
Abstract
Objectives
Essential workers in the United States need access to health care services for preventive care and for diagnosis and treatment of illnesses (coronavirus disease 2019 [COVID-19] or other infectious or chronic diseases) to remain healthy and continue working during a pandemic. This study evaluated access to health care services among selected essential workers.
Methods
We used the most recent data from the Behavioral Risk Factor Surveillance System, 2017-2018, to estimate the prevalence of 4 measures of health care access (having health insurance, being able to afford to see a doctor when needed, having a personal health care provider, and having a routine checkup in the past year) by broad and detailed occupation group among 189 208 adults aged 18-64.
Results
Of all occupations studied, workers in farming, fishing, and forestry occupations were most likely to have no health insurance (46.4%). Personal care aides were most likely to have been unable to see a doctor when needed because of cost (29.3%). Construction laborers were most likely to lack a personal health care provider (51.1%) and to have not had a routine physical checkup in the past year (50.6%). Compared with workers in general, workers in 3 broad occupation groups—food preparation and serving; building and grounds cleaning and maintenance; and construction trades—had significantly lower levels of health care access for all 4 measures.
Conclusion
Lack of health insurance and underinsurance were common among subsets of essential workers. Limited access to health care might decrease essential workers’ access to medical testing and needed care and hinder their ability to address underlying conditions, thereby increasing their risk of severe outcomes from some infectious diseases, such as COVID-19. Improving access to health care for all workers, including essential workers, is critical to ensure workers’ health and workforce stability.
In December 2019, coronavirus disease 2019 (COVID-19), caused by the newly identified severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in China; on March 11, 2020, the World Health Organization declared a global pandemic. 1 By mid-March, many states in the United States had begun implementing orders to stay at home and socially distance and for nonessential businesses to close temporarily. 2 On March 28, 2020, as part of the federal response to the spread of COVID-19, the US Department of Homeland Security (DHS) issued an advisory to define essential critical infrastructure workers and help state and local authorities identify “workers who conduct a range of operations and services that are typically essential to continued critical infrastructure viability.” 3 Risks for COVID-19 infection among these essential workers may be higher among those who are required to report to the workplace, rather than telework, and who cannot physically distance from health care patients, the general public, and/or coworkers. 4,5
Access to health care services is crucial for keeping workers healthy and able to work. Lack of health insurance is associated with poor health status and difficulty accessing preventive health services and medical care. 6 -10 Routine medical care is important for identifying and controlling chronic conditions, which are associated with a higher risk for severe outcomes of COVID-19. 11,12 In the context of infectious diseases with community spread such as COVID-19, workers with difficulty accessing health care services (and especially those lacking paid sick leave) may delay diagnosis and work while ill. Delayed diagnosis of COVID-19 is associated with severe outcomes, 13,14 including long-term effects that could hamper the return to full employment, 15 -18 and may expose coworkers and members of the public to infection.
Studies conducted since 2013 indicate that the prevalence of having no health insurance varies in the United States by broad occupational group. 6,19 Inability to see a physician when needed because of cost, lack of a personal health care provider, and not having a routine checkup are other important markers of inadequate health care access. To our knowledge, no studies have evaluated any of these measures by broad or detailed occupation. We undertook this study to evaluate prepandemic (baseline) access to health insurance coverage and 3 other measures of health care access among selected essential critical infrastructure workers, particularly those with constraints on physical distancing.
Methods
The Behavioral Risk Factor Surveillance System (BRFSS) is an annual, state-based, random-digit–dial telephone survey of noninstitutionalized adults aged ≥18 residing in the United States. Fifty states, the District of Columbia, and 3 territories administer the survey. BRFSS collects information on chronic health conditions, health risk behaviors, access to health care services, and use of preventive services. 20 One of the optional modules in BRFSS solicits information on the industry and occupation of respondents. We used the 2 most recent years (2017 and 2018) for which BRFSS industry and occupation data were available as a surrogate for the current pandemic period. We analyzed 2 years of data to ensure a sufficient sample size to produce stable estimates for workers in occupations with relatively few workers. Thirty-one states in 2017 and/or 2018 asked the industry and occupation questions: California, Connecticut, Delaware, Florida, Georgia, Hawaii, Idaho, Illinois, Kansas, Louisiana, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Pennsylvania, Rhode Island, South Carolina, Tennessee, Texas, Washington, and Wisconsin. Among the states that used the industry and occupation questions in each year, the median overall survey response rate was 42.5% in 2017 and 49.1% in 2018. 21,22 BRFSS was reviewed by the Human Research Protection Office of the Centers for Disease Control and Prevention and determined to be exempt research.
