
Abstract
Objectives:
The outbreak of COVID-19 in Massachusetts may have reduced ambulatory care access. Our study aimed to quantify this impact among populations with severely uncontrolled diabetes and hypertension; these populations are at greatest risk for adverse outcomes caused by disruptions in care.
Methods:
We analyzed multidisciplinary ambulatory electronic health record data from MDPHnet. We established 3 cohorts of patients with severely uncontrolled diabetes and 3 cohorts of patients with severely uncontrolled hypertension using 2017, 2018, and 2019 data, then followed each cohort through the subsequent 15 months. For the diabetes cohorts, we generated quarterly counts of glycated hemoglobin A1c (HbA1c) tests. For the hypertension cohorts, we generated monthly counts of blood pressure measurements. Finally, we assessed telehealth use among the 2019 diabetes and hypertension cohorts from January 2020 through March 2021.
Results:
HbA1c testing and blood pressure monitoring dropped considerably during the pandemic compared with previous years. In the 2019 diabetes cohort, HbA1c measurements declined from 44.0% in January–March 2020 (baseline) to 15.9% in April–June 2020 and was 11.8 percentage points below baseline in January–March 2021. In the 2019 hypertension cohort, blood pressure measurements declined from 40.0% in January 2020 to 4.5% in April 2020 and was 23.5 percentage points below baseline in March 2021. Telehealth use increased precipitously during the pandemic but was not uniform across subpopulations.
Conclusions:
Access to selected diabetes and hypertension services declined sharply during the pandemic among populations with severely uncontrolled disease. Although telehealth is an important strategy, ensuring equity in access is essential. Telehealth hybrid models can also minimize disruptions in care.
As COVID-19 spread in the United States, social distancing measures were implemented to control transmission. 1 With the March 2020 outbreak of COVID-19 in Massachusetts, a state of emergency and stay-at-home advisory were put into effect. 2
Although these measures were critical to prevent the acute health care system from being overwhelmed, many Massachusetts ambulatory care providers reduced operations or closed temporarily. As such, access to preventive care and chronic disease management was likely limited. Chronic diseases such as diabetes and hypertension are not only prevalent in Massachusetts (8.4% and 28.1%, respectively) but require ongoing care that may have been disrupted because of the pandemic.3-5
Natural disasters provide a glimpse into the impact of disruptions in health care on hypertension and diabetes management. After Hurricane Katrina in 2005, 1 in 5 people with chronic illnesses affected by the storm reported treatment disruptions, including an inability to obtain medication or see a physician. 6 Populations affected by Superstorm Sandy had proximate increases in acute care use for uncontrolled diabetes. 7 In addition, studies assessing the impact of Superstorm Sandy and Hurricane Katrina reported long-term changes in care use and control of hypertension and diabetes.8-10
Although disruptions in health care caused by natural disasters are different from those caused by a pandemic, these studies have important implications. Analyses conducted early in the COVID-19 pandemic reported reductions in access to hypertension, cholesterol, and diabetes services, which researchers warn may have long-term consequences for population health.11,12 Although rapid deployment of telehealth may have mitigated these early disruptions in care, the current impact of the pandemic on diabetes and hypertension ambulatory care services is not known.13,14 Disruptions in care are particularly salient for populations with severely uncontrolled disease, who are at greatest risk for adverse outcomes.
Our study assessed the impact of the COVID-19 pandemic on access to selected chronic disease management services among populations with severely uncontrolled diabetes and hypertension through March 2021. In addition, we assessed use of telehealth among these populations.
Methods
We analyzed electronic health record (EHR) data from MDPHnet.15-17 MDPHnet queries EHR data from 3 large multidisciplinary care practices and contains data on approximately 20% of the population of Massachusetts.18,19 These care practices include Atrius Health, which serves patients in eastern Massachusetts; Cambridge Health Alliance, which primarily serves urban locations in Boston and Cambridge; and the Massachusetts League of Community Health Centers, which includes data from 20 federally qualified health centers. Data extracts are created from the EHR on a nightly or weekly basis; these extracts include detailed data on health care providers, patients, laboratory results, medications, and visits, including diagnoses. EHR data captured by MDPHnet include data on primary care, specialty care, and behavioral health service encounters generated by any member of the clinical care team with EHR access. Validation of MDPHnet is continuous, including a comparison of data generated from source EHRs with MDPHnet reporting schema. MDPHnet demonstrates agreement with traditional surveillance estimates of the prevalence of chronic disease in Massachusetts. 20
We stratified the analyses by available demographic characteristics, including sex (male, female), age group (18-34, 35-54, 55-75 y), and race and ethnicity (non-Hispanic Asian, non-Hispanic Black, Hispanic, non-Hispanic “other,” non-Hispanic White). The “other” category includes non-Hispanic American Indian/Alaska Native and unknown. We queried data from MDPHnet using structured query language. Because this analysis was conducted for surveillance and did not involve human subjects, MDPH determined no need for institutional review board review.
