4-1.5), and births in rural counties had the highest risk (RR = 1.8; 95% CI, 1.7-1.9) compared with births in large urban counties. As with county poverty, the RR of congenital malformations increased slightly across classifications (from large urban counties to rural counties). Although the RR for term infant deaths due to perinatal conditions was similar between small–medium urban counties and large counties (RR = 1.1; 95% CI, 1.0-1.2), it was higher in rural counties than in urban counties (RR = 1.5; 95% CI, 1.4-1.7).
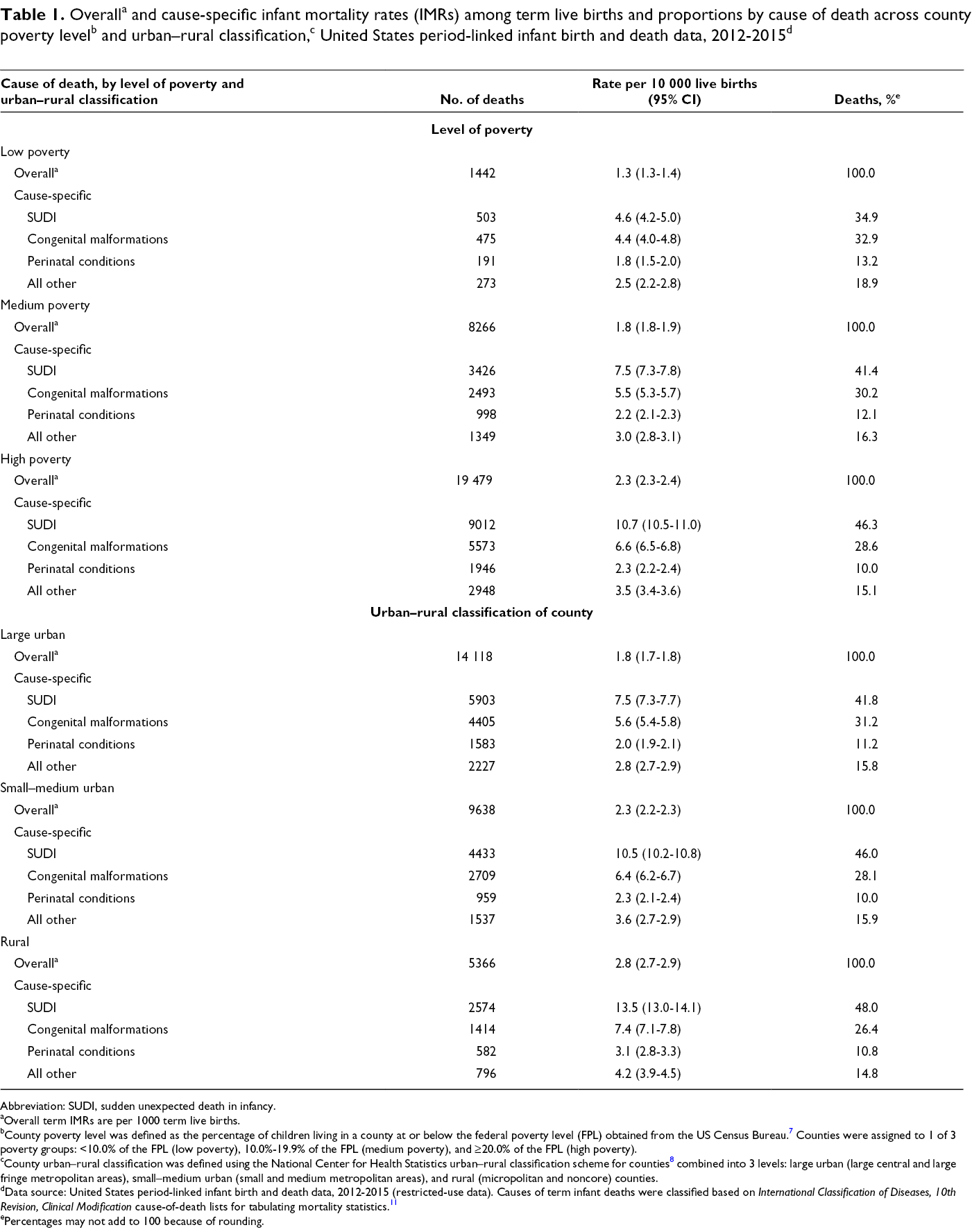
Abbreviation: SUDI, sudden unexpected death in infancy.
