
Abstract
Objectives:
This study was conducted to assess an intervention that was created by a community–academic partnership to address COVID-19 health inequities. We evaluated a community-engaged bidirectional pandemic crisis and emergency risk communication (CERC) framework with immigrant and refugee populations during the COVID-19 pandemic.
Methods:
A 17-year community-engaged research partnership adopted a CERC framework in March 2020 to address COVID-19 prevention, testing, and socioeconomic impacts with immigrant and refugee groups in southeast Minnesota. The partnership used bidirectional communication between communication leaders and their social networks to refine messages, leverage resources, and advise policy makers. We conducted a mixed-methods evaluation for intervention acceptability, feasibility, reach, adaptation, and sustainability through multisource data, including email communications, work group notes, semistructured interviews, and focus groups.
Results:
The intervention reached at least 39 000 people in 9 months. It was implemented as intended and perceived efficacy was high. Frequent communication between community and academic partners allowed the team to respond rapidly to concerns and facilitated connection of community members to resources. Framework implementation also led to systems and policy changes to meet the needs of immigrant and refugee populations.
Conclusions:
Community-engaged CERC is feasible and sustainable and can reduce COVID-19 disparities through shared creation and dissemination of public health messages, enhanced connection to existing resources, and incorporation of community perspectives in regional pandemic mitigation policies.
Keywords
Crisis and emergency risk communication (CERC) frameworks encourage public participation in pandemic prevention and containment,1,2 but effective implementation depends, in part, on reaching populations with a history of health disparities and limited access to culturally and linguistically tailored health information. Racial and ethnic minority groups have been disproportionately impacted by COVID-193,4 and are susceptible to experiencing communication gaps, 5 compounded by cultural discordance and mistrust of health institutions. 6 These community perspectives have not been well represented in the development and implementation of COVID-19 CERC, leading to reduced agency of communities to address mitigation strategies, thereby contributing to health disparities.7,8 These barriers indicate that a high level of community engagement is needed to reach populations in times of crisis. 1 Community-engaged CERC has the potential to reduce COVID-19 disparities through shared creation and dissemination of health messages, enhanced connection to existing resources, and incorporation of community voices in pandemic mitigation policies. 9
The Centers for Disease Control and Prevention (CDC) has not collected demographic data on citizenship or place of birth for COVID-19 incidence and outcomes, which prevents analysis of national data for pandemic impact on immigrant populations. However, regional studies have demonstrated that immigrant groups experienced disproportionate impacts from COVID-19, including lower testing rates, higher test positivity rates, and higher incidence rates than non-immigrant groups.10,11 Studies from other high-income countries have demonstrated high mortality attributed to COVID-19 among immigrant groups.12,13 Refugees to high-income countries have experienced amplified barriers to health care, economic support, education, and social support during the pandemic. 14 Taken as a whole, immigrant groups in the United States are disproportionately susceptible to COVID-19 and its complications because of limited English proficiency, low access to health care, fear of legal repercussions, employment in sectors where remote working is not possible, and crowded living conditions. 15 Likewise, immigrant groups are susceptible to economic fallout from the pandemic, including loss of employment, lower access to unemployment benefits, and food and housing insecurity. 15 Finally, some immigrant groups face the compounding impact of xenophobia 16 and raids on immigrant communities. 17
Community-engaged research (CEnR) partnerships are uniquely positioned to operationalize pandemic CERC among groups at risk for health disparities, including immigrants and refugees. CEnR partnerships, characterized by collaboration between community members and researchers through all phases of research, are increasingly ubiquitous in the United States. 18 They have organizational and technical capacity for interfacing with target populations in a research and evaluation context. 19
This study includes the description of a 17-year CEnR partnership adopting a bidirectional CERC framework in March 2020 to address COVID-19 prevention, testing, and socioeconomic impact in immigrant and refugee groups in Olmsted County, Minnesota, where 14% of the population is documented as non–US-born. 20 Bidirectional communication between communication leaders and their social networks was used to refine messages, leverage resources, and advise policy makers. We previously described our experience with the first 14 days of the intervention in March 2020, during which messages were delivered by 24 communication leaders in 6 languages across 9 virtual platforms to 9882 immigrants and refugees within their networks. 21 Here, we present an in-depth, mixed-methods evaluation of the intervention after 9 months of implementation, focusing on acceptability, reach, perceived efficacy, and sustainability.