Glycated Hemoglobin A1c (HbA1c) Monitoring Among Populations With Severely Uncontrolled Diabetes
To determine whether patients with severely uncontrolled diabetes continued to obtain HbA1c tests during the COVID-19 pandemic, we established 3 cohorts of patients, 1 each for calendar years 2017, 2018, and 2019, and then generated aggregate counts of HbA1c tests in the subsequent measurement periods. To establish each of the 3 cohorts, we used the following criteria: active diagnosis of type 1 or type 2 diabetes (International Classification of Diseases, Tenth Revision, Clinical Modification 21 [ICD-10-CM] code of E10 or E11) in the year before the measurement period; most recent HbA1c measurement >9% in the year before the measurement period; and patients aged 18-75 years as of December 31 of the year before the measurement period. We then followed each cohort beginning in January of the subsequent year for 15 months and generated counts of valid HbA1c tests. We aggregated data in 3-month (quarterly) groupings.
We determined that following 3 cohorts was the most robust method for controlling for declines in the frequency of HbA1c tests caused by nonpandemic factors, such as patients better controlling their diabetes over time (therefore, requiring HbA1c tests less frequently) or patients leaving the health care system under surveillance. We designed our algorithms based on current clinical guidelines for patients with uncontrolled diabetes and National Quality Forum measures.4,22,23 We grouped the counts of HbA1c tests in quarterly intervals based on clinical recommendations for follow-up of patients with severely uncontrolled diabetes. 4
Blood Pressure Monitoring Among Populations With Severely Uncontrolled Hypertension
To determine whether patients with severely uncontrolled hypertension continued to have their blood pressure monitored during the COVID-19 pandemic, we established 3 cohorts of patients, 1 each for calendar years 2017, 2018, and 2019, and then generated aggregate counts of valid blood pressure measurements in the subsequent measurement periods. To establish each of the 3 cohorts, we used the following criteria: active diagnosis of primary hypertension (ICD-10-CM code I10) in the year before the measurement period; most recent recorded blood pressure ≥140/90 mm Hg (stage 2 hypertension) in the fourth quarter of the year before the measurement period; and patients aged 18-75 years as of December 31 of the year before the measurement period. We then followed each cohort beginning in January of the subsequent year for 15 months and generated monthly aggregate counts of valid blood pressure measurements. Although these blood pressure measurements were mostly office-based measurements, our analysis also included some self-monitoring of blood pressure (ie, a valid blood pressure measurement associated with a telehealth encounter).
As with the diabetes algorithm, we determined that following 3 cohorts was the most robust method for controlling for declines in the frequency of monitoring caused by nonpandemic factors. We designed the uncontrolled hypertension algorithm based on current clinical guidelines for patients with uncontrolled hypertension and National Quality Forum measures.5,22,23 Although National Quality Forum measures include patients aged 18-85 years, we restricted our analyses to patients aged 18-75 years to align with the diabetes measure. Finally, we used monthly counts of valid blood pressure measurements based on clinical recommendations for follow-up of patients with severely uncontrolled hypertension. 5
Use of Telehealth
Given the rapidly changing landscape of telehealth policy during the pandemic, we assessed recent trends in telehealth use among patients meeting the criteria for the 2019 diabetes cohort and the 2019 hypertension cohort. We followed each cohort from January 2020 through March 2021 and generated monthly counts of patients with a telehealth encounter. To identify telehealth encounters, we analyzed a semistructured field for encounter type using the keywords “televisit,” “telemedicine,” “telehealth,” or “virtual.”
Statistical Analysis
We generated standard time-series plots depicting the percentage of patients from each of the diabetes and hypertension cohorts who obtained an HbA1c test or a valid blood pressure measurement in the respective measurement period. We created graphs in Excel (Microsoft Corp). In addition, we examined recent trends by calculating the difference between the first and last measurement for the 2019 diabetes cohort and the 2019 hypertension cohort. We stratified these data by demographic characteristics to assess disparities in subpopulations.
To assess access to telehealth, we ran 2 series of models: a series for the 2019 diabetes cohort and a series for the 2019 hypertension cohort. The outcome variable of the models was monthly counts of patients meeting cohort criteria with a telehealth encounter. We used negative binomial regression to account for overdispersion and generalized estimating equations with an autoregressive covariance structure to account for serial correlation. The models included age group (reference, 18-34 years), sex (reference, male), race and ethnicity (reference, non-Hispanic White), and month as predictors. We used the overall population counts of the hypertension and diabetes cohorts as offset variables in their respective models. Before running the models, we generated line charts of the data to determine whether models should be restricted to certain periods due to sudden shifts in telehealth use. We elected this approach rather than using knots to facilitate straightforward interpretation of results by subpopulation. We used the Wald χ2 test to determine significance and defined significance as P < .05. We analyzed data using SAS version 9.4 (SAS Institute, Inc).