Study Population
Our sample included nonmilitary respondents aged 18-64 and currently employed for wages or self-employed in the 31 states. We excluded members of the military because they had access to health care and because BRFSS excludes institutionalized adults and those residing outside the United States and, thus, is not representative of the military. We excluded respondents aged ≥65 because they were presumed eligible for Medicare.
Occupation
Survey participants who were currently employed at the time of their interview or who had been employed within the previous 12 months were asked the occupation question: “What kind of work do you do? For example, registered nurse, janitor, cashier, auto mechanic.” We coded participants’ free-text responses to the 2010 version of the US Census Bureau occupation numeric codes. 23 To select essential occupations, we identified census occupation codes that matched as closely as possible to the DHS guidance, which identifies work functions through a combination of industries and occupations but does not specify census codes. Because of this matching process, we reported some occupations in broad groupings of related census codes, and we reported other occupations at a more detailed level, consisting of individual census codes or narrower groups of related census codes. We identified 14 broad occupational groups and 29 detailed occupations that matched DHS criteria.
Health Care Access
The BRFSS asked all survey participants 4 questions on health care access: (1) “Do you have any kind of health care coverage, including health insurance, prepaid plans such as HMOs [health maintenance organizations], government plans such as Medicare, or Indian Health Service?” Possible responses were yes, no, don’t know/not sure, and refused. We classified respondents who answered no as uninsured. (2) “Was there a time in the past 12 months when you needed to see a doctor but could not because of cost?” Possible responses were yes, no, don’t know/not sure, and refused. We classified respondents who answered yes as not having been able to see a doctor when needed because of cost in the past 12 months. (3) “Do you have one person you think of as your personal doctor or health care provider?” Possible responses were yes (only 1), >1, no, don’t know/not sure, and refused. We classified respondents who answered no as not having a personal health care provider. (4) “A routine checkup is a general physical exam, not an exam for a specific injury, illness, or condition. About how long has it been since you last visited a doctor for a routine checkup?” Possible responses were within the past year (anytime <12 months ago), within the past 2 years (1 year but <2 years ago), within the past 5 years (2 years but <5 years ago), ≥5 years ago, don’t know/not sure, never, and refused. We classified respondents who replied never or >1 year as not having had a checkup in the past year. The first question pertained to health insurance coverage, and the other 3 questions indicated potential difficulty accessing health care because of lack of health insurance or because of underinsurance among the insured. The percentage of respondents excluded from the analysis of measures of health care access because the responses were don’t know/not sure, refused, or missing were 0.4% for health care coverage, 0.2% for not being able to see a doctor because of cost, 0.4% for not having a personal health care provider, and 1.0% for routine checkup.
Statistical Analysis
BRFSS statisticians weighted data using an iterative proportional weighting (raking) procedure to adjust for demographic differences between respondents and the population they represented. We analyzed the data accounting for the complex BRFSS sampling design using SAS Proc SURVEYFREQ version 9.4 (SAS Institute, Inc). We did not adjust the weights for states that contributed 1 year of data; however, for states that contributed 2 years of data, we divided the weights by 2 to achieve annualized estimates. To focus on the magnitude of the estimates, we calculated crude prevalences and did not adjust for factors such as age, sex, race/ethnicity, employment status (employed for wages vs self-employed), annual household income, Medicaid access, and having a chronic condition that can affect access to health care services. 6,9,24 We tabulated estimates for all eligible workers combined (regardless of essential worker status, hereinafter “all workers”) and for each essential worker group of interest. We considered differences between the estimates for all workers and the estimates for a specific group significant if 95% CIs did not overlap. We reported estimates with a relative SE >30% and ≤50%, but these estimates should be interpreted with caution because they do not meet standards of reliability or precision. We did not report estimates with an unweighted denominator <50 or a relative SE >50%. 25
Results
The sample consisted of 213 706 currently employed, nonmilitary workers, of whom 189 208 were aged 18-64 and eligible to be included in the analysis (Table 1). Of all workers, 14.3% (95% CI, 13.9%-14.8%) did not have health insurance, 13.9% (95% CI, 13.5%-14.2%) could not see a doctor when they needed to because of cost, 27.6% (95% CI, 27.1%-28.1%) did not have a personal health care provider, and 31.6% (95% CI, 31.0%-32.1%) did not have a routine checkup within the past year (Table 2).
