
Abstract
Objectives:
Although a known association exists between stress and alcohol consumption among health care workers (HCWs), it is not known how the COVID-19 pandemic has affected this association. We assessed pandemic work-related stress and alcohol consumption of HCWs.
Methods:
We emailed a cross-sectional, anonymous survey in June 2020 to approximately 550 HCWs at an academic hospital in New Orleans, Louisiana. HCWs from all departments were eligible to complete the survey. Questions measured work-related stress and emotional reactions to the pandemic (using the Middle East Respiratory Syndrome [MERS-CoV] Staff Questionnaire), depressive symptoms (using the Patient Health Questionnaire–9 [PHQ-9]), coping habits (using the Brief COPE scale), and pre–COVID-19 (March 2020) and current (June 2020) alcohol consumption. We measured alcohol consumption using the Alcohol Use Disorders Identification Test–Consumption (AUDIT–C), with scores >3 considered positive. We asked 4 open-ended questions for in-depth analysis.
Results:
One-hundred two HCWs participated in the survey. The average AUDIT–C scores for current and pre–COVID-19 alcohol consumption were 3.1 and 2.8, respectively. The level of current alcohol consumption was associated with avoidant coping (r = 0.46, P < .001). Relative increases in alcohol consumption from March to June 2020 were positively associated with PHQ-9 score and greater emotional reactions to the pandemic. Availability of mental health services was ranked second to last among desired supports. Qualitative data demonstrated high levels of work-related stress from potential exposure to COVID-19 and job instability, as well as social isolation and negative effects of the pandemic on their work environment.
Conclusions:
Ongoing prevention-based interventions that emphasize stress management rather than mental or behavioral health conditions are needed.
Among health care workers (HCWs) responding to the COVID-19 pandemic, increased stress, which manifests as symptoms of depression, anxiety, insomnia, and distress, has been noted worldwide.1,2 Known stressors for the COVID-19 pandemic include excessive work hours, witnessing COVID-19 deaths, fear of infection, and inadequate personal protective equipment (PPE). 3 A 2020 systematic review of the literature indicated worsening of mental health results from these experiences, with high levels of general psychological distress and vicarious trauma. 4 Such findings recapitulate work after the 2003 outbreak of severe acute respiratory syndrome (SARS) 5 and the 2014 Middle East Respiratory Syndrome (MERS) outbreak. 6 Factors contributing to increased mental health morbidity among HCWs during these previous outbreaks included threat of contagion, fear of infecting family members and colleagues, and stigmatization in their home communities.7,8 These same factors are also associated with increased experiences of burnout among HCWs, with resident physicians and nurses experiencing the highest risk.9,10
During any pandemic, traditional outlets for stress reduction (eg, gyms, parks) may have limited accessibility. Potential stressors at home, such as homeschooling children or caring for elderly family members, may also reduce the time needed for HCWs to decompress. 11 This combination of limited access to outlets for relief, reduced time, and increased work pressure may result in unmanaged stress and the adoption of maladaptive coping strategies. 9 In the context of the COVID-19 pandemic, the extensive duration and multiplicity of lockdowns (eg, in spring 2020 and again in fall 2020 among some European countries) 12 may have contributed to the adoption and cementation of such maladaptive coping behaviors.
One common maladaptive coping technique among HCWs is increased substance use and abuse. Lifetime prevalence of substance use disorders among HCWs is approximately 10% to 15%, 13 and alcohol use is known to increase in association with increased work-related stress. 14 Among HCWs, work-related stress is associated with increased alcohol use. 15 Overall, HCWs most commonly use or abuse (1) alcohol, (2) prescription drugs (most frequently opiates, anxiolytics), and (3) nonprescription drugs (opiates, illicit drugs). 16 Follow-up studies of HCWs exposed to SARS coronavirus 1 (SARS-CoV-1) found that working environments with a high risk of viral exposure or being quarantined was associated with alcohol use 3 years after the peak of the SARS outbreak. 17
Despite a growing body of evidence on the mental health responses of HCWs to pandemics and epidemics, to our knowledge no studies have evaluated current alcohol consumption and work-related stress together in the context of the COVID-19 pandemic. Given the known work-related stress associated with the COVID-19 pandemic, the likelihood of alcohol consumption as a maladaptive coping mechanism among HCWs responding to the crisis is elevated. The objectives of this study were to determine how stress related to the COVID-19 pandemic has contributed to alcohol consumption among HCWs and to understand their individual experiences.
Methods
Study Design
We conducted this mixed-methods study using a cross-sectional survey, administered electronically to HCWs working at an academic hospital during June 8-22, 2020. Data collected included both validated questionnaires, which we analyzed quantitatively, and open-ended questions, for qualitative analyses. Departmental business managers distributed the survey using department email lists (estimated distribution to approximately 550 recipients). Participation was open to all HCWs who interacted directly with patients. We obtained study approval from the Louisiana Health Sciences Center Institutional Review Board before survey distribution. Participants were allowed to skip any questions they did not wish to answer or terminate the survey at any time. All data were collected anonymously.
Research Setting
Before the emergence of COVID-19, the Louisiana health care system was already stressed: the southern United States had a higher prevalence of chronic disease than the United States in general, 18 and Louisiana ranked 49th in the nation for overall health. 19 As of March 31, 2020, southeast Louisiana was among the worst-hit areas of the country in COVID-19 cases per capita. When ranked by COVID-19 mortality per 100 000 residents, 4 of the top 6 counties in the United States were in the southeast Louisiana region. 20 Our study took place at an academic hospital in New Orleans, the largest city in this region of Louisiana.