Results
Populations With Severely Uncontrolled Diabetes
Our analysis identified the following populations meeting the criteria for severely uncontrolled diabetes: 9021 in the 2017 cohort; 9613 in the 2018 cohort; and 9782 in the 2019 cohort. These 3 cohorts were similar in demographic characteristics: the largest proportion of patients was non-Hispanic White (38.4%, 2017 cohort; 37.1%, 2018 cohort; 36.8%, 2019 cohort), male (54.8%, 2017 cohort; 55.2%, 2018 cohort; 55.0%, 2019 cohort), and aged 55-75 years (49.6%, 2017 cohort; 49.6%, 2018 cohort; 49.8%, 2019 cohort). The 2019 cohort was diverse by all measured demographic characteristics (Table 1).
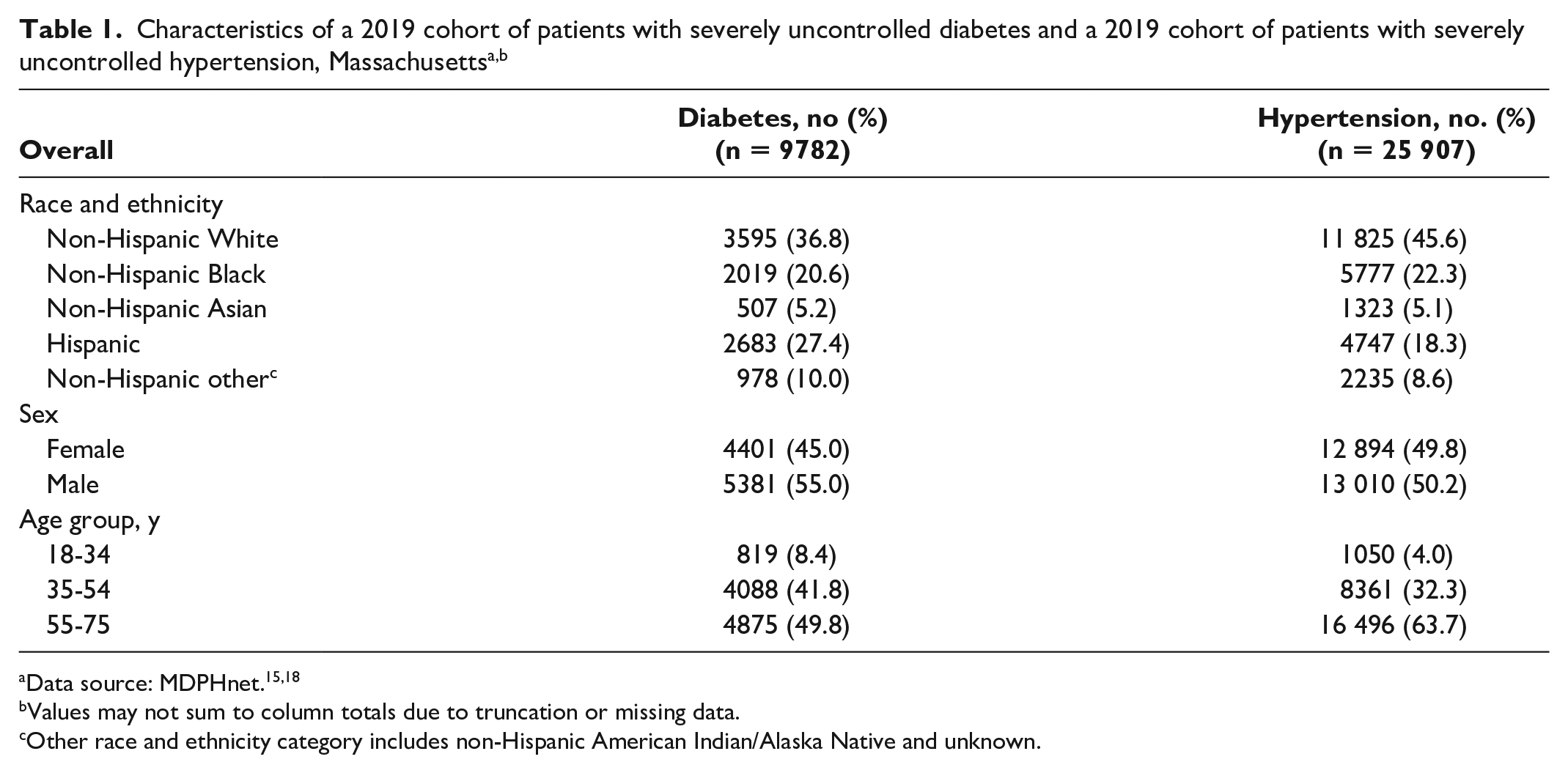
Values may not sum to column totals due to truncation or missing data.