Methods
CEnR Partnership Narrative
In 2004, a community–academic partnership developed between Mayo Clinic and an adult education center that primarily serves people of color, most of whom are new immigrants and refugees. This partnership matured by formalizing operating norms, adopting community-based participatory research principles, and adding partners from multiple sectors. 22 Rochester Healthy Community Partnership (RHCP) developed an effective community-based research infrastructure that has facilitated extensive research training for community partners.23,24 RHCP adapted an empirically derived community-based participatory research conceptual model through in-depth evaluation. 25 Community and academic partners jointly conduct every phase of research, disseminate results, implement sustainability plans together, and coauthor scientific products (eg, articles, presentations, policy briefs).26-28
At the start of the COVID-19 pandemic, RHCP community partners observed that credible COVID-19 information was not reaching immigrant communities. In March 2020, RHCP formed a community-based COVID-19 work group and adopted the CDC CERC framework for co-creation of an intervention targeting African and Hispanic immigrant populations. The work group consisted of 24 communication leaders representing 6 ethnic and community partner groups (Somali, Anuak, Cambodian, Hispanic, Ethiopian, and South Sudanese), academic partners, and county and city officials. All intervention components were informed directly by community priorities, and RHCP community partners co-created the intervention framework and evaluation strategy. Initially, communication leaders volunteered their time with RHCP. As funding was secured for the initiative, communication leaders were compensated for their time.
Intervention Framework
The intervention included communication and health assessment strategies driven by bidirectional CEnR (Figure 1). Communication strategies centered on COVID-19 message maps, 29 jointly developed by RHCP community and academic partners across 3 constructs: COVID-19 prevention and containment, SARS-CoV-2 testing, and social and economic impacts of COVID-19. Communication leaders were recruited by RHCP community partners to deliver messages. COVID-19 messages were delivered by bilingual communication leaders in their social networks. Because of physical distancing, messages were mostly delivered virtually. Communication leaders used the channels most appropriate for their communities (eg, voice calls, text messaging, social media). Recipients were encouraged to amplify messages to their social networks. Communication leaders solicited feedback on health and socioeconomic concerns through the same platforms. Communication leaders and RHCP partners had regular teleconferences (daily, then biweekly, now weekly) for 3 purposes. First, communication leaders shared their progress on emerging best practices. Second, message refinement and generation of new messages was achieved in response to community feedback and rapidly changing facts. Third, questions were answered in real time by infectious disease experts (academic partners) or community resource experts (community partners). Feedback was used to inform regional decision makers.
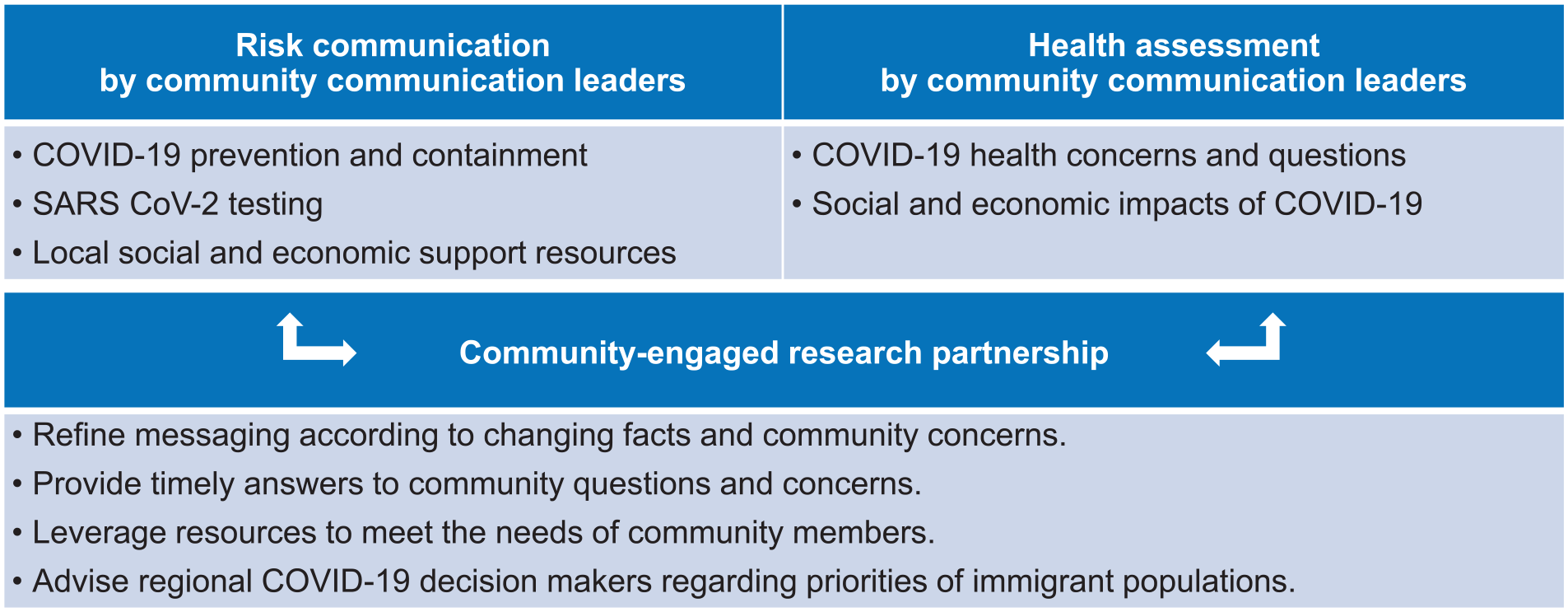
Bidirectional COVID-19 crisis and emergency risk communication framework. Adapted from Wieland et al. 21
Program Evaluation
To assess the forces that shaped intervention implementation, we conducted a mixed-methods evaluation of acceptability, feasibility, reach, adaptation, and sustainability. The evaluation interval was March 2020–January 2021 (9 months).
