
Abstract
Objectives:
Lead investigators in North Carolina found evidence that contaminated spices may contribute to children’s elevated blood lead levels. We compared lead levels in samples of spices and other consumable products by country of purchase to inform consumer safety interventions and regulations.
Methods:
From February 1, 2011, through October 22, 2020, North Carolina lead investigators sampled spices and other consumable products from 103 homes of children with confirmed elevated blood lead levels. In 2017, the study team purchased 50 products frequently sampled during lead investigations, as a “market basket” sample, from local stores in or near Raleigh, North Carolina. The State Laboratory of Public Health analyzed 423 product samples using mass spectrometry. We extracted environmental sample results from lead investigations from the North Carolina Electronic Lead Surveillance System.
Results:
The median market basket lead result was 0.07 mg/kg (SD = 0.17); the maximum lead result was 0.88 mg/kg. The median home lead investigation sample result was 0.26 mg/kg (SD = 489.44); the maximum lead result was 6504.00 mg/kg in turmeric purchased in India. Among all samples, products purchased in India had more than triple the median lead levels (0.71 mg/kg) of those purchased in the United States (0.19 mg/kg).
Conclusions:
Purchasing spices in the United States is an action that consumers can take that may reduce their lead poisoning risk. Regulatory agencies should consider a lead limit of <1 mg/kg as attainable for spices sold in US stores and for ingredients of any foods that may be consumed by children.
Lead investigations in New York, Massachusetts, and North Carolina found evidence that contaminated spices may contribute to children’s elevated blood lead levels.1-3 Spices are often grown in countries that still have a large amount of environmental lead contamination due to lead in gasoline and point source pollution from smelters, battery manufacturing plants, and mines. Sellers may also purposefully add vibrant lead-based pigment to increase the visual appeal of spices to customers. 4 Several studies have found that spices purchased in the countries of Georgia, Bangladesh, Pakistan, Nepal, and Morocco contained high levels of lead.2,4,5 The prolonged consumption of lead and other heavy metals can cause damaging neurological health effects and developmental delays in children. 6
In the United States, spices are not typically considered a food widely consumed by children. However, the North Carolina Childhood Lead Poisoning Prevention Program (CLPPP) has collected evidence that some children as young as 6 months of age consume spices as part of their regular diets (North Carolina Electronic Lead Surveillance System [NCLEAD], unpublished investigation reports, February 2011 through October 2020). Turmeric, a commonly adulterated spice, is being used increasingly for medicinal purposes, in beverages, and as a natural colorant for processed foods, including those marketed toward children. 7 Turmeric consumption can range from a few teaspoons monthly to 1 teaspoon daily among children and adults.2,8
Based on an analysis of baby food sampled in the 2017 US Food and Drug Administration (FDA) Total Diet Study, the Environmental Defense Fund estimated that 2.2 million US children had a maximum daily intake lead level that exceeded the current FDA standard. 9 The FDA recently revised its maximum daily intake level of lead to 3 micrograms per day (µg/day) for young children. 6 The FDA action level is 0.05 milligrams per kilogram (mg/kg) for children’s juice and 0.1 mg/kg for candy intended for consumption by children; however, no national standard lead limit exists for spices. 7 Since 2014, the FDA has published import alerts for spices and related products due to lead contamination. 10 Because more than 95% of spices in the United States are imported, enforcing compliance on this food may pose a particular challenge. 11 Because of cost or preference, many families purchase spices or other expensive consumable items overseas or have them sent by family or friends living in other countries. However, these small-scale imports circumvent food inspections intended to ensure that products are safe for consumption before they are sold.
The objective of our study was to explore a feasible lead level goal for spices and compare lead levels among consumable products by country of purchase to inform public health recommendations. We compared lead levels of spices purchased at local grocers with lead levels of spices collected during childhood lead poisoning investigations, and we examined lead levels for all consumable products with known country of purchase.