Other race and ethnicity category includes non-Hispanic American Indian/Alaska Native and unknown.
In the time-series plot, the percentage of patients in the 2017 and 2018 diabetes cohorts who obtained an HbA1c test through the 5 quarterly measurement periods (January–March 2018 to January–March 2019 and January–March 2019 to January–March 2020, respectively) was stable (Figure 1). The percentage of patients in the 2019 diabetes cohort who obtained an HbA1c test declined sharply from 44.0% in January–March 2020 (baseline) to 15.9% in April–June 2020; it then increased but remained below the percentage observed in the other 2 cohorts. Overall, the percentage of patients in the 2019 diabetes cohort who obtained an HbA1c test was 11.8 percentage points below baseline in the final measurement period. In addition, all subpopulations in this cohort were below baseline in the final measurement period (Table 2).
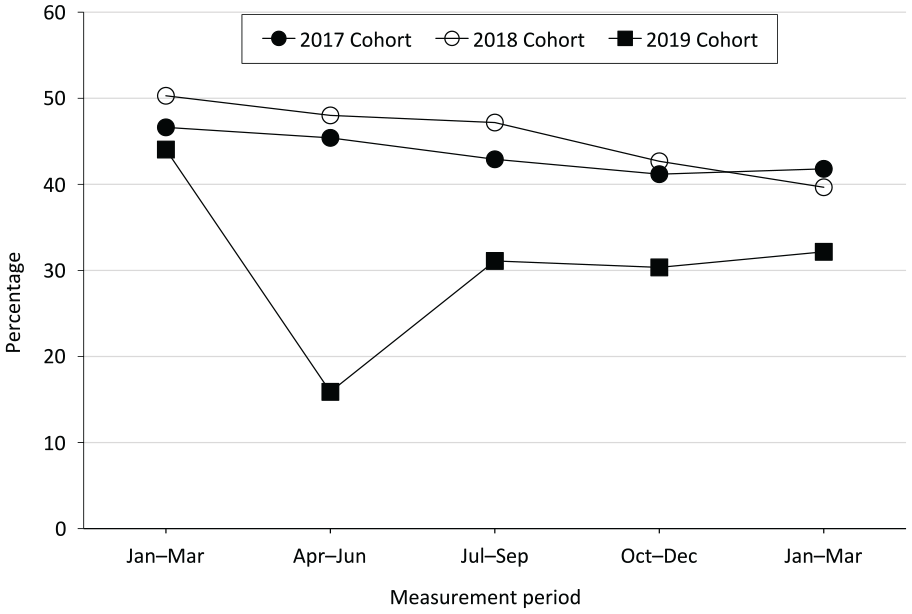
Percentage of adult patients aged 18-75 years in 3 cohorts with severely uncontrolled diabetes who obtained a quarterly glycated hemoglobin A1c test during 5 periods, Massachusetts. The measurement period was January–March 2018 through January–March 2019 for the 2017 cohort (n = 9021), January–March 2019 through January–March 2020 for the 2018 cohort (n = 9613), and January–March 2020 through January–March 2021 for the 2019 cohort (n = 9782). Note that the last measurement quarter of the 2017 and 2018 cohorts overlaps with the first measurement quarter of the subsequent cohort. Data source: MDPHnet.15,18
Differences between the first and last measurement period in the percentage of a 2019 cohort of patients with severely uncontrolled diabetes who obtained a glycated hemoglobin A1c test, by selected characteristics, Massachusetts, 2020-2021 a
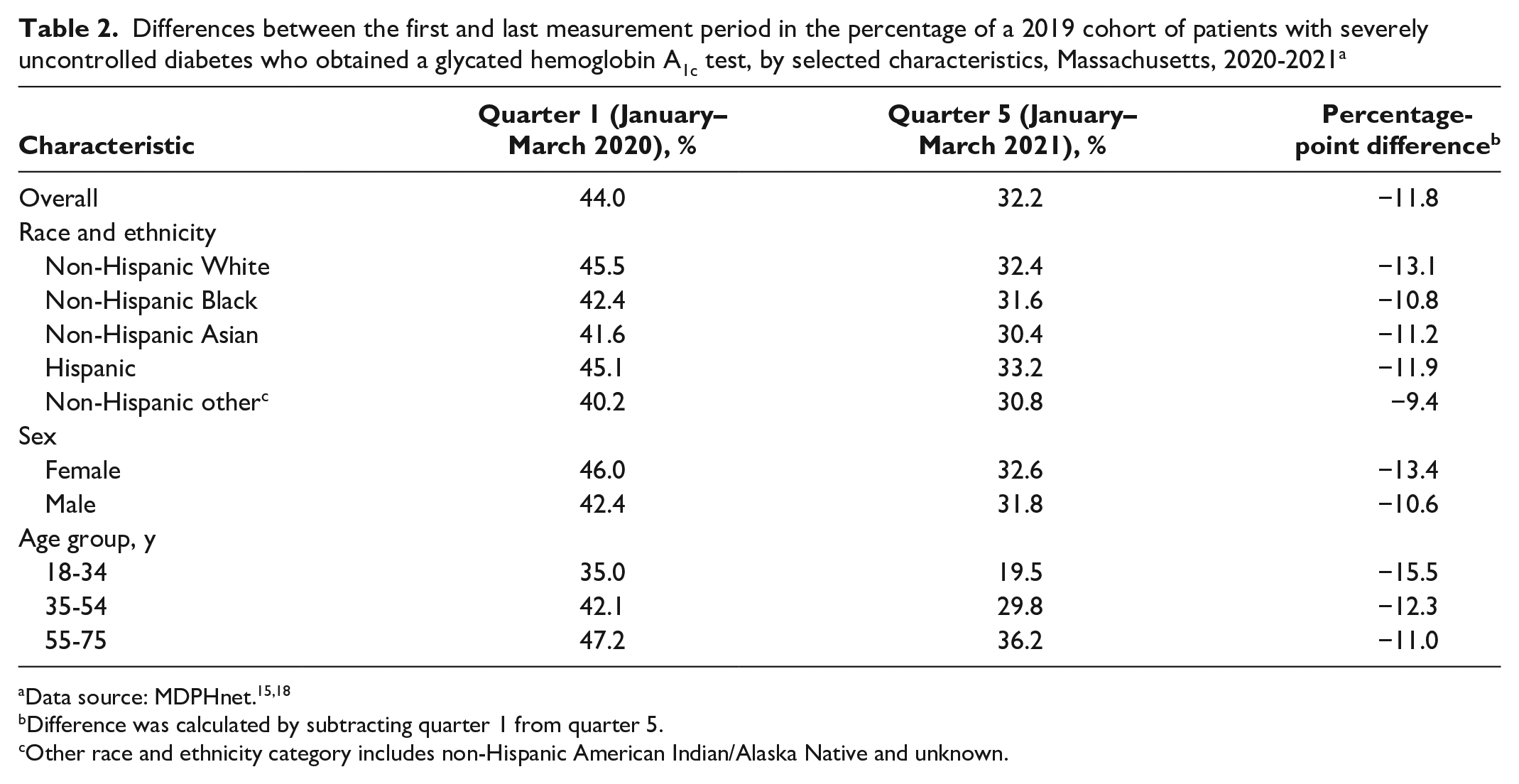
