
Abstract
Objectives
Although data on the prevalence of current asthma among adults and children are available at national, regional, and state levels, such data are limited at the substate level (eg, urban–rural classification and county). We examined the prevalence of current asthma in adults and children across 6 levels of urban–rural classification in each state.
Methods
We estimated current asthma prevalence among adults for urban–rural categories in the 50 states and the District of Columbia and among children for urban–rural categories in 27 states by analyzing 2016-2018 Behavioral Risk Factor Surveillance System survey data. We used the 2013 National Center for Health Statistics 6-level urban–rural classification scheme to define urban–rural status of counties.
Results
During 2016-2018, the current asthma prevalence among US adults in medium metropolitan (9.5%), small metropolitan (9.5%), micropolitan (10.0%), and noncore (9.6%) areas was higher than the asthma prevalence in large central metropolitan (8.6%) and large fringe metropolitan (8.7%) areas. Current asthma prevalence in adults differed significantly among the 6 levels of urban–rural categories in 19 states. In addition, the prevalence of current asthma in adults was significantly higher in the Northeast (9.9%) than in the South (8.7%) and the West (8.8%). The current asthma prevalence in children differed significantly by urban–rural categories in 7 of 27 states. For these 7 states, the prevalence of asthma in children was higher in large central metropolitan areas than in micropolitan or noncore areas, except for Oregon, in which the prevalence in the large central metropolitan area was the lowest.
Conclusions
Knowledge about county-level current asthma prevalence in adults and children may aid state and local policy makers and public health officers in establishing effective asthma control programs and targeted resource allocation.
Asthma is a chronic inflammatory condition characterized by wheezing, chest tightness, shortness of breath, and overproduction of mucus. 1 It is a chronic lung disease and can affect people of all ages, although the incidence rate is higher in children than in adults. 2 Although asthma cannot be cured, the symptoms can be controlled by reducing exposure to asthma-inducing agents and following appropriate treatment guidelines. 1 In the United States in 2018, 19.2 million (7.7%) adults aged ≥18 and 5.5 million (7.5%) children aged <18 reported having current asthma. 3 The current asthma prevalence differs not only by demographic and socioeconomic factors but also by geographic location (eg, US Census region and state). 4,5 Although data on the current asthma prevalence among adults and children are available at the national and state levels, similar data are limited at the substate level (eg, urban–rural classification and county).
The ability to identify the current asthma prevalence at the county level, rather than at the state level or by region, may help policy makers and practitioners develop and evaluate policies and programs that are more targeted and, therefore, potentially more effective than previous policies and programs. The objective of this study was to examine current asthma prevalence by urban–rural classification at the substate level to provide detailed data for decision making.
Methods
To estimate the current asthma prevalence among child and adult populations by urban–rural categories across states 6 in the United States and to obtain a sample size large enough (≥50 respondents in the denominator) 7 for substate estimations, we first combined and analyzed Behavioral Risk Factor Surveillance System (BRFSS) data from 2016, 2017, and 2018. 8 The BRFSS is an annual, state-based, random-digit–dial telephone survey designed to collect data on health risks and behaviors, health conditions, and health practices from noninstitutionalized US adults aged ≥18. The survey consists of the core component, optional modules, and state-added questions. Core modules contain questions that all states use. Optional modules, which focus on a set of questions about a specific topic, such as child asthma prevalence, are used at the discretion of individual states. State-added questions are developed and administered by state health officials. 9 The median BRFSS response rate for all states, territories, and the District of Columbia was 47.0% in 2016, 45.1% in 2017, and 49.9% in 2018. All responses were self-reported, and adult proxy interviews for children were conducted. Because this study was based on an analysis of secondary data, the Centers for Disease Control and Prevention (CDC) project review process determined that it was exempt from institutional review board review.
Aggregated 2016-2018 BRFSS data include information on adults with current asthma for all 50 states and the District of Columbia. However, because the module on child asthma is optional, data on children with current asthma were limited to the 27 states that opted to use the module. We did not analyze data on current asthma for adults and children collected by US territories, because the 2013 National Center for Health Statistics (NCHS) urban–rural classification scheme does not apply to US territories.