Methods
Market Basket Survey Samples
An intern purchased 50 spice samples from 9 grocers in or near Raleigh, North Carolina, from August 23 through November 14, 2017. The local lead investigator advised the intern on what brands of spices to purchase for 9 product categories (adobo, asafoetida, chicken tikka masala, chili powder/red pepper, cinnamon, garam masala, tea, turmeric, and whole chili peppers). These target categories were types of spices and other products commonly consumed by families living in the area and often found by the local lead investigator to have elevated lead levels compared with other frequently sampled products. The lead investigator also advised the intern on sampling locations based on where local families reported buying their spices (5 national grocery store chains, 2 small specialty grocery store chains, and 2 independent local specialty grocers). The intern also purchased 3 other products (githeri masala, tandoori masala, and masala–no description) that were excluded from the target category analysis because they could not be matched with investigation samples.
Lead Investigation Samples
Certified lead risk assessors conducted lead investigations and took environmental samples in households of North Carolina children with confirmed elevated blood lead levels to identify the sources of lead exposure. A standard lead investigation in North Carolina consists of an interview with the family about suspected sources of lead and daily activities, lead poisoning prevention education, lead measurements by x-ray fluorescence machines, and sample collection from paint chips, dust wipes, drinking water, soil, and, when applicable, consumable products such as foods or herbal remedies. After the investigation, lead investigators enter or upload investigation reports, sample results, sketches, photographs, and notes into a property record in NCLEAD for surveillance and regulatory purposes.
We extracted environmental lead sample analysis results for spices and other consumable products (n = 689) from NCLEAD for 103 home lead investigations, conducted from February 1, 2011, through October 22, 2020. These samples included other food items outside the target categories, including other spices such as black pepper, cumin, and tamarind. We analyzed environmental sample data, with no link to identifiable information or related biospecimens; therefore, this study did not meet the definition of human research as defined by the National Institutes of Health.
Laboratory and Data Analysis
Using methods described in the 2005 Methods of Analysis of AOAC International, 12 the North Carolina State Laboratory of Public Health incorporated dry ash into the sample, with stepwise heating to 450 °C to remove volatile organic materials, to increase the sample size up to 1 gram. The North Carolina State Laboratory of Public Health then digested the remaining ash material using hot block digestion following the National Institute of Occupational Safety and Health 7303/7082 measurement methods and quantitated the amount of lead by inductively coupled plasma optical emission spectrometry using the US Environmental Protection Agency (EPA) SW-846 6010D measurement method.13-15 Samples with lead levels <15 mg/kg were further analyzed using an inductively coupled plasma mass spectrometer, referencing EPA Method 200.8. 16 Samples were excluded if the lead level was missing from the investigation report, the laboratory analysis method was different than the previously mentioned methods, or the product was grown in the family’s own garden rather than purchased in a store or mailed to the family. Data were analyzed using SAS version 9.4 (SAS Institute, Inc). Descriptive statistics were calculated to compare the distributions of sample results between sample types and by country of purchase. A Wilcoxon 2-sample median test was used to compare the difference between median lead levels by country of purchase and sample type, with α = .05 considered significant. Because of the exponential differences between the minimum and maximum sample results, the authors transformed the data using the natural log (loge) to create the final data visualization on a graph in Tableau Software 2020.2 (Tableau Software, LLC).
Results
From the 9 spice categories examined, 227 samples were collected during lead investigations, and 47 samples were collected during the market basket survey (Table). All 47 market basket survey samples and 94 (41.4%) of the lead investigation samples were from the United States. The remaining lead investigation samples in the spice categories were purchased in India (n = 48, 21.2%), Mexico (n = 3, 1.3%), or an unknown country (n = 82, 36.1%). The median lead sample result from the lead investigations was 0.26 mg/kg (SD = 489.44); the maximum result was 6504.00 mg/kg of lead for a sample of turmeric. For the market basket samples, the median lead sample result was lower (0.07 mg/kg, SD = 0.17); the maximum lead sample result of 0.88 mg/kg was for a sample of tea. The median lead level for investigation samples was significantly higher than the median lead level for market basket samples (t = 12.33; z = −3.61; P < .001).