aOverall term IMRs are per 1000 term live births.
bCounty poverty level was defined as the percentage of children living in a county at or below the federal poverty level (FPL) obtained from the US Census Bureau. 7 Counties were assigned to 1 of 3 poverty groups: <10.0% of the FPL (low poverty), 10.0%-19.9% of the FPL (medium poverty), and ≥20.0% of the FPL (high poverty).
cCounty urban–rural classification was defined using the National Center for Health Statistics urban–rural classification scheme for counties 8 combined into 3 levels: large urban (large central and large fringe metropolitan areas), small–medium urban (small and medium metropolitan areas), and rural (micropolitan and noncore) counties.
dData source: United States period-linked infant birth and death data, 2012-2015 (restricted-use data). Causes of term infant deaths were classified based on International Classification of Diseases, 10th Revision, Clinical Modification cause-of-death lists for tabulating mortality statistics. 11
ePercentages may not add to 100 because of rounding.
Among term infant deaths classified as SUDI, the most common cause was SIDS across all county poverty levels, accounting for approximately 40% (range, 36.1%-41.8%) of all SUDI deaths, followed by unknown/ill-defined causes (range, 22.3%-25.2%), accidental suffocation and strangulation in bed (range, 16.7%-20.4%), and assault by unspecified means (range, 3.2%-3.8%; Table 2). The RR of SIDS was higher among term births in medium-poverty (RR = 1.5; 95% CI, 1.3-1.8) and high-poverty (RR = 2.0; 95% CI, 1.7-2.3) counties than in low-poverty counties. The RR of term infant deaths due to accidental suffocation and strangulation in bed were also higher among term births in medium-poverty (RR= 1.9; 95% CI, 1.5-2.4) and high-poverty (RR = 2.8; 95% CI, 2.3-3.6) counties than in low-poverty counties. The RR of assault by unspecified means was lower among births in low-poverty counties than in medium-poverty (RR = 1.4; 95% CI, 0.8-2.4) and high-poverty (RR = 2.2; 95% CI, 1.4-3.7) counties. We observed similar trends with more modest effects when examining causes of SUDI by county urban–rural classification. The RR of term infant deaths due to accidental suffocation and strangulation in bed was higher in small–medium urban (RR = 1.5; 95% CI, 1.4-1.7) and rural (RR = 1.7; 95% CI, 1.5-1.9) counties than in large urban counties. We also found small differences in the RR of term infant deaths due to assault by unspecified means in small–medium urban (RR = 1.2; 95% CI, 1.0-1.5) and rural (RR = 1.9; 95% CI, 1.5-2.5) counties than in large urban counties.