The BRFSS includes 2 questions to assess current asthma status: “Has a doctor, nurse, or other health professional ever told you that you had asthma?” and “Do you still have asthma?” Survey respondents who answered yes to both questions were considered to currently have asthma. 9,10
The BRFSS lacked sufficient data for a reliable estimation of current asthma prevalence in most US counties. Thus, we aggregated county-level data in each state into 6 groups using the 2013 NCHS 6-level urban–rural classification scheme for US counties and county-equivalent entities. 6 At the state level, we analyzed adult and child current asthma prevalence by the 6-level urban–rural categories outlined by the 2013 NCHS urban–rural classification scheme. 6 This scheme was developed to monitor the health of residents in urban areas versus rural areas. The 2013 NCHS urban–rural classification scheme classified US counties and county-equivalents into 6 categories ranging from large central metropolitan to noncore. Large central metropolitan areas include counties in metropolitan statistical areas (MSAs) that have a population ≥1 million and contain the entire or part of the population of the principal city; large fringe metropolitan areas include counties in MSAs that have a population ≥1 million and include the surrounding counties of the MSA; medium metropolitan areas include counties in MSAs that have a population of 250 000-999 999; small metropolitan areas include counties in MSAs that have a population <250 000; micropolitan areas include counties in micropolitan statistical areas that have a population of 10 000-49 999; and noncore areas include most rural counties that did not qualify to be micropolitan. 6 We calculated current asthma prevalence for adults and children for all available urban–rural categories in each state and current adult prevalence for each of the 4 US Census regions (ie, Northeast, Midwest, South, and West).
We used SAS version 9.4 (SAS Institute, Inc) and SAS-callable SUDAAN version 11 (RTI International) to account for the complex survey design of the data in calculating weighted prevalence estimates with SEs and 95% CIs. We used survey weights to adjust for nonresponse and to produce estimates generalizable to a participating state’s population. 11 We used the Wald χ2 test of association and nondirectional 2-tailed z tests for testing group differences, with α = .05 considered significant.
According to the 2013 NCHS urban–rural classification scheme, 23 states (Alaska, Arkansas, Connecticut, Delaware, Hawaii, Idaho, Iowa, Kansas, Maine, Mississippi, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New Mexico, North Dakota, Rhode Island, South Carolina, South Dakota, Vermont, West Virginia, and Wyoming) and the District of Columbia did not have areas in all 6 levels of urban–rural categories. For example, Rhode Island had only 2 levels, and Delaware had only 3 levels. 6