Difference was calculated by subtracting quarter 1 from quarter 5.
Other race and ethnicity category includes non-Hispanic American Indian/Alaska Native and unknown.
Cohort of Patients With Severely Uncontrolled Hypertension
Our analysis identified the following populations meeting the criteria for severely uncontrolled hypertension: 28 805 in the 2017 cohort; 27 994 in the 2018 cohort; and 25 907 in the 2019 cohort. These 3 cohorts were similar in demographic characteristics: the largest proportion was non-Hispanic White (50.4%, 2017 cohort; 48.2%, 2018 cohort; 45.6%, 2019 cohort) and most were aged 55-75 years (64.0%, 2017 cohort; 64.3%, 2018 cohort; 63.7%, 2019 cohort). Sex was nearly evenly split (49.6% male, 2017 cohort; 49.4% male, 2018 cohort; 50.2% male, 2019 cohort). The 2019 cohort was diverse by all measured demographic characteristics (Table 1).
In the time-series plot, the percentage of patients in the 2017 and 2018 hypertension cohorts who obtained a valid blood pressure measurement was generally stable through their respective measurement periods (January 2018–March 2019 and January 2019–March 2020, respectively), except that the percentage of patients in the 2018 hypertension cohort who obtained a valid blood pressure measurement declined in the final measurement month (March 2020) (Figure 2). The percentage of patients in the 2019 hypertension cohort who obtained a valid blood pressure measurement declined sharply from 40.0% in January 2020 (baseline) to 4.5% in April 2020. The percentage then increased but remained below the percentage observed in the other 2 cohorts. Overall, the percentage of patients in the 2019 hypertension cohort who obtained a valid blood pressure measurement was 23.5 percentage points below baseline in the final measurement period in March 2021. In addition, all subpopulations were below baseline in March 2021 (Table 3).