All workers and selected essential critical infrastructure workers aged 18-64, by occupation, Behavioral Risk Factor Surveillance System (BRFSS), 31 states, 2017-2018 a
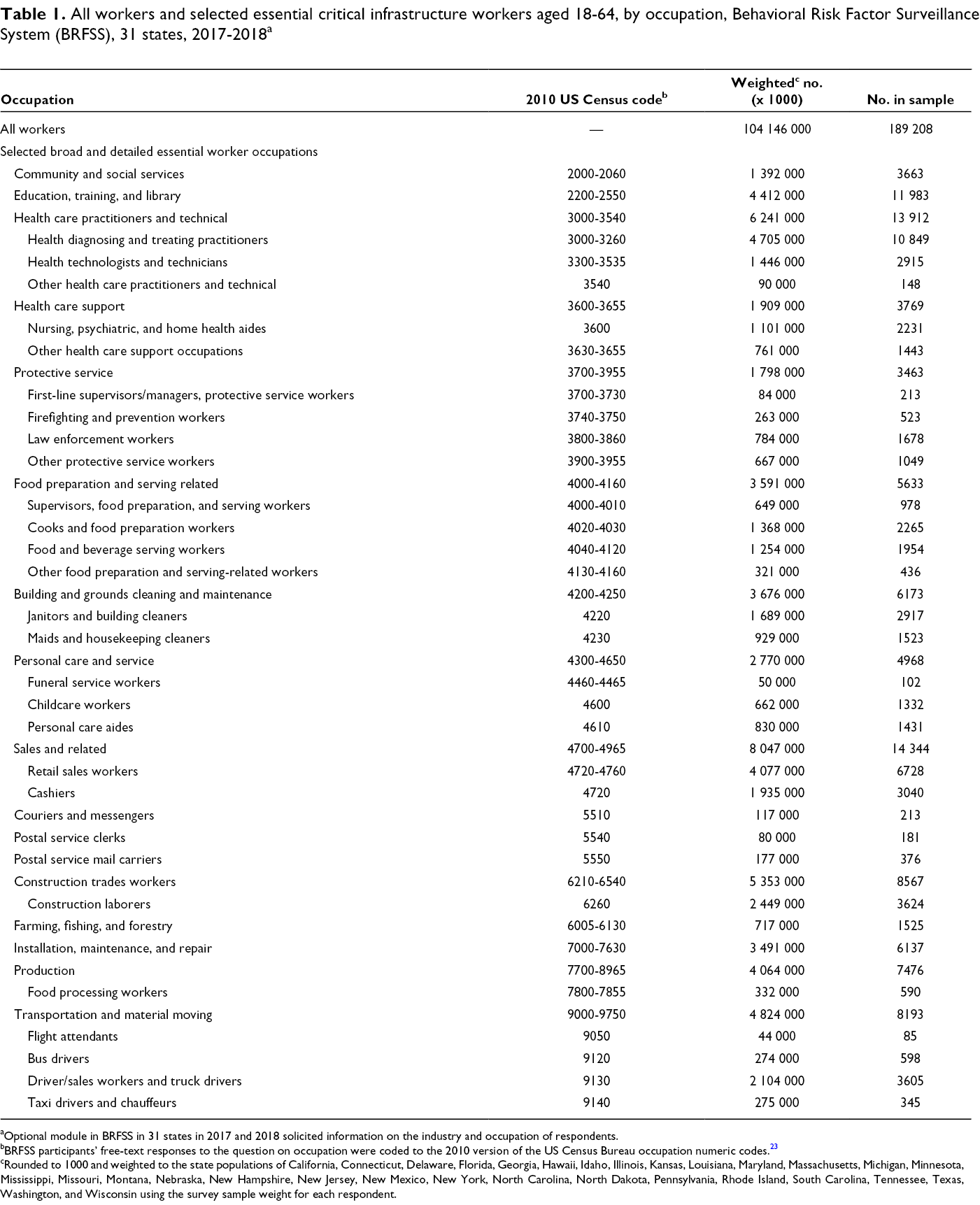
aOptional module in BRFSS in 31 states in 2017 and 2018 solicited information on the industry and occupation of respondents.
bBRFSS participants’ free-text responses to the question on occupation were coded to the 2010 version of the US Census Bureau occupation numeric codes. 23
cRounded to 1000 and weighted to the state populations of California, Connecticut, Delaware, Florida, Georgia, Hawaii, Idaho, Illinois, Kansas, Louisiana, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Pennsylvania, Rhode Island, South Carolina, Tennessee, Texas, Washington, and Wisconsin using the survey sample weight for each respondent.