Results
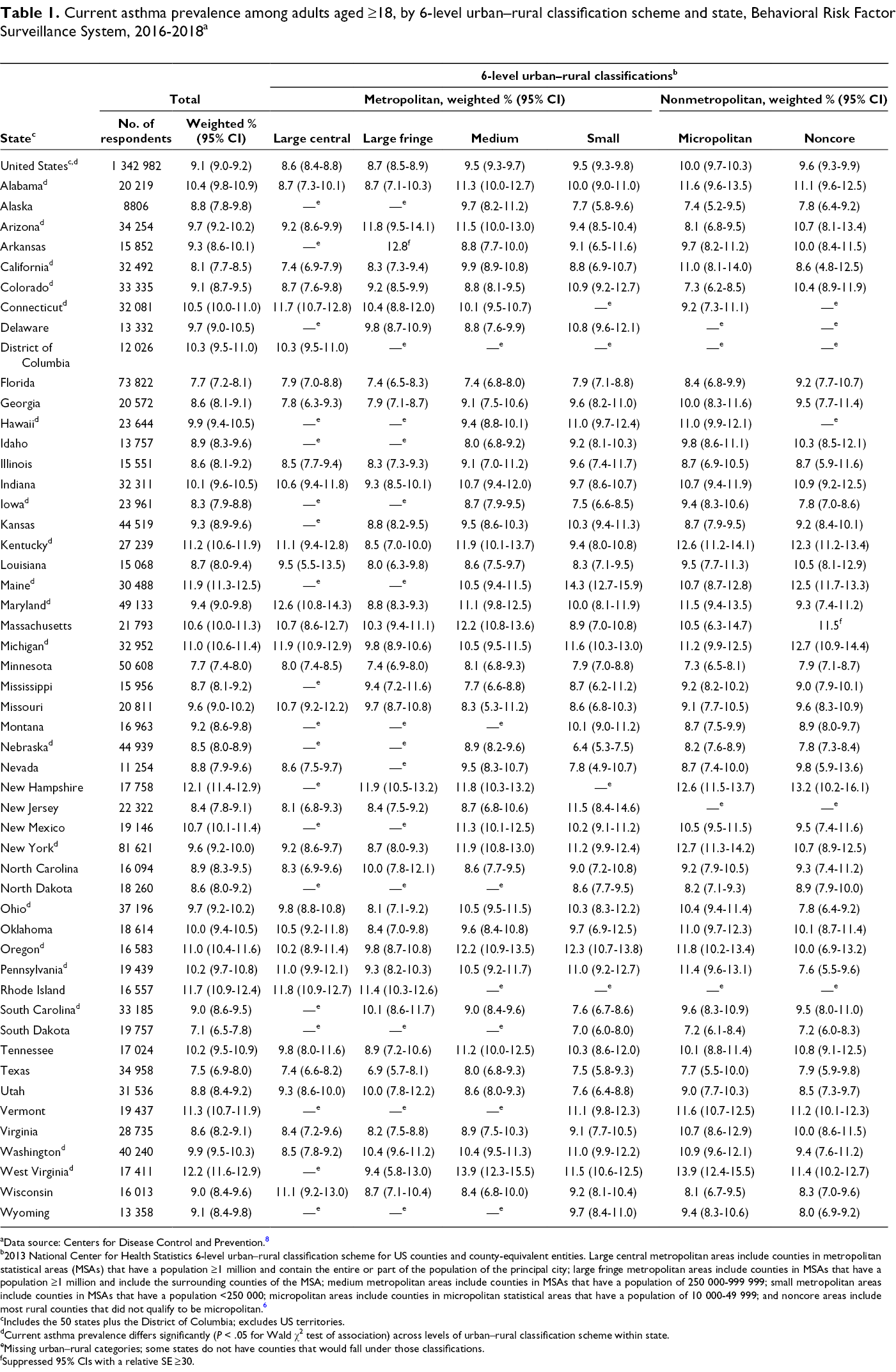
Current asthma prevalence among adults varied by state and urban–rural classification in each state (Table 1). During 2016-2018, the overall US adult current asthma prevalence was 9.1% (95% CI, 9.0%-9.2%), ranging from 8.6% (95% CI, 8.4%-8.8%) in large central metropolitan areas to 10.0% (95% CI, 9.7%-10.3%) in micropolitan areas. The overall current asthma prevalence among US adults in large central metropolitan areas (8.6%; 95% CI, 8.4%-8.8%) and large fringe metropolitan areas (8.7%; 95% CI, 8.5%-8.9%) was lower than the prevalence in medium metropolitan (9.5%; 95% CI, 9.3%-9.7%), small metropolitan (9.5%; 95% CI, 9.3%-9.8%), micropolitan (10.0%; 95% CI, 9.7%-10.3%), and noncore (9.6%; 95% CI, 9.3%-9.9%) areas. For 19 states, the adult current asthma prevalence differed significantly among the urban–rural categories in each state. Adult current asthma prevalence ranged from a low of 7.1% (95% CI, 6.5%-7.8%) in South Dakota to a high of 12.2% (95% CI, 11.6%-12.9%) in West Virginia.
Current asthma prevalence among adults aged ≥18, by 6-level urban–rural classification scheme and state, Behavioral Risk Factor Surveillance System, 2016-2018 a
aData source: Centers for Disease Control and Prevention. 8
b2013 National Center for Health Statistics 6-level urban–rural classification scheme for US counties and county-equivalent entities. Large central metropolitan areas include counties in metropolitan statistical areas (MSAs) that have a population ≥1 million and contain the entire or part of the population of the principal city; large fringe metropolitan areas include counties in MSAs that have a population ≥1 million and include the surrounding counties of the MSA; medium metropolitan areas include counties in MSAs that have a population of 250 000-999 999; small metropolitan areas include counties in MSAs that have a population <250 000; micropolitan areas include counties in micropolitan statistical areas that have a population of 10 000-49 999; and noncore areas include most rural counties that did not qualify to be micropolitan. 6
cIncludes the 50 states plus the District of Columbia; excludes US territories.
dCurrent asthma prevalence differs significantly (P < .05 for Wald χ2 test of association) across levels of urban–rural classification scheme within state.
eMissing urban–rural categories; some states do not have counties that would fall under those classifications.
fSuppressed 95% CIs with a relative SE ≥30.