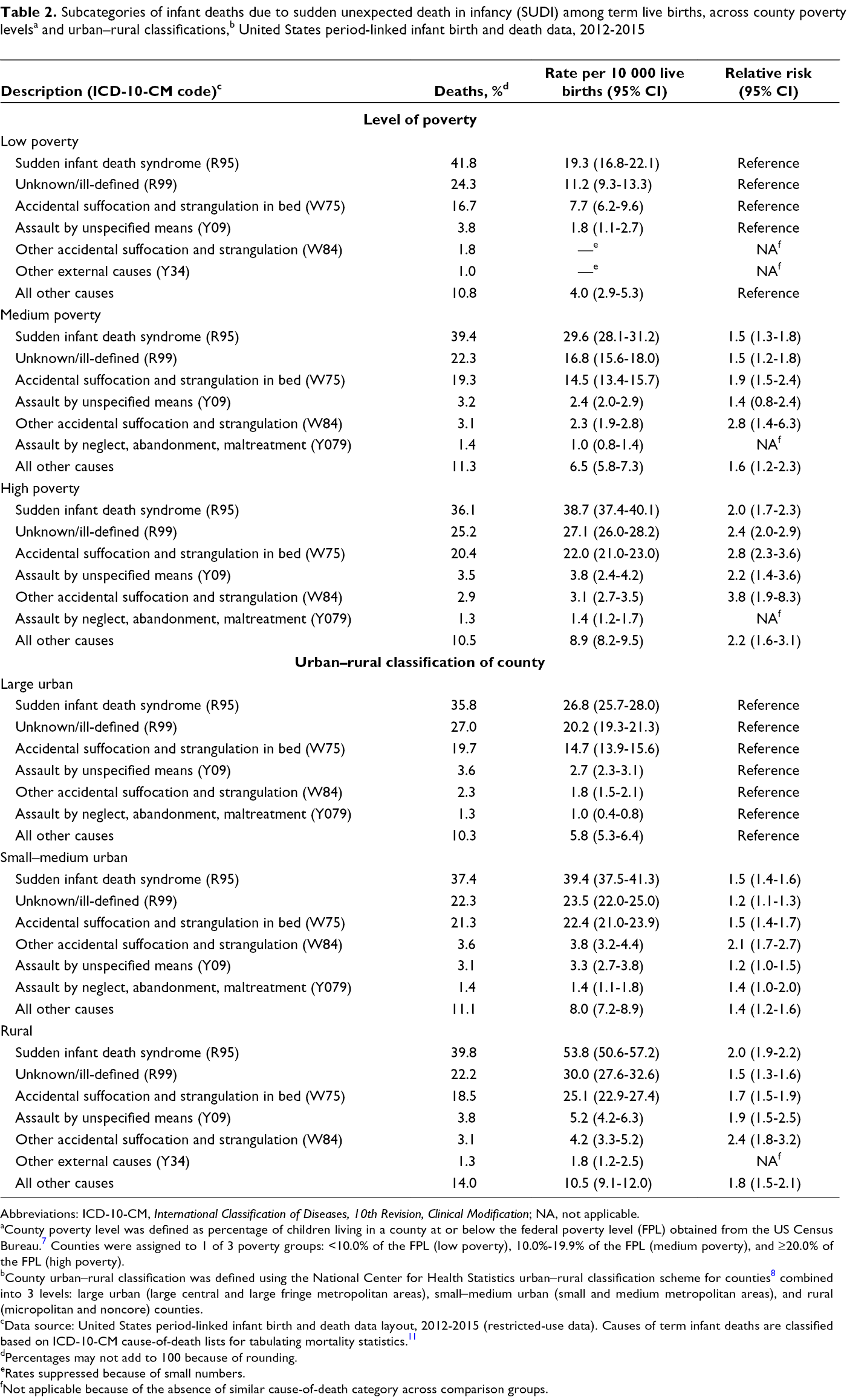
Abbreviations: ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification; NA, not applicable.
aCounty poverty level was defined as percentage of children living in a county at or below the federal poverty level (FPL) obtained from the US Census Bureau. 7 Counties were assigned to 1 of 3 poverty groups: <10.0% of the FPL (low poverty), 10.0%-19.9% of the FPL (medium poverty), and ≥20.0% of the FPL (high poverty).
bCounty urban–rural classification was defined using the National Center for Health Statistics urban–rural classification scheme for counties 8 combined into 3 levels: large urban (large central and large fringe metropolitan areas), small–medium urban (small and medium metropolitan areas), and rural (micropolitan and noncore) counties.
cData source: United States period-linked infant birth and death data layout, 2012-2015 (restricted-use data). Causes of term infant deaths are classified based on ICD-10-CM cause-of-death lists for tabulating mortality statistics. 11
dPercentages may not add to 100 because of rounding.
eRates suppressed because of small numbers.
fNot applicable because of the absence of similar cause-of-death category across comparison groups.