Measures
Demographic data
We collected data on demographic characteristics, including sex (male, female), race (Black, White, American Indian/Alaska Native, Asian, Native Hawaiian/Other Pacific Islander), and age (18-29, 30-39, 40-49, 50-59, ≥60); years of experience (continuous); professional role (physician, nurse, “other” [ie, physician assistant, medical assistant, respiratory therapist]); and home life (married/living with a partner, living with children, living with elderly people).
Stress-related measures
The MERS coronavirus (MERS-CoV) Staff Questionnaire was developed and used to measure HCW responses to increased work-related stress during the 2014 MERS-CoV outbreak. 6 At the time of our study, this questionnaire was one of the only questionnaires available that had been validated in the context of a similar infectious epidemic. The questionnaire consists of 5 individually validated subsections: (1) emotional responses, (2) factors contributing to stress, (3) stress reduction supports made available to staff members, (4) personal coping strategies that respondents may have used, and (5) possible incentives that could promote willingness to participate in future coronavirus outbreaks. 6 We examined COVID-19–related stress using subsections 1 and 2. We analyzed composite scores per subscale as continuous variables. For data on coping, we included the Brief COPE scale in lieu of subsections 3 and 4 (which capture similar information but do not have as much literature support for comparison of results). The Brief COPE scale is a 28-item questionnaire in which participants report their use of various coping techniques. 21 We merged individual Brief COPE scale items into 3 primary factors as standardized by Litman 22 : (1) social support coping, (2) avoidant coping, and (3) self-sufficient coping. The Brief COPE scale has been validated cross-culturally and repeatedly shown to have strong face validity.23,24 We assessed HCWs’ motivations for future work during a pandemic with the MERS-CoV subsection 5. We ranked subsection factors according to the average Likert score assigned by all participants. We used the ranking of individual factors to evaluate the importance of tangible and intangible supports.
Mental health measures
The Patient Health Questionnaire–9 (PHQ-9) assesses depression criteria; scores ≥10 indicate clinically significant symptoms of depression (score range, 0-27). 25 The Primary Care Posttraumatic Stress Disorder Checklist (PC-PTSD) is a screening tool for posttraumatic stress. Scores ≥3 indicate clinically significant symptoms of PTSD (range, 0-5). Posttraumatic stress symptoms were previously identified among HCWs at hospitals with a high SARS-CoV-1 patient case load. 26
Alcohol Consumption
The Alcohol Use Disorders Identification Test–Consumption (AUDIT–C) is a 3-item measure for alcohol consumption derived from the AUDIT tool, originally developed by the World Health Organization. 27 AUDIT–C has been shown to perform as well as the original AUDIT tool. Scores for the AUDIT–C range from 0 to 12, with scores >3 considered positive in women and scores >4 considered positive in men. 28 We asked participants about current and pre–COVID-19 levels of alcohol consumption via duplicate administration of AUDIT–C. We considered the change in AUDIT–C score (from pre–COVID-19 to current ratings of alcohol consumption) to be the primary outcome variable during statistical analyses. Additional analyses examined current reported alcohol use via participant responses to AUDIT–C asking about their current consumption. We used these latter data to identify overall need among HCWs for targeted interventions.
Qualitative Data
To supplement and provide narrative context to the structured survey questions, we included qualitative prompts at the end of the survey. Open-ended response sections allowed participants to elaborate on lived experiences during the COVID-19 pandemic in response to 4 open-ended questions:
What aspects of the COVID-19 pandemic contribute most to your work-related stress?
How has the COVID-19 pandemic personally affected you (work, personal, or otherwise)?
How have social distancing recommendations affected you?
How have you managed any stress you have felt because of COVID-19?
Statistical Analysis
We conducted statistical analyses using SAS version 9.4 (SAS Institute, Inc). We used bivariate analyses to evaluate relationships between the predictor/adjustment variables and AUDIT–C. We calculated Pearson correlation coefficients to assess bivariate analyses between continuous study variables of interest. We used a multivariate linear regression model to evaluate predictors of increased alcohol consumption, including all adjustment variables with significant associations according to the bivariate analysis. We tested additional demographic variables for bivariate associations with change in AUDIT–C score; significant associations resulted in these variables also being included in the final regression model. We considered α = .05 to be significant. All tests were 2-tailed.
Thematic Analysis
We also conducted thematic analyses on responses to the 4 open-ended questions. Thematic analysis is typically used to examine self-reported interview data, but empirical evidence shows it can also be used to analyze text data if the questions are open-ended. 29 We used thematic analysis in our study because it provides a direct representation of a respondent’s point of view or experience. 30
In the first phase of the thematic analysis, 3 study investigators (K.B., C.T., R.W.) read the participant responses twice to become familiar with the qualitative data. They then identified the provisional themes that emerged from responses to each question to identify all possible analytic categories and ensure agreement on the final set of codes. Two investigators (K.B., C.T.) then developed a revised code set to combine repetitive codes and refine other codes to reflect total accuracy of the associated responses. Using the final coding structure, the 3 investigators independently recoded all responses and resolved discrepancies. Answers with multiple themes described by a respondent were assigned >1 code.
Results
Demographic Characteristics
One hundred two HCWs participated in the survey, although not all participants answered all questions (Table 1). Most participants self-identified as White (n = 80, 78.4%), as a physician (n = 68, 66.7%), and as working in internal medicine (n = 29, 28.4%) and surgery (n = 25, 24.5%) departments. We found no differences by sex.