Data Sources
Emails
Email communication between members of the RHCP COVID-19 work group was accessed on the email platform used by academic, public health, and community partners to provide information about community resources and related information and updates. As of January 2021, 63 RHCP partners were on the email platform. Email content included new and revised COVID-19 co-created messages, questions and concerns about COVID-19 or work group processes (representing questions from social network members), and information about new and evolving community resources. All emails from March 2020 through January 2021 were collated for analysis.
RHCP COVID-19 work group meeting notes
During work group meetings, communication leaders shared their progress in disseminating messages, as well as concerns and questions curated from their social networks. Problem solving occurred in real time. Meetings were recorded and notes were taken.
Reflection interviews
Guided virtual reflections 30 with communication leaders were used to understand the intervention process as it unfolded. Reflections started as weekly interviews and later evolved into biweekly meetings that documented events across the life cycle of the intervention efforts, capturing information on context and unfolding processes for dissemination, adaptation, and improvement ideas. The reflection interview guide was developed based on relevant evaluation (adaptation, feasibility, acceptability, and sustainability) and CEnR constructs18,31 (motivations, partnership and engagement, empowerment and participation). Communication leaders were asked about key factors that facilitated or impeded the implementation and delivery process. Twenty communication leader reflection interviews were conducted: Somali (n = 5), South Sudanese (n = 3), Hispanic (n = 4), Cambodian (n = 5), and Ethiopian (n = 3). All reflections were audio recorded and notes were taken.
Postimplementation focus groups
To assess the perceived effectiveness and sustainability of the intervention from the communication leaders’ point of view, 3 focus groups representing 6 language groups were conducted. A focus group guidebook included questions on evidence of success, perceived efficacy and feasibility, sustainability, and opportunities for scalability, following previous study methods.32,33 Focus groups were recorded, transcribed, and reviewed.
Communication leader tracking sheets
Each communication leader completed a weekly tracking sheet, which included structured and open-text fields to document intervention reach and engagement activities using various mediums and communication mechanisms. All tracking sheets were collated into a spreadsheet for analysis.
Program sustainability was explored throughout the intervention from all data sources listed previously to understand sustainability and scalability concepts in the community-engaged COVID-19 CERC framework for tailored intervention.
Data Analysis
We analyzed qualitative data using a rapid analysis approach,34-36 whereby we summarized each data source using a template of domains and then generated matrices from the summaries. For data domains, we generated matrices from summaries of emails, reflection interviews, and meetings. Themes and directions for further intervention refinement were identified and categorized into key activities of communication leaders, community response and concerns, strategies that were working, new strategies to be adapted, and recommendations from the work group. Tracking sheets were collated; reach and engagement were quantified by language groups and communication mediums using descriptive statistics.