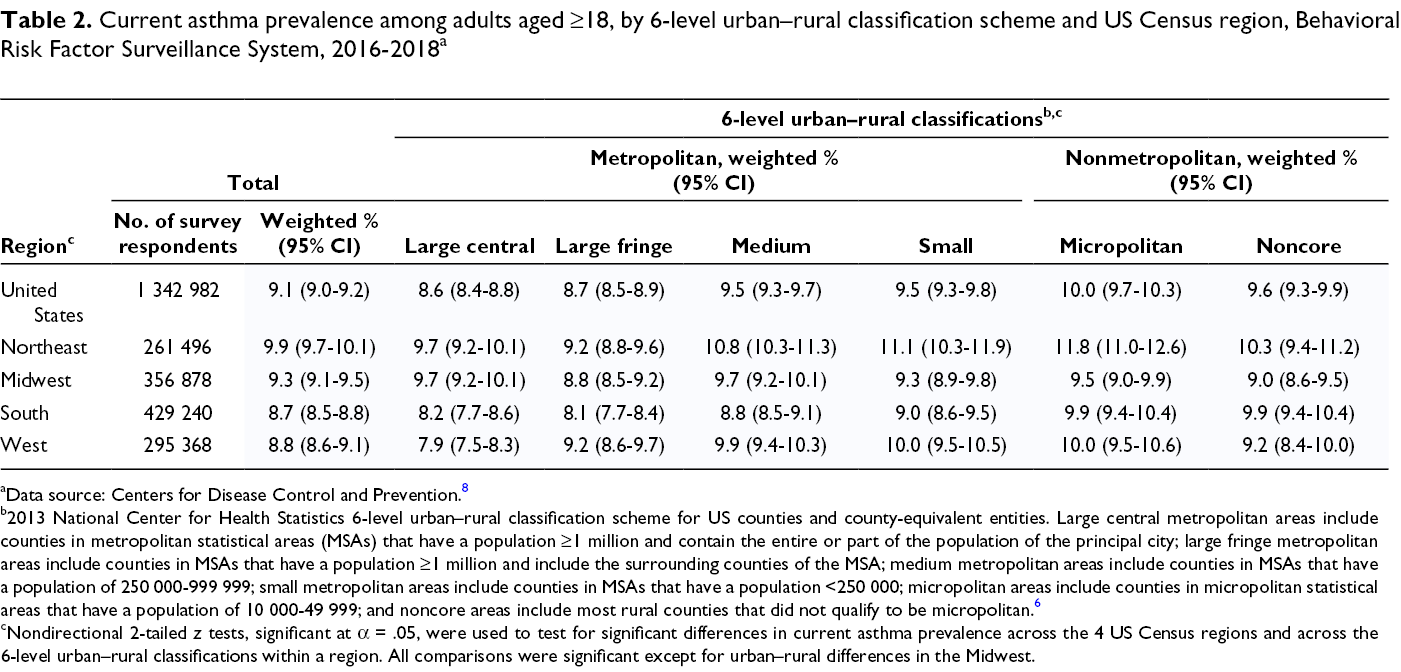
By US Census region, the current asthma prevalence among US adults was significantly higher in the Northeast (9.9%; 95% CI, 9.7%-10.1%) than in the South (8.7%; 95% CI, 8.5%-8.8%) and West (8.8%; 95% CI, 8.6%-9.1%) (Table 2). Current asthma prevalence among US adults in the Northeast, South, and West (but not Midwest) differed significantly by urban–rural classification. In both the Northeast and South, the prevalence was higher in medium metropolitan, small metropolitan, and micropolitan areas than in both large central and large fringe metropolitan areas. The prevalence was higher in noncore areas than in only large fringe metropolitan areas in the Northeast, but the prevalence was higher in noncore areas than in both large central and large fringe metropolitan areas in the South. In the West, the current asthma prevalence was higher in large fringe metropolitan, medium metropolitan, small metropolitan, micropolitan, and noncore areas than in large central metropolitan areas. Differences in asthma prevalence were significant for urban–rural categories in the Northeast (2.6%), the West (2.1%), and the South (1.8%) but not in the Midwest (0.9%).
Current asthma prevalence among adults aged ≥18, by 6-level urban–rural classification scheme and US Census region, Behavioral Risk Factor Surveillance System, 2016-2018 a
aData source: Centers for Disease Control and Prevention. 8
b2013 National Center for Health Statistics 6-level urban–rural classification scheme for US counties and county-equivalent entities. Large central metropolitan areas include counties in metropolitan statistical areas (MSAs) that have a population ≥1 million and contain the entire or part of the population of the principal city; large fringe metropolitan areas include counties in MSAs that have a population ≥1 million and include the surrounding counties of the MSA; medium metropolitan areas include counties in MSAs that have a population of 250 000-999 999; small metropolitan areas include counties in MSAs that have a population <250 000; micropolitan areas include counties in micropolitan statistical areas that have a population of 10 000-49 999; and noncore areas include most rural counties that did not qualify to be micropolitan. 6
cNondirectional 2-tailed z tests, significant at α = .05, were used to test for significant differences in current asthma prevalence across the 4 US Census regions and across the 6-level urban–rural classifications within a region. All comparisons were significant except for urban–rural differences in the Midwest.