Demographic characteristics of health care workers at an academic hospital who responded to a survey assessing experiences with work-related stress and alcohol consumption before and during the COVID-19 pandemic, New Orleans, Louisiana, 2020 a
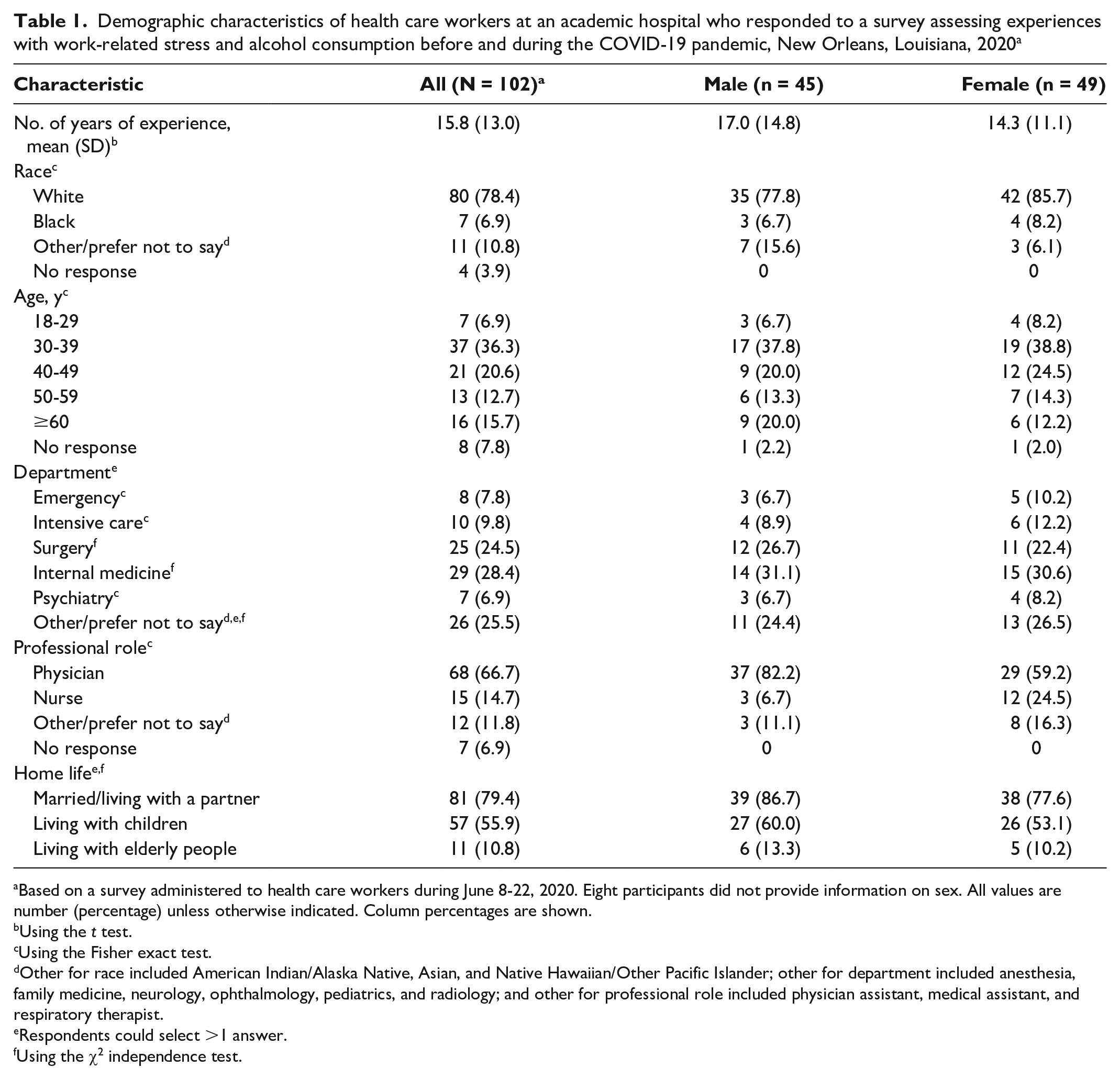
Based on a survey administered to health care workers during June 8-22, 2020. Eight participants did not provide information on sex. All values are number (percentage) unless otherwise indicated. Column percentages are shown.
Using the t test.
Using the Fisher exact test.
Other for race included American Indian/Alaska Native, Asian, and Native Hawaiian/Other Pacific Islander; other for department included anesthesia, family medicine, neurology, ophthalmology, pediatrics, and radiology; and other for professional role included physician assistant, medical assistant, and respiratory therapist.
Respondents could select >1 answer.
Using the χ2 independence test.
Quantitative Data
The mean (SD) PC-PTSD score was 1.2 (1.5), and the mean (SD) PHQ-9 score was 5.1 (4.9). Of 81 respondents, 15 (18.5%) had PC-PTSD scores ≥3 and a PHQ-9 score ≥10.
Pre–COVID-19, 22 of 44 (50.0%) men scored ≥4 and 21 of 47 (44.7%) women scored ≥3 on the AUDIT–C. For current alcohol consumption, 17 of 38 (44.7%) men scored ≥4 and 20 of 42 (47.6%) women scored ≥3. We observed no significant differences in AUDIT–C scores by sex. For both pre–COVID-19 and current alcohol consumption, AUDIT–C scores were higher among younger participants, particularly participants aged 18-29 (pre–COVID-19: 3.9; current: 4.2) and 30-39 (pre–COVID-19: 3.4; current: 4.1) than among participants aged 40-49 (pre–COVID-19: 1.7; current: 2.1) (Table 2). However, the change in AUDIT–C scores from pre-pandemic to current alcohol consumption was not significant across age groups (P = .66). Years of medical experience was negatively associated with current ratings of alcohol consumption (r = −0.24; P = .03) and with social support coping (r = −0.23; P = .04).