For most county poverty level and urban–rural classifications, the 2 most common causes of deaths due to congenital malformations were Trisomy 18 (Edwards syndrome) and congenital malformations of the heart (Table 3). The 2 most common causes of deaths due to perinatal conditions were hypoxic ischemic encephalopathy and birth asphyxia. For each of these causes of term infant deaths (congenital malformations and perinatal conditions), we found a small change in the proportion of term infant deaths across county poverty levels and urban–rural classifications. The risk of term infant death due to perinatal conditions was similar across both county-level factors. However, compared with low-poverty counties, the risk of death due to congenital malformations of the heart was higher (RR = 1.9; 95% CI, 1.6-2.4) in high-poverty counties. Similarly, the risk of death due to congenital malformations of the heart was higher (RR = 1.4; 95% CI, 1.3-1.5) in rural counties than in large urban counties.
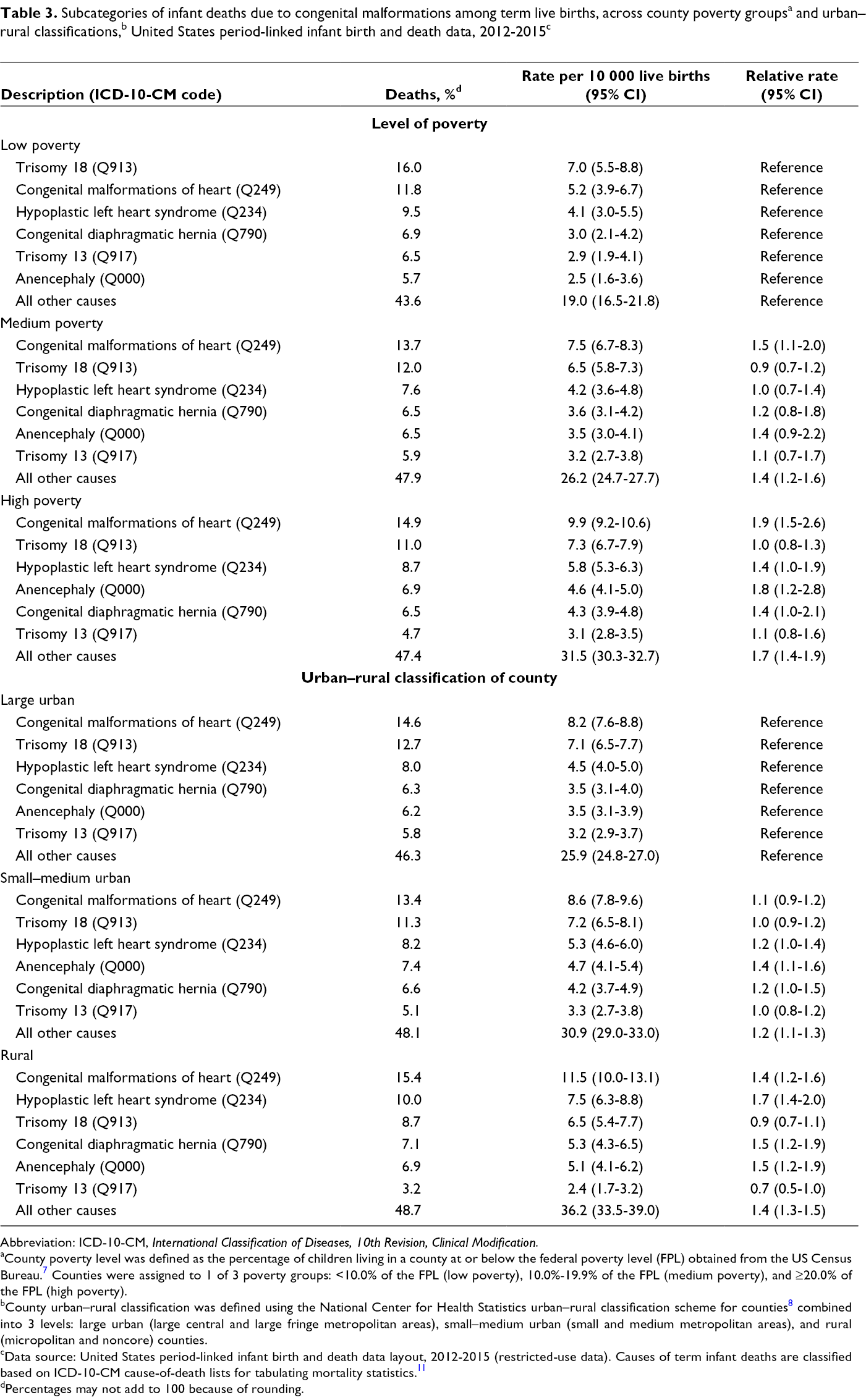
Abbreviation: ICD-10-CM, International Classification of Diseases, 10th Revision, Clinical Modification.