Lead results (mg/kg) of spices sampled (N = 274), by product and sample type, North Carolina, 2011-2020
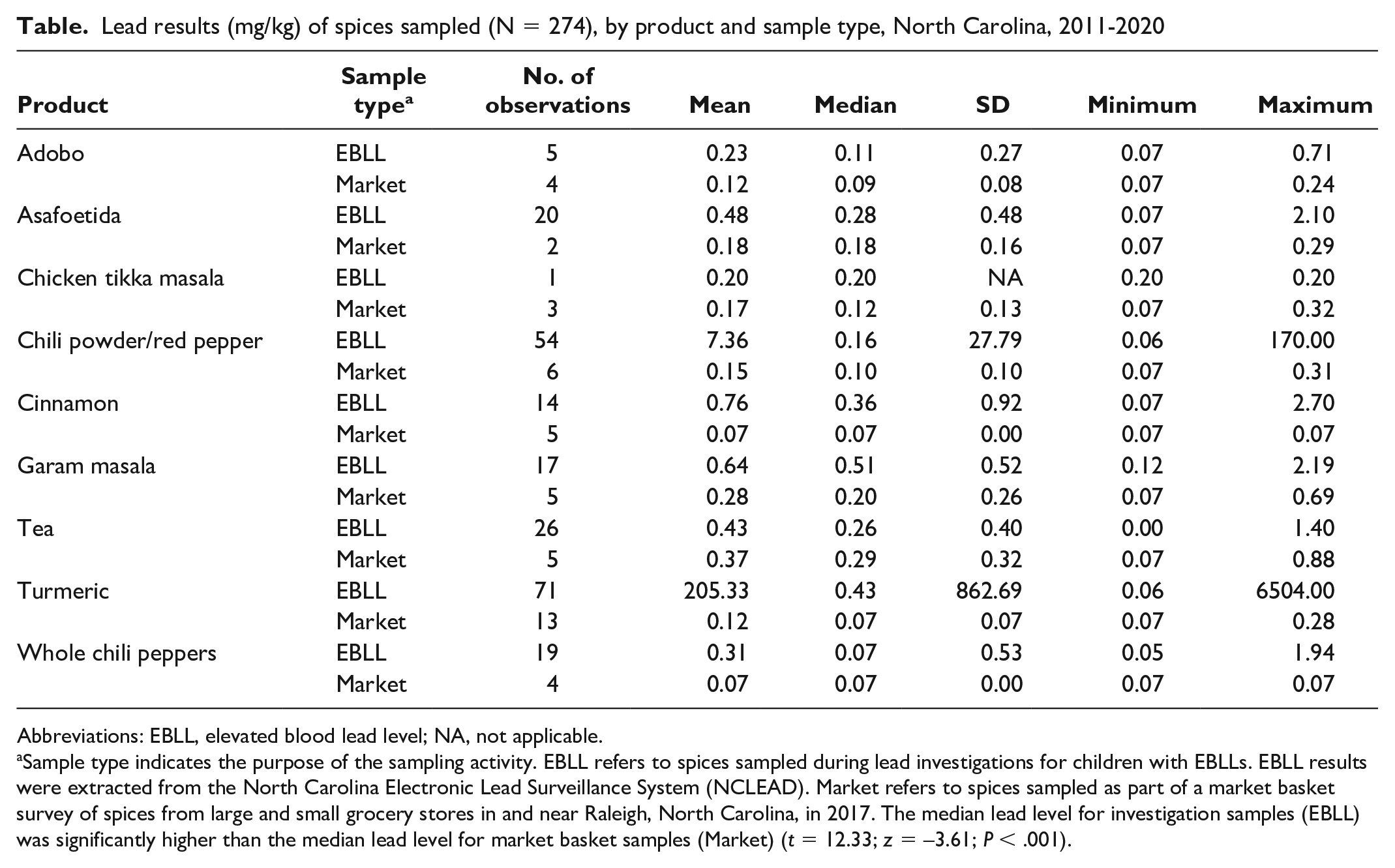
Abbreviations: EBLL, elevated blood lead level; NA, not applicable.