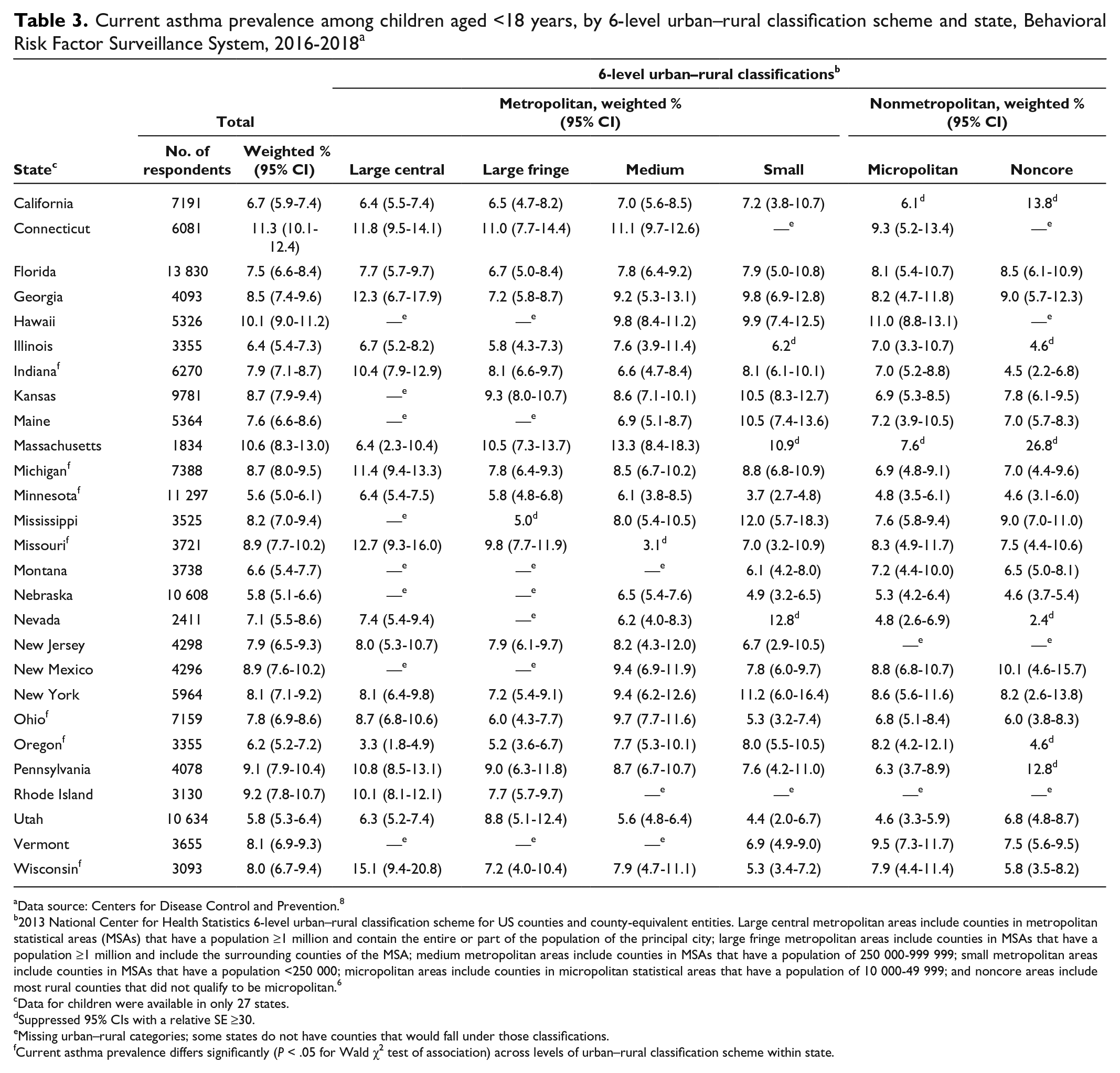
During 2016-2018, the current asthma prevalence among children in the 27 states that used the optional module to survey for asthma ranged from 7.3% (95% CI, 6.7%-7.9%) in micropolitan areas to 8.2% (95% CI, 7.6%-8.7%) in medium metropolitan areas but did not differ significantly by urban–rural classification (Table 3). Among those 27 states, asthma prevalence ranged from 5.6% (95% CI, 5.0%-6.1%) in Minnesota to 11.3% (95% CI, 10.1%-12.4%) in Connecticut. For all but 7 states (Indiana, Michigan, Minnesota, Missouri, Ohio, Oregon, and Wisconsin), asthma prevalence did not differ significantly by urban–rural classification. For those 7 states, the asthma prevalence in children was higher in large central metropolitan areas than in micropolitan or noncore areas (except for Oregon, in which the asthma prevalence in children in the large central metropolitan areas was the lowest).