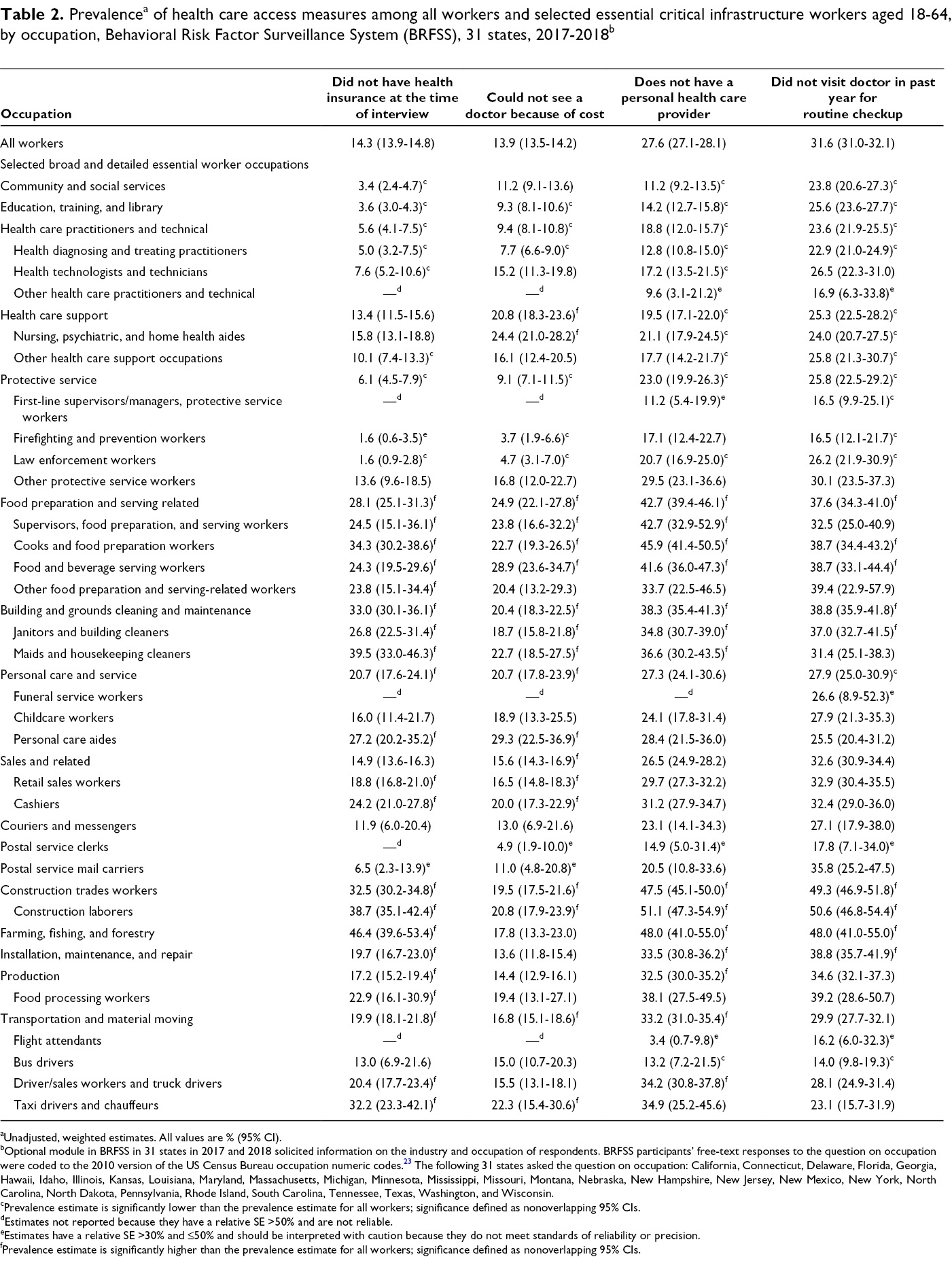
aUnadjusted, weighted estimates. All values are % (95% CI).