Sample type indicates the purpose of the sampling activity. EBLL refers to spices sampled during lead investigations for children with EBLLs. EBLL results were extracted from the North Carolina Electronic Lead Surveillance System (NCLEAD). Market refers to spices sampled as part of a market basket survey of spices from large and small grocery stores in and near Raleigh, North Carolina, in 2017. The median lead level for investigation samples (EBLL) was significantly higher than the median lead level for market basket samples (Market) (t = 12.33; z = −3.61; P < .001).
Next, we examined the distribution of all consumable product lead sample results with a known country of purchase (n = 423) from all market basket samples (n = 50) and lead investigation samples (n = 373) (Figure 1). For consumable products purchased in India (n = 93), the median lead level was 0.71 mg/kg (SD = 862.69; maximum = 6504.00 mg/kg) compared with a median of 0.19 mg/kg (SD = 1.66; maximum = 25.00 mg/kg) for products purchased in the United States (n = 319), and a median of 0.12 mg/kg (SD = 2.95; maximum = 8.50 mg/kg) for products purchased in Mexico (n = 8). The last 3 samples were purchased in the Dominican Republic (0.71 mg/kg lead) and Egypt (31.00 and 0.62 mg/kg). The median lead level for consumable products purchased in India was significantly higher than the median lead level for products purchased in the United States (t = 57.00; z = 2.47; P = .007).
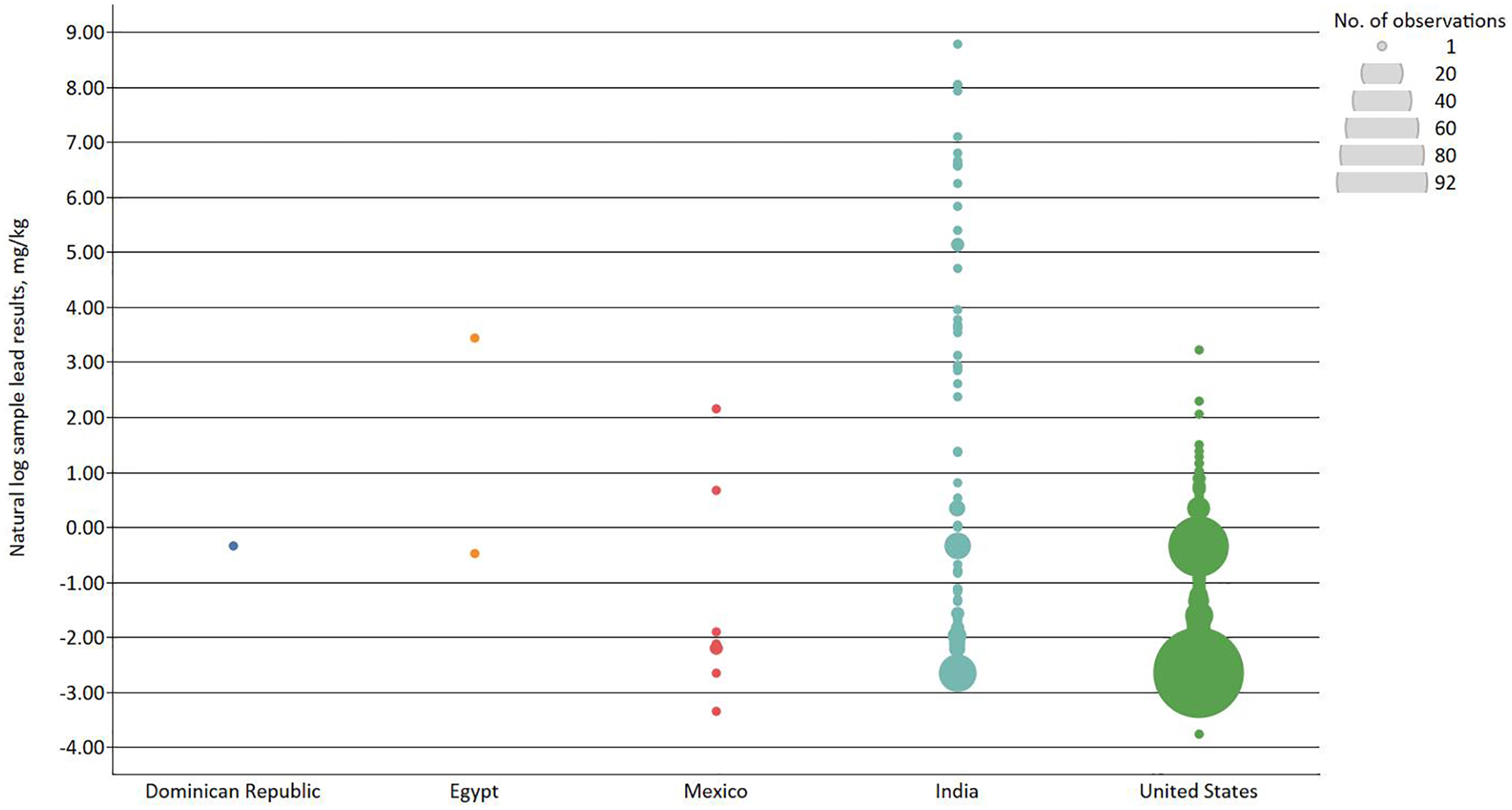
Comparison of natural log-transformed lead levels measured in milligrams per kilogram (mg/kg) for samples of spices and other consumable products (N = 423), by country of purchase. Samples were collected from February 1, 2011, through October 22, 2020, during childhood lead poisoning investigations (n = 373) or were purchased at local grocers (n = 50) in or near Raleigh, North Carolina, as a market basket sample. Circle size indicates the number of sample results at each lead level. The median lead level for consumable products purchased in India was significantly higher than the median lead level for products purchased in the United States (t = 57.00; z = 2.47; P = .007).
Discussion
A 2021 report by the US House of Representatives Committee on Oversight and Reform found that several ingredients used in manufacturing baby food, such as rice flour and spices such as cinnamon, cumin, and turmeric, contained high levels of lead and other heavy metals, exceeding the standards for juice and water; final products were not regularly tested by manufacturers for heavy metal content. 7 Although no federal standard for these metals in baby food or spices currently exists, cumulative exposure to heavy metals may cause developmental delays in young children. 7 Both the FDA and food manufacturers have the responsibility to US consumers to enforce strict product purity guidelines to reduce levels of lead and other heavy metals in food, especially foods marketed toward children.