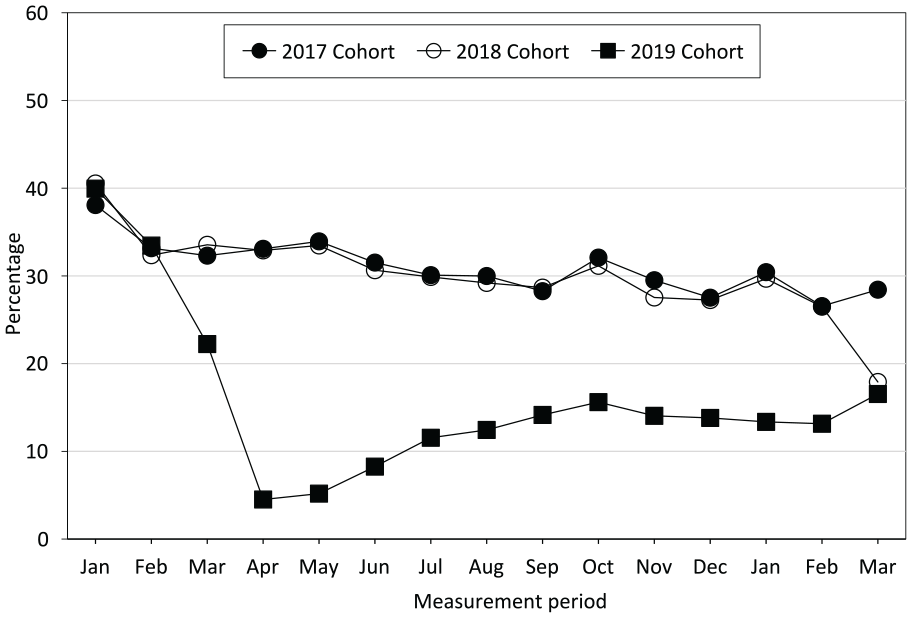
Percentage of adult patients aged 18-75 years in 3 cohorts with severely uncontrolled hypertension who obtained a monthly blood pressure measurement during 15 months, Massachusetts. The measurement period was January 2018 through March 2019 for the 2017 cohort (n = 28 805), January 2019 through March 2020 for the 2018 cohort (n = 27 994), and January 2020 through March 2021 for the 2019 cohort (n = 25 907). Note that the last 3 measurement months of the 2017 and 2018 cohorts overlap with the first 3 measurement months of the subsequent cohort. Data source: MDPHnet.15,18
Differences between the first and last measurement period in the percentage of a 2019 cohort of patients with severely uncontrolled hypertension who obtained a valid blood pressure measurement, by selected characteristics, Massachusetts, 2020-2021 a
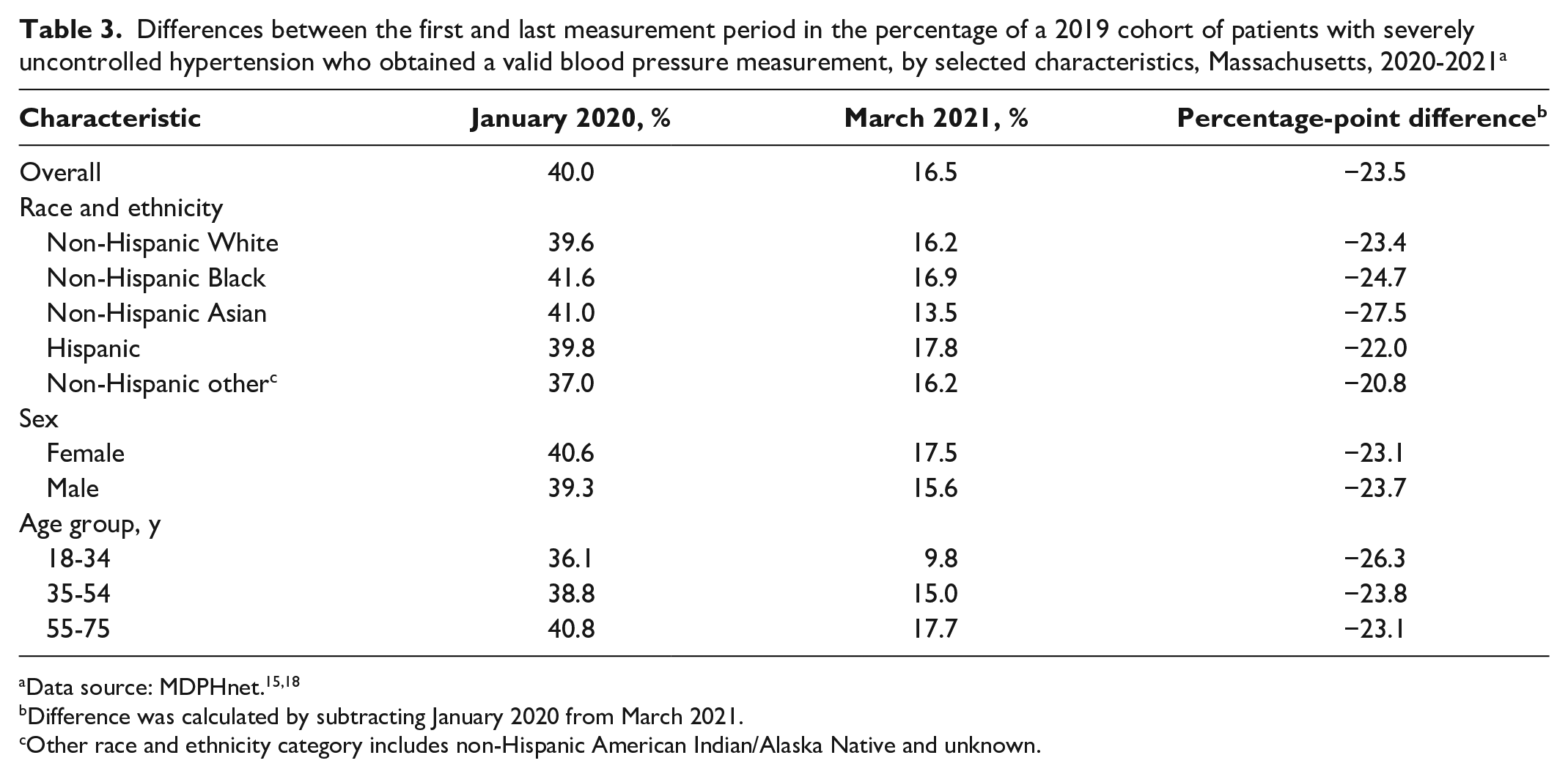
Difference was calculated by subtracting January 2020 from March 2021.
Other race and ethnicity category includes non-Hispanic American Indian/Alaska Native and unknown.
Use of Telehealth
Monthly counts of patients with severely uncontrolled diabetes and hypertension accessing telehealth indicated nearly identical patterns. Few patients accessed telehealth in January and February 2020 (<150 for both months), followed by a precipitous increase through June 2020 (1708 and 3944 for the diabetes and hypertension cohorts, respectively). After June 2020, a minor downward trend began, although telehealth use remained high through March 2021. As such, we ran 1 model for each cohort spanning February–June 2020 and a second model for each cohort spanning June 2020–March 2021.