aCounty poverty level was defined as the percentage of children living in a county at or below the federal poverty level (FPL) obtained from the US Census Bureau. 7 Counties were assigned to 1 of 3 poverty groups: <10.0% of the FPL (low poverty), 10.0%-19.9% of the FPL (medium poverty), and ≥20.0% of the FPL (high poverty).
bCounty urban–rural classification was defined using the National Center for Health Statistics urban–rural classification scheme for counties 8 combined into 3 levels: large urban (large central and large fringe metropolitan areas), small–medium urban (small and medium metropolitan areas), and rural (micropolitan and noncore) counties.
cData source: United States period-linked infant birth and death data layout, 2012-2015 (restricted-use data). Causes of term infant deaths are classified based on ICD-10-CM cause-of-death lists for tabulating mortality statistics. 11
dPercentages may not add to 100 because of rounding.
The interaction effect between urban–rural classification and county poverty level on the risk of term infant deaths was modest (Table 4) and not significant (P = .09). The risk of term infant death was lowest in large urban counties and low-poverty counties (RR = 1.3; 95% CI, 1.2-1.4) and highest in rural high-poverty counties (RR = 3.0; 95% CI, 2.9-3.1). We calculated the cause-specific excess mortality for all term births in the United States (2012-2015) using large urban, low-poverty counties as the reference