With this goal in mind, the FDA recently published an action plan for setting heavy metal limits for baby food, titled “Closer to Zero.” 17 One stage of this plan includes determining the feasibility of compliance by the food production industry when deciding action levels for heavy metals in consumable items. 17 We demonstrated the feasibility of finding spices with <1 mg/kg lead when purchased in US stores, using New York State’s Class II recall action level of ≥1 part per million (ppm) of lead, established in 2016, as a guideline. 18 In 2021, New York State announced that it will lower its Class II recall action level for lead in spices to >0.21 ppm effective January 2023, based on exposure and toxicological data, to draw nearer to a health-based reference level, recognizing that no known safe level of lead in humans exists. 18 We found the median level of lead in spices purchased in the United States to be 0.19 mg/kg, suggesting the new action level in New York is likely achievable.
Our results also suggest that spices purchased in the United States have lower levels of lead than spices purchased overseas or sent from family living abroad. Therefore, consumers should buy spices from local stores whenever possible rather than purchasing them from flea markets or internet-based retailers that may not follow standard import procedures. We were unable to assess the importing practices of local stores. However, consumers can take actions to protect themselves, including (1) choosing spices with detailed product labels that allow the products to be traced in the event of a recall or other evidence of contamination, (2) keeping product labeling for foods prone to contamination, (3) signing up for FDA recall alerts and Consumer Product Safety Commission recall alerts for heavy metals, and (4) having young children’s blood lead levels tested annually.19,20
These findings have been incorporated into public health practice in North Carolina. Fliers with a prevention message advising consumers to buy spices locally whenever possible are published on the North Carolina Healthy Homes website in English, Spanish, Burmese, Mandarin, and Hindi. 21 In 2019, the North Carolina CLPPP adopted a reportable lead limit of 1 ppm for spices, modeled after New York State’s Class II recall action level for lead. 18 Lead investigators in North Carolina were trained to record results from spice samples ≥1 mg/kg as an exposure to consumable products containing lead and upload documentation (eg, a spice consumption survey, photographs of the product) into NCLEAD. Lead investigators advised parents to discontinue cooking with the spice. The North Carolina CLPPP epidemiologist is now alerted by NCLEAD when lead investigators have reported a consumable product with elevated lead level. The epidemiologist reports this information to the FDA for further investigation.