A final stage of confirmatory analysis was established by a participatory interpretation approach via 3 consecutive “data walk” (an interactive way for community partners to engage with research findings)37,38 presentations with academic partners and communication leaders. Results from multiple data domains were presented within the framework of process evaluation adapted from Moore and colleagues 39 to achieve a robust analysis and understanding of intervention efforts, implementation processes, and mechanisms of impact (Figure 2). Data walks were presented according to each data domain (work group meetings, reflection interviews, emails, and tracking), which allowed the study team to consider all aspects and implications and to adjust intervention efforts while making recommendations intentional and enriching the CEnR process. A list of observations and suggestions was compiled to refine and reframe data for subsequent data walks. As a result, study findings encompassed the evolution of work group efforts as the pandemic progressed, as well as framework dissemination and the relational engagement and empowerment that were otherwise challenging to quantify.
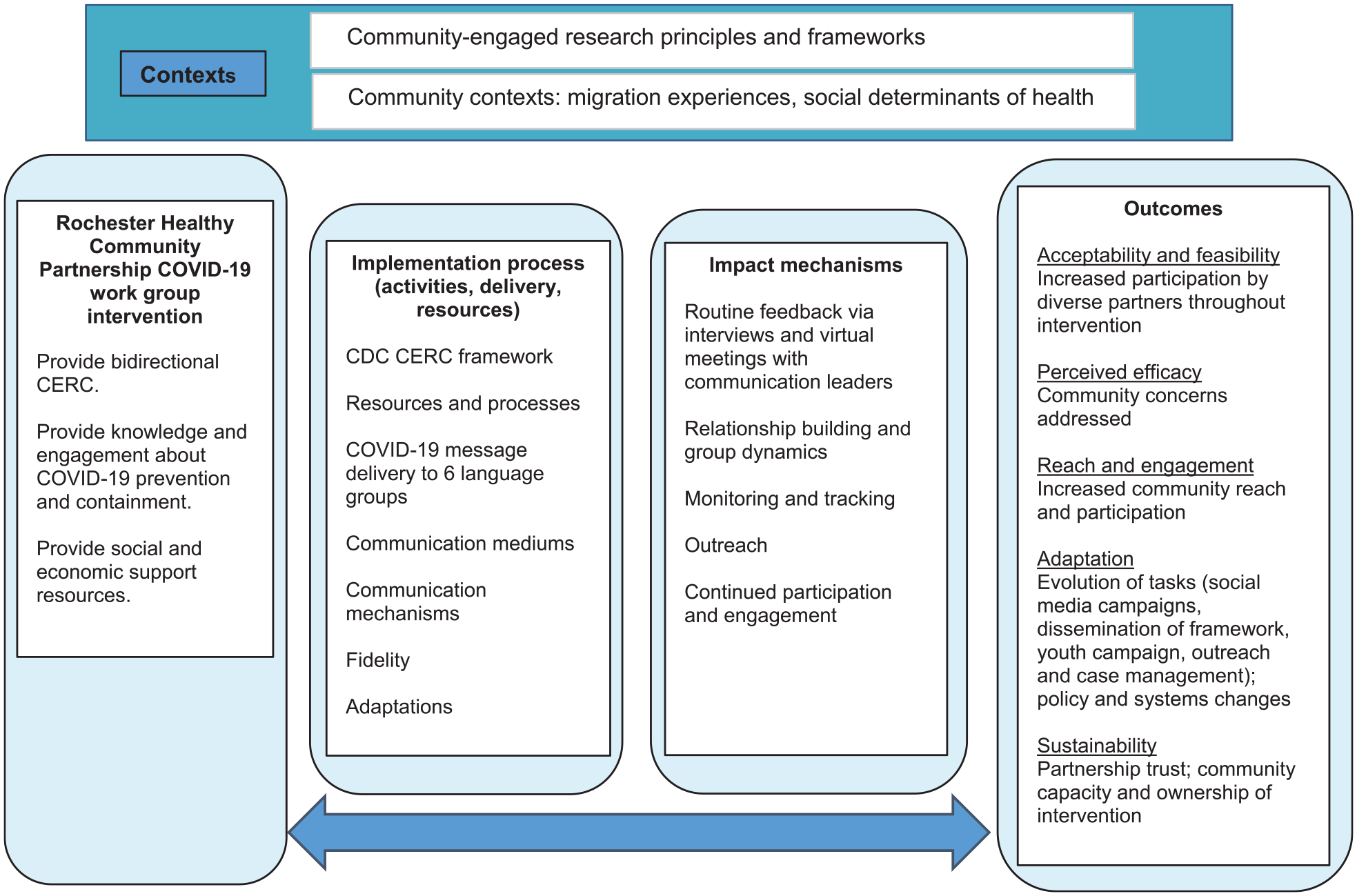
Process evaluation for assessing community-engaged research partnerships for crisis and emergency risk communication (CERC) to immigrant and refugee populations during the COVID-19 pandemic. Adapted from Moore et al. 39 Abbreviation: CDC, Centers for Disease Control and Prevention.