Categorical variables and associations with alcohol consumption as measured by the AUDIT–C, assessed among a sample (N = 102) of health care workers responding to the COVID-19 pandemic in New Orleans, Louisiana, 2020 a
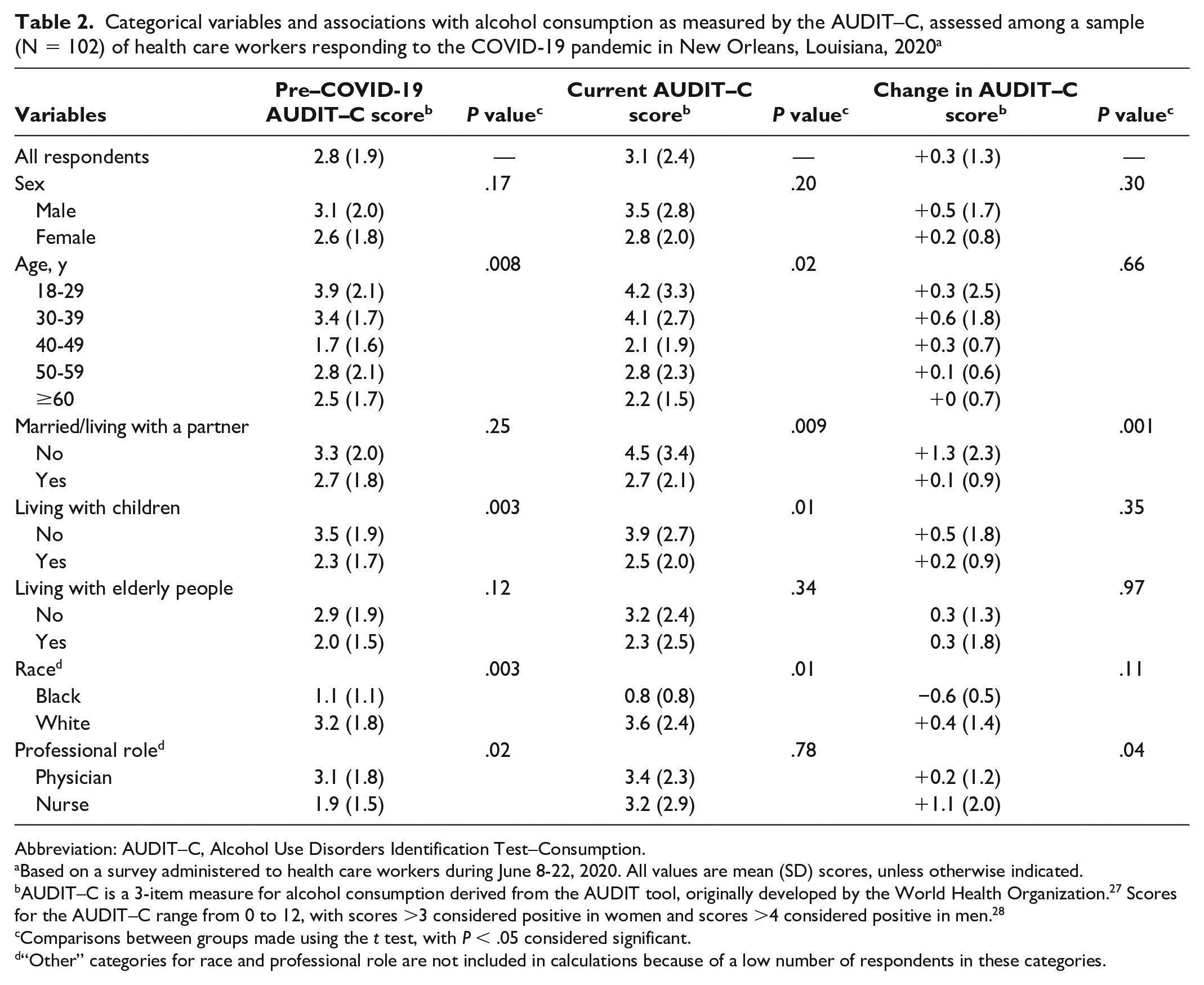
Abbreviation: AUDIT–C, Alcohol Use Disorders Identification Test–Consumption.
Based on a survey administered to health care workers during June 8-22, 2020. All values are mean (SD) scores, unless otherwise indicated.
AUDIT–C is a 3-item measure for alcohol consumption derived from the AUDIT tool, originally developed by the World Health Organization. 27 Scores for the AUDIT–C range from 0 to 12, with scores >3 considered positive in women and scores >4 considered positive in men. 28
Comparisons between groups made using the t test, with P < .05 considered significant.
“Other” categories for race and professional role are not included in calculations because of a low number of respondents in these categories.
AUDIT–C scores were significantly higher among participants not living with children (vs participants living with children) and among White (vs Black) participants (Table 2). Pre–COVID-19 AUDIT–C scores did not differ significantly between respondents who were married/living with a partner and respondents who were single, but scores increased significantly more among single respondents, such that single respondents scored nearly 2 points higher on the AUDIT–C for current alcohol consumption than for pre–COVID-19 alcohol consumption. Similarly, pre–COVID-19 AUDIT–C scores were significantly higher among physicians than among nurses, but scores increased significantly more among nurses than among physicians, such that both nurses and physicians endorsed equivalent current alcohol consumption.