group (Table 5). We estimate that if the cause-specific term IMR in the United States was reduced to the rate observed in low-poverty, large urban counties, 10 936 (95% CI, 8830-12 763) excess term infant deaths could have been prevented.
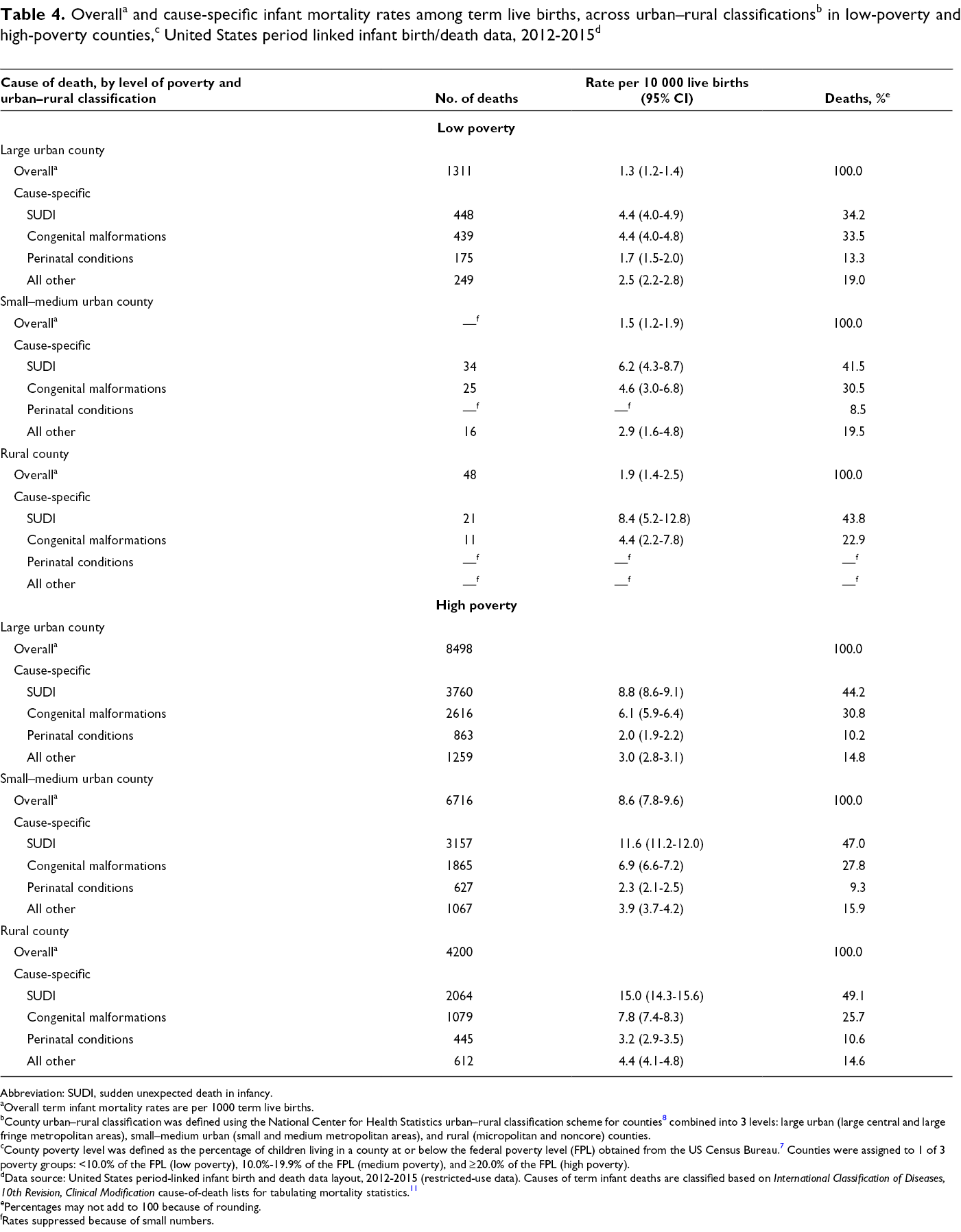
Abbreviation: SUDI, sudden unexpected death in infancy.
aOverall term infant mortality rates are per 1000 term live births.
bCounty urban–rural classification was defined using the National Center for Health Statistics urban–rural classification scheme for counties 8 combined into 3 levels: large urban (large central and large fringe metropolitan areas), small–medium urban (small and medium metropolitan areas), and rural (micropolitan and noncore) counties.
cCounty poverty level was defined as the percentage of children living in a county at or below the federal poverty level (FPL) obtained from the US Census Bureau. 7 Counties were assigned to 1 of 3 poverty groups: <10.0% of the FPL (low poverty), 10.0%-19.9% of the FPL (medium poverty), and ≥20.0% of the FPL (high poverty).
dData source: United States period-linked infant birth and death data layout, 2012-2015 (restricted-use data). Causes of term infant deaths are classified based on International Classification of Diseases, 10th Revision, Clinical Modification cause-of-death lists for tabulating mortality statistics. 11
ePercentages may not add to 100 because of rounding.
fRates suppressed because of small numbers.