Results
Findings and outcomes resulted from more than 400 emails, summaries of 32 recorded work group meetings, 20 reflection interviews, and 3 postimplementation focus groups.
Acceptability, Feasibility, and Perceived Efficacy
Communication leaders had overall positive perceptions about the RHCP COVID-19 intervention. They indicated that RHCP was a trusted and credible information source of COVID-19 information. Community members became well informed on COVID-19 and learned how to take precautionary measures to protect themselves and their community. Continued engagement in work group meetings, which received a wide range of representation from the community, attendance from public health experts, city and county officials, and neighboring county officials, occurred over time.
The intervention was implemented as intended. Feasibility was supported by documentation of strategies for implementation, which were mapped to the CDC CERC framework and reported previously. Community concerns addressed through real-time access to RHCP partners and government officials included unemployment issues, economic burdens, and strategies to reach particularly hard-to-reach populations (eg, elderly members of the community who resided alone). Addressing these concerns enhanced the community’s information-seeking behaviors as community members looked to their community leaders and RHCP for assistance on COVID-19–related information.
Reach and Engagement
During a 6-month period, COVID-19 messages were delivered by 24 communication leaders in 7 languages (Somali, Anuak, Khmer, Amharic, Arabic, Spanish, and English) to 6 ethnic groups’ (Somali, Hispanic, Cambodian, Anuak, South Sudanese, and Ethiopian) social and individual networks using various mechanisms and mediums (Table 1). The intervention delivered to targeted populations reached 39 875 people. Communication leaders said that messages delivered in their native languages reached a wide range of audience members who would otherwise not have received information. Interview data showed that social media reach (estimated number of people who were exposed to messages) was higher than engagement (estimated number of people who acted on the content) (Table 1). Communication leaders reported that social media engagement was not an accurate reflection of how community members engaged with the intervention, as many community members did not engage on social media platforms. However, communication leaders reported that community members frequently acknowledged (via text message, telephone call, etc.) seeing the messages and acting on a resource or suggestion from the message.