The MERS Stress subscale score was significantly associated with change in AUDIT–C score from pre-pandemic to current, respondent PHQ-9 score and PC-PTSD score, and avoidant coping score (Table 3). The MERS Emotions subscale was similarly associated with PHQ-9, PC-PTSD, and current AUDIT–C scores.
Pearson correlations between continuous variables assessed among a sample of health care workers (N = 102) responding to the COVID-19 pandemic, New Orleans, Louisiana, 2020 a
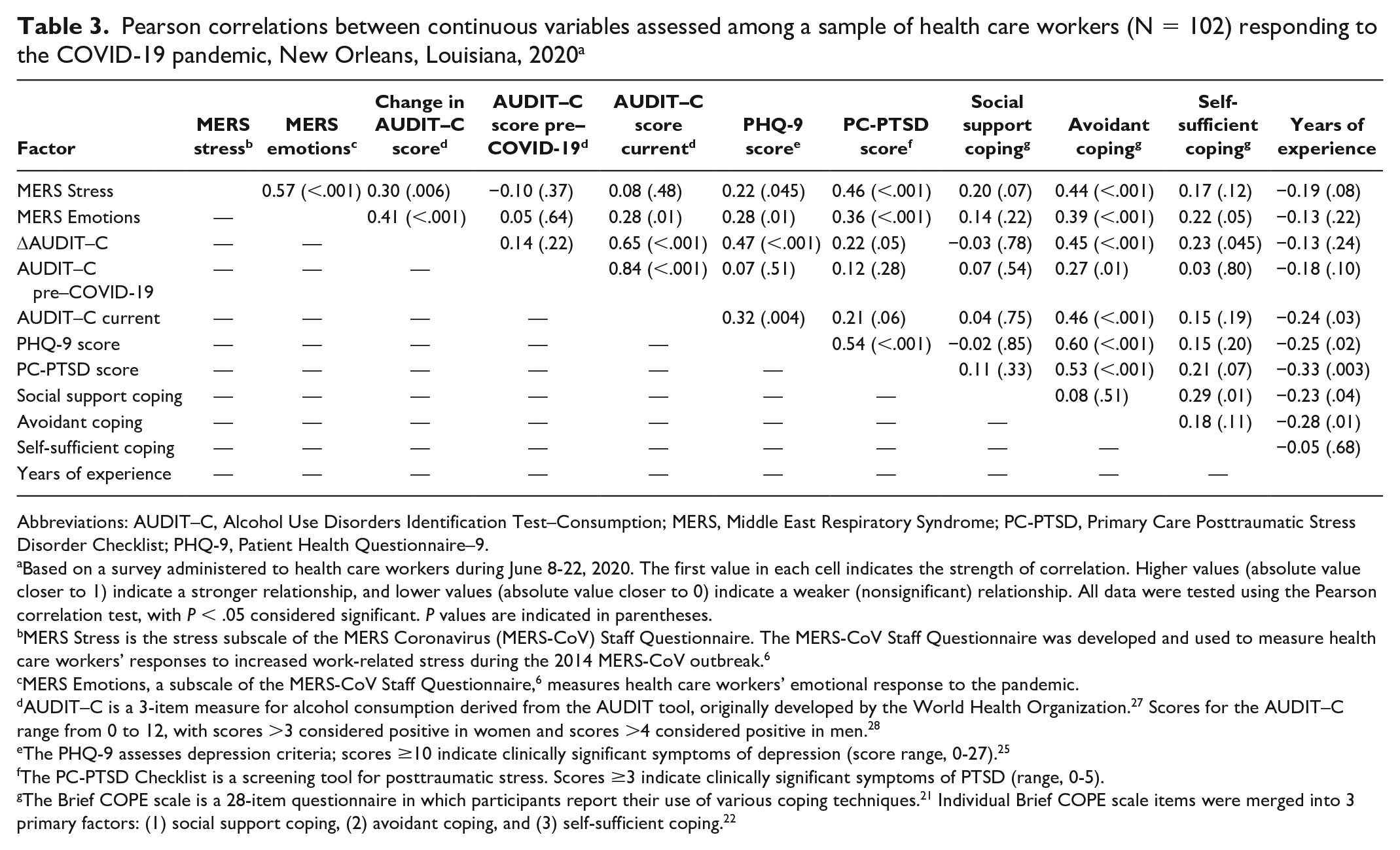
Abbreviations: AUDIT–C, Alcohol Use Disorders Identification Test–Consumption; MERS, Middle East Respiratory Syndrome; PC-PTSD, Primary Care Posttraumatic Stress Disorder Checklist; PHQ-9, Patient Health Questionnaire–9.
Based on a survey administered to health care workers during June 8-22, 2020. The first value in each cell indicates the strength of correlation. Higher values (absolute value closer to 1) indicate a stronger relationship, and lower values (absolute value closer to 0) indicate a weaker (nonsignificant) relationship. All data were tested using the Pearson correlation test, with P < .05 considered significant. P values are indicated in parentheses.
MERS Stress is the stress subscale of the MERS Coronavirus (MERS-CoV) Staff Questionnaire. The MERS-CoV Staff Questionnaire was developed and used to measure health care workers’ responses to increased work-related stress during the 2014 MERS-CoV outbreak. 6
MERS Emotions, a subscale of the MERS-CoV Staff Questionnaire, 6 measures health care workers’ emotional response to the pandemic.