bOptional module in BRFSS in 31 states in 2017 and 2018 solicited information on the industry and occupation of respondents. BRFSS participants’ free-text responses to the question on occupation were coded to the 2010 version of the US Census Bureau occupation numeric codes. 23 The following 31 states asked the question on occupation: California, Connecticut, Delaware, Florida, Georgia, Hawaii, Idaho, Illinois, Kansas, Louisiana, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Jersey, New Mexico, New York, North Carolina, North Dakota, Pennsylvania, Rhode Island, South Carolina, Tennessee, Texas, Washington, and Wisconsin.
cPrevalence estimate is significantly lower than the prevalence estimate for all workers; significance defined as nonoverlapping 95% CIs.
dEstimates not reported because they have a relative SE >50% and are not reliable.
eEstimates have a relative SE >30% and ≤50% and should be interpreted with caution because they do not meet standards of reliability or precision.
fPrevalence estimate is significantly higher than the prevalence estimate for all workers; significance defined as nonoverlapping 95% CIs.
The prevalence of all 4 measures of difficulty in accessing health care was significantly higher in 3 broad occupations than among all workers: food preparation and serving related; building and grounds cleaning and maintenance; and construction trades. Three other broad occupations had significantly higher prevalence than all workers for 3 of the measures: farming, fishing, and forestry; installation, maintenance, and repair; and transportation and material moving. Several detailed occupations within these groups also had significantly higher prevalence for multiple measures. In addition, the broad occupation production and 3 detailed occupations within other broad occupations—personal care aides, retail sales workers, and cashiers—had significantly higher prevalences than all workers for at least 2 measures.
Farming, fishing, and forestry workers had the highest prevalence of not having health insurance (46.4%) (Table 2). Personal care aides had the highest prevalence of not being able to see a doctor when needed because of cost (29.3%). Construction laborers had the highest prevalence of not having a personal health care provider (51.1%) and not having had a routine checkup (50.6%).
The prevalence of not having health insurance was more than 30% among respondents in 4 other detailed occupations: maids and housekeeping cleaners (39.5%), construction laborers (38.7%), cooks and food preparation workers (34.3%), and taxi drivers and chauffeurs (32.2%) (Table 2). More than 22% of workers in 6 detailed occupations were not able to see a doctor when needed because of cost: food and beverage serving workers (28.9%); nursing, psychiatric, and home health aides (24.4%); supervisors, food preparation, and serving workers (23.8%); maids and housekeeping cleaners (22.7%); cooks and food preparation workers (22.7%); and taxi drivers and chauffeurs (22.3%). More than 40% of workers in 3 detailed occupations (all in food preparation or serving occupations) lacked a personal health care provider: cooks and food preparation workers (45.9%); supervisors, food preparation, and serving workers (42.7%); and food and beverage serving workers (41.6%).
Some workers in essential occupations had better access to health care than all workers. Broad occupations with significantly higher levels than all workers of access for several measures were community and social services; education, training, and library; health care practitioners and technical; and protective services. Among detailed occupations, the following had the lowest prevalences for various measures: law enforcement workers for being uninsured (1.6%), firefighting and prevention workers for not being able to see a doctor when needed because of cost (3.7%), and bus drivers for not having a personal health care provider (13.2%) and not having had a routine checkup in the past year (14.0%) (Table 2).
Discussion
Keeping the nation functioning during the COVID-19 pandemic requires millions of essential workers, some of whom may be at elevated risk for infection and may need to access needed health care services should they become ill. Our baseline (prepandemic) examination found that adult workers (aged 18-64) in many essential occupations were significantly less likely than the general working population to have full access to health care. Workers in the broad occupations of food preparation and serving related; building and grounds cleaning and maintenance; construction trades; farming, fishing, and forestry; installation, maintenance, and repair; and transportation and material moving had significantly higher prevalences than all workers for at least 3 measures of difficulty accessing health care. Among detailed occupations within other broad groups, personal care aides, retail sales workers, and cashiers had significantly higher prevalences than all workers for 2 measures.