Reach and engagement of a bidirectional COVID-19 crisis and emergency risk communication intervention among immigrants and refugees, by language group, Minnesota, March 2020–January 2021
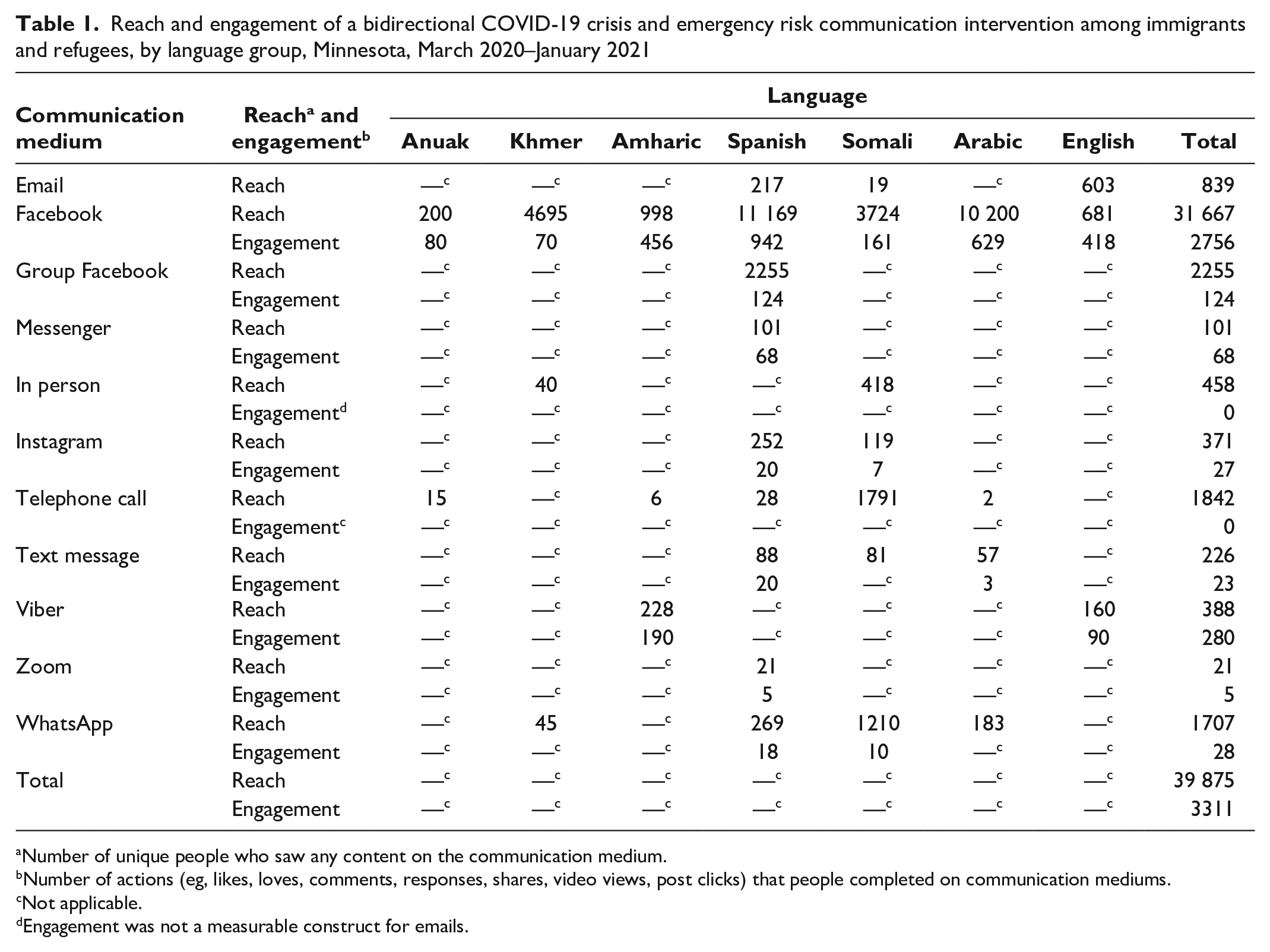
Number of unique people who saw any content on the communication medium.
Number of actions (eg, likes, loves, comments, responses, shares, video views, post clicks) that people completed on communication mediums.
Not applicable.
Engagement was not a measurable construct for emails.
Interviews and focus group data demonstrated that elements of engagement and growth were seen for individual communication leaders by spending time forging relationships with other communication leaders as they reached out to each other for support to address community concerns. Communication leaders became more engaged, motivated, and empowered to provide consultations in their communities knowing they had direct access to peers and health experts.
Adaptation
Interviews and focus group data showed that reflection interviews, emails, and work group meetings provided real-time feedback to refine messaging, streamline processes, and curate community concerns. Feedback resulted in changes to intervention processes and improvements in provision of essential services (food, housing, health). Communication leaders learned through the process how to reach their communities and networks using different mediums and messaging styles. Although social media platforms worked for some, others noted that direct conversations, face-to-face communication, and telephone calls had more impact.
Sustainability
During a 9-month period, sustainability was facilitated by commitment to partnership history and bidirectional communication between communication leaders and academic partners, as well as by the development of work groups that focused on evolving needs. These work groups included a message creation work group; RHCP COVID-19 social media group to supplement communication leader dissemination at the level of individual social networks; RHCP COVID-19 coalition that focused on outreach to adolescents and young adults; and a work group to connect COVID-19–positive patients to an RHCP-partnered community-based organization for assessment and provision of essential services. Communication leaders attested that they now feel prepared for future pandemics (Table 2).