Scenario estimating excess cause-specific term infant mortality, assuming mortality rates in large, urban, low-poverty areas, United States, 2012-2015 a
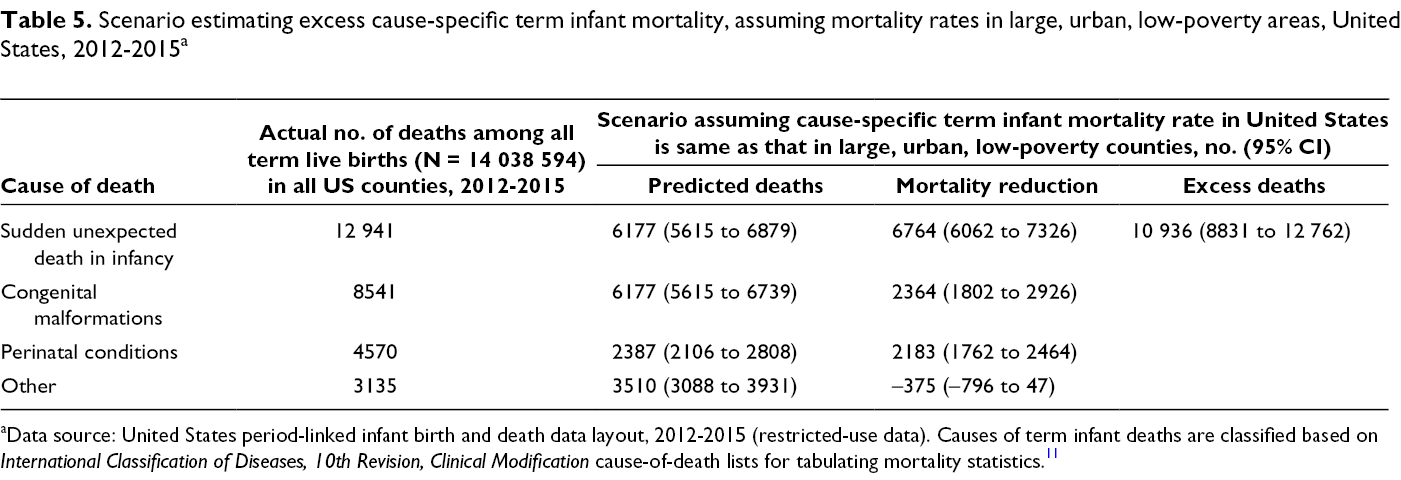
aData source: United States period-linked infant birth and death data layout, 2012-2015 (restricted-use data). Causes of term infant deaths are classified based on International Classification of Diseases, 10th Revision, Clinical Modification cause-of-death lists for tabulating mortality statistics. 11
Discussion
By using county of maternal residence to examine the causes of term infant deaths by county poverty level and urban–rural classification, we captured differences in IMRs among infants born at term that could be related to differences in conditions during pregnancy and directly after birth. We found heterogeneity in term IMRs across both county-level factors that were driven mostly by high rates of SUDI as a result of increased rates of SIDS, unknown causes, accidental suffocation and strangulation in bed, and unspecified assault.
A link between low socioeconomic status and SUDI, defined at the area level (eg, area deprivation score) or individual level (eg, paternal occupation), has been established across countries and time. 16 A 2018 report found that the risk of postneonatal mortality in general, and SIDS in particular, was highest in rural US counties. 4 Although the mechanisms by which SIDS occurs are not clearly understood, they are likely multifactorial. Although some mechanisms may involve underlying physiologic susceptibility, residing in high-poverty or rural counties may increase the risk of SIDS distally by affecting maternal behaviors (eg, smoking, drinking) and/or housing conditions (eg, heating and space that may lead to overwrapping or co-sleeping). 4,16 -19 The latter is suggested by the higher rates of accidental suffocation and strangulation in bed observed with increasing county levels of poverty and rurality and may be a consequence of context rather than nonadherence to safe sleep recommendations.