AUDIT–C is a 3-item measure for alcohol consumption derived from the AUDIT tool, originally developed by the World Health Organization. 27 Scores for the AUDIT–C range from 0 to 12, with scores >3 considered positive in women and scores >4 considered positive in men. 28
The PHQ-9 assesses depression criteria; scores ≥10 indicate clinically significant symptoms of depression (score range, 0-27). 25
The PC-PTSD Checklist is a screening tool for posttraumatic stress. Scores ≥3 indicate clinically significant symptoms of PTSD (range, 0-5).
In the linear model of respondent current alcohol consumption, which included race and avoidant coping subscale score, the AUDIT–C score increased by an average of 0.38 points for each 1-point increase in avoidant coping subscale score (P < .001) (Table 3). In addition, White respondents scored an average of 2.4 points higher than Black respondents on the AUDIT–C (P = .009). In the linear model assessing change in AUDIT–C score, which included the MERS Emotions subscale, PHQ-9, and married/living with a partner, all variables were significant in the final model. Higher PHQ-9 scores were positively associated with an increase in AUDIT–C score (P = .007). In addition, being single was associated with an increase in AUDIT–C score (P = .02). Greater emotional stress, measured by the MERS Emotions subscale, was associated with greater increases in AUDIT–C score change (P = .004).
The highest ranked factor for work in future pandemics was availability of PPE (average rating, 2.7), followed by family support (average rating, 2.4) (Table 4). The lowest ranked factors for willingness to work in a future pandemic were availability of psychiatric support (average rating, 1.5) and reductions of work hours (average rating, 1.4). Availability of psychiatric support as a motivating factor was not significantly associated with higher PHQ-9 scores (P = .39), PC-PTSD scores (P = .14), or current alcohol consumption (P = .06).
Rank order of factors that are the most important motivators for work in a future pandemic, among a sample of health care workers (N = 102), New Orleans, Louisiana, 2020 a
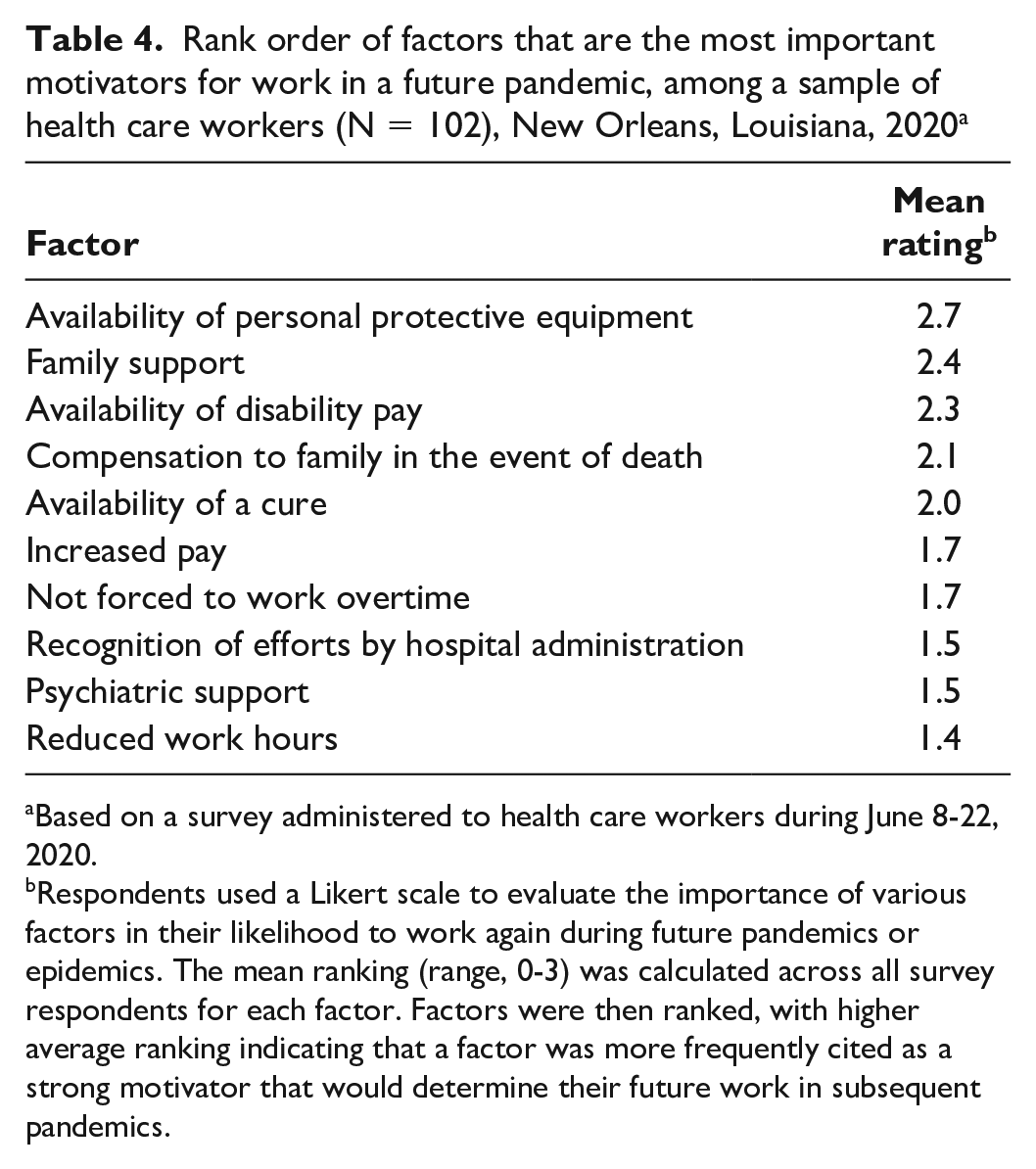
Based on a survey administered to health care workers during June 8-22, 2020.