Limitations
This study had several limitations. First, samples collected from lead investigations often had missing product labels, whereas the market basket samples were collected by study staff members who deliberately recorded the product origin information and retained the clearly labeled packaging. Therefore, purity could not be compared between product brands because of the small number of samples with product labels and large number of brands represented. Without clear product labeling, lead investigators also cannot report heavy metal contamination to the FDA or other regulatory agencies to trace the source and issue a recall. Unfortunately, product labeling for spices sold in the United States is inconsistent and does not always include information about where the products were grown and manufactured.
Second, insufficient data were available to estimate spice consumption rates or the contribution of lead from contaminated spices to children’s blood lead levels. In late 2018, NC CLPPP implemented the North Carolina Spice and Home Remedy Survey, a survey tool created for lead investigators to gather spice and home remedy consumption data and product information (Figure 2). Since NC CLPPP halted lead investigations during the COVID-19 pandemic and many families refused investigations that were offered, lead investigators have not had many opportunities to administer the survey to families. Still, NC CLPPP has evidence that lead-contaminated spices contributed, at least in part, to many children’s elevated blood lead levels. 1 An analysis of these data could provide estimates of typical spice consumption rates among young children in North Carolina and better estimate the contribution of spices to elevated blood lead levels.

A mother demonstrating for the lead investigator how much of each spice she uses in cooking. During lead investigations, getting product information can be challenging because families often do not have the packaging and do not remember where they purchased the products. Photo credit: Christen Klaus.
Third, whole spice samples were not collected as frequently as ground spice samples; as such, median lead levels could not be compared between the two forms of the same spices. Several studies have linked lead poisoning to repair of grinding machinery used for processing flour.22-24 One turmeric sample included in the analysis, which contained 890 ppm of lead, was grown in India and ground by a relative who used a metal container and hammer to grind the turmeric before sending the spice to the family, who ate it for a year. By the time the source of lead was discovered, the child had a venous lead level of 15 µg/dL, which dropped to 9 µg/dL within 9 months after discontinuing consumption of the turmeric (NCLEAD, unpublished investigation report, 2011). For spices that consumers can purchase unprocessed, such as turmeric, chili peppers, and cinnamon, grinding the spices at home using a food-grade grinder may reduce a potential opportunity for heavy metal contamination.
Conclusion
Future research should examine spice consumption rates among children from various ethnic backgrounds who are living in the United States. In addition, knowing whether contaminant levels differ between ground and whole spices may inform potential interventions to improve processing equipment. Finally, a research question with direct application to consumer interventions is whether cooking methods or acidic ingredients may increase the bio-accessibility of lead from spices, similar to what has been studied with lead in game meat to develop consumer-level interventions for lead poisoning prevention. 25
Footnotes
Acknowledgements
The authors thank North Carolina Child for purchasing, collecting, and submitting the market basket samples for laboratory analysis; Christen “Christy” Klaus for taking the photograph used in this article; the North Carolina State Laboratory of Public Health for analyzing the market basket samples free of charge; the registered environmental health specialists Christy Klaus, Jason Dunn, and Tasharra Kenion for collecting most of the lead investigation samples; Christy Klaus, Ezan Chaudry, and Deidre Bean for assisting with early project development; and Ed Norman, MPH, program manager of the North Carolina Childhood Lead Poisoning Prevention Program, for his continuous support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The North Carolina Childhood Lead Poisoning Prevention Program is supported by funding from the Centers for Disease Control and Prevention (CDC), CDC grant #UE1EH001276-01.