The models spanning February–June 2020 indicated that female patients were more likely than male patients to access telehealth (diabetes incident rate ratio [IRR] = 1.26 [95% CI, 1.14-1.41]; hypertension IRR = 1.16 [95% CI, 1.05-1.29]). The 35-54 age group (diabetes IRR = 0.71 [95% CI, 0.60-0.84]; hypertension IRR = 0.66 [95% CI, 0.56-0.77]) and 55-75 age group (diabetes IRR = 0.67 [95% CI, 0.56-0.79]; hypertension IRR = 0.58 [95% CI, 0.49-0.69]) were less likely than the 18-34 age group to access telehealth. We found no significant differences by race and ethnicity, except that in the hypertension cohort, non-Hispanic Asian patients were more likely than non-Hispanic White patients to access telehealth (IRR = 1.27; 95% CI, 1.05-1.54).
The June 2020–March 2021 model for the diabetes and hypertension cohorts indicated similar patterns. For both cohorts, female patients used telehealth more frequently than male patients (diabetes IRR = 1.29 [95% CI, 1.19-1.40]; hypertension IRR = 1.15 [95% CI, 1.07-1.24]), and the 35-54 age group (diabetes IRR = 0.78 [95% CI, 0.66-0.92]; hypertension IRR = 0.81 [95% CI, 0.70-0.94]) and the 55-75 age group (diabetes IRR = 0.82 [95% CI, 0.69-0.97]; hypertension IRR = 0.83 [95% CI, 0.72-0.95]) used telehealth less frequently than the 18-34 age group. Finally, in the hypertension cohort, non-Hispanic Black (IRR = 0.87 [95% CI, 0.81-0.95)] and non-Hispanic Asian (IRR = 0.86 [95% CI, 0.78-0.93]) patients were less likely than non-Hispanic White patients to use telehealth, whereas Hispanic patients were more likely than non-Hispanic White patients to use telehealth services (IRR = 1.17 [95% CI, 1.05-1.29]).
Discussion
Our analysis of ambulatory care EHR data in Massachusetts during the COVID-19 pandemic indicates a substantial and sustained reduction in blood pressure monitoring and HbA1c tests among populations with severely uncontrolled disease through March 2021. We observed these reductions in all subpopulations. Although it is reassuring to see that these populations are using telehealth, these data have important implications for mitigating sequelae caused by disruptions in care.