Respondents used a Likert scale to evaluate the importance of various factors in their likelihood to work again during future pandemics or epidemics. The mean ranking (range, 0-3) was calculated across all survey respondents for each factor. Factors were then ranked, with higher average ranking indicating that a factor was more frequently cited as a strong motivator that would determine their future work in subsequent pandemics.
Qualitative Data
Seventy participants responded to the open-ended questions (Table 5). Thematic analyses showed reports of high levels of stress related to working conditions and the effect of work on respondents’ personal lives. Respondents indicated that work-related stress stemmed largely from risk of viral exposure (n = 29), which contained subthemes related to lack of PPE, fears of infection, and fears of transmitting the virus to others. Thirty-three (47.1%) respondents indicated that social distancing guidelines had led to feelings of social isolation—the largest proportion of agreement among any of the themes. Descriptions of isolation varied from lack of contact with family and friends to experiences of rejection from others as a result of observing guidelines. One respondent said: “My husband and I have been very strict in keeping ourselves distanced. . . . We feel almost ostracized from our community because of our adherence to the rules that everyone else readily disobey.”
Summary of responses to open-ended questions on the experiences of a sample of health care workers (N = 102) during the COVID-19 pandemic, New Orleans, Louisiana, 2020
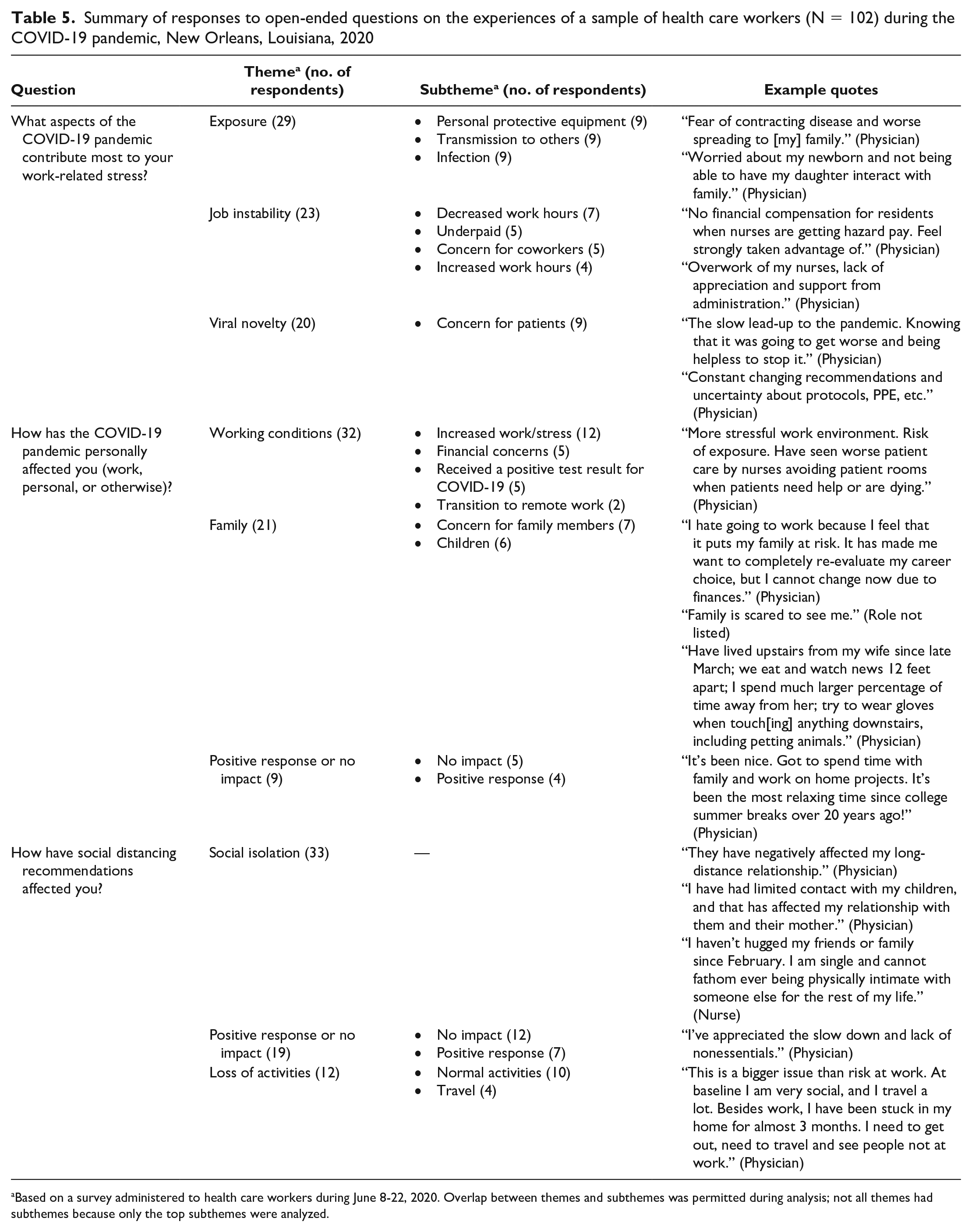
Based on a survey administered to health care workers during June 8-22, 2020. Overlap between themes and subthemes was permitted during analysis; not all themes had subthemes because only the top subthemes were analyzed.