We found small increases in the risk of term infant death due to congenital malformations and perinatal conditions across both county poverty levels and urban–rural classifications. These small increases in risk suggest that reduced access to health care associated with high poverty levels and rural counties as a result of lack of health insurance or proximity to the nearest hospital, 18 for example, may not fully explain the higher term IMR observed across both county-level factors. Recent improvements in the survival of infants born with congenital malformations of the heart, the most common cause of deaths due to congenital malformations, have been credited to improvements in screening and medical surgical interventions during pregnancy or immediately after delivery. 20,21 Similarly, interventions to reduce mortality due to both primary causes of perinatal conditions (hypoxic ischemic encephalopathy and birth asphyxia) are related to the quality of clinical care during the perinatal period. 22,23
Although we did not find evidence of an interaction between county poverty level and urban–rural classification on term infant survival, the term IMR in low-poverty, large urban counties (1.3 per 1000 term live births) was close to the European benchmark of <1.25 per term IMR defined by Bairoliya and Fink. 2 Our study finding that term IMRs in urban, low-poverty areas are close to the European benchmarks suggests that interventions targeted at reducing SUDI could have a major effect on reducing disparities in infant mortality between the United States and other developed countries. As per our excess term IMR estimation, we found that if the cause-specific term IMR was reduced to the rate observed in low-poverty, large urban counties, 10 937 excess term infant deaths could have been prevented, 62% of which were due to SUDI. Evidence from European studies suggests that most SIDS deaths could be attributed to sleeping and maternal drug consumption. 24 Through programs that target prevention of smoking during pregnancy, discourage bed sharing, encourage the use of an empty crib, and encourage putting the baby “back to sleep,” the incidence of SIDS was lowered by 75% in Sweden and Scotland, 2 countries with low term IMRs. 25,26 Similar programs put in place in the United States since the early 1990s led to a decline in the rate of SIDS by 55% from 1992 to 2005. 27 However, the decline in SIDs rates has plateaued in recent years, and the adoption of sleep recommendations remains a challenge in the United States, 27 particularly among socioeconomically disadvantaged communities. 28,29 A better understanding of those challenges within the context of both poverty level and rurality is needed.
Limitations
This study had several limitations, mostly related to the possible misclassification of the causes of death. First, the underlying cause of death can be difficult to verify without autopsy. This limitation is particularly true in the case of SIDS, which is based on a diagnosis of exclusion. Differential distribution of resources, training of medical examiners, and the workload of infant death scene investigators may explain some of the observed differences in rates in high-poverty or rural counties. To mitigate this potential misclassification, we relied on convention, based on previous literature and NCHS, to define cause-of-death categories, 2,11,30 and we used a broad category of SUDI for most of the analysis. In addition, we examined the classification of causes of term infant deaths by state to investigate whether state differences in reporting were driving observed patterns across county poverty levels and urban–rural classification, but we were unable to discern any pattern by state. Second, the use of maternal residence to assign county measures was a limitation, because mothers may have moved to another county right before or right after delivery. Third, because of small numbers of infant deaths, particularly with stratifications, we did not examine differences by racial/ethnic groups across county poverty levels and rural–urban classifications. As with preterm births, the rate of term infant deaths was higher among Black infants than among White infants. 31 In addition, because of structural racism, Black infants are more likely than White infants to be born in high-poverty counties. 32 Therefore, an important next step is to examine the effect of county-level and other area factors on racial/ethnic disparities in term infant deaths. Finally, both poverty level and rural–urban classification are distal factors in their association with term IMR. An understanding of more proximal factors influenced by county poverty level and urban–rural classification would provide additional insight into interventions that could be used to reduce term IMR in certain areas.
Conclusions
Our findings emphasize the need to understand the effect of geographic area factors on infant survival. Most research examining area factors such as poverty and neighborhood socioeconomic effects in the past 2 decades have focused on preterm births and low birth weight as the outcome of interest. 5 The increased risk of term infant death across both county-level factors driven mostly by higher rates of SUDI suggests that more research is needed to better understand factors influencing the survival of term infants. Social programs targeted at alleviating the effects of prenatal poverty, including state-earned income tax credit programs, which have been shown to reduce low birth weight and maternal smoking, 33 could have an important role to play in reducing the incidence of SUDI and, therefore, term IMR. Finally, although much of the substantial reduction in infant mortality in the United States during the past century may have resulted from increased access to high-quality obstetric and neonatal care, 34 our findings suggest that further reductions in term infant death may require more than improved health care access. More work is needed to understand how interventions and policies targeting broader contextual factors, such as housing, public safety, and socioeconomic opportunity, may lead to lower levels of term infant death.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by the National Institute of General Medical Sciences of the National Institutes of Health under award number R25GM083252. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Availability of Data
Data are only available through permission from the National Association for Public Health Statistics and Information Systems (NAPHSIS) as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program.