Outcomes and exemplar quotes from a bidirectional COVID-19 crisis and emergency risk communication intervention among immigrants and refugees in Minnesota, March 2020–January 2021
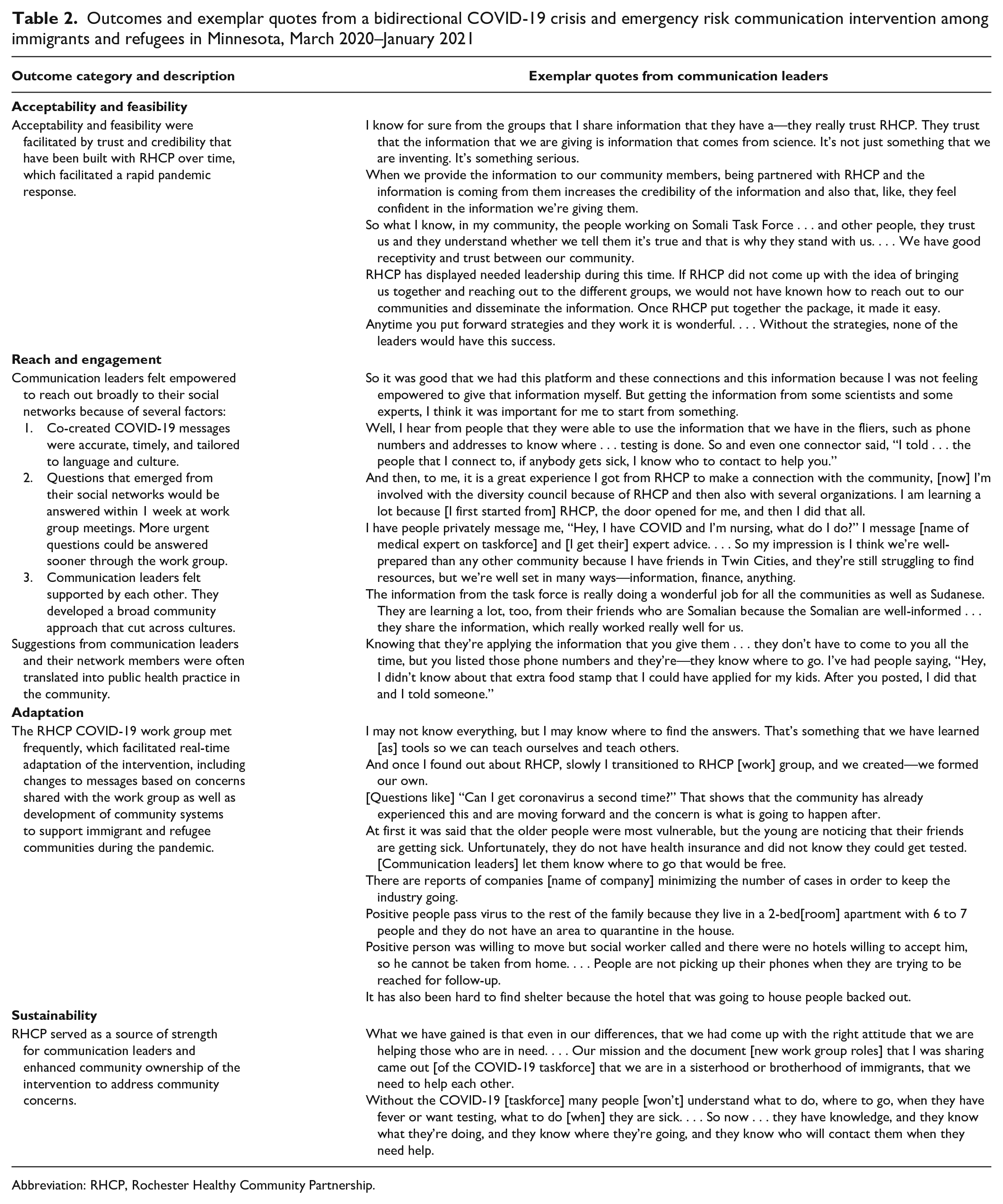
Abbreviation: RHCP, Rochester Healthy Community Partnership.
RHCP served as a source of strength for communication leaders, enabling community ownership of the intervention. The intervention facilitated a sense of empowerment in addressing community concerns. Opportunities to improve sustainability included the following:
Consistent funding to support communication leaders’ work and recruit more communication leaders.
A simplified tracking system with less time burden for communication leaders.
Defined roles and expectations for communication leaders and community partners early in the process.
Creation of a system/database that captures and documents community concerns, solutions, and resources in real time.
Building on existing RHCP trusting relationships to expand outreach efforts via other networks to avoid overlapping community efforts.