Our findings add to growing concerns about management of chronic disease during the COVID-19 pandemic. A small study found a significant drop in services related to diabetes and cholesterol management through May 2020, including initiation of new medication therapy and testing. 11 Although testing increased over time, the rebound is likely insufficient to account for the backlog of tests generated by delays in care. 11 In addition, a large study conducted at a national laboratory indicated a significant reduction in HbA1c test volumes early in the pandemic. 12 Our findings confirm these observations in a large, diverse patient population using data through March 2021. Further, our analysis assessed populations with severely uncontrolled disease, which magnifies concerns about population-level impact, and simultaneously assessed their use of telehealth.
As such, implementation of approaches to manage diabetes and hypertension during the ongoing pandemic is crucial. Telehealth is an important component of these efforts.24,25 Telehealth enables access to selected services while permitting social distancing, an important benefit given the risk to populations with diabetes and hypertension associated with COVID-19 infection. 26 In addition, self-monitoring of blood pressure and blood glucose can be conducted via telehealth.4,27 The Centers for Medicare & Medicaid Services’ expanded reimbursement for telemedicine visits has been pivotal in expanding the use of telehealth. 13 Also, health systems moved at a remarkable pace to roll out telehealth.24,25,28 The large uptick we observed in our analysis reflects the rapid implementation of telehealth technologies in Massachusetts, which had been essentially a nonexistent component of primary care before the pandemic. 29
However, researchers have raised questions about equity in telehealth. Unfortunately, robust literature on accessibility of telehealth among various populations is lacking, often relying on samples from homogenous and self-selected populations. 30 The limited research on telehealth and equity suggests that patients with limited health literacy and low English proficiency, people of color, older patients, and low-income populations likely face barriers to accessing telehealth. 30 Furthermore, many of these populations are less likely than the general population to have access to resources to participate in telehealth at home, including broadband internet access, a computer, or a smartphone. 31 Likely compounding these barriers is the cost of medical supplies, including blood pressure cuffs and supplies for self-monitoring of blood glucose.32-34 Health insurance coverage of blood pressure cuffs is especially variable and may cost up to $100 out of pocket. 35 Taken together, the populations that are the most socioeconomically marginalized are the least likely to benefit from telehealth. 36
Our findings suggest that the use of telehealth is not uniform; therefore, steps should be taken to ensure equitable access. The Federal Communications Commission’s Connected Care Pilot Program, which supports implementation of broadband connectivity and network equipment to reach populations that are underserved by telecommunication and telehealth services, announced awards in January 2021. 37 In addition, the Health Resources and Services Administration in partnership with the Office of Minority Health awarded funds under the National Hypertension Control Initiative in January 2021. These funds support the purchasing of Bluetooth or wireless-enabled devices for self-monitoring of blood pressure for populations with hypertension that are medically underserved. 38
However, for health centers that do not have such resources or funds, another strategy is hybrid telehealth models, which integrate telehealth components with office-based encounters. For example, health centers can design workflows that triage patients to determine whether the appointment can be delayed, can be accomplished via telehealth visit, or requires an in-person encounter. 39 Patients at highest risk for adverse events caused by disruptions in care can receive priority for office-based visits. 39 Other hybrid telehealth models integrate virtual and in-person components during a single encounter, thereby limiting exposure to infectious disease among patients and frontline staff members. 40 A hybrid model may be an appropriate solution for people uncomfortable with or unable to use telehealth services.
Limitations
Our study had several limitations. First, MDPHnet is not a census and is skewed toward eastern Massachusetts. Second, blood pressure measurements taken outside a clinic may have been undercounted because they were not recorded in the EHR or they were recorded in an unstructured field. Third, an inability to access Current Procedural Terminology codes limited our analysis of telehealth encounters, including assessment of specific services rendered. Finally, data on sociodemographic characteristics in MDPHnet are broad and may mask inequities in HbA1c testing, blood pressure measurements, use of telehealth services, and other related outcomes.
Conclusions
We found a large reduction in blood pressure monitoring and HbA1c tests among patients with severely uncontrolled disease during the COVID-19 pandemic. Continued deployment of telehealth while addressing health equity—especially in populations with limited access to the internet, smart devices, and medical equipment—is an important strategy for monitoring disease. In addition, hybrid telehealth models are a complementary strategy, which can potentially reach populations unable to access telehealth. Acute care data should be monitored for sequelae of uncontrolled hypertension and diabetes, including diabetic ketoacidosis, hypertensive crisis, and myocardial infarction.
Footnotes
Acknowledgements
The authors thank Cambridge Health Alliance, Atrius Health, and the Massachusetts League of Community Health Centers for contributing data to this analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This analysis was funded by the Centers for Disease Control and Prevention under the Improving the Health of Americans Through Prevention and Management of Diabetes and Heart Disease and Stroke cooperative agreement (NU58DP006518).