Current asthma prevalence among children aged <18 years, by 6-level urban–rural classification scheme and state, Behavioral Risk Factor Surveillance System, 2016-2018 a
aData source: Centers for Disease Control and Prevention. 8
b2013 National Center for Health Statistics 6-level urban–rural classification scheme for US counties and county-equivalent entities. Large central metropolitan areas include counties in metropolitan statistical areas (MSAs) that have a population ≥1 million and contain the entire or part of the population of the principal city; large fringe metropolitan areas include counties in MSAs that have a population ≥1 million and include the surrounding counties of the MSA; medium metropolitan areas include counties in MSAs that have a population of 250 000-999 999; small metropolitan areas include counties in MSAs that have a population <250 000; micropolitan areas include counties in micropolitan statistical areas that have a population of 10 000-49 999; and noncore areas include most rural counties that did not qualify to be micropolitan. 6
cData for children were available in only 27 states.
dSuppressed 95% CIs with a relative SE ≥30.
eMissing urban–rural categories; some states do not have counties that would fall under those classifications.
fCurrent asthma prevalence differs significantly (P < .05 for Wald χ2 test of association) across levels of urban–rural classification scheme within state.
Discussion
Similar to previous studies, 3 -5 our study found that the current asthma prevalence differed by geographic location. The overall current asthma prevalence among adults in the 50 states and the District of Columbia was 9.1%, ranging from 7.1% in South Dakota to 12.2% in West Virginia, and among children in 27 states was 7.7%, ranging from 5.6% in Minnesota to 11.3% in Connecticut.
During 2016-2018, the current asthma prevalence among US adults in large central metropolitan (8.6%) and large fringe metropolitan (8.7%) areas was lower than in medium metropolitan (9.5%), small metropolitan (9.5%), micropolitan (10.0%), and noncore (9.6%) areas. We found similar patterns among adults in the Northeast, South, and West regions. We did not assess regional differences in current asthma prevalence among children because data were available from only 27 states and did not accurately represent the region where they were located. Although the prevalence of current asthma differed significantly by urban–rural classification among adults in 19 states and among children in 7 states, in most states the prevalence did not differ by urban–rural classification.
To our knowledge, our study is the first to provide data on the current asthma prevalence among adults and children by the 6-level urban–rural classifications in the 50 states and the District of Columbia (for adults), the 27 states where data were available (for children), and the 4 US Census regions. The benefit of our study is that the substate-level prevalence estimates can be used to estimate prevalence for any county in a particular state by referring to the prevalence estimate for that county’s urban–rural classification. For example, in Georgia, the current asthma prevalence among adults for the large central metropolitan area was 7.8%, and Fulton County, Georgia, is part of the large central metropolitan area as outlined in 2013 NCHS urban–rural classification data. Therefore, the current asthma prevalence in adults for Fulton County, according to its large central metropolitan status in Georgia, is expected to be about 7.8%.
Limitations
Our study had several limitations. First, the data were self-reported; therefore, the findings may be affected by recall bias. However, a standardized asthma case definition for surveillance has been used by most national and state surveys since 2001. Second, data for children were available from only 27 states; therefore, the findings might not be generalizable to children in states where we had no data. Finally, previous studies have suggested that asthma among inner-city children is often severe and difficult to control and that the prevalence of current asthma is higher among children in inner-city areas than in non–inner-city areas. 12,13 However, county-level asthma prevalence estimates in our study do not address asthma prevalence status in inner cities.
Conclusions
Current asthma prevalence estimates in adults and children for individual counties in each state can be derived from estimates provided by this study. Future research is needed to identify data collection methods and funding resources to collect county-level data to estimate asthma prevalence for individual counties directly. Knowing county-level current asthma prevalence is important for state and local health officials in establishing effective asthma control programs and strategies.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.