Discussion
This mixed-methods program evaluation described the feasibility, acceptability, reach, perceived efficacy, and 9-month sustainability of a community-engaged bidirectional CERC intervention with immigrant and refugee populations during the COVID-19 pandemic. Because sociocultural factors, personal control, trust in institutions, and multisource misinformation all shape reception of CERC messaging, 40 we also documented adaptations to the intervention that occurred in real time to account for the rapidly changing externalities throughout the pandemic. This study addresses a gap in the literature about ways community partnerships may plan for and implement pandemic CERC. The study also focused on CERC with immigrant and refugee populations that have been disproportionately impacted by the COVID-19 pandemic and face unique barriers to pandemic messaging and collaboration with health institutions.
The results of interviews and focus groups demonstrated high acceptability and perceived efficacy of the intervention framework. RHCP partners adopted a CERC framework, co-created messages with community partners and health experts, and modified messages regularly, which led communication leaders to feel supported in disseminating accurate messages to their networks. Frequent communication between community and academic partners allowed the team to respond rapidly to concerns and obstacles. The bidirectional communication facilitated connection of community members to resources through group-based troubleshooting. For example, the need for masks, food, and information about accessing unemployment benefits was addressed by community experts. Finally, bidirectional communication led to systems and policy changes to meet the needs of immigrant and refugee populations. For example, expressed community concerns influenced regional SARS-CoV-2 testing (and, later, vaccination) policies for patients with limited English proficiency. Likewise, a regional system was created that linked patients with limited English proficiency who received a positive test result for SARS-CoV-2 to a community-based organization that works with immigrant groups collaborating with county officials on provision of essential services. In these ways, our study provides details about how previously described best practices for pandemic CERC (from the 2009 influenza pandemic) may be applied with populations at risk for health disparities. 41
This study demonstrated 9 months of intervention sustainability, which has now exceeded 12 months. Sustainability of interventions beyond grant funding is challenging.19,42 Barriers to sustainability include time demands, limited resources, and maintaining morale and energy for CEnR. 42 However, a strong and enduring partnership can be an important facilitator for sustainability of CEnR interventions. 43 Integration of interventions into existing programs, partnership capacity building, and community ownership of interventions are also important facilitators for sustainability. 19 The intervention in our study was built on the foundation of an experienced CEnR partnership.25,26,44 Frequent communication between communication leaders and academic partners, and the broader community acceptance of RHCP as a reliable source of health information, helped to sustain the intervention. One communication leader noted, “Without the COVID-19 [work group] many people [won’t] understand what to do, where to go when they have fever or wanted testing, what to do [when] they are sick. . . . So now . . . they have knowledge, and they know what they’re doing, and they know where they’re going, and they know who will contact them when they need help.”
CEnR partnerships focused on achieving health equity goals are increasingly common. 18 Our study showed that they are uniquely poised to respond to pandemic communication needs through ready access to disease content expertise from academic partners and community expertise from community partners that includes community capacity for evaluation and data collection. Processes and products from this bidirectional CERC framework may be adapted by other CEnR partnerships to meet local needs. As examples, the framework has been adapted by partnerships in Minnesota, Florida, and Mississippi. 45 Future directions include the development of a toolkit for community-engaged CERC for pandemic preparedness with populations at risk for health inequities.
Limitations
This study had several limitations. First, dissemination of messages beyond the initial distribution from communication leaders was not quantified. Therefore, the full intervention reach could not be assessed across social networks (message amplification). Second, the number of people reached by communication leaders may have been overestimated if people received messages from more than 1 communication leader via overlapping networks. On the other hand, the tracking sheets substantially underestimated true reach and engagement because of low completion rates by communication leaders. Third, we did not assess risk-related behaviors and outcomes, which limits quantitative conclusions about intervention impact. Finally, CEnR partnership work is highly contextual; as such, this process may not be generalizable to some partnerships.
Conclusion
Community-engaged CERC is feasible, sustainable, and effective in reducing COVID-19 disparities through shared creation and dissemination of public health messages, enhanced connection to existing resources, and incorporation of community voices in regional pandemic mitigation policies.
Footnotes
Acknowledgements
The authors thank the RHCP partners who contributed to the organization, implementation, and dissemination of this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by Clinical and Translational Science Awards grant no. UL1 TR000135 from the National Center for Advancing Translational Science and the Mayo Clinic Center for Health Equity and Community Engagement Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health. The funding bodies had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the article; and in the decision to submit the article for publication.