Nine respondents indicated minimal to no impact of the pandemic, and 19 respondents described the effect of social distancing guidelines on their lives (Table 5). Of these 19 respondents, more respondents indicated no or minimal effects (n = 12) than reported positive effects (n = 7). Seven respondents reported alcohol and substance use as a stress management technique. One participant self-reported seeing a mental health professional to manage pandemic-related stress. Twelve participants reported reliance on prayer or meditation to manage their increased stress.
Discussion
Our study found that the COVID-19 pandemic has increased stress among HCWs, and approximately half of HCWs reported high current alcohol consumption such that they fulfilled screening criteria for alcohol use disorder. Significant predictors of higher consumption during the pandemic included White race and high use of avoidant coping. Significant predictors of greater magnitude of change from pre-pandemic to current alcohol consumption included a stronger emotional reaction to the pandemic, a higher level of depression symptoms, and being single. These findings are consistent with predictions of excessive alcohol consumption among people with negative emotional states during the pandemic. 31 Conversely, analyses of qualitative data suggested that a small number of respondents (n = 7) were managing stress through alcohol or substance use, although a strong emotional reaction to the pandemic was a significant predictor of increased alcohol consumption relative to the pre-pandemic baseline. This discrepancy between quantitative scores and qualitative reports of alcohol consumption may be the result of social desirability bias. 32 Alternatively, HCWs may not recognize their own alcohol consumption as problematic, particularly in the context of a pandemic. If social norms among HCWs develop such that increased alcohol consumption in response to this heightened level of work-related stress becomes common and accepted, particularly during an extended pandemic such as COVID-19, these behaviors may be harder to change in the future. After the 2003 SARS epidemic, studies showed that alcohol abuse and dependence persisted among HCWs who had experienced high exposure during their hospital work, at 3-year follow-up. 17
Despite the need for behavioral health interventions to reduce the risk of initiating or continuing alcohol abuse, access to such services was not rated by HCWs as a strong motivator for future pandemic work. Although many HCWs in this study were managing well, HCWs with the greatest risk for increased alcohol consumption had the highest avoidant coping and emotional distress related to the pandemic. These data demonstrate the importance of broad stress management interventions to reduce unhealthy, avoidant coping.
Qualitative analyses indicated that some respondents also relied in part on their spirituality to cope with pandemic-related stress. Although religion and coping was not the explicit focus of our study, other researchers have found that religious coping is associated with reductions in depression and anxiety.9,33 Although not all HCWs have strong religious sentiments, future interventions should inquire about the spiritual needs of HCWs, given the current knowledge base. More broadly, such interventions to address all facets of HCW wellness should be made accessible and sustainable via long-term health surveillance systems.34,35 Models for policy-level changes emphasizing mental health have emerged, such as the Mental Health PPE model, which is a program designed to enhance resilience among HCWs. 36 However, data are currently lacking on the efficacy of such programs.36,37 In addition to program evaluation overall, developers should assess the adaptability of models such as the Mental Health PPE for potential rapid deployment in the context of future crises.
Pandemics and outbreaks have greater effects on nurses than on physicians. 38 In our study, unadjusted analyses found increased alcohol consumption among nurses compared with physicians that was not significant in adjusted analyses. Studies should continue to engage medical professionals to assess the ways that COVID-19–related stress manifests. Perceived stress has been positively associated with distress among physicians under normal conditions, 39 and our study showed significant bivariate associations among COVID-19–related work stress, depression, and PTSD symptoms. Although we did not find differences in changes in alcohol consumption by professional role, the mental health needs of physicians and nurses, manifest from their respective roles, should be explored.
Factors outside the hospital environment may be relevant to the level of stress felt by HCWs in various roles: a quad-lingual international study of HCWs from 173 countries found that bullying outside the hospital environment was common during the first wave of the COVID-19 pandemic (April and May 2020). 40 A study based in Mexico similarly found that stress during the COVID-19 pandemic occurred as a result of work-area xenophobia (bullying, similar to the aforementioned study), the stress of working with COVID-19 patients, and having a high daily patient census. 41
Strengths and Limitations
This study had 2 limitations. First, our study included a disproportionately high number of White respondents, which potentially limited the generalizability of our findings. However, most HCWs in the United States (approximately 65%) are White, and this percentage is higher among physicians. 42 Future research on this topic should focus on the experiences of HCWs of color. Second, asking participants to quantify alcohol consumption before the pandemic may have been subject to recall bias; however, no other approximation was available.
This study also had several strengths. First, we gathered data on the health effects of the COVID-19 pandemic on HCWs and the needs of HCWs during the pandemic, at the time during which these stressors were experienced. A second strength was the period of data collection: our data reflect the conditions of HCWs during the first wave of the pandemic. Thus, our data are useful not only for demonstrating areas of needed follow-up work to ensure restoration of well-being for HCWs but also for guiding the responses of hospital administrators managing additional waves of the pandemic. Finally, our study included qualitative and quantitative data. Use of this mixed-methods approach allowed us to capture the full scope of feelings of HCWs in our sample.
Conclusions
COVID-19 continues unabated, 12 and the stress of the pandemic on HCWs will likely also continue. As seen in countries with recent experiences of humanitarian or public health crises, and countries with earlier cases of COVID-19, support during and after the pandemic is vital to preventing long-term mental health morbidity among HCWs.43,44 Interventions should emphasize stress management and the stated needs reported by HCWs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.