Reports in 2020 identified large numbers of COVID-19 cases among people working in the essential workforce, including several occupations identified in our study. Groups identified to date include health care workers, 26 -30 meatpacking workers, 31 correctional and detention facility staff members, 32 taxi drivers, 29 retail sales workers, 29 housekeepers, 29 construction laborers, 29 public safety workers, 29 and homeless shelter staff members. 33 Among these groups, we observed a significantly higher prevalence than among all workers of difficulty accessing health care services in the following occupations: food processing workers, taxi drivers and chauffeurs, retail sales workers, maids and housekeepers, and construction laborers. We also found some health care and public safety workers had better-than-average access to health care.
Many essential groups of workers face barriers to timely diagnosis and treatment of infection. Numerous studies indicate that not having health insurance and being unable to see a health care provider when needed because of cost are barriers to health care access. 9 Both barriers are more prevalent among adults with low annual household income than among workers with higher income, 7,9,34 because low-wage workers may not have employer-sponsored health insurance 34 -36 or because they are insured but cannot meet out-of-pocket costs. 37 In 2019, the federal poverty level for a family of 4 was $25 750. 38 Many groups of essential workers identified in our study as having difficulty accessing health care had annual mean wages below this level: cashiers, childcare workers, and some food preparation and serving workers. 39 -41 Uninsured adults are more likely than insured adults to have untreated conditions, 9,10,42 -44 and people with preexisting conditions are more likely than people without preexisting conditions to have severe COVID-19. 11,12 Therefore, any limits on access to health care services among uninsured essential workers may decrease their ability to receive treatment for conditions that put them at risk for severe COVID-19. Lack of paid sick leave and transportation may further impede access to health care services. Recent federal legislation passed in response to the COVID-19 pandemic provided temporary paid sick leave for some workers 45 and free testing for SARS-CoV-2 but did not provide comprehensive COVID-19 care or treatment for other new or preexisting medical conditions. 46 Our analysis focused on the pre–COVID-19 pandemic period; if workers in the occupations assessed in our study lost employment and, hence, health care coverage during the pandemic, the estimates presented here might underestimate disparities in health care access today.
Among multiple subgroups of essential workers, risks of exposure to an infection such as COVID-19, combined with barriers to accessing health care services, could delay diagnosis, increasing both the likelihood of severe disease in affected people and the likelihood of disease transmission. 47,48
Limitations
Our study was based on a robust sample of current workers, which allowed analysis of health care access by detailed occupation. However, the findings in this article are subject to several limitations. First, because we wanted to focus on the magnitude of the estimates, we presented crude prevalences; as previously stated, we did not adjust for factors that affect lack of health insurance and underinsurance, data that BRFSS collects. Second, data on several factors that are not collected by BRFSS can influence access to employer-sponsored health insurance, such as employer size and the employee’s citizenship and employment status (full-time, part-time, permanent, temporary, or contract). 6,24,35,49 Third, because some essential workers as defined by DHS do not match census occupation codes, we were not able to estimate their prevalences.
Fourth, additional limitations pertain to the use of survey data. BRFSS data are self-reported and potentially subject to recall bias and social desirability bias. Almost one-sixth (15.6%) of the sample had an uncodable occupation, which could introduce bias to the occupation-level estimates. For the smallest occupation groups, point estimates were imprecise, and some could not be reported. Finally, households without telephones are excluded from BRFSS, and access to health care services varies by household telephone status. However, this limitation should have had little effect on our results, because only an estimated 3.2% of households in 2017 and 3.1% of households in 2018 did not have a telephone. 50,51
Conclusion
In 2017 and 2018, workers in the United States may have had limited access to health care services, at least in part because they did not have health insurance. These workers include many essential workers, who have an important societal role and an elevated vulnerability to infection during the COVID-19 pandemic. Addressing barriers to health insurance coverage and health care services is critical to ensuring the health of essential workers during the COVID-19 pandemic.
Footnotes
Acknowledgments
The authors thank Katrina Bicknaver, Jan Birdsey, Susan Burton, Matt Hirst, Jenny Huddleston, Jeff Purdin, Pam Schumacher, Elizabeth Smith, Marie Haring Sweeney, and Surprese Watts of the Division of Field Studies and Engineering, National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, for their valuable contributions to this study. We are also grateful for the efforts of the BRFSS state coordinators, interviewers, and managers from the 31 states that provided industry and occupation data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.